
When a member of our online community wrote in last spring describing his husband's sudden, severe right-thigh pain, twenty-pound weight loss over six weeks, and growing difficulty climbing stairs, the family had already been through four doctors and three working diagnoses. Hip arthritis. Lumbar disc problem. Possible cancer. Each visit added more uncertainty and more fear. By the time someone finally said the words “diabetic amyotrophy,” the husband had been in pain for nearly three months without a clear name for what was happening to him.
That story is far more common than it should be. Diabetic amyotrophy — a rare but distinctive type of diabetes-related nerve damage — is one of those conditions that almost nobody outside neurology hears about until they have it. It doesn't look like the classic “tingling toes” neuropathy most of us picture when we hear the word. It hits the wrong leg, in the wrong place, at the wrong tempo, and it brings weight loss that triggers cancer fears in everyone involved.
I'm Janet, and I write about neuropathy as a patient advocate, not a doctor. What I want to do in this article is walk you through diabetic amyotrophy in plain English — what it is, how it shows up, why it's so often missed, what doctors actually do about it, and what realistic recovery looks like. If you or someone you love is in the middle of this confusing picture right now, my hope is that you finish this page with names for things you've been feeling and questions you can take to your next appointment.
What Diabetic Amyotrophy Actually Is
The medical name your neurologist is most likely to use is diabetic lumbosacral radiculoplexus neuropathy, often shortened to DLRPN. Older texts call it Bruns-Garland syndrome after the two physicians who described it. You may also hear “proximal diabetic neuropathy” or just “diabetic amyotrophy.” All of these refer to the same condition.
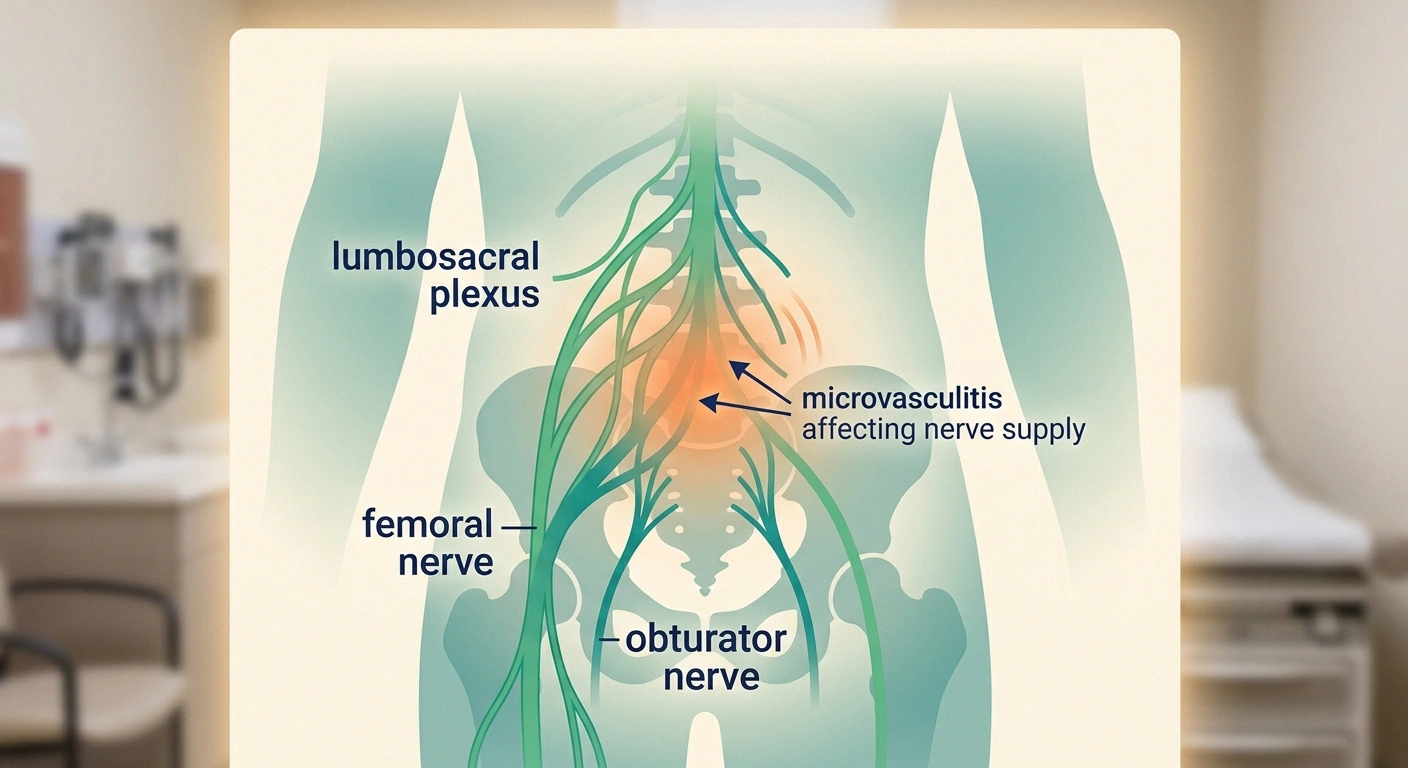
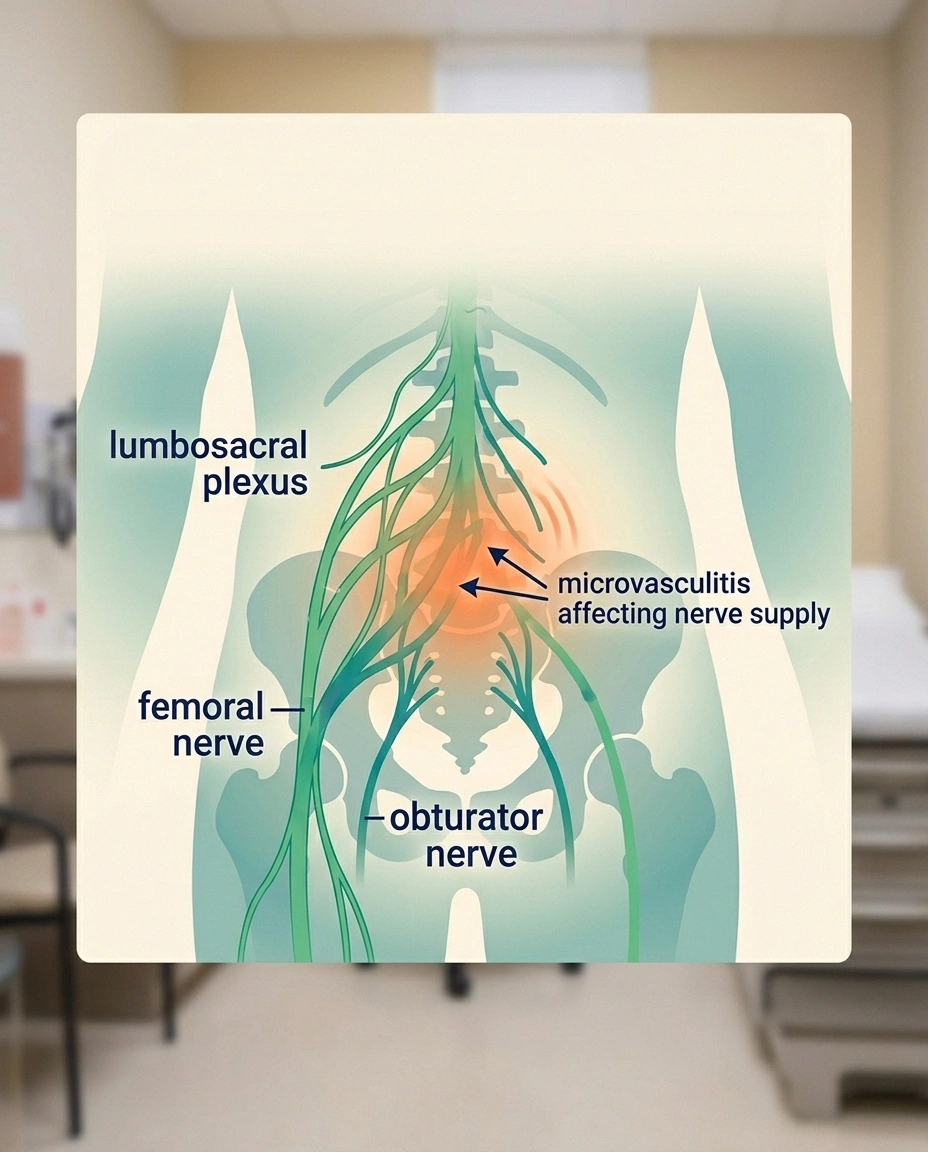
Diabetic amyotrophy is not the same as standard diabetic peripheral neuropathy. It involves inflammation of small blood vessels feeding the nerve plexus — a microvasculitis — which is why it presents suddenly, asymmetrically, and often in patients with relatively good glucose control.
The “amyotrophy” part of the name comes from two Greek roots that together mean “lack of muscle nourishment.” That's exactly what you see: the muscles in the affected thigh, hip, and sometimes calf start to waste visibly as the nerve damage progresses. The “lumbosacral radiculoplexus” part is the medical map of the affected territory — the lumbar nerve roots, the sacral nerve roots, and the network where they bundle together before traveling down the leg. Damage to that network is what produces the pattern of symptoms.
What makes diabetic amyotrophy genuinely different from the more common kinds of diabetic neuropathy is the underlying mechanism. Standard diabetic peripheral neuropathy is mostly a slow metabolic injury to the longest nerves in the body — toes first, then feet, then gradually upward over years. Diabetic amyotrophy is different. The current evidence points toward an inflammatory injury to the small blood vessels feeding the lumbosacral nerve network — a microvasculitis. The nerves are damaged not directly by sugar, but by inflammation in the vessels supplying them.
That distinction matters because it explains many of the confusing features: the sudden onset, the asymmetry, the eventual partial recovery, and the response to treatments that target inflammation rather than just glucose.
The Classic Three-Part Story
If you ask a neuromuscular specialist to describe the classic presentation of diabetic amyotrophy, they will tell you a three-part story that unfolds over weeks to months. Almost every patient hits at least two of the three parts in roughly the same order.
Approximately half of diabetic amyotrophy patients eventually develop similar symptoms in the opposite leg — typically less severe than the first side, starting weeks to months later. This bilateral involvement is part of the natural history of the condition, not a separate recurrence.
Part one: severe, deep, one-sided pain. It usually begins in a hip, a buttock, the front or side of a thigh, or — less commonly — the lower back. Patients describe it as deep, burning, aching, or stabbing. It is almost always far worse than ordinary muscle soreness. It is typically worst at night. It frequently wakes people from sleep. The pain comes on relatively suddenly, often over days rather than months. Many patients can name the week it started.
Part two: progressive weakness in the same leg. Within two to four weeks of the pain starting, weakness develops in the same area. The muscles most often affected are the quadriceps (thigh muscles for straightening the knee), the iliopsoas (hip flexor for lifting the leg), and the hip abductors. Functionally, this looks like difficulty climbing stairs, trouble standing up from a chair without using the arms, and a tendency for the affected knee to buckle. Some patients describe their leg as feeling “heavy” or “weak from the inside.” Visible muscle wasting often follows.
Part three: substantial unintentional weight loss. This is the symptom that throws everyone off the trail. Most patients with active diabetic amyotrophy lose ten to thirty pounds over a few weeks without trying. Some lose more. The combination of severe pain, reduced appetite, increased metabolic demand, and disrupted sleep adds up to weight loss that looks alarming. Many patients undergo extensive cancer evaluations during this stage. Those workups are appropriate — you have to rule out the dangerous things — but the weight loss in diabetic amyotrophy is a consequence of the syndrome itself, not a separate problem.
About half of patients eventually develop similar symptoms on the opposite side — typically less severe, typically starting weeks or months after the first side. The full picture, once it has declared itself, can include numbness or burning in the leg, exaggerated knee or ankle reflexes loss, and sometimes a feeling that the front of the thigh has become numb to touch.
Who Gets It, and Why
One of the most counterintuitive things about diabetic amyotrophy is who gets it. The typical patient is not someone with badly controlled long-standing diabetes. The typical patient is a type 2 diabetic over the age of fifty, often with reasonable or even excellent glucose control, sometimes recently diagnosed. Men are affected slightly more often than women, though the difference is small.
Unintentional weight loss typical during the active phase of diabetic amyotrophy. This pattern triggers cancer fears in nearly every family, but the weight loss is a consequence of the syndrome itself — and reverses naturally as pain resolves.
Some patients had been told their diabetes was well managed and were stunned to develop something so disabling without warning. Others had A1C levels that were dropping fast — for example, after starting a new medication or losing significant weight — which appears to be one of the triggers in some cases. A few patients develop diabetic amyotrophy at the same time their type 2 diabetes is first diagnosed; the nerve syndrome and the diabetes diagnosis show up almost simultaneously.
What does not seem to predict it well is duration of diabetes, traditional measures of glucose control, or the presence of other complications. This is part of why it surprises everyone, including the patient, when it arrives.
Why It Gets Missed for So Long
I want to spend a few paragraphs here because the pattern of misdiagnosis is so consistent across the patient stories I've read and heard. Knowing what diabetic amyotrophy is commonly mistaken for can help you push past the wrong working diagnosis faster.
Hip osteoarthritis. The pain is deep, one-sided, and gets worse with use. Many patients are sent first for hip X-rays. If the X-rays show any wear-and-tear changes (and most older adults' hips do), the picture seems to fit. The problem: hip arthritis pain doesn't usually wake people from sleep at night with severe burning, doesn't typically produce significant weight loss, and doesn't cause measurable weakness above and beyond what pain-related guarding produces.
Lumbar radiculopathy from a herniated disc. A pinched nerve in the back can produce one-sided leg pain and weakness, so an MRI is often the next test. The trouble is that older adults frequently have some degree of degenerative spine changes on MRI without any actual nerve compression at all. A “positive” MRI gets blamed for symptoms that are actually coming from a completely different process.
Cancer. The unintentional weight loss, in someone over fifty, with severe pain, makes everyone in the room think of cancer. This is a reasonable concern that has to be ruled out. CT scans, blood markers, and sometimes PET scans get ordered. When they come back negative, the patient is left feeling validated about the seriousness of the symptoms but still without an answer.
Femoral neuropathy from another cause. The femoral nerve runs to the front of the thigh and the quadriceps. Compression of that nerve — from a hip injection, a hematoma after a procedure, prolonged hip flexion during surgery, or rarely an abdominal mass — can mimic part of the picture. The difference: isolated femoral neuropathy doesn't usually come with severe burning night pain, weight loss, or eventual bilateral involvement.
Depression or psychogenic pain. This is the one that hurts the most. Patients who have been through several specialists, whose imaging looks unimpressive, whose pain remains severe, are sometimes told the problem is anxiety or depression. While chronic pain absolutely affects mood, the underlying nerve damage in diabetic amyotrophy is real and measurable. The test that actually settles the question is an EMG and nerve conduction study.
How the Diagnosis Gets Made
The diagnosis of diabetic amyotrophy is ultimately clinical — meaning it rests on the doctor recognizing the pattern of symptoms in someone with diabetes — and supported by a few specific tests. There is no single blood test that says “yes” or “no.”

The Diagnostic Pathway
The test that contributes the most diagnostic information is the EMG and nerve conduction study, performed by a neurologist. In diabetic amyotrophy, the EMG typically shows asymmetric damage to the lumbosacral plexus with evidence of denervation in multiple muscles supplied by different nerve roots on the affected side. The pattern is distinctive enough that a neuromuscular specialist can often recognize it on the day of the test.
An MRI of the lumbar spine is commonly done to rule out structural causes — a herniated disc compressing nerves, a tumor in the spinal canal, a spinal infection. In diabetic amyotrophy itself, the lumbar MRI is usually relatively normal or shows only age-appropriate changes. Some specialized MRI protocols can show inflammation along the affected nerves, but this isn't always available.
Some neurologists obtain a spinal fluid sample, which often shows elevated protein levels — a nonspecific marker of nerve inflammation that helps support the diagnosis when the picture is otherwise unclear. Blood work is run to rule out other inflammatory neuropathies, vitamin deficiencies, and rarer causes.
Once the diagnosis is reasonably confident, the question shifts from “what is this?” to “what do we do?”
Treatment While the Storm Is Active
Treatment of active diabetic amyotrophy is largely supportive. There is no medication that has been definitively proven to stop the underlying nerve damage or shorten the course of the illness. What treatment does, and does well, is help you survive the active phase with as little permanent damage as possible.
Pain control is the first priority. Most neurologists start with one of the medications used for nerve pain in general: gabapentin or pregabalin (which target the same receptor and overlap in benefit), duloxetine (which addresses both nerve pain and the depression that frequently accompanies it), or sometimes amitriptyline or nortriptyline. Topical lidocaine patches and capsaicin cream can supplement systemic medications. Some patients need short courses of stronger pain medicines including, occasionally, opioids — used briefly, under close supervision, with a clear plan to transition off once the pain peaks have passed.
Glucose control matters but should not be aggressive. There is a complication called treatment-induced neuropathy that can develop when blood sugar is lowered too rapidly. The general principle in diabetic amyotrophy is to aim for steady, moderate glucose control rather than rushing toward perfect numbers. Working with an endocrinologist or a primary care doctor experienced in advanced diabetes care is helpful here.
Immune-modifying therapy is controversial. Because the underlying problem appears to be inflammatory, some specialists try intravenous immunoglobulin (IVIG) or high-dose corticosteroids during the active phase. The evidence supporting these treatments is mixed; large randomized trials have not consistently shown that they shorten the course of the illness. Some patients seem to benefit, especially when treated early in severe cases. The decision is individualized and should be made with a neuromuscular specialist.
Physical therapy starts during pain, intensifies during recovery. Even when the active pain is significant, gentle range-of-motion work helps prevent the joint stiffness and muscle contracture that can develop when an affected leg is favored. As pain begins to subside and weakness becomes the dominant issue, physical therapy moves toward graduated strengthening, balance training, and gait retraining. This phase often lasts many months.
Nutrition and weight regain follow pain control. Most patients begin to regain lost weight naturally once pain subsides and appetite returns. There's no special diet that speeds nerve recovery, but adequate protein and overall calorie intake matter during the rebuilding phase. Talk with your care team if appetite stays poor or weight loss continues despite improved pain.
What Recovery Actually Looks Like
Here is the part of the story I want most to deliver clearly, because it is the part patients are starving to hear in the dark middle of the illness: most people with diabetic amyotrophy recover significant function. The condition is not progressive in the way that the worst-feared neurological diseases are progressive. There is a long active phase, then a long recovery phase, and the typical trajectory bends back toward something resembling normal.
The active phase — the time when new symptoms are still developing — usually lasts six to eighteen months. During that window, the pain may shift, the weakness may spread, and the contralateral leg may become involved. This stretch is exhausting for everyone in the family and worth being honest about with yourself and your support people. It is not a one-month thing. Plan accordingly.
The recovery phase begins as the pain starts to fade and the weakness begins to plateau. From there, strength usually returns gradually over twelve to twenty-four months. Most patients regain functional use of the affected leg, though not always to the level they had before the illness. Mild persistent weakness in the quadriceps is common. Some patients walk with a slight limp permanently. A handful continue to need a cane or walker for distance. The minority — usually those with the most severe initial damage or other complicating conditions — have more lasting limitations.
The weight you lost during the active phase usually comes back as appetite returns. Some patients are happy about the weight loss and want to keep it off; if you are one of them, this is a conversation worth having with your doctor, because intentional further weight loss during recovery can stall nerve repair if it's too aggressive.
Recurrence in the same leg is uncommon. Recurrence in the opposite leg, as mentioned earlier, happens in roughly half of patients, but usually within the first year and usually less severely.
Practical Survival Strategies for the Active Phase
Beyond the medical treatments your specialists will guide, there are practical strategies that make the active phase more livable. These are the things patient families have shared with me over the years.

A few signs are not diabetic amyotrophy and need emergency evaluation:
- Loss of bowel or bladder control with leg weakness — possible cauda equina syndrome
- Rapid progression in hours rather than weeks — possible spinal cord process
- Fever with severe back pain — possible epidural abscess
- Stroke-like sudden weakness — call 911
- Get a cane, walker, or rollator early, even if you feel like you don't need one yet. Reduced sensation and weakness combine to make falls likely. A walker beside the bed for nighttime bathroom trips can prevent a much worse outcome.
- Move your sleeping arrangement to a single floor if you can. Stairs become genuinely difficult during the weakness phase.
- Set up a comfortable recliner as command central during the most pain-heavy weeks. Many patients find that a slightly reclined position takes pressure off the hip and reduces nighttime awakening.
- Plan for help with bathing, dressing, and getting up from low surfaces during the worst weeks. This is not a sign of failure; it's a sign of injury, and injuries require support during healing.
- Tell your support people what's actually happening. The instinct to minimize (“I'm fine, just a bit of leg pain”) leaves the people who could help you guessing. Honest communication preserves relationships during long illnesses.
- Track your pain on a daily 0-10 scale in a simple notebook. The trend matters more than any single day. Slow improvement is real even when day-to-day variation is large.
- Take care of your mental health proactively. Severe chronic pain and the loss of physical capability are powerful depressogenic forces. Antidepressants, therapy, or support groups for chronic illness are not optional luxuries during this phase.
Symptoms That Are Not Diabetic Amyotrophy and Need Emergency Evaluation
Diabetic amyotrophy develops over days to weeks, not over hours. Certain symptom patterns are not diabetic amyotrophy and need urgent evaluation in an emergency department, not a routine specialist appointment:
- Loss of bowel or bladder control with leg weakness — possible cauda equina syndrome, a surgical emergency
- Rapidly progressive weakness in hours rather than weeks — possible spinal cord process
- Fever, severe back pain, and progressive neurological symptoms — possible epidural abscess
- New severe back pain in someone with a history of cancer — possible vertebral metastasis
- Acute weakness with stroke-like onset — call 911
If any of these apply to what you're experiencing, this article is the wrong resource. Get emergency care now.
Carrying the Diagnosis Forward
When the community member I mentioned at the start finally received the diabetic amyotrophy diagnosis, the strangest part was how much relief came with it. Not because the condition was easy — it wasn't, and the recovery took most of two years — but because finally there was a name, an explanation, and an expected trajectory. The fear of cancer faded. The frustration of being passed between specialists eased. The family could plan: rough months ahead, gradual recovery, probable significant return of function, occasional residual weakness.

The active phase typically lasts six to eighteen months, followed by twelve to twenty-four months of gradual recovery. Most patients regain significant function. Some residual weakness is common, but the trajectory bends back toward something resembling normal for the majority.
If you or someone you love is in the middle of an unexplained picture of one-sided thigh pain, weight loss, and growing weakness — and there is diabetes in the picture, even recently diagnosed or mildly controlled diabetes — ask your doctor specifically about diabetic amyotrophy. Ask for an EMG and nerve conduction study with a neurologist familiar with neuromuscular disease. Ask the question that breaks the cycle of “we don't know what this is” and starts the cycle of “now we know, here's the plan.”
It is a hard condition to live through. It is a rewarding condition to recover from. And you are not alone in either part.
Frequently Asked Questions
Is diabetic amyotrophy reversible?
For most patients, yes — at least partially. The active phase of pain and progressive weakness usually peaks within six to eighteen months, followed by gradual recovery over another twelve to twenty-four months. Most patients regain significant function of the affected leg, though some residual weakness is common. Complete return to pre-illness strength happens in a minority of cases. The trajectory bends back toward normal but not always all the way.
How long does diabetic amyotrophy last?
The active phase, during which new symptoms develop, generally lasts six to eighteen months. The recovery phase, during which strength gradually returns, often lasts another twelve to twenty-four months. From first symptom to maximum recovery is therefore typically two to three years for most patients. Some recover faster, some take longer. Permanent residual weakness, when it occurs, becomes apparent in the second year.
What is the difference between diabetic amyotrophy and regular diabetic neuropathy?
Regular diabetic peripheral neuropathy is a slow, symmetric, distance-dependent nerve injury that starts in the toes and gradually progresses upward over years. Diabetic amyotrophy is sudden, asymmetric, and proximal — it affects one thigh, hip, or upper leg first, comes with severe pain and significant weight loss, and is thought to involve inflammation of small blood vessels rather than purely metabolic injury. The two conditions can coexist in the same patient.
Can you get diabetic amyotrophy if your diabetes is well controlled?
Yes. Surprisingly, the typical patient with diabetic amyotrophy is a type 2 diabetic over fifty with relatively good or only mildly elevated glucose control. Some patients are newly diagnosed. Some had A1C levels dropping quickly because of a new medication or weight loss. Long-standing poor control is not the typical setup. This is part of why the diagnosis is so often missed initially.
Why does diabetic amyotrophy cause weight loss?
The weight loss has several contributors. Severe chronic pain suppresses appetite. Disrupted sleep elevates stress hormones that affect metabolism. The systemic inflammation involved in the underlying microvasculitis appears to increase energy expenditure. The combination produces the characteristic ten- to thirty-pound unintentional weight loss seen in most patients during the active phase. Weight typically returns as pain resolves and appetite recovers, though the process takes months.
What kind of doctor diagnoses diabetic amyotrophy?
A neurologist is usually the specialist who makes the diagnosis, and a neuromuscular subspecialist if your case is complicated or initial workup is inconclusive. The diagnosis depends on recognizing the clinical pattern, performing an EMG and nerve conduction study, and ruling out other causes of the symptoms with appropriate imaging and blood work. Your primary care doctor is the right starting point for the referral.
Will steroids or IVIG cure diabetic amyotrophy?
Probably not cure, but they may help in selected cases. Because the underlying problem involves inflammation, some neuromuscular specialists try high-dose corticosteroids or intravenous immunoglobulin (IVIG) during the active phase. The supporting evidence is mixed, with most controlled trials failing to show large benefits across all patients. Individual patients sometimes appear to respond well. The decision should be made with a neuromuscular specialist who can weigh the potential benefits against the real side effects of these treatments in your specific situation.
Can diabetic amyotrophy happen again on the other side?
Yes, in roughly half of patients. The opposite leg typically becomes involved within months of the first side, usually less severely. The pattern is so common that most neuromuscular specialists consider it part of the natural history of the condition rather than a separate recurrence. Bilateral involvement does not typically worsen the long-term prognosis. True later recurrences, years after recovery, are uncommon.


