If you've been living with neuropathy pain for any length of time, you've probably noticed something frustrating: the pain doesn't just hurt your body. It seeps into everything — your mood, your sleep, your motivation, your sense of who you are. That's why I find duloxetine (sold under the brand name Cymbalta) so interesting as a neuropathy treatment. Unlike medications that only target pain, duloxetine works in the brain on pathways that influence both pain and mood — addressing two of the biggest challenges we face as neuropathy patients in one medication.
I've heard from many people in our support community who've had positive experiences with duloxetine, and I've also heard from those who struggled with it. In this article, I want to give you the complete picture — the science behind how it works, who it tends to help most, what the side effects really look like in practice, and practical tips for getting the best results if you and your doctor decide to try it.
Key Takeaway
Duloxetine (Cymbalta) is unique among neuropathy medications because it addresses both pain and mood through a single mechanism — boosting serotonin and norepinephrine in the brain. It's FDA-approved for diabetic neuropathic pain, generally weight-neutral, and may be especially helpful if chronic pain has been affecting your emotional well-being.
Browse all our treatments and therapies guides for more articles like this one.
How Duloxetine Works for Neuropathic Pain
Duloxetine belongs to a class of medications called SNRIs — serotonin-norepinephrine reuptake inhibitors. You might recognize this drug class from its more common use: treating depression and anxiety. But the same brain chemistry that affects mood also plays a critical role in how your body processes pain, and that's the key to understanding why duloxetine may help with neuropathy.
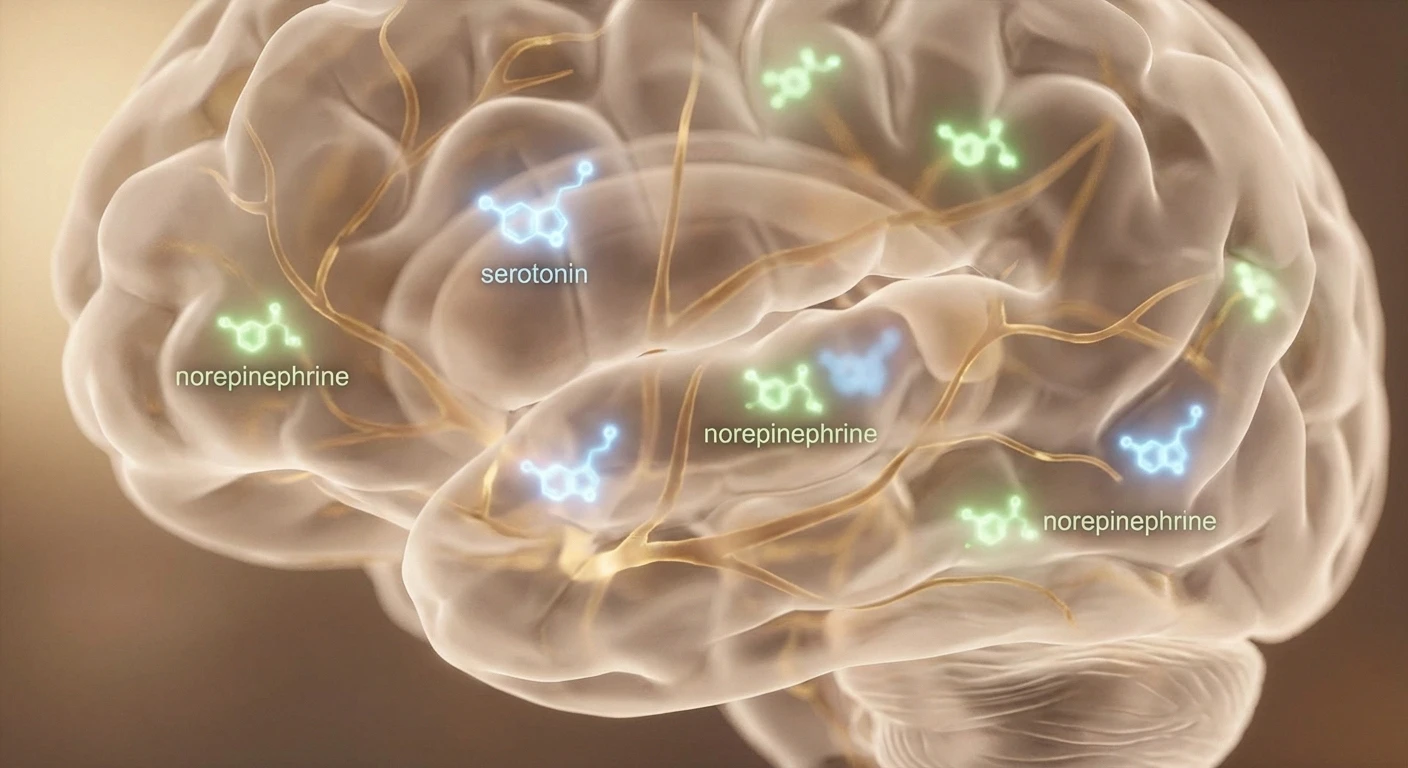
Your brain has a built-in pain modulation system — a set of pathways that can dial pain signals up or down before you consciously experience them. Two neurotransmitters are especially important in this system: serotonin and norepinephrine. These chemicals help activate what's called the descending inhibitory pain pathway — essentially your brain's natural “volume control” for pain.
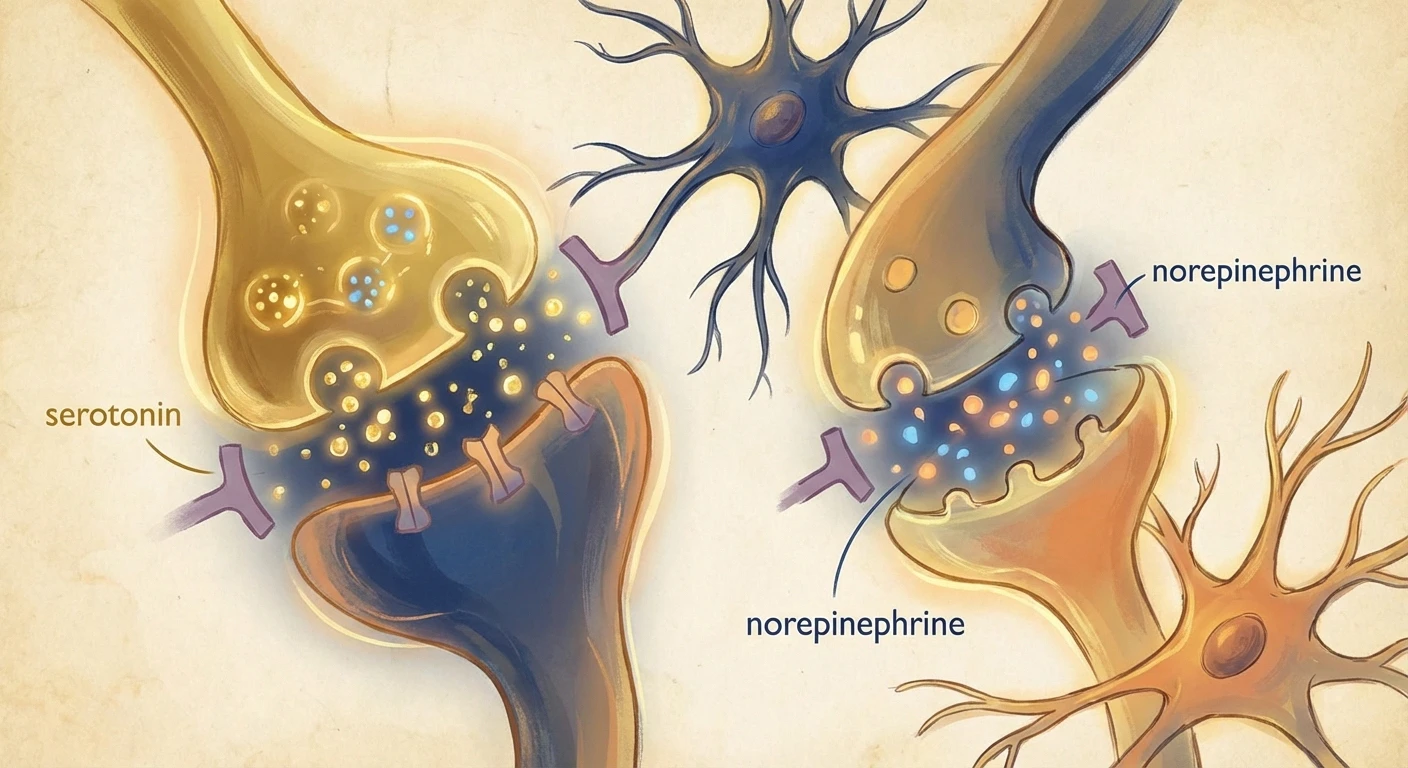
When you have chronic neuropathic pain, this natural pain-dampening system often becomes less effective. Your damaged nerves keep sending pain signals, and your brain's ability to filter them weakens over time. Duloxetine works by blocking the reabsorption (reuptake) of serotonin and norepinephrine, keeping more of these chemicals active in the spaces between nerve cells. This strengthens your brain's natural ability to suppress pain signals coming from your peripheral nerves.
It's a fundamentally different approach from medications like pregabalin or gabapentin, which work by calming overexcited peripheral nerves directly. Duloxetine works more “top-down” — it enhances your brain's ability to manage pain rather than quieting the pain signals at their source. Understanding the stages of neuropathy can help you appreciate why this central approach matters, especially as the condition progresses.
What the Clinical Evidence Shows
Duloxetine is one of only three medications with FDA approval specifically for diabetic peripheral neuropathic pain (alongside pregabalin and tapentadol). The evidence supporting its use is solid and comes from multiple well-designed clinical trials.
A comprehensive Cochrane review — the gold standard of evidence-based reviews — found that duloxetine at 60 mg daily is effective for painful diabetic peripheral neuropathy. The key finding: patients were 73% more likely to achieve at least a 50% reduction in pain compared to those taking a placebo (risk ratio of 1.73). In practical terms, roughly one in five patients who take duloxetine will get meaningful relief that they wouldn't have gotten from a placebo alone.
What's particularly noteworthy is that this benefit was seen consistently across multiple trials and held up at the 12-week mark. The 60 mg daily dose emerged as the sweet spot — 120 mg daily didn't produce significantly better pain relief but did increase side effects, while 20 mg daily was less effective.
More recently, duloxetine has shown promise for chemotherapy-induced peripheral neuropathy (CIPN), a type of nerve damage caused by cancer treatments. A 2022 study highlighted by OncLive found significant pain reduction in CIPN patients taking duloxetine — an exciting finding because very few treatments have shown clear benefit for this particular type of neuropathy.
more likely to achieve significant pain relief with duloxetine 60 mg vs. placebo in clinical trials
The Mood-Pain Connection: Duloxetine's Dual Benefit
Here's something that isn't discussed enough in neuropathy circles: chronic pain and depression have a bidirectional relationship. Pain worsens mood, and depressed mood amplifies pain perception. They share overlapping brain pathways, and they can create a vicious cycle that makes both conditions harder to treat.
This is where duloxetine has a meaningful advantage over some other neuropathy medications. Because it boosts both serotonin and norepinephrine, it can simultaneously address the pain and the emotional burden that comes with it. I can't overstate how significant this can be. Many people in our community report that duloxetine didn't just reduce their physical pain — it helped lift the cloud of hopelessness and frustration that chronic neuropathy can bring.
To be clear, you don't need to have clinical depression to benefit from duloxetine's mood effects. Even subclinical low mood, the kind of persistent emotional heaviness that living with chronic pain creates, may respond to duloxetine's neurotransmitter support. If you find that neuropathy pain that worsens at night is affecting your mental state during the day, this dual mechanism may be worth discussing with your doctor.
Who Is Duloxetine Best Suited For?
Based on the research and what I've observed in our community over the years, duloxetine tends to work particularly well for certain profiles:
People with diabetic peripheral neuropathy. This is the condition it's FDA-approved for, and the evidence base is strongest here. If diabetes is driving your neuropathy, duloxetine is considered a first-line option by most clinical guidelines.
Those dealing with both pain and mood challenges. If chronic pain has been dragging down your emotional well-being — or if you have a history of depression or anxiety — duloxetine's dual mechanism can be especially valuable.
People concerned about weight gain. Unlike pregabalin and gabapentin, which often cause some weight gain, duloxetine is generally weight-neutral and some people actually lose weight on it due to reduced appetite. For people with diabetes who are working hard to manage their weight, this can be a significant advantage.
Patients with coexisting fibromyalgia. Duloxetine is also FDA-approved for fibromyalgia, and some neuropathy patients also have fibromyalgia-like widespread pain. One medication addressing both conditions simplifies treatment.
People who experienced too many side effects from gabapentinoids. If pregabalin or gabapentin caused unacceptable drowsiness, cognitive fog, or weight gain, duloxetine offers a mechanistically different approach that may agree with you better.

Common Side Effects and How to Manage Them
Like all medications that affect brain chemistry, duloxetine comes with side effects that you should know about before starting. Here's what the clinical data and real-world experience tell us:
Nausea is by far the most common side effect and the most frequent reason people stop duloxetine in clinical trials. It affects roughly 20-25% of patients, particularly during the first 1-2 weeks. The crucial tip: taking duloxetine with food significantly reduces nausea for most people. If your doctor starts you at the full 60 mg dose and nausea is unbearable, ask about starting at 30 mg for the first week or two and then increasing.
Dry mouth is reported by about 10-15% of patients. Keep a water bottle handy and consider sugar-free lozenges or gum to stimulate saliva production. This usually becomes less bothersome over time.
Fatigue and drowsiness affect some people, while others find duloxetine somewhat energizing. If it makes you drowsy, try taking it at bedtime. If it's energizing, take it in the morning. Pay attention to how it affects you in the first week and adjust accordingly.
Constipation occurs in about 10% of patients. Staying hydrated, eating fiber-rich foods (a good habit for nerve health anyway if you're following a neuropathy-supportive diet), and gentle movement can help prevent this.
Decreased appetite can occur, particularly in the first few weeks. Some people view this as a benefit, but if you're already underweight or struggling to maintain nutrition, it's worth monitoring.
Sweating — including night sweats — is reported by some patients and can be persistent. This is one of the less-discussed side effects but can be bothersome enough to affect quality of life.
Sexual side effects including decreased libido and difficulty reaching orgasm can occur with SNRIs. This is an underreported issue because many people feel uncomfortable discussing it, but it's important to bring up with your doctor if it affects you — there are strategies to manage it.

The Discontinuation Challenge
This is perhaps the most important practical consideration about duloxetine that doesn't get enough attention: it must be tapered gradually when stopping. Abrupt discontinuation can cause a withdrawal syndrome that includes dizziness, nausea, headache, irritability, “brain zaps” (brief electrical shock sensations in the head), insomnia, and anxiety.
These discontinuation symptoms can range from mild to quite unpleasant, and they're one of the most common complaints I hear in support groups. The good news is that they're completely avoidable with proper tapering. If you and your doctor decide duloxetine isn't right for you, insist on a slow, gradual dose reduction — typically over at least 2-4 weeks, and sometimes longer if you've been taking it for a long time.
This isn't a reason to avoid duloxetine — it's simply a reason to work closely with your healthcare provider and never stop the medication on your own without medical guidance.
Duloxetine vs. Other Neuropathy Medications
Understanding how duloxetine compares to other common neuropathy medications can help you and your doctor make an informed choice:
Duloxetine vs. pregabalin (Lyrica): Both are considered first-line treatments for diabetic neuropathic pain. Pregabalin may provide somewhat stronger pain relief on average but tends to cause more drowsiness and weight gain. Duloxetine has the advantage of mood support and is typically weight-neutral. Some doctors prescribe both together for patients with severe pain who don't respond adequately to either alone.
Duloxetine vs. gabapentin (Neurontin): Similar considerations as with pregabalin. Gabapentin is less expensive and may cause fewer GI side effects, but duloxetine offers the mood-pain dual benefit and doesn't cause the same degree of cognitive dulling that some people experience with gabapentin.
Duloxetine vs. amitriptyline: Amitriptyline is an older tricyclic antidepressant that's also used for neuropathic pain. Both affect serotonin and norepinephrine, but amitriptyline affects additional neurotransmitter systems and generally has more side effects (dry mouth, urinary retention, sedation, cardiac effects). Duloxetine is considered the more modern, targeted option with a better side effect profile for most patients.
Duloxetine vs. topical treatments: Topical treatments like nerve pain creams work locally with minimal systemic side effects — a great option for localized foot or hand pain. However, duloxetine works systemically and may help with more widespread neuropathy symptoms. Many people use both approaches together, supporting nerve health from multiple angles. If you're considering topical options, we've reviewed some of the best creams for neuropathy elsewhere.
Important Warning
Never stop duloxetine abruptly. Sudden discontinuation can cause withdrawal symptoms including brain zaps, dizziness, nausea, and irritability. Always taper gradually under your doctor's supervision — typically over 2-4 weeks or longer.
Starting Duloxetine: A Practical Timeline
Knowing what to expect during the first few weeks can help you stick with duloxetine long enough to give it a fair trial. Here's a realistic timeline based on clinical data and community experience:
Week 1: Your doctor will typically start you at 30 mg daily (some start directly at 60 mg). Nausea and initial side effects are most likely during this week. Take it with food, preferably the same time each day. You may notice some changes in appetite, sleep, or energy. Significant pain relief is unlikely yet.
Weeks 2-3: If you started at 30 mg, your doctor will likely increase to 60 mg. Side effects usually begin to settle. Some people start noticing mild improvement in pain and mood around this time, though the full effect hasn't kicked in yet.
Weeks 4-6: This is typically when you'll know if duloxetine is going to work for you. Pain reduction, if it's going to happen, usually becomes clearly apparent by this point. Mood improvements are often noticeable as well. Side effects that are going to persist become clear by now.
Weeks 8-12: Maximum benefit is usually achieved within this timeframe. If you haven't noticed meaningful improvement by 8-12 weeks at 60 mg, your doctor may consider increasing to 120 mg or switching to a different medication.
Important Considerations and Interactions
Before starting duloxetine, make sure your doctor knows about:
Liver health. Duloxetine is processed by the liver, and it should not be used by people with significant liver disease. Your doctor may check liver function tests before prescribing and periodically during treatment.
Other medications. Duloxetine interacts with several common drugs. MAO inhibitors are a dangerous combination and must be avoided. Blood thinners like warfarin may be affected. Other serotonin-affecting medications (including some migraine drugs called triptans) can increase the risk of serotonin syndrome — a rare but serious condition. Always give your doctor and pharmacist a complete list of everything you take, including supplements like St. John's Wort.
Alcohol use. Combining duloxetine with heavy alcohol use increases the risk of liver damage. Moderate alcohol consumption should be discussed with your doctor, and many providers recommend limiting alcohol while on duloxetine.
Kidney function. While duloxetine is primarily processed by the liver, severe kidney impairment may require dose adjustments or make the medication inappropriate.
Blood pressure. Duloxetine can modestly increase blood pressure in some patients. If you already have hypertension, your blood pressure should be monitored when starting treatment.
Glaucoma. Duloxetine should be used with caution (or avoided) in people with uncontrolled narrow-angle glaucoma.
Complementing Duloxetine with Lifestyle Approaches
Medication works best when it's part of a comprehensive approach to managing neuropathy. While duloxetine addresses the pain and mood components, supporting your overall nerve health can enhance its effectiveness:
Stay physically active. Regular gentle exercise — walking, swimming, yoga, or seated exercises — supports nerve function and naturally boosts the same neurotransmitters that duloxetine targets. If you're looking for guidance, exercises specifically designed for neuropathy can help you stay active safely.
Support your nutritional foundation. B vitamins, alpha-lipoic acid, and anti-inflammatory nutrients support nerve health from a different angle than medication. Consider whether any vitamin deficiencies could be contributing to your neuropathy and discuss supplementation with your healthcare provider.
Prioritize sleep hygiene. Good sleep supports both pain management and mood. Duloxetine may help or hinder sleep depending on the individual — if it's activating for you, take it in the morning. Create a consistent sleep routine and keep your bedroom cool and dark.
Manage blood sugar carefully. If your neuropathy is diabetes-related, tight blood sugar control is the single most important factor in slowing nerve damage progression. Duloxetine manages the pain, but blood sugar control addresses the root cause.
Frequently Asked Questions About Duloxetine for Neuropathy
Making the Right Choice With Your Doctor
Choosing a neuropathy medication is a very personal decision that depends on your specific type of neuropathy, your other health conditions, the medications you're already taking, and what matters most to you in terms of benefits and side effects. Duloxetine is a strong option with genuine advantages — particularly its dual effect on pain and mood, its weight-neutral profile, and its solid evidence base for diabetic neuropathy.
If you're considering duloxetine, go into that conversation with your doctor prepared. Bring a list of your current medications and supplements. Be honest about any mood or anxiety challenges you're experiencing alongside your pain. Ask about the nausea management strategies from the start, and discuss a realistic timeline for evaluating whether it's working.
Most importantly, remember that finding the right medication sometimes takes patience. If duloxetine doesn't turn out to be the right fit, there are other well-studied options available, and your doctor can help you find the one that works best for your unique situation. You deserve relief, and with the right approach, it's absolutely possible to find it.


