I still remember sitting in my primary care doctor's office, papers from three different specialists fanned out on the exam table, asking the question that had been bothering me for months: “Who actually treats this? My PCP says neurologist. My neighbor with diabetes swears by her endocrinologist. My sister-in-law's coworker sees a podiatrist for the exact same numb feet. Where am I supposed to start?”
If you've ever stared at a list of specialists and felt that familiar frustration — the one where every door seems half-open and you can't tell which one to walk through first — you are not alone. Neuropathy is one of those conditions that doesn't belong to any single specialty. It belongs to half a dozen, and the right doctor for you depends entirely on why your nerves are unhappy and what they're doing about it.
I'm Janet, and I write here as someone who has walked this exact maze. I'm not a doctor — I'm a patient advocate who reads the research and shares what I've learned with our community. What I want to give you today is a clear map: the doctors who actually treat neuropathy, what each one does, and the decision logic that tells you which one to see first, second, and (if needed) third. By the time you finish, you'll have a routing plan you can take to your next appointment.
Start Here: Your Primary Care Doctor
For about 95% of people who develop neuropathy symptoms, the right first stop is the same one you'd pick for any new health concern: your primary care doctor. Internal medicine, family medicine, or general practice — whoever you usually see for your physicals. There's a reason for this, and it's not laziness on the system's part.
Your primary care doctor is the right first stop for almost all new neuropathy symptoms. They can order the blood work (CBC, CMP, A1C, B12 + MMA, TSH, SPEP, ANA) that resolves many cases without a specialist ever being needed.
Many causes of neuropathy are findable and reversible with basic blood work that any PCP can order. Vitamin B12 deficiency. Uncontrolled diabetes. Thyroid imbalance. Sometimes even early-stage kidney trouble or a problem with a medication you're already taking. None of those needs a specialist to discover. They need someone willing to order the right panel of labs and look at the results carefully.
When you go to your first appointment, ask your PCP to consider running:
- Complete blood count (CBC)
- Comprehensive metabolic panel (CMP) — kidney and liver function
- Hemoglobin A1C and fasting glucose — even if you've never been told you have diabetes
- Vitamin B12 and methylmalonic acid (MMA) — MMA catches deficiency the regular B12 test misses
- Thyroid-stimulating hormone (TSH)
- Serum protein electrophoresis (SPEP) — flags rare blood protein issues that cause neuropathy
- ANA — screens for autoimmune disease
That blood-work package can resolve the question of why in a surprising number of people. If your B12 is low and your symptoms started recently, replacement therapy may be the whole answer. If your A1C came back at 6.8 and you didn't know you were prediabetic, you've just discovered both the cause and the treatment target.
What your PCP cannot easily do is the deeper diagnostic work — confirming what type of neuropathy you have, where exactly in the nerve the damage sits, and whether anything more serious is hiding underneath. That's where the next layer of specialists comes in.
The Neurologist: The Diagnostic Quarterback
If you only see one specialist for neuropathy in your life, it should probably be a neurologist. They are the doctors trained specifically in disorders of the nervous system — central and peripheral, motor and sensory, common and rare. When a PCP says “I think you need to see someone,” nine times out of ten they mean a neurologist.

EMG and nerve conduction studies remain the single highest-yield diagnostic test for classifying peripheral neuropathy. The American Academy of Neurology lists them as the standard of care when the cause is unclear after initial blood work, and they are the test most likely to change the working diagnosis.
What a neurologist actually does for neuropathy patients is more interesting than most people expect. They don't just confirm what your PCP suspected. They classify the neuropathy along several axes:
- Which fibers are affected. Small-fiber neuropathy (burning, temperature changes, autonomic symptoms) versus large-fiber neuropathy (numbness, weakness, balance loss) require different testing and sometimes different treatments.
- Where the damage sits. Axonal damage (the nerve fiber itself) versus demyelinating damage (the insulating sheath around the nerve) point toward different causes — and demyelinating patterns can mean treatable autoimmune conditions like CIDP.
- The pattern of spread. Length-dependent neuropathy (starting in the toes and working up) suggests metabolic causes. Asymmetric or patchy patterns suggest something else entirely — vasculitis, compression, multifocal motor neuropathy.
- Motor versus sensory versus mixed. Pure motor neuropathies are rare and important to catch.
To do this classification, the neurologist typically orders an EMG (electromyography) and a nerve conduction study (NCS). These are the tests where they send small electrical impulses through your nerves and watch how the signals travel. It's uncomfortable but not awful — most people describe it as similar to repeated small static shocks — and the information it provides cannot be obtained any other way.
The reason this matters: two patients with identical-sounding symptoms can have very different underlying conditions, and treatment depends on knowing which one you have. A neurologist's classification is what unlocks the right next step.
When to Push for a Neuromuscular Specialist
Within neurology, there's a subspecialty called neuromuscular medicine. These doctors do all the things a general neurologist does, but they spend their entire careers on conditions of the nerves and muscles. If your case is complicated — rapidly progressive weakness, an inconclusive workup, a possible inherited condition, or a suspected autoimmune neuropathy like CIDP — a neuromuscular specialist is the higher-resolution camera. Academic medical centers and large neurology groups usually have one. Ask.
The Endocrinologist: When the Cause Is Metabolic
Roughly half of all peripheral neuropathy in the United States is caused by diabetes or prediabetes. That single statistic explains why endocrinologists end up so deeply involved in neuropathy care. They are not the doctors who treat the nerve damage directly — that role belongs to the neurologist and to your pain management team. They are the doctors who treat the cause.

of all peripheral neuropathy in the United States is caused by diabetes or prediabetes — which is why endocrinologists end up so deeply involved in neuropathy care.
If you have diabetes and your hemoglobin A1C is above 7%, you need to be working with an endocrinologist (or a primary care doctor experienced in advanced diabetes management). Tight blood-sugar control is the single most powerful intervention we have for slowing the progression of diabetic neuropathy. Newer tools — continuous glucose monitors that show time-in-range, GLP-1 medications that simultaneously improve glucose and protect against complications — have made this a far more nuanced field than it was a decade ago.
Endocrinologists also handle thyroid disease, severe B12 deficiency requiring injection, and the various pituitary and adrenal conditions that can occasionally show up as nerve damage. If your blood-work pointed toward a hormonal or metabolic cause, the endocrinologist is the specialist who fine-tunes the treatment.
The Podiatrist: The Foot Specialist Every Neuropathy Patient Needs
Podiatrists confuse a lot of neuropathy patients because their role overlaps with neurology in ways that aren't intuitive. Let me make this as simple as I can: a podiatrist is not the doctor who diagnoses or treats the underlying neuropathy itself. A podiatrist is the doctor who keeps your feet from being damaged because of neuropathy.
That distinction matters enormously. When sensation in your feet is reduced — even partially — small problems become invisible. A pebble in your shoe. A blister forming. A toenail growing inward. A callus thickening over a pressure point. A burn from a heating pad that wasn't as warm as you thought. Without the early-warning system of normal pain sensation, those small problems can quietly progress to wounds, infections, and (in worst cases) amputations.
A good podiatrist does several things for the neuropathy patient that no other specialist will:
- Quarterly or annual full-foot exams to catch problems you cannot feel
- Professional callus and corn management — you should never attempt to cut these yourself with reduced sensation
- Toenail trimming, especially if you cannot reach your feet easily or have thickened nails
- Custom diabetic shoe and insole prescriptions (often covered by Medicare for qualified patients)
- Early detection of Charcot foot — a serious complication where the bones in the foot collapse painlessly
- Ulcer treatment and wound care if a problem develops
If you have diabetic neuropathy or any neuropathy affecting your feet with significant numbness, an annual podiatrist visit is the minimum standard of care. Many patients with higher risk see one quarterly. It is one of those small habits that prevents large catastrophes.
The Pain Management Physician: When Medications Stop Being Enough
Most neuropathy pain is managed by a combination of your PCP, your neurologist, and a handful of standard medications — gabapentin, pregabalin, duloxetine, sometimes amitriptyline or nortriptyline, sometimes topical lidocaine or capsaicin. For about half of patients, that toolkit produces meaningful relief.

The 3-Step Routing Decision
For the other half, the journey is harder. After two or three medication trials at appropriate doses without adequate pain control, it is reasonable to ask for a referral to a pain management physician — sometimes called an interventional pain specialist or an anesthesiologist-pain doctor.
What pain management adds to your toolkit is mostly things the other specialists do not offer:
- Spinal cord stimulation — an implanted device that interrupts pain signals
- Dorsal root ganglion stimulation — newer, more targeted version of the above
- Nerve blocks and steroid injections for focal nerve pain
- Ketamine infusions in select cases
- Combination medication strategies that primary doctors are sometimes reluctant to try
- Comprehensive pain rehabilitation programs that combine medication, therapy, and behavioral work
A good pain management physician will not push you toward an implant or an opioid prescription on the first visit. They'll evaluate the whole picture and recommend the least invasive option that has a real chance of helping you.
The Rheumatologist: When the Immune System Is the Culprit
A surprising fraction of difficult-to-diagnose neuropathies turn out to be autoimmune in origin. Sjögren's syndrome can cause small-fiber neuropathy and burning feet. Lupus can attack peripheral nerves. Vasculitis — inflammation of small blood vessels — can produce asymmetric, painful, rapidly progressive neuropathy. Rheumatoid arthritis and other connective tissue diseases occasionally cause nerve damage as well.
If your initial workup hinted at autoimmune disease — a positive ANA, elevated inflammatory markers, dry eyes and dry mouth, a rash, joint swelling, or unexplained fevers — a rheumatologist is the specialist who untangles which condition you actually have. Their treatments often include immune-modulating drugs that, when they work, can stop the neuropathy from progressing further. This is one of those situations where finding the right specialist quickly can change the long-term outcome dramatically.
The Orthopedist or Physiatrist: For Compression and Mechanical Problems
Not every nerve problem is metabolic or autoimmune. Some are mechanical — a nerve compressed by a tight tunnel of tissue, a herniated disc pressing on a nerve root, a hand position causing chronic irritation at the wrist. Carpal tunnel syndrome at the wrist, ulnar nerve compression at the elbow, peroneal nerve compression at the knee, and lumbar radiculopathy from the spine all fall into this category.
For these, an orthopedic surgeon or a physiatrist (a doctor of physical medicine and rehabilitation) is often the right specialist. They evaluate whether the problem can be solved with splinting, bracing, physical therapy, and activity modification — or whether surgical decompression is the better path forward. Physiatrists in particular often serve as the bridge between diagnosis and rehabilitation, building exercise and recovery programs that other specialists don't have time to design.
Physical and Occupational Therapy: The Quiet Heroes
Physical therapists and occupational therapists are not technically doctors who diagnose or prescribe, but they are absolutely part of the team that treats neuropathy. A good physical therapist can teach you balance exercises that prevent the falls that derail so many people with foot numbness. They can build the leg strength that compensates for diminished proprioception. They can guide you through the gait retraining that turns shuffling back into walking.
An occupational therapist focuses on the hands and the daily activities — buttoning a shirt, opening a jar, using a keyboard, gripping a steering wheel — that hand neuropathy threatens. They are the people who introduce you to adaptive tools and reteach you techniques that work with your changed nervous system rather than against it.
Both can be accessed with a doctor's referral and are usually covered by insurance for a defined number of visits. If your specialist hasn't mentioned them, ask directly.
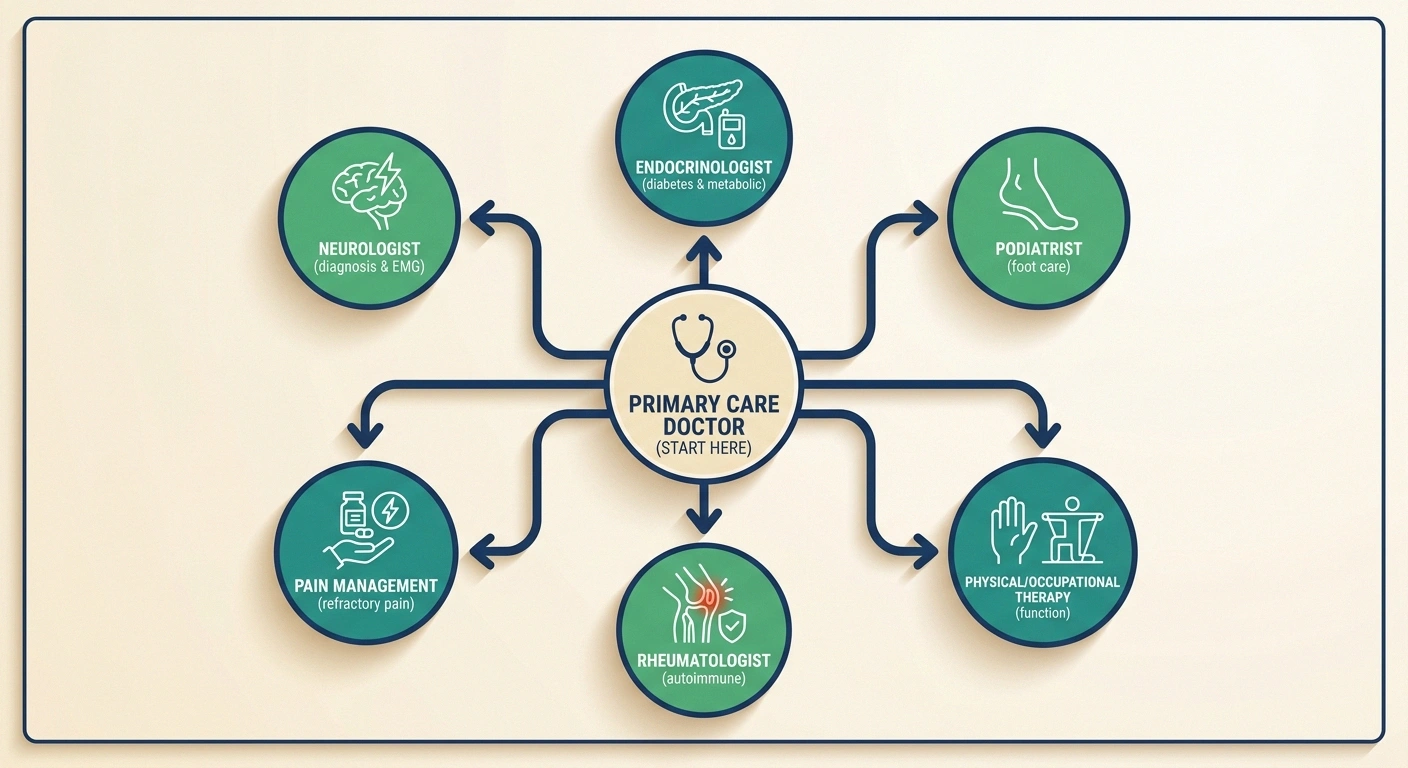
The Decision Tree: Who Do I See First?
Reading about every possible specialist is useful for context, but what most people want is a simple rule. Here's the routing logic I'd offer based on the most common presentations.

A few presentations need an emergency department immediately — not a specialist referral:
- Sudden rapidly progressive weakness over hours to days
- Weakness paired with loss of bowel or bladder control
- Sudden double vision, slurred speech, or facial drooping with weakness
- Foot infection with red streaking up the leg, fever, or any dead-looking tissue
- If you have new or recently developing numbness, tingling, burning, or weakness — see your primary care doctor first. Get the basic blood work. Most of the time this is the right starting point.
- If your PCP's blood work is mostly normal but symptoms continue — ask for a referral to a neurologist. They'll do the EMG and figure out what type of neuropathy you actually have.
- If you have diabetes or prediabetes — work with an endocrinologist (or a diabetes-focused PCP) on tight glucose control, see a podiatrist annually for foot care, and add a neurologist if symptoms are progressing despite good control.
- If your feet are noticeably numb regardless of cause — get a podiatrist in your rotation. Annual exam minimum. This is the highest-value low-cost step almost everyone skips.
- If medications aren't controlling pain after two or three honest trials — request a pain management referral.
- If your symptoms come with dry eyes, dry mouth, joint pain, rashes, or unusual fatigue — push for a rheumatologist evaluation.
- If your symptoms are concentrated in one area, one limb, or one hand — orthopedist or physiatrist for likely compression neuropathy.
When Symptoms Are an Emergency, Not a Specialist Referral
Most neuropathy develops slowly. But there are presentations that should go directly to an emergency room, not a specialist office:
- Sudden, rapidly progressive weakness over hours or days — possible Guillain-Barré syndrome
- Weakness paired with loss of bowel or bladder control — possible cauda equina syndrome
- Sudden double vision, slurred speech, or facial drooping along with new weakness — stroke until proven otherwise
- Severe sudden pain with a new skin rash spreading along a nerve distribution — possible severe shingles requiring urgent treatment
- Foot infection with redness streaking up the leg, fever, or any black/dead tissue — limb-threatening emergency
If any of these describe what you're experiencing, this article is not the right resource. Call 911 or get to an emergency department now.
Navigating Insurance and Referrals
The hardest part of this whole system isn't medical. It's logistical. A few practical notes that have saved me time and frustration over the years:

Always bring a one-page written summary of your symptoms, timeline, current medications, and any blood work results to a new specialist appointment. They will not have read your chart in advance. The patients who do best are the ones who help the doctor get up to speed in the first five minutes.
- Most HMO and some PPO plans require a PCP referral before a specialist visit will be covered. Make sure that referral is in place before you book.
- Neurologist wait times in many parts of the country run six to twelve weeks. Get on the schedule the day your PCP recommends one. You can always cancel.
- Medicare covers neurology, endocrinology, podiatry, pain management, rheumatology, and orthopedics with appropriate referral. Diabetic foot care has specific coverage rules — ask your podiatrist's billing office.
- If you're uninsured, community health centers can usually serve as your PCP and have referral relationships with specialists who accept sliding-scale fees.
- Always bring a one-page written summary of your symptoms, timeline, current medications, and any blood-work results to a new specialist appointment. They will not have read your chart in advance. The patients who do best are the ones who help the doctor get up to speed in the first five minutes.
Building Your Team, One Door at a Time
When I look back at the question I asked my primary care doctor that day — who actually treats this? — I realize the honest answer is: you do, with help. You are the only person who sees every appointment, who knows every symptom, who notices every change. The specialists each see a slice of the picture. Your job is to assemble that picture and make sure the right slices are talking to each other.
A typical neuropathy patient's team, over time, ends up looking like this: a primary care doctor as the coordinator, a neurologist for the diagnostic and ongoing nerve picture, an endocrinologist if metabolic causes are involved, a podiatrist as the standing line of defense for foot health, a physical therapist when balance or strength need work, and one or two others added as needs evolve. You don't build this team overnight. You build it one referral, one appointment, one phone call at a time.
Start where you are. Call your primary care doctor this week. Ask for the blood work. Ask the question that's bothering you. The maze is real, but there is a way through it, and the first door is almost always the closest one.
Frequently Asked Questions
Should I see a neurologist or a podiatrist for neuropathy in my feet?
You probably need both, but in different roles. The neurologist diagnoses what type of neuropathy you have and treats the underlying nerve condition. The podiatrist protects your feet from the complications that come with reduced sensation — checking for sores you cannot feel, managing calluses safely, prescribing diabetic shoes, and catching problems like Charcot foot early. If you can only pick one to start with, see the neurologist for diagnosis; once you have a diagnosis, add the podiatrist for ongoing foot care.
Can my regular doctor treat neuropathy or do I have to see a specialist?
Many cases of neuropathy can be diagnosed and treated by a primary care doctor, especially when the cause is a vitamin deficiency, diabetes, thyroid disease, or medication side effect. The PCP can order the necessary blood work, prescribe replacement therapy or first-line nerve pain medications, and coordinate care. A specialist becomes necessary when the cause is unclear, symptoms are progressing despite treatment, or the picture suggests something more complex.
What is the difference between a neurologist and a neuromuscular specialist?
A neurologist is trained in all disorders of the nervous system, from migraines to strokes to neuropathy. A neuromuscular specialist is a neurologist who completed additional fellowship training specifically in conditions affecting nerves and muscles. For straightforward neuropathy, a general neurologist is usually enough. For complicated cases — rapidly progressive symptoms, suspected hereditary neuropathy, possible autoimmune neuropathy like CIDP, or any case where the diagnosis is unclear after initial workup — a neuromuscular specialist's deeper expertise pays off.
When should I see an endocrinologist for neuropathy?
See an endocrinologist when the cause of your neuropathy is metabolic. Most commonly this means diabetes that isn't well controlled, prediabetes that's already producing nerve symptoms, severe vitamin B12 deficiency that needs more than oral supplementation, or thyroid disease. Endocrinologists treat the cause, not the nerve damage itself, but addressing the cause is often the most powerful thing you can do to slow or stop progression.
How long should I wait for a neurology referral?
Neurology wait times in many parts of the United States run six to twelve weeks for non-urgent appointments. If your PCP marks the referral as urgent — for rapidly progressing weakness, suspected serious underlying condition, or significant functional impairment — many practices will see you sooner. Get on the schedule the day your PCP makes the referral. If a much earlier slot opens up at a different practice, you can take it and cancel the original.
Do I need a referral to see a podiatrist?
For most insurance plans, you do not need a referral to see a podiatrist for routine foot care. Medicare covers a podiatrist visit every nine weeks for diabetic patients with documented neuropathy and loss of protective sensation, no referral required, as part of its diabetic foot care benefit. Check your specific plan; if a referral is needed, your PCP can usually provide one with a phone call.
What if my neurologist cannot figure out what is causing my neuropathy?
Up to 30% of peripheral neuropathies are classified as idiopathic, meaning no clear cause is found even after thorough workup. If your general neurologist has not identified a cause, the next steps to consider are: a referral to a neuromuscular subspecialist at an academic medical center, a skin punch biopsy to test for small-fiber neuropathy, and a second opinion at a different institution. Sometimes a fresh set of eyes catches what was missed the first time.
Should I see a pain management doctor right away if my neuropathy hurts?
Usually no, not right away. Start with your PCP or neurologist for a trial of first-line nerve pain medications like gabapentin, pregabalin, or duloxetine. These are well-studied for neuropathic pain and most general doctors are comfortable prescribing them. Pain management specialists add value when first-line medications have not worked at adequate doses, when interventional options like spinal cord stimulation are being considered, or when the pain is significantly affecting your function despite multiple treatment attempts.


