Peripheral Neuropathy vs. Central Neuropathy: What's the Difference
People say “neuropathy” as if it automatically means a problem in the feet or hands. Usually that is true. But not always. Some symptoms that feel like neuropathy actually come from the brain or spinal cord, not the peripheral nerves. If you mix those up, the workup, the urgency, and the treatment plan can all go sideways.
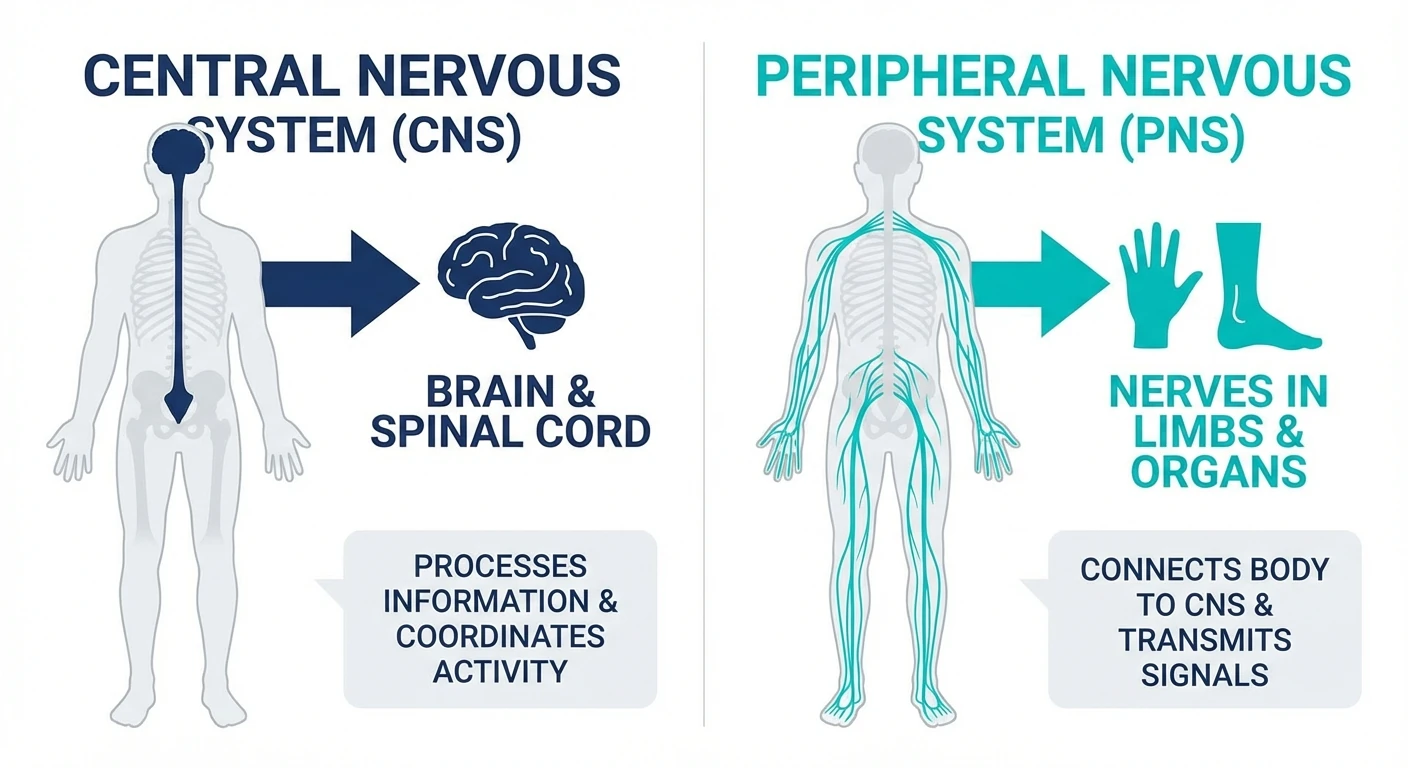
The simplest distinction is this: peripheral neuropathy comes from damage to nerves outside the brain and spinal cord. Central neuropathic symptoms come from disease or injury inside the central nervous system itself. The sensations can overlap — numbness, burning, tingling, weakness, balance issues — but the pattern usually does not. This guide explains the difference in patient language without pretending the two are interchangeable.
What Peripheral Neuropathy Means
Peripheral neuropathy affects the nerves that travel between the central nervous system and the rest of the body. That is why classic patterns often begin in the toes and feet, then move upward in a length-dependent “stocking” pattern. In more advanced cases the hands become involved too. If you want the broader architecture, our symptom overview and stages article help.
Common peripheral drivers include diabetes, vitamin deficiency, alcohol use, chemotherapy, toxins, entrapment, hereditary neuropathies, autoimmune disease, and infections. The key feature is that the problem lives in the peripheral wiring — the nerve itself, its myelin, or both.
What Central Neuropathic Symptoms Mean
Central neuropathic pain or central sensory dysfunction comes from the brain or spinal cord. That includes conditions like multiple sclerosis, spinal cord injury, cervical myelopathy, stroke, or other lesions that disrupt how the central nervous system processes sensation and movement. Patients still may say “my nerves are messed up,” but the source is upstream.
That distinction matters because central problems are more likely to bring additional neurologic clues: gait stiffness, abnormal reflexes, bowel or bladder dysfunction, visual changes, speech issues, facial involvement, or symptoms that do not fit a peripheral nerve distribution. Some people feel burning or electric pain, but the map looks wrong for standard peripheral neuropathy.
The Fastest Way to Tell the Difference
Pattern first. Tests second. Before you even get to EMG or MRI, the distribution of symptoms tells you a lot.
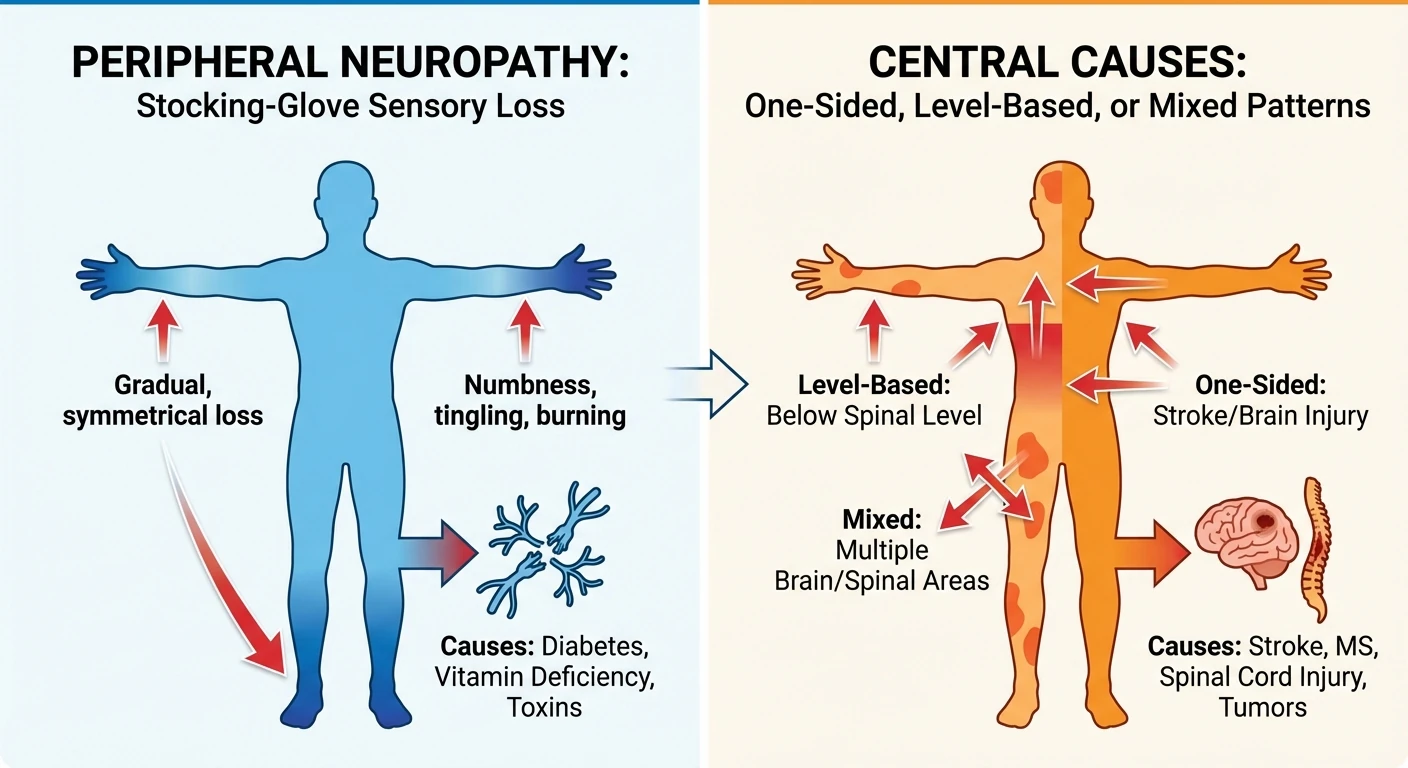
- Peripheral neuropathy usually starts distally and symmetrically — toes, feet, then possibly hands.
- Central problems are more likely to be patchy, one-sided, level-based, or tied to other brain/spinal cord signs.
- Peripheral weakness is often linked to specific nerves or a length-dependent pattern.
- Central weakness is more likely to involve spasticity, brisk reflexes, coordination problems, or bowel/bladder clues.
If symptoms are asymmetric, dermatomal, rapidly progressive, or paired with speech, vision, or incontinence issues, do not just label it neuropathy and move on. The AAFP differential logic is blunt on this point, and our pages on leg weakness differentials and tingling in hands show how that pattern-matching works.
How Testing Differs
For peripheral neuropathy, the core tools are usually history, exam, lab work, and sometimes EMG / nerve conduction studies. Those tests help identify axonal vs demyelinating patterns, severity, and whether the problem is diffuse or focal. In small-fiber cases, EMG may even be normal, which is why small fiber neuropathy can require skin biopsy or clinical pattern recognition.

For central causes, EMG may be normal or may not explain the symptom picture. That shifts attention toward MRI of the brain or spine, formal neurologic examination, and cause-specific testing. In other words, the wrong test can reassure you falsely if you are asking a peripheral question about a central problem.
Why Misclassification Matters
If you call a central problem “just neuropathy,” you can miss time-sensitive conditions like spinal cord compression, inflammatory CNS disease, or stroke-related deficits. If you call a peripheral problem central, you can send someone into a more dramatic workup than they need while missing common reversible causes like diabetes, B12 deficiency, alcohol use, or medication injury.
Wrong map, wrong workup
Treating a spinal cord or brain problem like routine peripheral neuropathy can delay urgent care. Treating common peripheral neuropathy like a dramatic central lesion can waste time and confuse the next step.
This is why a good differential is not academic. It changes urgency, the specialist you need, and the next test. If the picture is unclear, that is the moment to move beyond guesswork and get a more serious neurology evaluation.
Red Flags That Push the Needle Toward a Central Cause
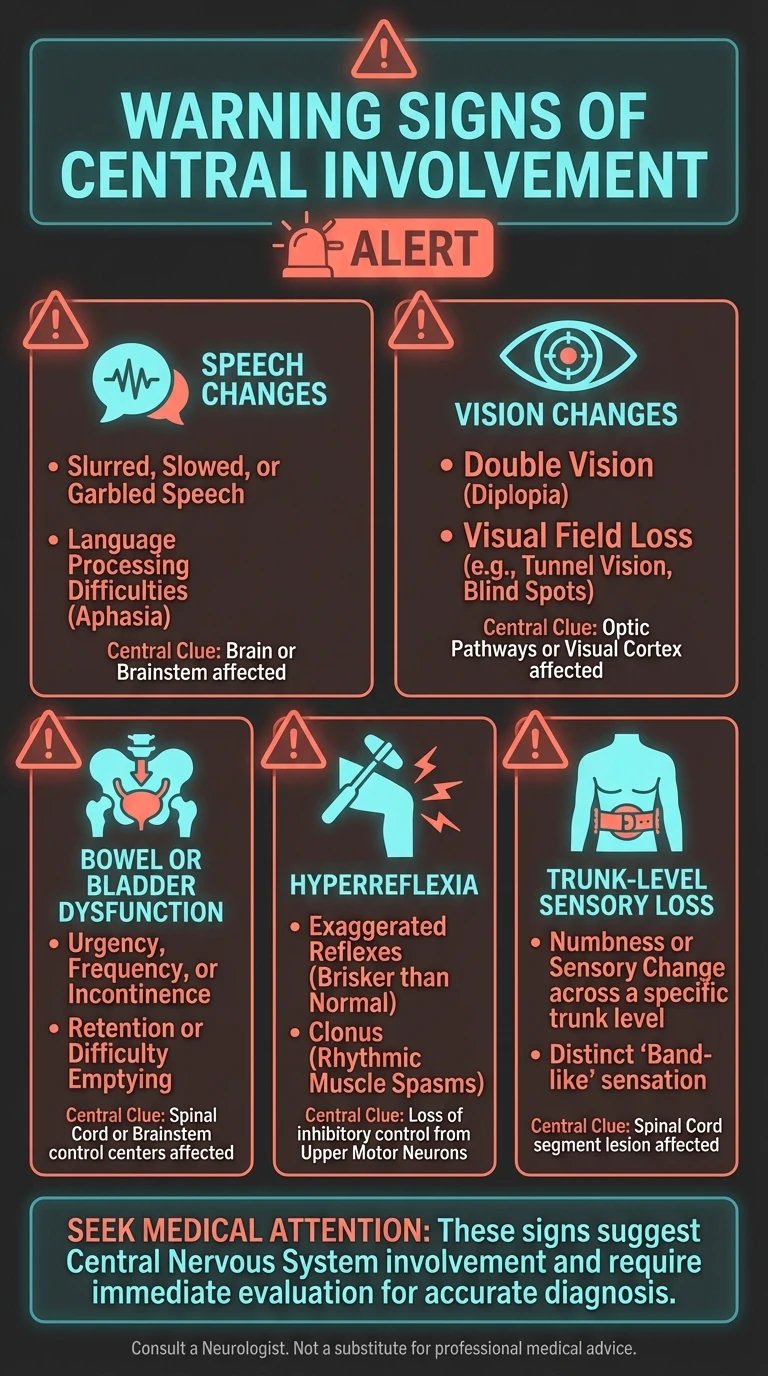
- Speech changes or facial weakness
- Double vision or other new visual symptoms
- Bowel or bladder dysfunction
- Hyperreflexia, leg stiffness, or spasticity
- A sensory level on the trunk or band-like symptoms around the torso
- Major imbalance that seems out of proportion to foot numbness alone
Those signs do not prove a central lesion, but they are enough to justify a broader workup. The cost of under-reacting is higher there than the cost of being a little cautious.

Central-leaning red flags
- Speech or facial changes
- Vision changes
- Bowel or bladder dysfunction
- Hyperreflexia or spasticity
- A sensory level on the trunk
The Bottom Line
Peripheral neuropathy is a wiring problem outside the brain and spinal cord. Central neuropathic symptoms come from the control center itself. The sensations can sound similar, but the map, exam, and testing logic are different. If your symptoms do not fit the usual stocking-glove script — or they come with bowel, bladder, vision, speech, or pronounced coordination issues — treat that as a signal, not background noise.
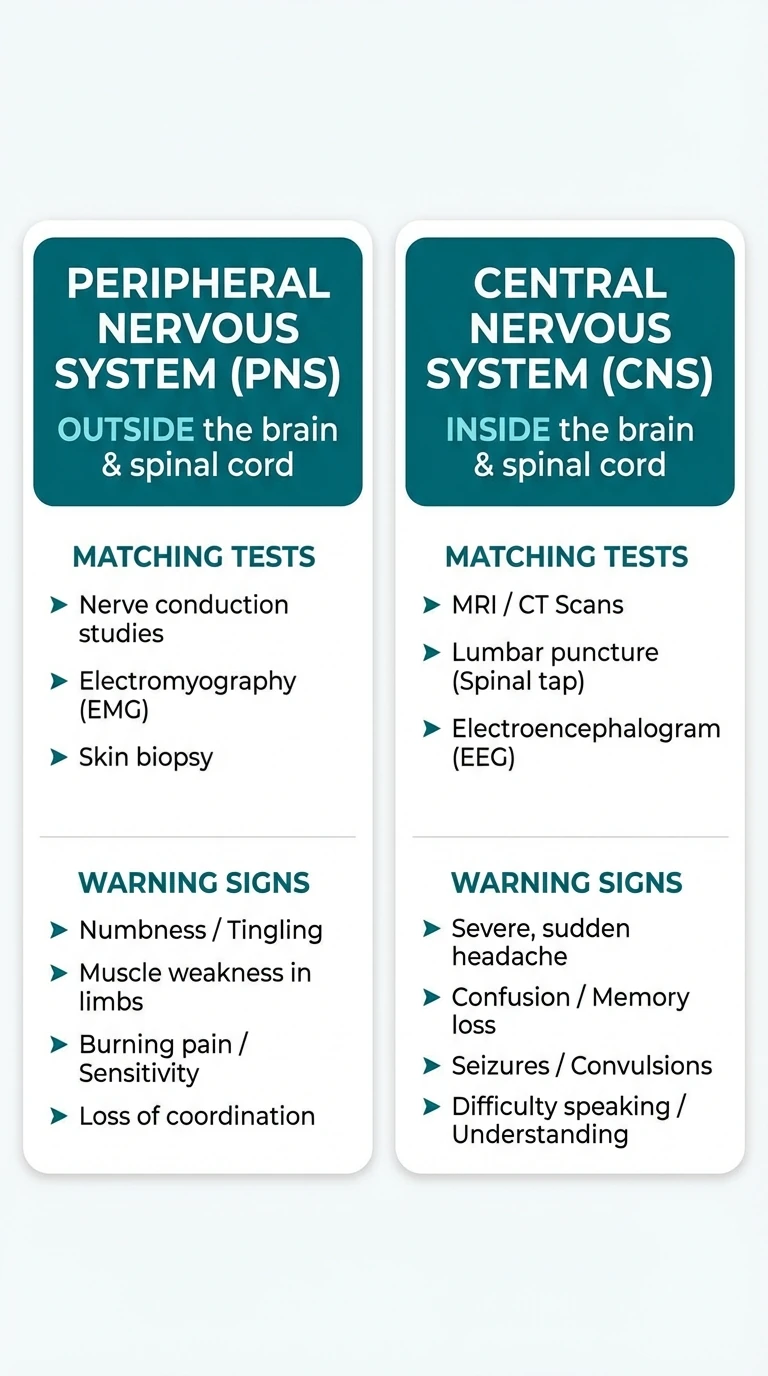
Peripheral = outside
Hands, feet, distal spread, EMG relevance, metabolic and toxic causes.
Central = inside
Brain or spinal cord involvement, higher urgency, MRI and neurologic exam matter more.
Frequently Asked Questions
What is the main difference between peripheral and central neuropathy?
Peripheral neuropathy starts in nerves outside the brain and spinal cord, while central neuropathic pain or central sensory problems come from injury or disease in the brain or spinal cord itself. The location of the damage changes the symptom pattern, exam findings, and treatment path.
Can central nervous system problems feel like neuropathy?
Yes. MS, spinal cord compression, stroke, and other central conditions can cause numbness, pain, weakness, or abnormal sensations that patients describe as neuropathy. That is why pattern recognition matters.
Is EMG useful for central neuropathy?
EMG and nerve conduction studies are most useful for peripheral nerve disorders. They may be normal when symptoms come from the brain or spinal cord, which is itself a clue.
When should I worry that symptoms are central instead of peripheral?
Think central if you have bowel or bladder changes, gait instability, hyperreflexia, speech or vision changes, facial involvement, or symptoms that do not follow a stocking-glove or nerve-root pattern.
Can someone have both peripheral and central nerve problems?
Yes. Diabetes, spinal stenosis, stroke history, multiple sclerosis, or cervical myelopathy can overlap. Mixed cases are exactly why a lazy one-label explanation can miss the real architecture.


