Ulnar Neuropathy: When the Funny Bone Nerve Is No Joke
Everyone's hit their “funny bone” at some point — that sharp, electric jolt that shoots down your forearm into your ring and pinky fingers when you bang the inside of your elbow. What most people don't realize is that what they're actually hitting is the ulnar nerve, and for millions of people, that nerve isn't just annoying when bumped — it's a source of chronic pain, numbness, and hand weakness that can seriously impact daily life.
Ulnar neuropathy is the second most common compressive neuropathy in the upper extremity, right behind carpal tunnel syndrome. Yet it doesn't get nearly the same attention. When I first started experiencing persistent numbness in my ring and pinky fingers, I assumed it was related to my general peripheral neuropathy. It took months before a neurologist identified the ulnar nerve as the specific culprit — and that distinction mattered for treatment.
Whether you're dealing with numbness in your last two fingers, a weakening grip, or that persistent electric sensation in your elbow, this guide will help you understand what's happening, why, and what you can do about it.
What Is Ulnar Neuropathy?
The ulnar nerve is one of the three major nerves in your arm, running from the side of your neck all the way down to your hand. It's responsible for sensation in your ring and pinky fingers and controls most of the small muscles in your hand that let you do precise movements — like typing, playing piano, buttoning a shirt, or gripping a jar lid.
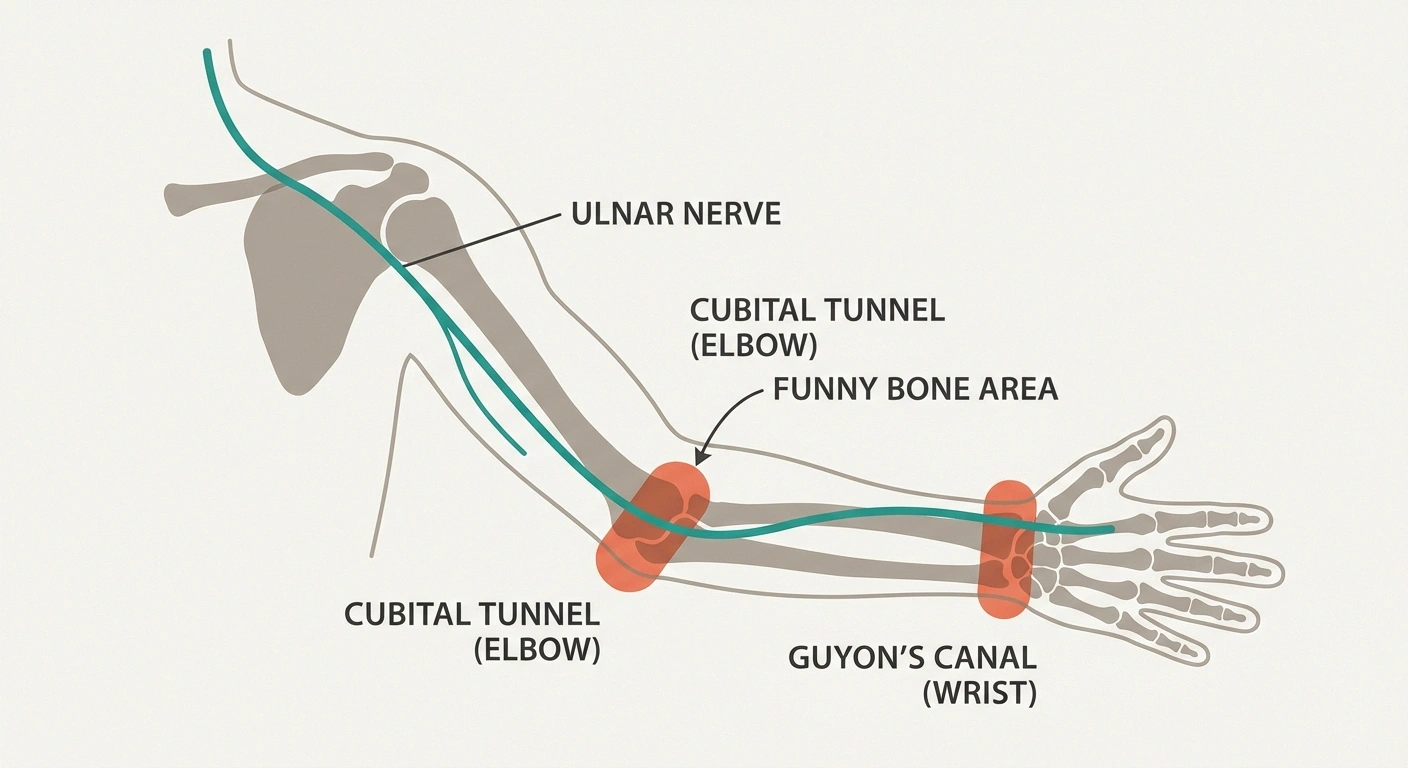
Ulnar neuropathy occurs when this nerve becomes compressed, stretched, or irritated at some point along its path. While the nerve can be affected anywhere from the neck to the wrist, the two most common trouble spots are:
- The elbow (cubital tunnel syndrome) — This accounts for the vast majority of ulnar neuropathy cases. The nerve passes through a narrow channel called the cubital tunnel, right behind that bony bump on the inside of your elbow (the medial epicondyle). This is your “funny bone” — and at this point, the nerve sits very close to the skin with almost no cushioning or protection.
- The wrist (Guyon's canal syndrome) — Less common, but the nerve can also be compressed as it passes through a tunnel called Guyon's canal at the base of the palm.
Understanding where the compression is happening is critical because it determines the symptoms you experience and the treatment approach that's most likely to help.
What Causes Ulnar Neuropathy?
Unlike some forms of neuropathy that develop from systemic conditions like diabetes, ulnar neuropathy is most often caused by mechanical factors — things that physically put pressure on or irritate the nerve.

Prolonged or Repetitive Elbow Flexion
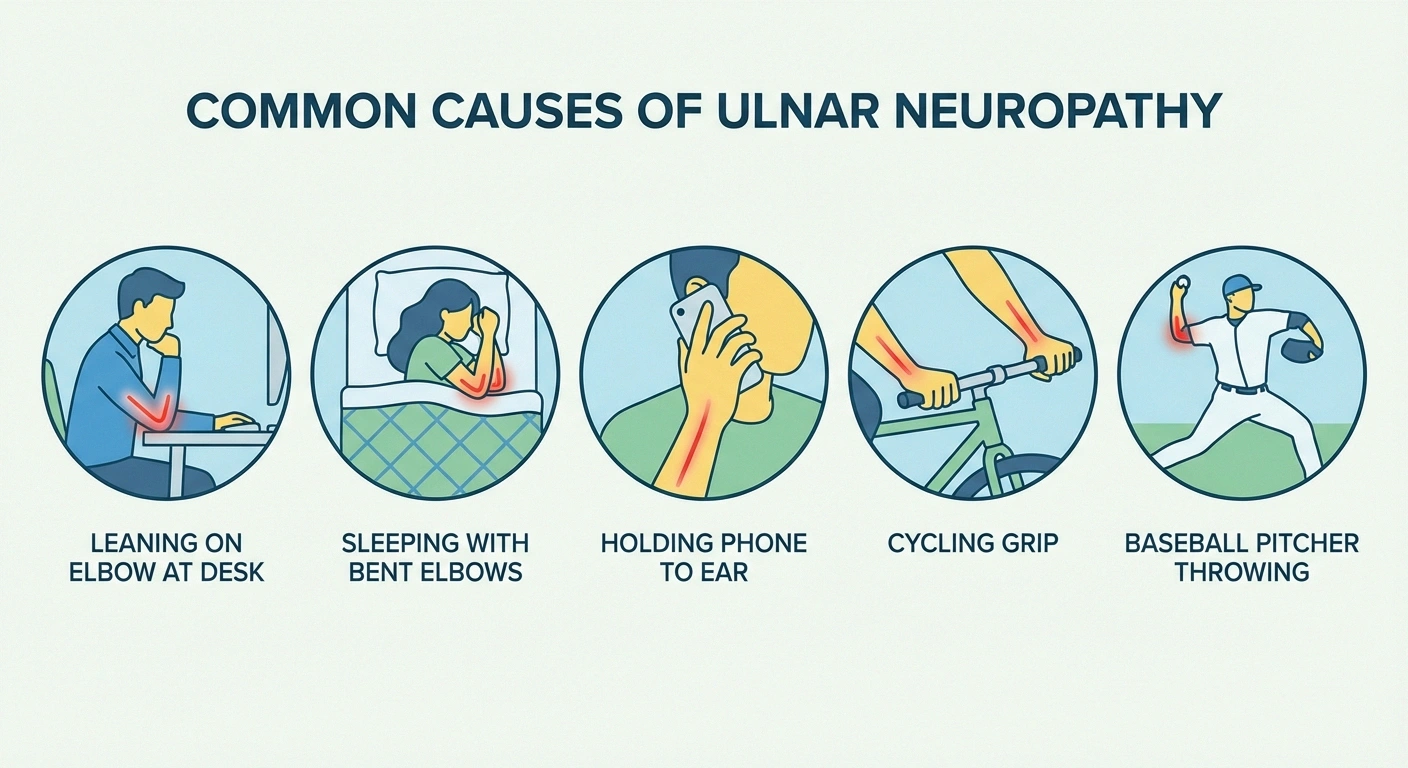
When you bend your elbow, the ulnar nerve stretches and its blood supply temporarily decreases. Brief bending is fine — your nerve is designed for it. But keeping your elbow bent for extended periods (sleeping with bent elbows, holding a phone to your ear, resting on your elbows while working) can irritate the nerve over time. This is one of the most common causes of cubital tunnel syndrome.
Direct Pressure on the Elbow
Leaning on your elbow — on a desk, armrest, car window, or table — puts direct pressure on the unprotected nerve. Over time, this repeated compression can cause inflammation and nerve damage. This is why cubital tunnel syndrome is sometimes called “cell phone elbow” or “computer elbow.”
people are affected by ulnar neuropathy each year — the second most common compressive nerve condition
Anatomy Variations
Some people's ulnar nerves naturally slide back and forth over the bony bump of the medial epicondyle when they bend and straighten their elbow. This subluxation creates friction that can gradually damage the nerve. Others may have a naturally narrower cubital tunnel, leaving less room for the nerve to move without compression.
Trauma and Injury
A broken elbow, dislocated elbow, or even a bad fall onto an outstretched hand can damage the ulnar nerve directly or create scar tissue that compresses it later. Previous elbow surgery can also create scarring around the nerve.
Medical Conditions That Increase Risk
Several systemic conditions make you more susceptible to ulnar neuropathy:
- Diabetes — high blood sugar makes all nerves more vulnerable to compression injury
- Rheumatoid arthritis — inflammation around the elbow joint can narrow the cubital tunnel
- Thyroid problems — hypothyroidism can cause fluid retention that compresses nerves
- Elbow arthritis or bone spurs — can physically narrow the space available for the nerve
- Obesity — increases the risk of nerve compression throughout the body
Occupational and Activity Risk Factors
Certain activities and occupations carry higher risk:
- Manual laborers who perform repetitive elbow movements
- Wheelchair users who lean on armrests
- Desk workers who rest elbows on hard surfaces
- Musicians, especially guitarists and pianists
- Baseball pitchers (the throwing motion puts significant stress on the inner elbow)
- Cyclists who grip handlebars for extended periods (wrist compression)
Recognizing the Symptoms
Ulnar neuropathy symptoms typically develop gradually, though they can start suddenly after an injury. The pattern of symptoms depends on where the nerve is compressed and how severely.
Early Symptoms
- Numbness and tingling in the ring and pinky fingers — This is usually the first sign. It often comes and goes, worsening when your elbow is bent (driving, holding a phone, sleeping)
- “Falling asleep” sensation — Similar to the feeling when a limb “falls asleep,” but localized to just those two fingers
- Aching pain on the inner side of the elbow — Sometimes mistaken for tennis elbow (which affects the outer elbow)
- Symptoms that wake you at night — Many people sleep with their elbows bent, which compresses the nerve for hours. Waking with numb or tingling fingers is a hallmark sign
Progressive Symptoms
- Weakened grip strength — Difficulty opening jars, turning doorknobs, or holding objects securely
- Loss of fine motor coordination — Trouble typing, playing instruments, or manipulating small objects
- Pain that radiates from the elbow down to the hand
- Difficulty spreading fingers apart or bringing them together
Advanced Symptoms
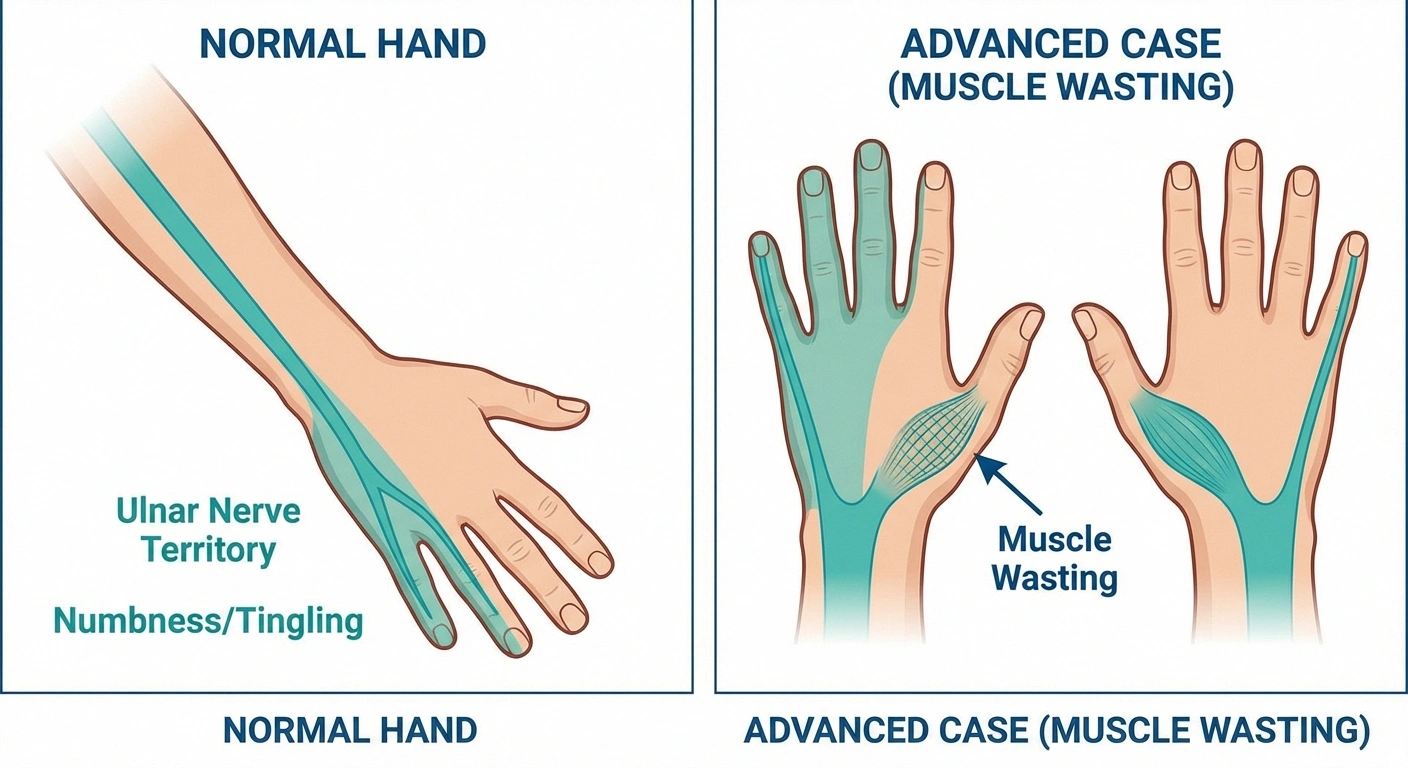
- Visible muscle wasting in the hand — The spaces between the knuckles become hollow as the small hand muscles atrophy. Once this occurs, it's often not fully reversible.
- “Claw hand” deformity — In severe, untreated cases, the ring and pinky fingers can curl into a fixed bent position
- Constant numbness — Sensation loss that no longer comes and goes but is always present
Important timing: If you have symptoms lasting more than 6 weeks, or if you notice any weakness or muscle wasting in your hand, see a doctor promptly. The longer the nerve is compressed, the harder it becomes to achieve full recovery.
🟢 Early Stage
• Intermittent tingling in ring & pinky fingers
• “Falling asleep” sensation
• Worsens with elbow bending
🟡 Progressive
• Weakened grip strength
• Loss of fine motor skills
• Radiating elbow-to-hand pain
🔴 Advanced
• Visible muscle wasting
• “Claw hand” deformity
• Constant, irreversible numbness
How Ulnar Neuropathy Is Diagnosed
Getting the right diagnosis is important because ulnar neuropathy can mimic other conditions — and the treatment approach depends on precisely where and how the nerve is affected. Your diagnostic workup will typically include:
Talk to Your Doctor
If you notice hand weakness or muscle wasting, seek medical evaluation promptly. Once significant muscle atrophy occurs from ulnar nerve compression, it may not be fully reversible — even with surgery. Early intervention gives the best chance of complete recovery.
Physical Examination
Your doctor will perform several specific tests:
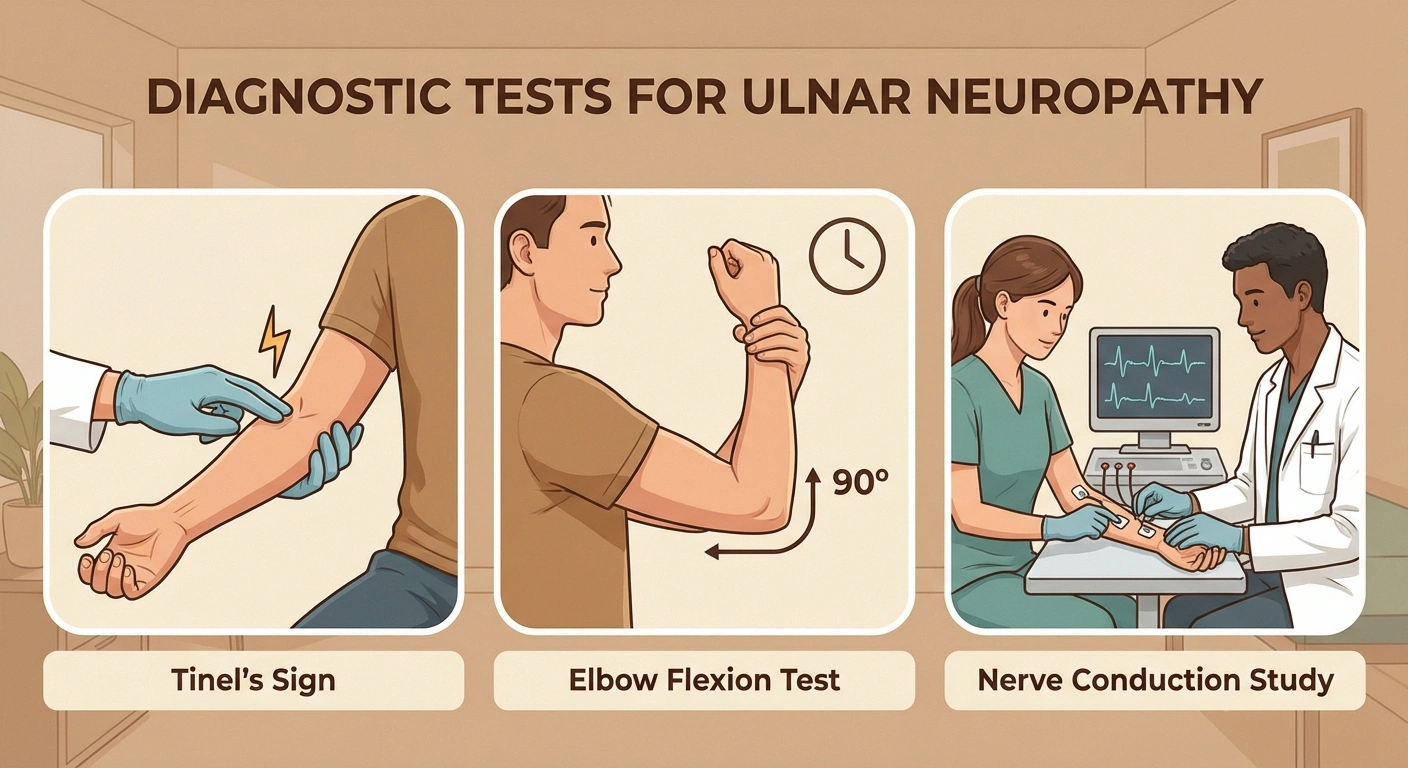
- Tinel's sign — Tapping over the nerve at the funny bone. If the nerve is irritated, this produces a tingling or shock sensation into the ring and pinky fingers.
- Elbow flexion test — Holding the elbow fully bent for 60 seconds. If symptoms are reproduced, this suggests cubital tunnel syndrome.
- Froment's sign — Tests for weakness in the adductor pollicis muscle (controlled by the ulnar nerve) by having you pinch a piece of paper between your thumb and index finger.
- Grip strength and finger spread testing
- Neck and shoulder examination — Pinched nerves in the cervical spine can cause similar symptoms and need to be ruled out
Nerve Conduction Studies and EMG
Electrodiagnostic testing is the gold standard for confirming ulnar neuropathy and determining its severity. Nerve conduction studies measure how fast electrical signals travel through the ulnar nerve — a slowing at the elbow confirms cubital tunnel syndrome. EMG (electromyography) examines the muscles controlled by the ulnar nerve to assess whether the nerve damage has progressed to the point of affecting muscle function.
Imaging
- X-rays — Check for bone spurs, arthritis, or previous fractures that may be compressing the nerve
- Ultrasound — Can visualize the nerve directly, showing swelling, compression, or subluxation
- MRI — Sometimes used to look for masses, cysts, or other structural causes of compression
Conservative Treatment: The First Line of Defense
The good news is that many cases of ulnar neuropathy — especially when caught early — respond well to conservative (non-surgical) treatment. The goal is to reduce pressure on the nerve and give it time to heal.
Activity Modification
The simplest and most important step is changing the habits that are compressing your nerve:
- Avoid leaning on your elbows — use a cushion or pad if you need armrest support
- Hold your phone at chest level instead of bending your elbow to your ear (or use speakerphone/earbuds)
- If you work at a desk, keep your arms at a comfortable angle — avoid resting your elbows on hard surfaces
- Take breaks during repetitive activities that involve elbow bending
Night Splinting
Since many people bend their elbows while sleeping — sometimes severely — wearing a splint or brace that keeps the elbow straight at night can provide significant relief. A simple approach is wrapping a towel around your elbow at bedtime to prevent bending, or wearing an elbow pad backwards (so the padding prevents full flexion).
Elbow Padding
Wearing an elbow pad during the day protects the nerve from direct pressure. This is especially helpful for people whose work or hobbies involve resting on their elbows.
Nerve Gliding Exercises
Physical and occupational therapists can teach you nerve gliding (neural mobilization) exercises that help the ulnar nerve move more smoothly through the cubital tunnel and reduce adhesions. These gentle movements are designed to improve the nerve's ability to slide within its tunnel without catching or being compressed. Talk to your healthcare provider before starting nerve gliding exercises, as they need to be performed correctly to avoid further irritation.
Living With Ulnar Neuropathy: Day-to-Day Management
Whether you're managing conservatively or recovering from surgery, these daily strategies can help:
Ergonomic Adjustments
- Set up your workspace so your elbows rest at about 90 degrees, not fully bent
- Use an ergonomic keyboard if typing worsens symptoms
- Adjust your car seat and steering wheel position to minimize elbow bending while driving
- Use cushioned armrest pads on chairs
Sleep Positioning
- Keep your arms relatively straight while sleeping (the towel trick works well)
- Avoid tucking your hands under your pillow, which forces elbow flexion
- Consider a body pillow to maintain comfortable arm positioning
Adaptive Strategies for Weak Grip
- Use jar openers, ergonomic kitchen tools, and built-up grip utensils
- Button hooks and zipper pulls can help with dressing if fine motor skills are affected
- Voice-to-text software can reduce typing demands
- Consider occupational therapy for personalized adaptive strategies
How Ulnar Neuropathy Relates to Other Types of Neuropathy
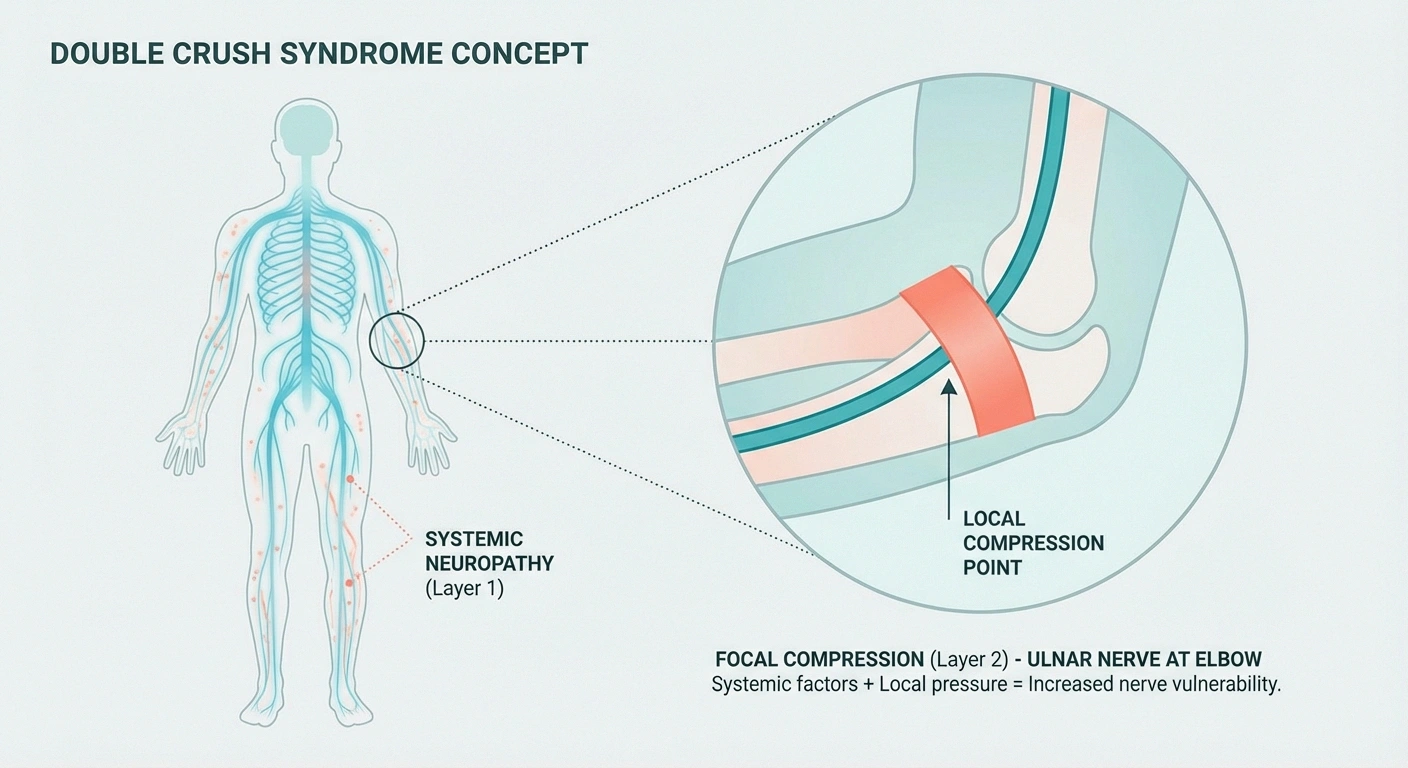
If you're already living with peripheral neuropathy — whether from diabetes, idiopathic causes, or another condition — you may be at higher risk for developing ulnar neuropathy. Nerves that are already compromised by systemic neuropathy are more vulnerable to compression injuries, a concept neurologists call “double crush syndrome.”
This means that if you have general peripheral neuropathy and start experiencing symptoms specifically in your ring and pinky fingers, it's worth getting evaluated for possible ulnar nerve compression on top of your existing condition. The treatments are different, and addressing the compression can provide meaningful improvement even if your underlying neuropathy remains.
Frequently Asked Questions
What does ulnar neuropathy feel like?
Most people first notice numbness or tingling in the ring and pinky fingers, often described as a “pins and needles” or “falling asleep” sensation. Some people also feel aching pain on the inner side of the elbow. In more advanced cases, you may notice weakness in your grip, difficulty with fine motor tasks like typing or buttoning clothes, and in severe cases, visible thinning of the muscles between your knuckles.
Can ulnar neuropathy heal on its own?
Mild cases — especially those caused by habits like leaning on your elbow or sleeping with bent elbows — may improve significantly with activity modification and ergonomic changes alone. However, if symptoms persist beyond a few weeks despite these changes, or if you notice any hand weakness, see a doctor. The nerve is unlikely to recover on its own if the compression is structural or has been present for a long time.

Key Takeaway
If you already have peripheral neuropathy and develop numbness specifically in your ring and pinky fingers, get evaluated for ulnar nerve compression separately. “Double crush syndrome” means compromised nerves are more vulnerable to local compression — and treating the compression can improve symptoms even when the underlying neuropathy remains.
How is ulnar neuropathy different from carpal tunnel syndrome?
Both are compression neuropathies, but they affect different nerves and produce different symptom patterns. Carpal tunnel affects the median nerve at the wrist, causing numbness in the thumb, index, and middle fingers. Ulnar neuropathy affects the ulnar nerve (usually at the elbow), causing numbness in the ring and pinky fingers. The affected fingers are the simplest way to tell them apart.
Is ulnar neuropathy surgery successful?
Success rates vary depending on the severity of nerve damage before surgery. Patients with mild to moderate neuropathy generally have good outcomes, with significant improvement in pain and numbness. However, if significant muscle wasting has already occurred, recovery may be incomplete. Early surgical consultation (before advanced damage develops) gives the best chance of full recovery.
Can I prevent ulnar neuropathy?
While not all cases are preventable (some relate to anatomy or prior injuries), you can reduce your risk significantly by avoiding prolonged elbow flexion, not leaning on your elbows, using ergonomic workstation setups, taking breaks during repetitive arm activities, and keeping your elbows straight or slightly bent while sleeping.
Should I wear a brace for ulnar neuropathy?
A nighttime elbow brace or splint that prevents full elbow flexion is one of the most commonly recommended conservative treatments. Daytime elbow pads can also help by protecting the nerve from direct pressure. Your doctor or physical therapist can recommend the best type of brace for your specific situation.
Don't Wait Until It's “Funny” No More
The irony of ulnar neuropathy is that it's named after the same nerve behind the “funny bone” — something we all laugh about. But there's nothing funny about chronic numbness, losing your grip strength, or watching the muscles in your hand waste away because you waited too long to seek help.
If you're experiencing persistent numbness in your ring and pinky fingers, pain on the inner side of your elbow, or any weakness in your hand — talk to your doctor. Early detection and treatment of ulnar neuropathy can make the difference between a full recovery and permanent nerve damage.
And if you're already managing general peripheral neuropathy, stay alert for ulnar-specific symptoms that may need separate attention. Your nerves deserve a comprehensive approach — not just for the whole system, but for each individual nerve that's calling for help.
Want to learn more about different types of neuropathy? Explore our guides to small fiber neuropathy, autonomic neuropathy, and how neuropathy is diagnosed.