If you wear dentures and use a tube of denture cream a week, there's a quiet possibility almost nobody talks about: that adhesive could be slowly damaging your nervous system. Not through anything that sounds toxic — through the zinc inside it, which blocks your body from absorbing copper. And copper deficiency causes a kind of nerve damage that looks almost exactly like the kind doctors usually blame on something else entirely: vitamin B12.
Most people with this condition don't wear dentures, though. Some had weight-loss surgery a decade ago. Some have been taking a daily zinc supplement for their immune system since 2020. Some have undiagnosed celiac disease. What they share is a deficiency almost no one tests for — until they're walking with a cane and have already lost function that may not fully come back.
I'd never heard of copper deficiency neuropathy either until I started digging through the research on conditions that mimic the more familiar B12 deficiency. What I found was a real, documented, treatable cause of neuropathy that gets routinely missed — and that costs people permanent neurologic function when the diagnosis arrives late.
This article walks you through what it is, what causes it, why it gets missed, what testing actually looks like, and what to ask your doctor. Like everything I write here, it's information — not a diagnosis. If anything I describe sounds like what you're experiencing, the next step is a conversation with a clinician, not a self-conclusion.
What Copper Deficiency Neuropathy Actually Is
Copper is a trace mineral your body needs in tiny amounts but cannot function without. Among many other jobs, copper is essential for maintaining the myelin sheath — the insulating layer wrapped around nerve fibers that lets nerve signals travel quickly and cleanly. It also plays a role in iron metabolism, immune function, and the formation of red and white blood cells.
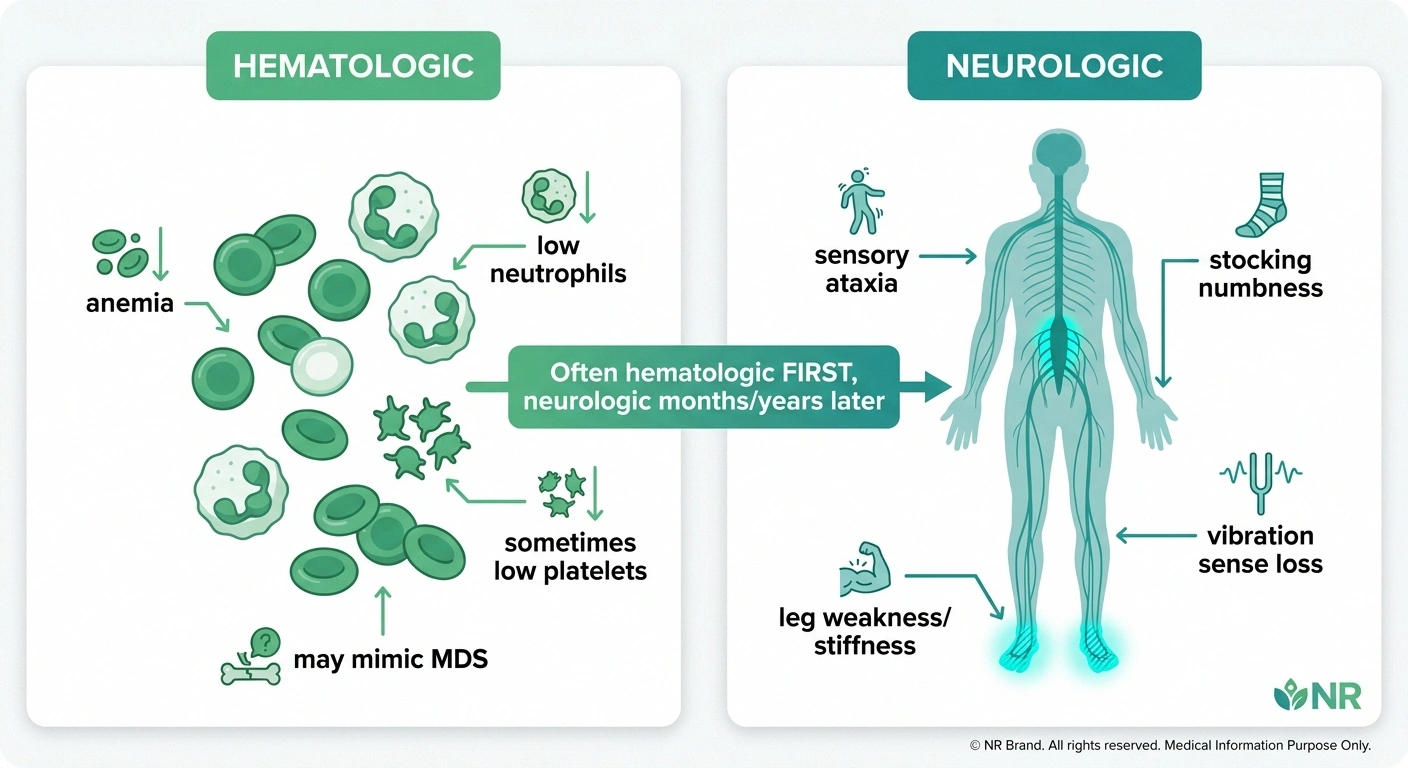
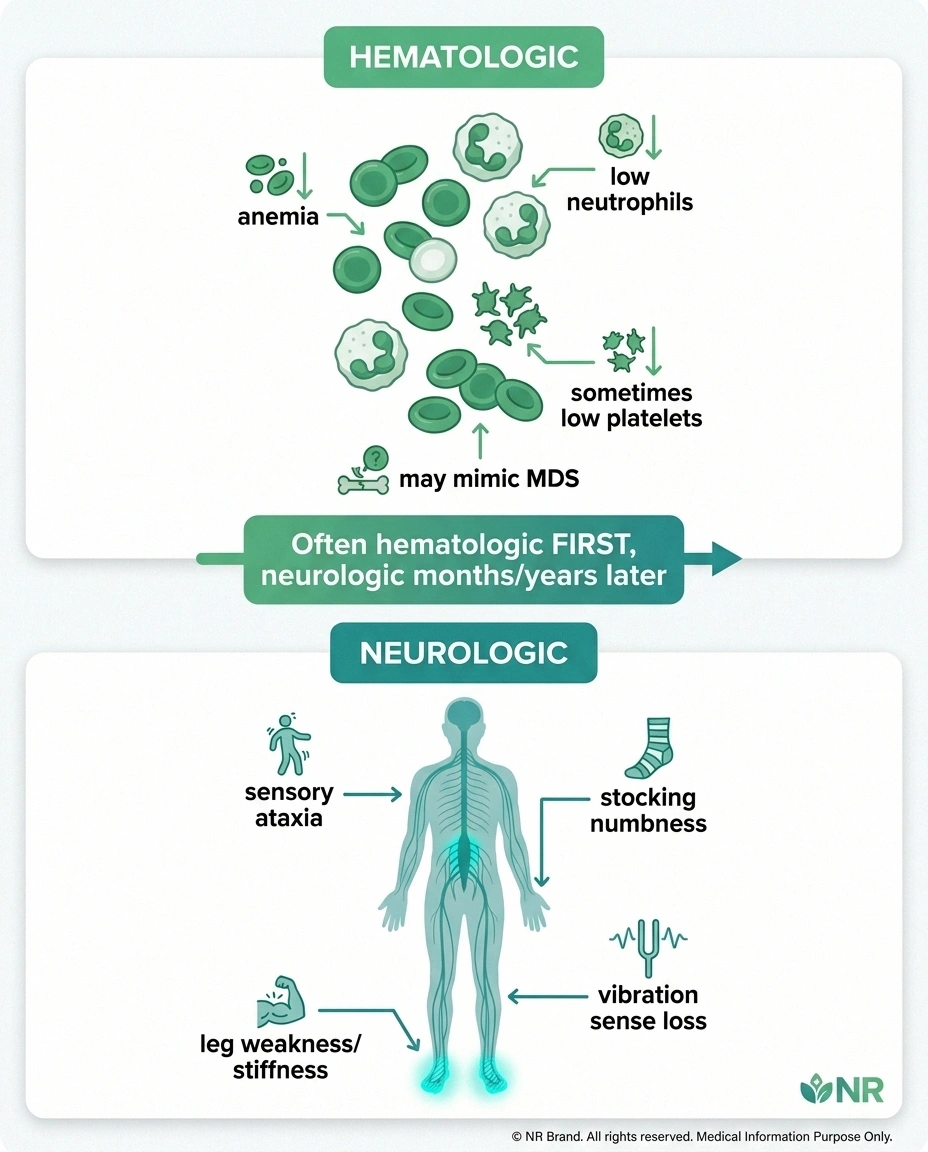
When the body runs out of copper, two things start to go wrong at the same time. The first is hematologic — anemia (often unexplained), low white blood cell counts (especially neutrophils), and bone marrow changes that can mimic a serious blood cancer called myelodysplastic syndrome. The second is neurologic — damage to the spinal cord and peripheral nerves that produces a specific pattern of symptoms doctors call “myeloneuropathy.”
This neurologic picture is so identical to the subacute combined degeneration caused by vitamin B12 deficiency that the conditions look the same on MRI, present with the same symptoms, and even produce similar lab work outside of the actual copper and B12 levels. The first researchers to describe this in detail — Neeraj Kumar and colleagues at Mayo Clinic, starting in the early 2000s — borrowed a term from veterinary medicine to describe it: “human swayback,” after the syndrome that develops in copper-deficient sheep and cattle.
The disease is rare, but it is increasingly recognized. The reason it matters out of proportion to its rarity is that, unlike many causes of neuropathy, copper deficiency is treatable — and the longer it goes undiagnosed, the less of the damage will reverse.
What It Feels Like: The Clinical Picture
Copper deficiency myeloneuropathy usually develops over months rather than days. The most common pattern looks like this:
Loss of balance and an unsteady gait. This is often the first complaint that brings people in. The floor feels unreliable. Walking in the dark, or in a dark room, is suddenly much harder than it used to be. People describe feeling like the ground is moving underneath them, or like they're walking on a mattress. A doctor checking for this might do a Romberg test — asking you to stand with your feet together and close your eyes. Falling or swaying badly is a clue that the dorsal columns of the spinal cord (which carry position-sense information) are involved.
Numbness and tingling in the feet, often spreading. This part feels like classic peripheral neuropathy — stocking-pattern paresthesias, pins-and-needles, that “walking on cotton” feeling. It often starts in the feet and gradually involves the hands. For more on this pattern in general, our overview of what neuropathy feels like describes the sensations many readers recognize.
Leg weakness and stiffness. Because the corticospinal tracts can be involved too, people may notice their legs feel heavy, stiff, or weak. Reflexes are often brisker than expected, and a doctor may find a Babinski sign on exam — the toes fanning upward instead of curling down when the sole is stroked.
Loss of vibration and position sense. A tuning fork held to the bony parts of the ankle or toe should feel like a clear hum. In copper deficiency myeloneuropathy, that vibration is often dramatically reduced or absent. The same goes for joint-position sense — being able to tell, with your eyes closed, whether a doctor is bending your toe up or down.
Bladder and bowel changes can appear in more advanced cases.
Vision problems are rare but documented — an optic neuropathy can develop, especially in patients who became copper deficient after bariatric surgery.
On the blood side — and this part often comes first, sometimes by months or years before the neurologic symptoms catch up — copper-deficient patients commonly show up with unexplained anemia, low neutrophil counts, occasionally low platelets, and sometimes a bone marrow picture that prompts a hematology referral for suspected myelodysplastic syndrome. The bone marrow may show ring sideroblasts and vacuolated red and white cell precursors. A normal karyotype is one of the clues that copper deficiency, not actual MDS, is the cause — but you have to be looking for it.
Why This Diagnosis Gets Missed
Here's the painful truth: by the time most patients are diagnosed with copper deficiency myeloneuropathy, they have already been through months or years of testing for something else. The clinical picture screams “B12 deficiency” — so the workup tests B12. When B12 comes back normal (or even when it's low and supplementation doesn't fix the symptoms), many workups stall. Copper is not a routine part of the standard neuropathy panel at most labs.
Other common misdiagnoses include multiple sclerosis (because the spinal cord MRI looks similar), idiopathic neuropathy, chemotherapy-related neuropathy in cancer survivors, paraneoplastic syndrome, and chronic inflammatory demyelinating polyneuropathy.
On the blood side, patients are sometimes referred for evaluation of suspected MDS — a serious diagnosis that can lead to bone marrow biopsy, complex genetic testing, and even discussion of stem cell transplant — without anyone testing copper. There are published cases of patients being worked up for transplant for what turned out to be a copper deficiency that resolved with supplementation.
The diagnosis hides in plain sight because three simple, cheap blood tests — serum copper, ceruloplasmin, and serum zinc — are not part of the default neuropathy or anemia panels. You have to ask for them by name. That is the single most actionable thing in this article.
The Causes — Ranked by How Often They Actually Cause This
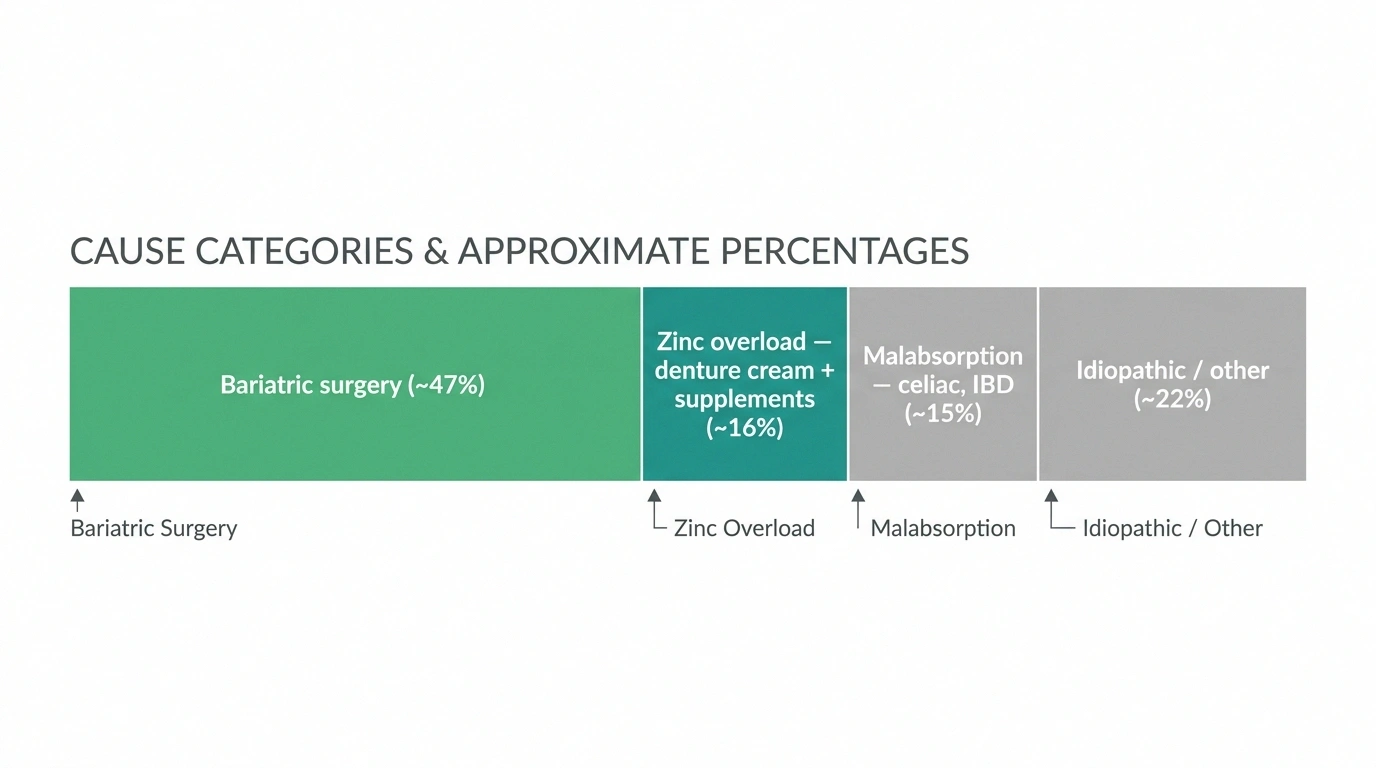
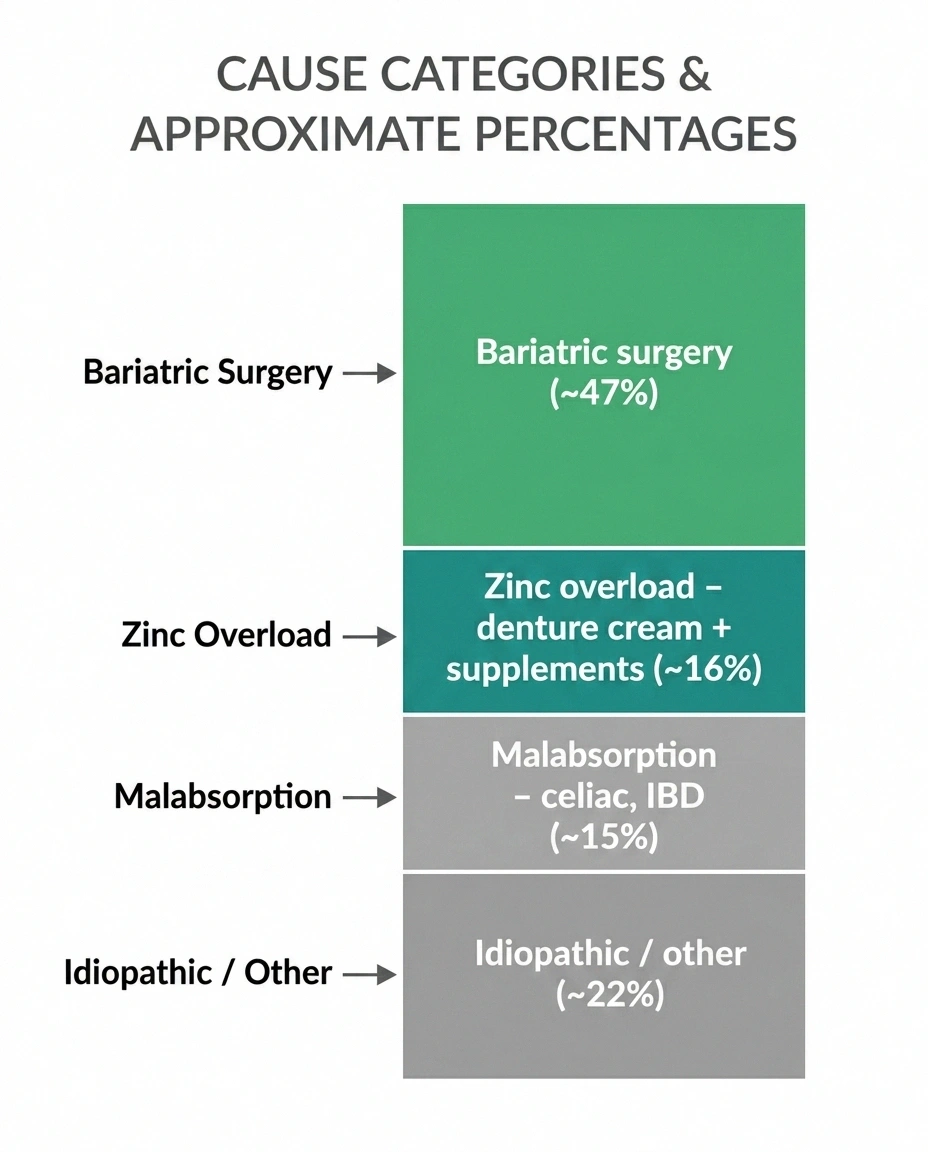
Across published case series, the most common causes break down roughly like this: previous upper gastrointestinal surgery accounts for about 47 percent of cases, excess zinc exposure for about 16 percent, malabsorption syndromes for about 15 percent, and the remainder are idiopathic or attributable to less common causes. Let's go through them.
Bariatric Surgery (Especially Roux-en-Y Gastric Bypass)
Copper is absorbed in the stomach and the upper part of the small intestine — the exact stretch of digestive tract that Roux-en-Y gastric bypass surgery routes food around. Estimates suggest that without prophylactic copper supplementation, somewhere between 9.6 and 18.8 percent of Roux-en-Y patients develop copper deficiency over time.
Here's the part that surprises people: the deficiency often shows up years to decades after the surgery. A patient who had bariatric surgery in 2010 and is just now developing balance trouble in 2026 may not connect the two — and neither may their neurologist, unless someone specifically asks about distant surgical history.
Other bariatric and gastric procedures carry similar risk: duodenal switch, single-anastomosis gastric bypass, the older jejunoileal bypass surgeries. Sleeve gastrectomy carries lower but non-zero risk. Anyone with a bariatric history needs lifelong vitamin and mineral monitoring that includes copper, and they need to advocate for it themselves if their bariatric program isn't doing it routinely.
Zinc-Containing Denture Cream
This is the cause that put copper deficiency neuropathy on the medical map. In 2008, a team led by Sharon Nations published a landmark case series in the journal Neurology describing four patients with profound neurologic disease — all heavy denture cream users, all with low copper and high zinc on lab work. The cream they were using contained zinc, and chronic ingestion of large amounts (which happens when ill-fitting dentures require a tube of cream a week or more) was the source.
The mechanism is elegant in its own awful way. Zinc, when consumed in excess, induces the body to make a protein called metallothionein in the gut lining. Metallothionein binds copper more tightly than it binds zinc, traps it in the intestinal cells, and prevents it from being absorbed into the bloodstream. The trapped copper is then shed with the intestinal cells during their normal turnover. Over months or years, chronic high zinc intake systematically depletes the body of copper.
The 2008 paper triggered a wave of litigation against the manufacturers of zinc-containing denture creams. GlaxoSmithKline reformulated Super Poligrip to be zinc-free in 2010, and reportedly settled the bulk of its cases. Most denture creams sold in the United States today are zinc-free or labeled as such, but older tubes and some imported products may still contain zinc. The takeaway for any current denture wearer: check your tube. If the ingredients list zinc oxide or zinc anything, switch to a zinc-free formulation, and consider getting your dentures refitted so you need less adhesive in the first place.
Zinc Supplements (The COVID-Era Resurgence)
This one is fresh and relevant. The recommended dietary allowance for zinc is 8 to 11 milligrams a day depending on age and sex. The tolerable upper intake level — the amount above which chronic intake starts to cause problems — is 40 milligrams a day for adults.
That single number explains a recent wave of cases. Many “immune support” zinc supplements and lozenges sold over the counter contain 50 milligrams per dose, and many people took one or more per day for months during and after the COVID-19 pandemic. Doses of 50 milligrams a day sustained over weeks to months are well-documented to inhibit copper absorption. A 2024 abstract presented at the American Academy of Neurology described a new cohort of patients with zinc-induced copper deficiency myeloneuropathy that traced back specifically to pandemic-era supplementation practices.
Zinc lozenges deliver an additional twist: by dissolving in the mouth and slowly releasing zinc over an hour or more, they expose the gastrointestinal tract to prolonged elevated zinc levels, which seems to drive copper deficiency more efficiently than a single zinc pill swallowed whole.
If you've been taking 50 milligrams of zinc daily for months or longer, that's worth a conversation with your doctor — not because you need to stop without guidance, but because the dose is above the long-term safety ceiling and you may need a check of your copper and zinc levels and a discussion of whether continued zinc is necessary.
Malabsorption Syndromes — Especially Celiac Disease
Conditions that damage the small intestine can impair copper absorption. Undiagnosed celiac disease is the most striking example — there are published case reports of patients whose first manifestation of celiac was a copper-deficiency myeloneuropathy, with gut symptoms either silent or so mild they had never sought attention. Inflammatory bowel disease (especially Crohn's, which can involve the small bowel), short bowel syndrome from previous surgical resection, and chronic diarrhea of any cause can all impair copper absorption over time.
If you've never been tested for celiac and you're being worked up for unexplained neuropathy, asking for a tissue transglutaminase IgA test is a reasonable addition to the panel.
Wilson Disease Overtreatment
Wilson disease is the inverse problem — the body holds onto too much copper, and treatment involves either chelators that remove copper or prescribed zinc therapy that blocks absorption. If zinc therapy is dosed too aggressively, or if monitoring lapses, a Wilson patient can swing into copper deficiency. This is a niche but important scenario: if you have Wilson disease and you start developing balance trouble, sensory changes, or unexplained anemia, talk to your hepatologist before assuming your symptoms are unrelated to your treatment. And critically: do not stop prescribed zinc therapy on your own. That can be dangerous.
Other Causes
Long-term total parenteral nutrition without adequate copper supplementation, nephrotic syndrome (urinary copper loss), and rare cases that remain idiopathic despite full workup round out the picture.
One important distinction: copper deficiency that develops in adults — what this article is about — is completely different from Menkes disease, a rare genetic disorder of copper transport that presents in infants. Don't confuse them. Menkes is a separate condition and is not what this article addresses.
How Copper Deficiency Is Diagnosed
The diagnosis rests on a small, cheap, accessible blood panel — when ordered. The challenge is that this panel is usually not ordered unless someone specifically thinks to look. Here is the panel that actually answers the question:
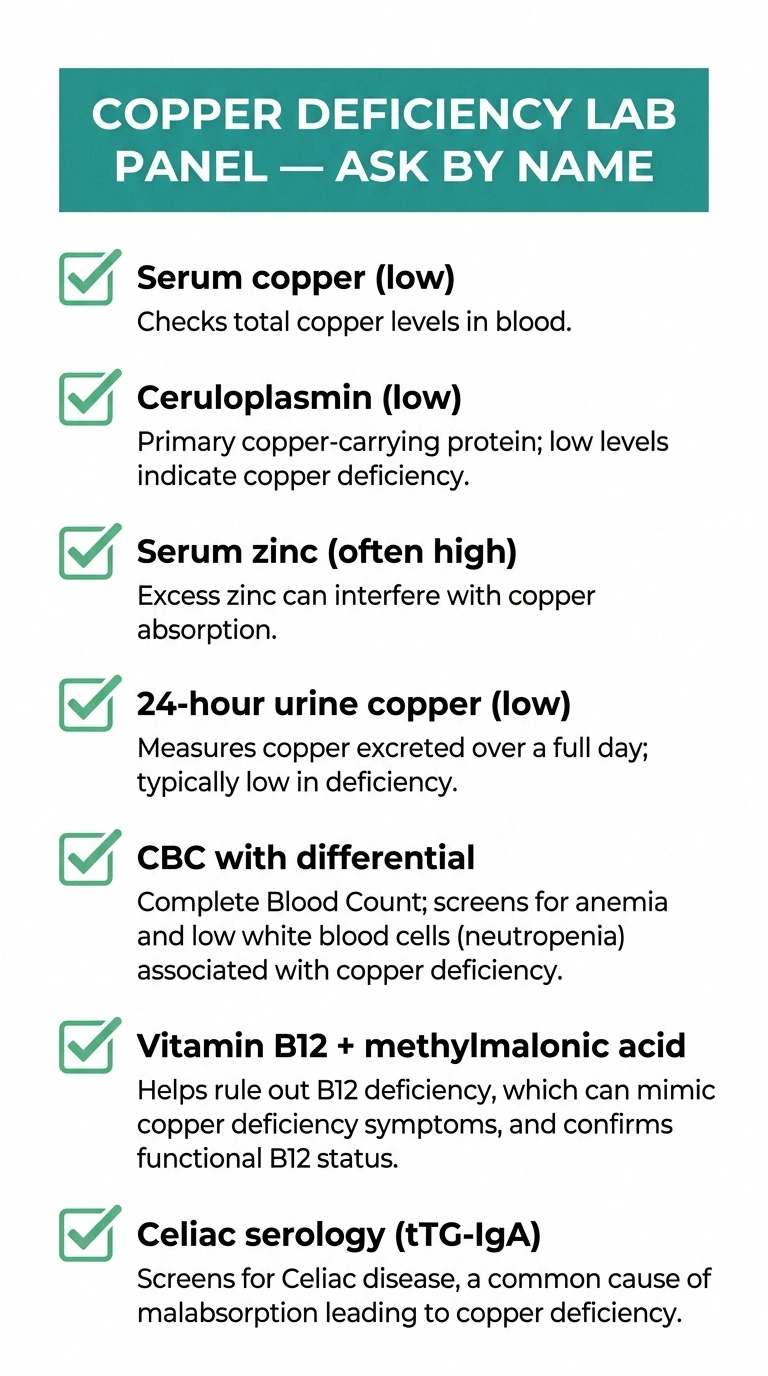
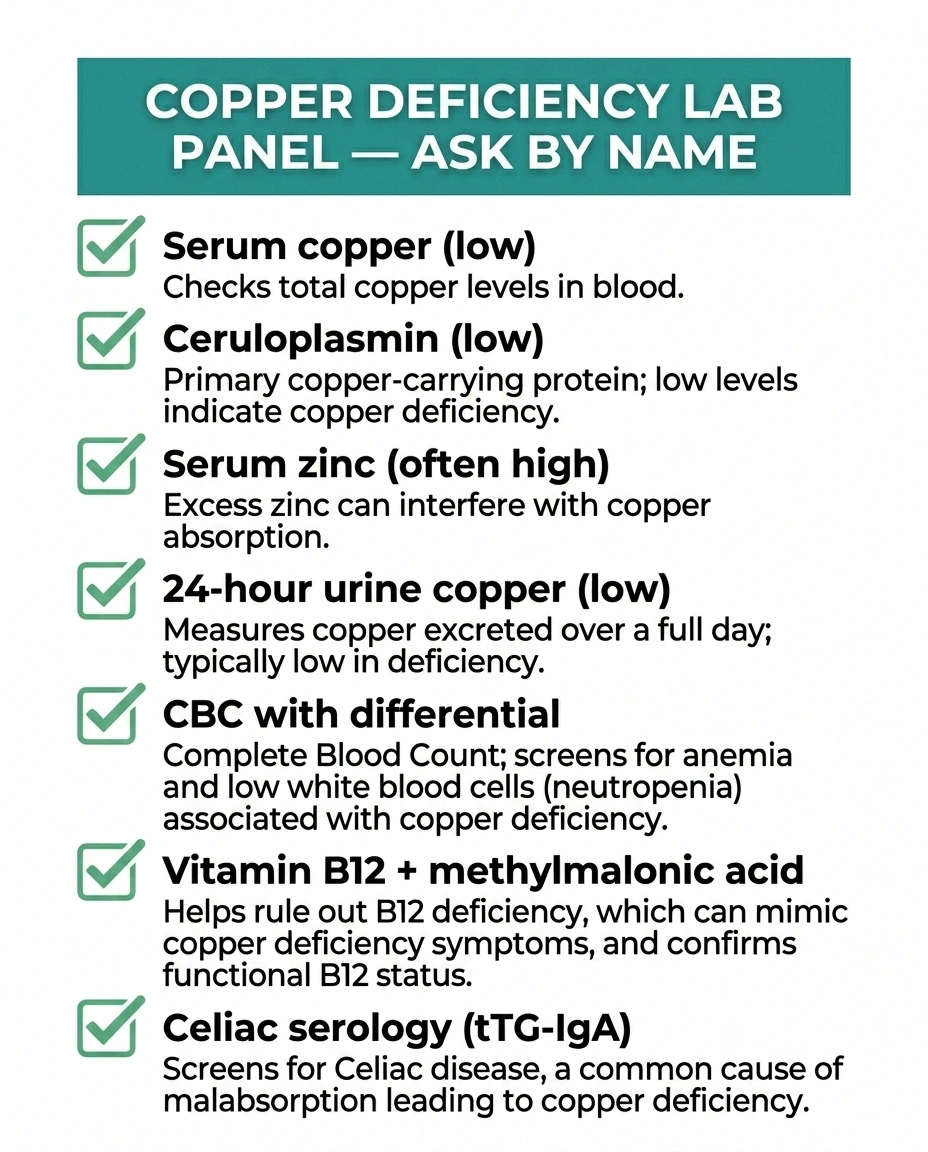
Serum copper. In copper deficiency, this is low. Normal adult range is typically about 70 to 140 micrograms per deciliter, though reference ranges vary by lab.
Serum ceruloplasmin. Ceruloplasmin is the protein that carries about 90 percent of plasma copper. In copper deficiency, it's low — typical reference range is around 20 to 35 milligrams per deciliter. Copper and ceruloplasmin move together; both being low strengthens the case.
Serum zinc. Especially in zinc-induced cases (denture cream, supplements, Wilson's treatment overshoot), serum zinc is often elevated. Normal zinc doesn't rule out zinc-induced disease in chronic users, but an elevated level adds a strong clue.
24-hour urine copper. Typically low in copper deficiency. This is also useful for distinguishing from Wilson disease, where 24-hour urine copper is high — a key discriminator.
Complete blood count with differential and peripheral smear. Looking for anemia, low neutrophils, low platelets, and any abnormalities the lab tech notices on the smear (such as vacuolated cells or ring sideroblasts).
Vitamin B12 and methylmalonic acid. Because B12 deficiency produces a nearly identical picture, and because both deficiencies can coexist (especially post-bariatric), checking B12 in parallel is essential. For more on B12-related neuropathy, our piece on vitamin deficiency and neuropathy goes into the B12 side in detail.
Celiac serology (tissue transglutaminase IgA). Especially if no obvious zinc source or surgical history surfaces.
Supporting workup often includes MRI of the cervical and thoracic spine looking for the characteristic T2 hyperintensity in the posterior columns, and nerve conduction studies and EMG showing an axonal sensorimotor polyneuropathy pattern. These look the same in copper deficiency as in B12 deficiency — the blood work is what tells them apart.
The history matters as much as the labs. A clinician evaluating you for possible copper deficiency should ask about: every supplement you take (including multivitamins and “immune support” lozenges, in their exact doses), denture use and how much adhesive you go through, any previous bariatric surgery (even decades ago), gut symptoms or known IBD or celiac, and family history of Wilson disease.
How It's Treated — and the Honest Prognosis
Treatment is straightforward in concept and rests on three things: stop whatever's depleting your copper, replace the copper, and monitor the levels long-term.

Removing the source. Switch to zinc-free denture cream if denture adhesive is the cause, and consider having your dentures refitted to reduce how much adhesive you need. Stop unnecessary zinc supplements after talking to your doctor. For Wilson disease patients, the dose adjustment must be made by your hepatologist — do not reduce or stop zinc therapy on your own. Treat the underlying malabsorption condition (gluten-free diet for celiac, IBD management, etc.).
Copper repletion. The typical clinical protocol uses oral elemental copper at about 2 to 8 milligrams per day, with higher doses (commonly 6 to 8 milligrams a day) for the first 1 to 3 months to rebuild levels and a maintenance dose (often around 2 milligrams a day) thereafter. Copper gluconate and copper sulfate are common forms. For severe cases or patients who can't absorb oral copper, intravenous copper is used short-term followed by oral maintenance. None of this is something to do on your own with an internet-bought supplement. Doses should be determined and monitored by a physician, and copper supplementation in the wrong context (Wilson disease, for example) is harmful.
Monitoring. Serum copper and ceruloplasmin are typically rechecked every 1 to 2 months until normalized, then every 6 to 12 months for life if the underlying cause is permanent (like prior bariatric surgery). Complete blood counts track hematologic recovery, which usually leads the neurologic recovery by weeks.
Now the hard part — the honest prognosis. The hematologic abnormalities (anemia, low white cell count) usually recover quickly and completely within weeks to a few months after copper repletion. The neurologic damage is a different story. Copper repletion reliably arrests the progression of neuropathy and myelopathy in most patients, but full neurologic recovery is the exception, not the rule. Published outcomes suggest roughly 49 percent of patients see some neurologic improvement; complete recovery is uncommon; sensory ataxia and gait instability are the most likely deficits to persist.
The longer the deficit has been present before diagnosis, the less recovery you can expect. This is why catching it early matters so much — and why we're talking about it.
I want to be clear about that picture because the alternative — promising reversal — sets people up for disappointment that hurts more than the truth. The honest framing is this: early diagnosis can stop this from getting worse, and may give back some function. It rarely gives back everything. The most important thing is finding it early.
What to Ask Your Doctor
If something in this article sounds like it could fit your situation, here is the conversation script I'd suggest. Bring this exact list to your appointment if it helps you remember.
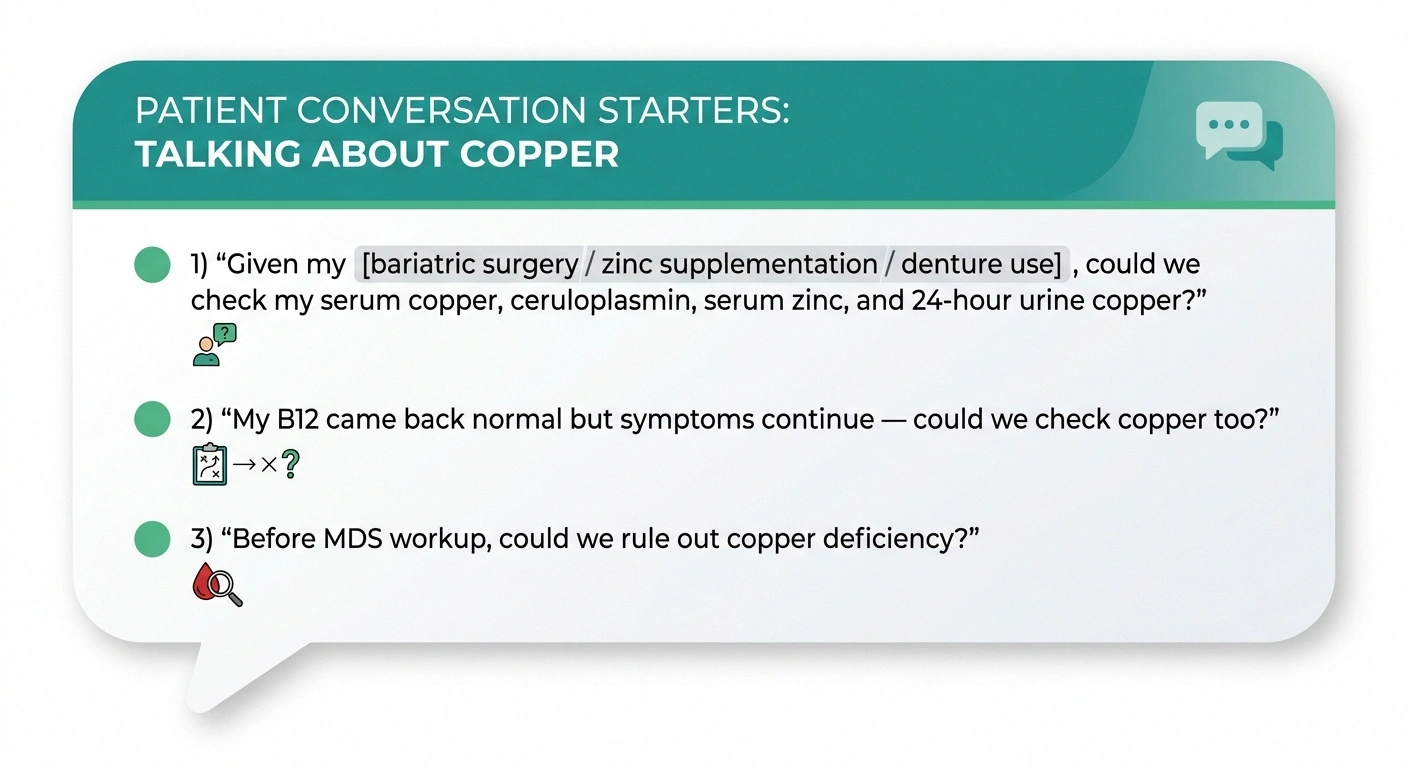
“I've been reading about copper deficiency myeloneuropathy. Given my history of [bariatric surgery / denture use with adhesive / long-term zinc supplementation / unexplained anemia / celiac disease / Wilson disease treatment], could we check my copper status? Specifically, I'd like to know my serum copper, ceruloplasmin, serum zinc, and a 24-hour urine copper if that's appropriate. And could we look at my CBC for any cytopenias?”
If you've already been told your B12 is normal but your neuropathy symptoms are still progressing or unexplained: “My B12 came back normal but I'm still having balance and sensation symptoms. Could we test copper as well? I understand the clinical picture can look identical.”
If you've been referred to hematology for possible MDS: “Before we proceed with the more invasive workup, could we rule out copper deficiency? It can mimic MDS on bone marrow exam, and treatment is dramatically different.”
Doctors generally welcome specific, well-formed questions. You're not telling them what to do — you're helping them think about a less-common cause they may not have on their default list. For more on how to advocate for yourself in medical appointments, our guide on how to talk to your doctor about neuropathy pain has some useful framing.
When to Push for Testing — Red-Flag Combinations
You don't need every symptom on the list. But certain combinations should prompt asking about copper specifically:

Progressive numbness, tingling, or balance trouble plus any of: a history of bariatric surgery (any era), heavy denture-cream use, daily zinc supplementation at 50 milligrams or more for months, known or suspected malabsorption, unexplained anemia or low white blood cell counts, or B12 testing that came back normal but symptoms continued.
An MRI of the spine showing T2 hyperintensity in the posterior columns is another strong signal — it's classically described in B12 deficiency, but copper deficiency produces an identical finding.
A hematology referral for evaluation of possible MDS in a patient who also has neurologic symptoms deserves a copper check before invasive workup.
The Bottom Line
Copper deficiency neuropathy is rare but real, treatable but often incompletely reversible, and underdiagnosed in ways that cost patients permanent function. It hides behind a clinical picture that looks like B12 deficiency, and the people most likely to develop it — patients years out from bariatric surgery, people taking high-dose zinc supplements, denture wearers who go through more adhesive than they should, and people with quiet malabsorption — aren't routinely screened for it.
If any of those describe you, the single most useful thing you can do is ask your doctor for a copper panel. Three blood tests. Maybe a urine collection. That's it. Either the labs come back normal and you can rule it out, or they reveal something that changes the trajectory of a serious, otherwise-progressive neurologic problem.
This is one of those conditions where the cost of testing is trivial and the cost of missing it can be catastrophic. The math of the workup should be easy. The challenge is getting the test on the order. Asking by name is how you get there.
Frequently Asked Questions
What are the early signs of copper deficiency?
The earliest signs are usually hematologic — unexplained anemia (which can be macrocytic, normocytic, or microcytic), low white blood cell counts, and sometimes low platelets. Fatigue and frequent infections can follow. Neurologic symptoms typically appear later and include numbness and tingling in the feet, balance trouble that worsens in the dark, leg stiffness or weakness, and reduced vibration sense. The hematologic findings often precede the neurologic ones by months or years.
Can too much zinc cause neuropathy?
Yes, indirectly. Chronic high zinc intake (especially above the 40 milligram per day upper safe limit) blocks copper absorption in the gut, leading to copper deficiency. The neuropathy is caused by the copper deficiency, not by zinc directly damaging nerves. The most common sources are zinc-containing denture creams (now mostly reformulated but still around), high-dose zinc supplements taken long-term, and excess zinc lozenges.
How is copper deficiency diagnosed?
Through blood tests: serum copper (low), serum ceruloplasmin (low), and serum zinc (often elevated in zinc-induced cases). A 24-hour urine copper test (low in deficiency) helps confirm and helps distinguish from Wilson disease. Complete blood count looks for anemia and low cell counts. The doctor will also take a careful history of supplements, denture use, surgical history, and any gut issues. None of these are routine on standard neuropathy panels, so they usually need to be ordered specifically.
Is copper deficiency neuropathy reversible?
Partially. Copper repletion reliably stops progression in most patients. Hematologic abnormalities (anemia, low cell counts) usually recover fully within weeks to months. Neurologic recovery is less complete — published outcomes show roughly 49 percent of patients see some neurologic improvement, but full reversal is uncommon. Sensory ataxia and gait instability are the deficits most likely to persist. The earlier the diagnosis, the more recovery is possible.
Can bariatric surgery cause copper deficiency years later?
Yes — and this is one of the most under-recognized presentations. Copper is absorbed in the stomach and upper small intestine, which Roux-en-Y gastric bypass routes around. Without lifelong copper monitoring and supplementation, somewhere between 9.6 and 18.8 percent of Roux-en-Y patients develop deficiency, often a decade or more after surgery. Anyone with a bariatric history needs ongoing nutritional monitoring that includes copper, not just iron and vitamin B12.
How much zinc is safe to take daily?
The recommended dietary allowance for adults is 8 to 11 milligrams per day. The tolerable upper intake level for chronic use is 40 milligrams per day. Many “immune support” zinc supplements contain 50 milligrams per dose, which is above the long-term safety ceiling. Short-term higher doses for acute illness are different from chronic daily use. If you're taking more than 40 milligrams a day for months at a time, talk to your doctor about whether you need to continue and whether your copper status should be checked.
Can denture cream still cause copper deficiency today?
It's much less common now than it was 15 years ago. After the 2008 Nations paper in Neurology, GlaxoSmithKline reformulated Super Poligrip to be zinc-free in 2010, and most denture creams sold in the United States today are zinc-free. But older tubes, imported products, and some formulations may still contain zinc. Check the ingredient list on your tube. If it lists zinc anything, switch to a zinc-free product. Ill-fitting dentures that require heavy adhesive use are the main risk factor — addressing the fit reduces the need for cream in the first place.
What is the difference between copper deficiency and B12 deficiency neuropathy?
Clinically and on imaging they can be nearly identical — both produce a myeloneuropathy with sensory ataxia, balance trouble, stocking-distribution numbness, posterior column signs, and characteristic T2 hyperintensity on spine MRI. The blood work is what tells them apart: B12 deficiency shows low B12 and elevated methylmalonic acid; copper deficiency shows low copper and ceruloplasmin (often with elevated zinc). The two can also coexist, especially in post-bariatric patients, so both should be checked. The clinical pictures are mimics — they don't replace each other in your workup.


