
Pain Catastrophizing and Neuropathy: Breaking the Cycle That Makes Everything Worse
There's a thought pattern that shows up in almost everyone I've ever met with neuropathy — and it's doing more damage than most people realize. It happens in the middle of the night when a burning flare wakes you up: “This is never going to get better. I can't take this anymore. Something terrible is happening.” It happens when a new symptom appears: “It's spreading. I'm going to end up in a wheelchair. My life is over.”
If you recognize those spiraling thoughts, you're not losing your mind and you're not being dramatic. You're experiencing pain catastrophizing — a well-studied psychological pattern that amplifies pain, worsens outcomes, and makes neuropathy significantly harder to manage. The good news: once you understand how it works, you can learn to interrupt it.
What Is Pain Catastrophizing?
Pain catastrophizing is a cognitive-emotional response pattern where you mentally magnify pain, feel helpless against it, and become unable to stop thinking about it. It's not the same as being worried about your health — everyone with chronic pain worries. Catastrophizing is the runaway train version: the worry takes on a life of its own and becomes bigger than the pain itself.
Pain catastrophizing is the strongest psychological predictor of chronic pain outcomes — more predictive than pain severity itself
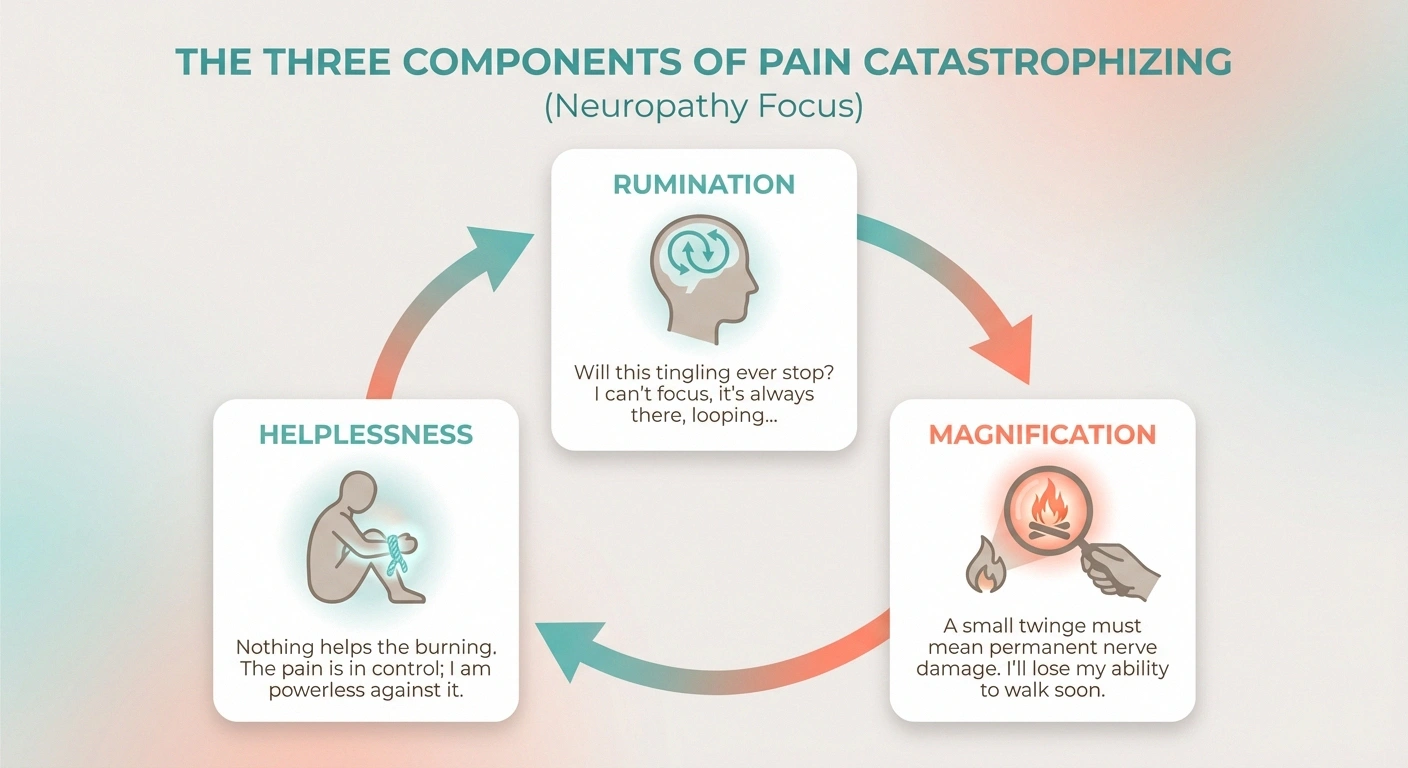
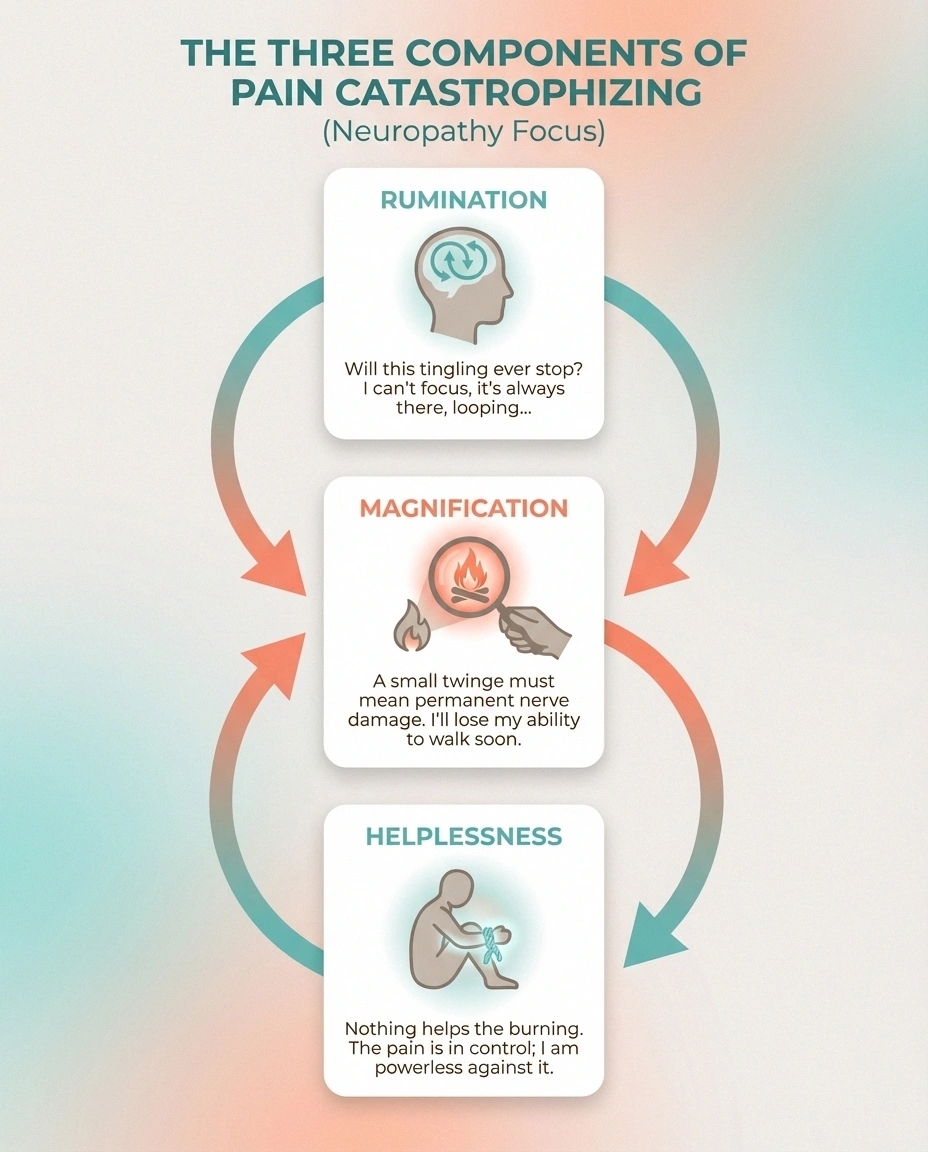
The concept was formalized by psychologist Michael Sullivan through the Pain Catastrophizing Scale (PCS), which measures three distinct components:
- Rumination — You can't stop thinking about your pain. It dominates your mental landscape. “I keep thinking about how much it hurts. I can't seem to keep it out of my mind.”
- Magnification — You interpret pain sensations as worse than they may actually be, or you assume the worst possible outcome. “Something serious must be happening. This pain means the damage is getting worse.”
- Helplessness — You feel powerless to do anything about your pain. “There's nothing I can do. It's never going to change. I can't go on like this.”
All three components feed each other. Rumination keeps your attention locked on the pain, magnification escalates the perceived threat, and helplessness removes any sense of agency. The result is a mental prison that's far worse than the physical sensation alone.
Why Neuropathy Is Uniquely Vulnerable to Catastrophizing
Not all chronic pain conditions trigger the same level of catastrophizing. Neuropathy is particularly fertile ground for it, and here's why:
Why Neuropathy Is Different
Neuropathy pain is uniquely prone to catastrophizing because it's unpredictable, produces strange sensations your brain reads as dangerous, can progress over time, and intensifies at night when you have the fewest coping resources. Understanding these triggers is the first step to breaking the pattern.
The pain is unpredictable. Unlike conditions where you can anticipate pain based on activity, neuropathy pain arrives on its own schedule. A random burning flare at 2am, tingling that intensifies for no apparent reason, shooting pain that strikes while you're sitting still. When pain is unpredictable, your brain's threat detection system stays permanently engaged — scanning for the next attack.
The sensations are strange. Burning, electric shocks, pins and needles, ice-cold patches — neuropathy produces sensations that feel dangerous precisely because they're unusual. Your brain interprets novel sensations as more threatening than familiar ones. A dull muscle ache might not trigger catastrophizing because you've felt it before. A lightning bolt shooting through your foot at 3am absolutely will.
The condition can progress. Unlike a sprained ankle that will heal, neuropathy may get worse over time. When you know that progression is possible, every new symptom becomes potential evidence of decline. A 2023 study of 1,310 small fiber neuropathy patients found that higher pain catastrophizing was significantly associated with both anxiety and depression — and that the fear of progression was a major driver.
Nighttime amplification. Neuropathy pain gets worse at night — the exact time when you have the fewest distractions, the most quiet, and the least access to coping strategies. The dark bedroom becomes a catastrophizing incubator.
The Neuroscience of Why Catastrophizing Makes Pain Worse
Here's what makes catastrophizing truly destructive: it doesn't just change how you think about pain. It physically changes how you experience pain. This isn't psychology — it's neuroscience.
Brain imaging studies have shown that people who catastrophize about pain show increased activity in brain regions responsible for attention to pain (the anterior cingulate cortex), emotional processing of pain (the amygdala and insula), and anticipation of pain (the prefrontal cortex). In other words, catastrophizing recruits more of your brain into the pain experience — turning up the volume on every pain signal your nerves send.
Research from the Comprehensive Algorithm for Management of Neuropathic Pain confirms that catastrophizing directly increases central sensitization — the process by which your spinal cord and brain become hypersensitive to pain signals. Central sensitization is already a problem in neuropathy. Catastrophizing pours fuel on it.
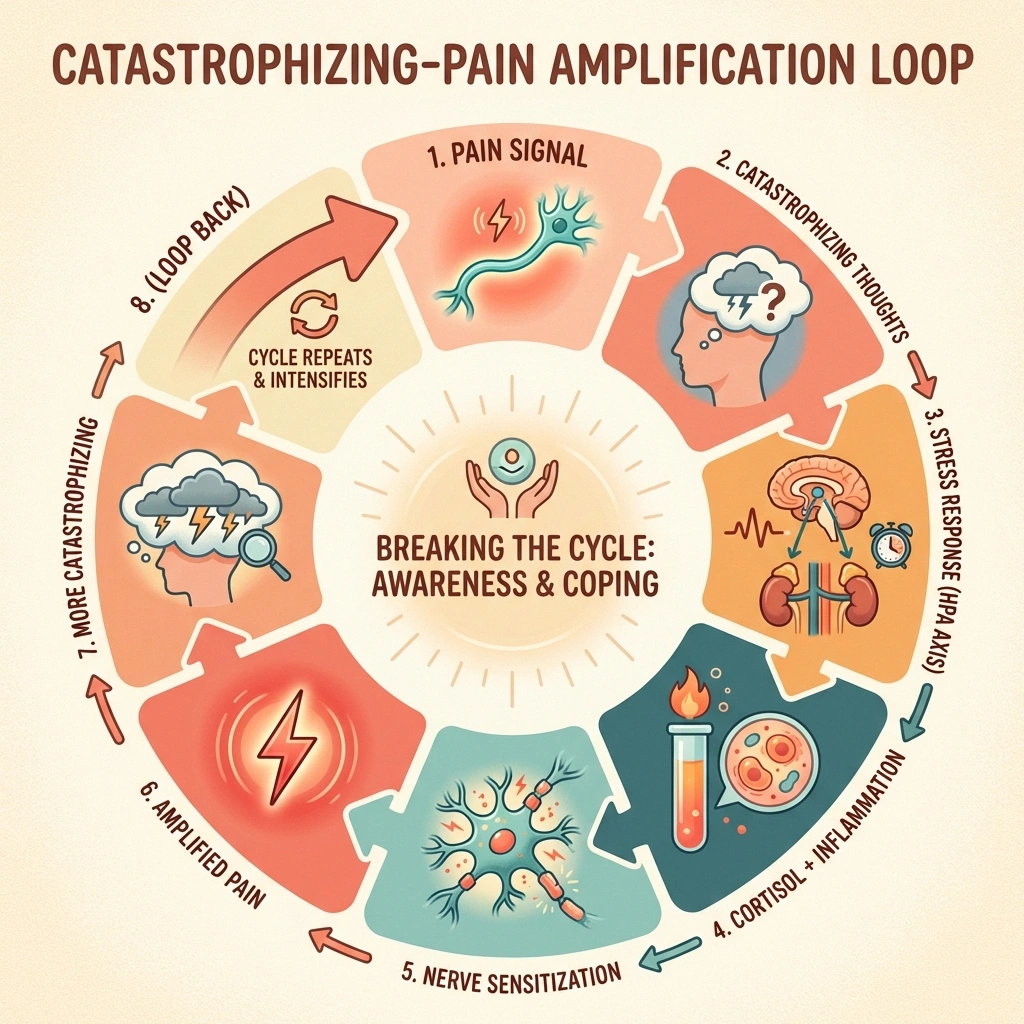
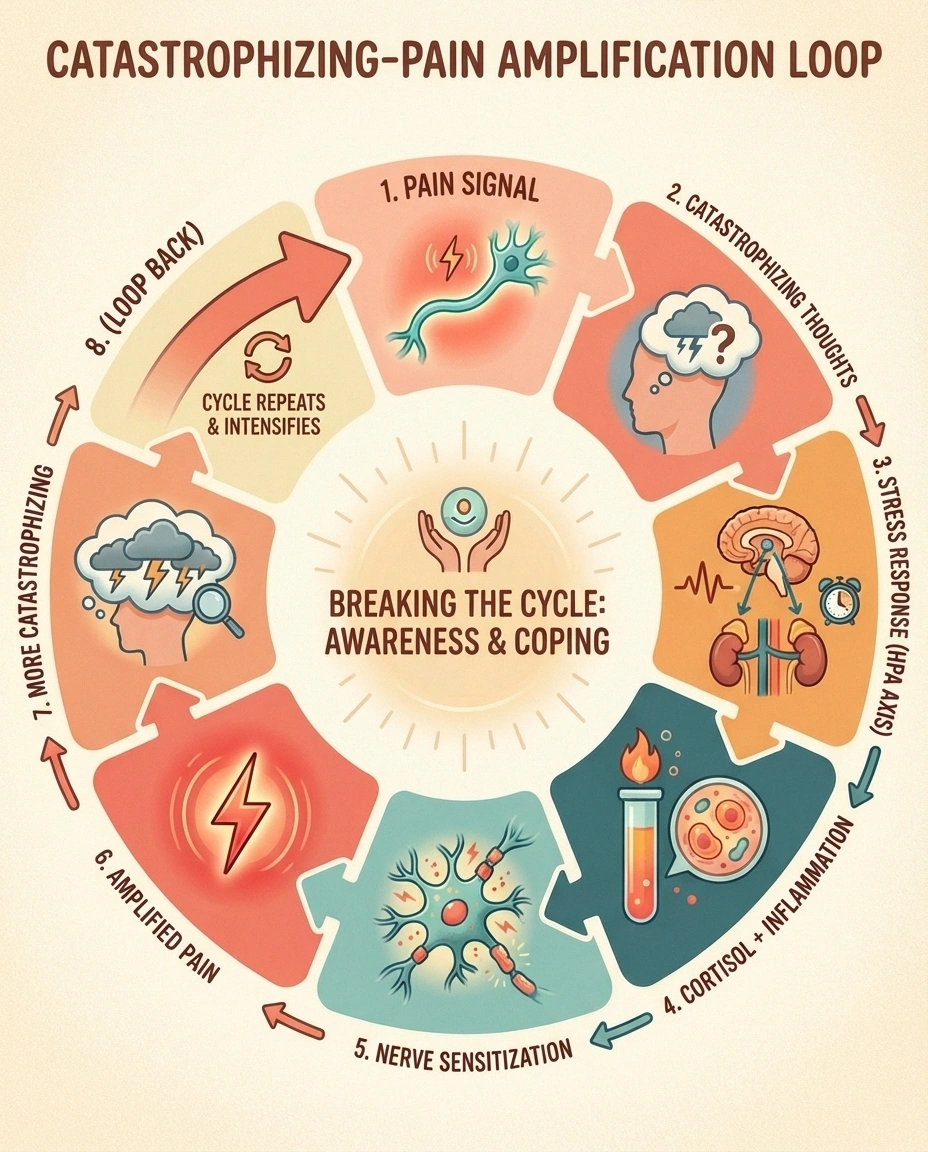
The biological cascade looks like this:
- Neuropathic pain signal arrives at your brain
- Catastrophizing thought pattern activates: “This is terrible, it's getting worse, I can't handle it”
- Your brain's threat response activates the HPA axis (stress response)
- Cortisol and adrenaline flood your system, increasing inflammation
- Inflammation further sensitizes already-damaged nerves
- Nerves send stronger pain signals to the brain
- The brain, now hyper-focused on pain due to catastrophizing, amplifies these signals
- Pain perception increases, triggering more catastrophizing
This is a self-reinforcing loop. The pain causes the catastrophizing which worsens the pain which deepens the catastrophizing. Without intervention, the cycle tends to accelerate over time — not because your nerve damage is necessarily getting worse, but because your nervous system's response to it keeps ratcheting up.
How to Recognize Your Own Catastrophizing Patterns
Catastrophizing is slippery because it feels like rational analysis. When you think “this pain means the nerve damage is spreading,” it doesn't feel like a cognitive distortion — it feels like a reasonable conclusion. That's what makes it so hard to catch in the moment.
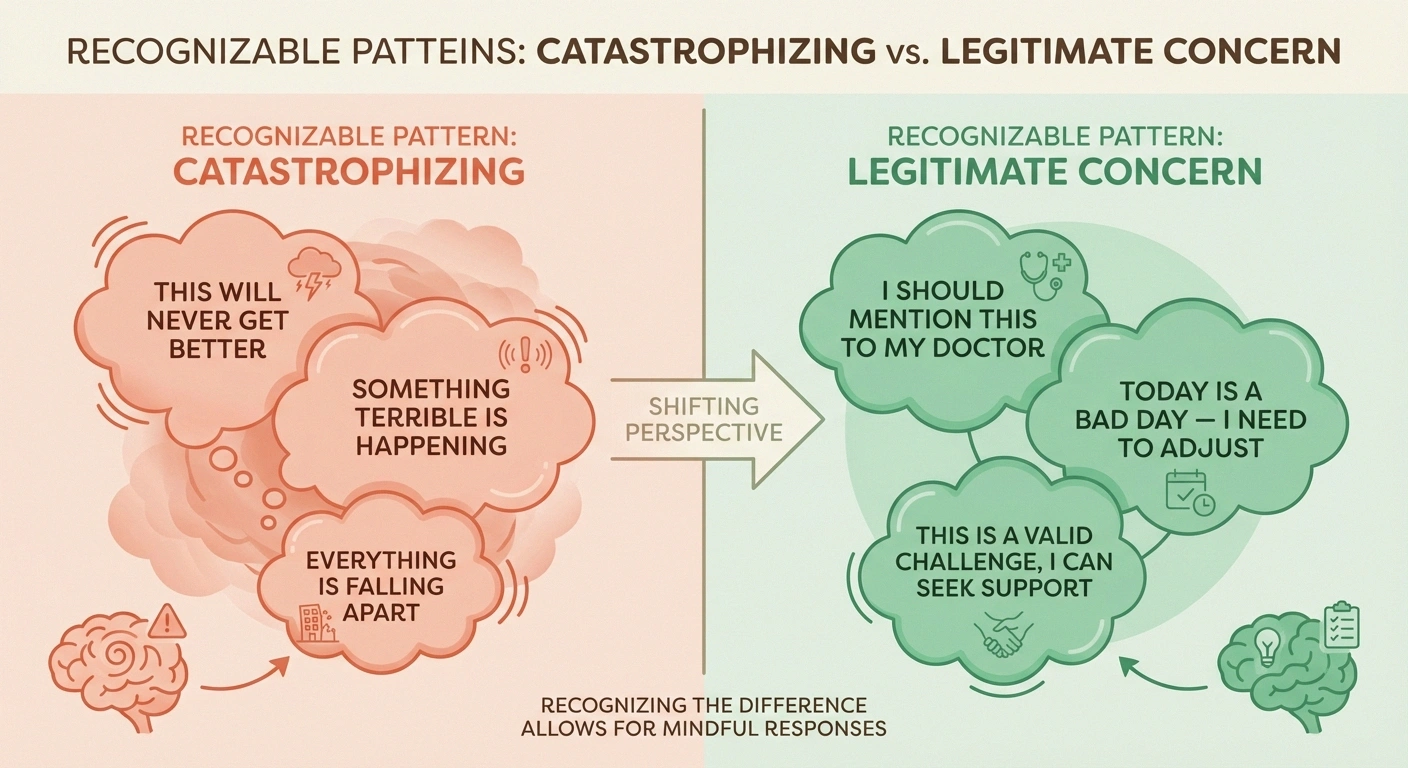
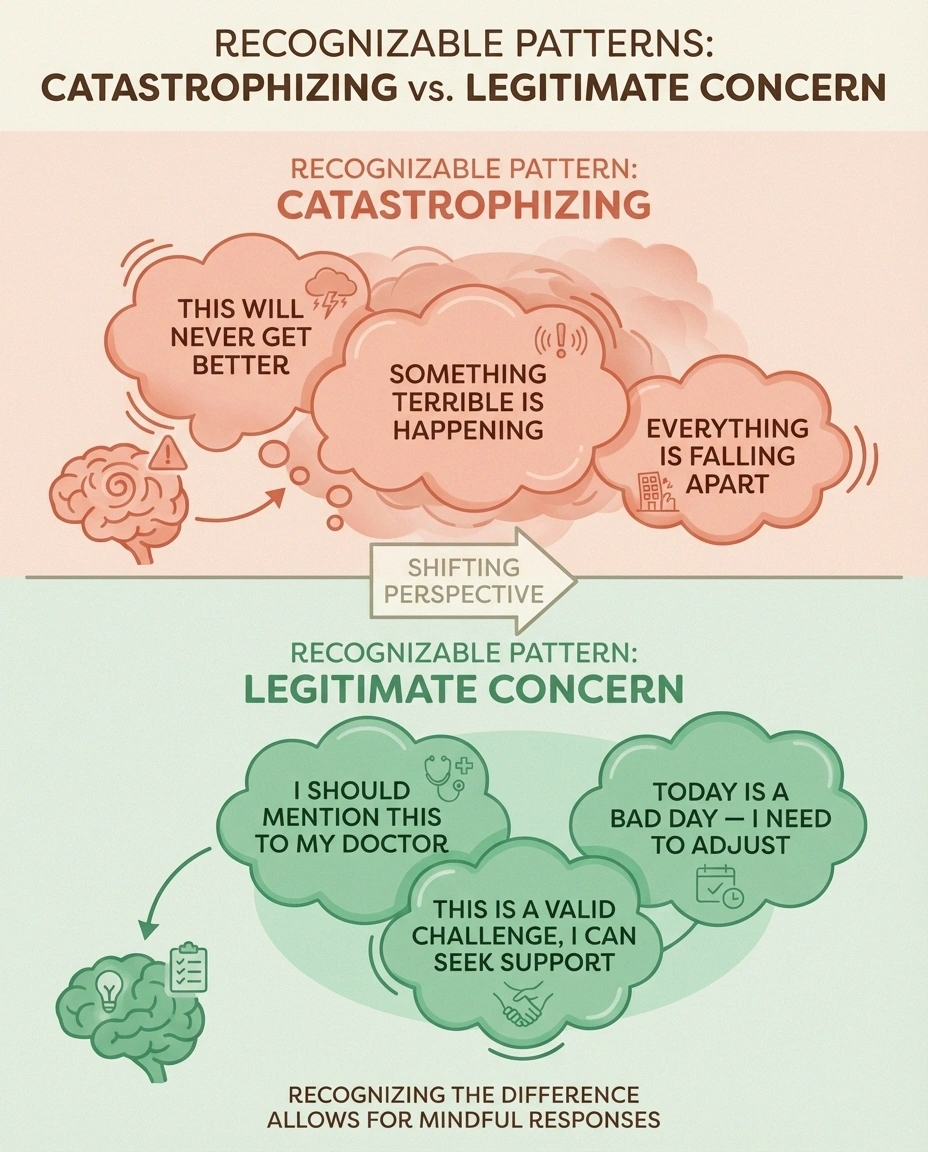
Here are the signatures of catastrophizing versus legitimate concern:
Catastrophizing sounds like:
- “This will never get better — it's only going to get worse”
- “I can't stand another minute of this”
- “Something terrible must be happening inside my body”
- “I'm going to end up completely disabled”
- “No one understands how bad this is”
- “There's nothing that can help me”
Legitimate concern sounds like:
- “This symptom is new — I should mention it to my doctor”
- “Today is a bad pain day. I need to adjust my plans”
- “I'm worried about progression and want to discuss it at my next appointment”
- “I need more tools for managing nighttime flares”
The key difference: legitimate concern leads to action. Catastrophizing leads to paralysis. If your thoughts are producing specific steps you can take, you're problem-solving. If your thoughts are spiraling without generating any actionable path forward, you're catastrophizing.
Breaking the Catastrophizing Cycle: Evidence-Based Strategies
Catastrophizing is a learned pattern, and like any learned pattern, it can be unlearned. Research consistently shows that pain catastrophizing is one of the most modifiable predictors of chronic pain outcomes. That means changing this one thing — how you mentally relate to your pain — may improve your experience more than any single medication.
Cognitive Defusion: Separating You from Your Thoughts
Cognitive defusion is a technique from Acceptance and Commitment Therapy (ACT) that doesn't try to change your catastrophizing thoughts — it changes your relationship with them. Instead of believing “this pain will never stop” as a fact, you learn to notice it as a thought: “I'm having the thought that this pain will never stop.”
Cognitive Defusion in Practice
Notice the Thought
“This pain will never stop” appears in your mind during a flare
Label It
“I notice I'm having the thought that this pain will never stop”
Observe, Don't Engage
The thought becomes a mental event you're watching — not a fact you're living. Your brain shifts from alarm mode to analytical mode.
This sounds trivially different, but the neurological effect is significant. When you observe a thought rather than fuse with it, you activate the prefrontal cortex (rational processing) and reduce activity in the amygdala (threat response). You're literally rerouting the thought from your alarm system to your analytical system.
Practice: When you notice a catastrophizing thought, mentally prefix it with “I notice I'm having the thought that…” Do this consistently and your brain begins to treat these thoughts as mental events rather than facts about reality.
Thought Records: Evidence Testing
Cognitive behavioral therapy uses thought records to systematically challenge catastrophizing. When a catastrophizing thought hits, you write down:
- The situation: What was happening when the thought started?
- The automatic thought: Exactly what went through your mind?
- Evidence FOR the thought: What objective facts support it?
- Evidence AGAINST the thought: What objective facts challenge it?
- A more balanced thought: What's a realistic way to see this situation?
Example: You wake up with burning feet and think “The nerve damage is spreading — I'm going to lose the ability to walk.”
- Evidence for: The burning feels more intense tonight. I've had neuropathy for two years and it has progressed.
- Evidence against: I've had nights this bad before that didn't mean progression. My last doctor's visit showed stable nerve function. Pain intensity varies from night to night naturally. Many people with neuropathy never lose the ability to walk.
- Balanced thought: “Tonight is a bad night. Bad nights happen. I'll mention it at my next appointment. Right now, I can use my foot soak routine and breathing exercises to manage it.”
Graded Exposure: Proving Yourself Wrong
Catastrophizing makes predictions: “If I walk more than ten minutes, the pain will be unbearable.” “If I go to the dinner party, I'll be miserable.” These predictions feel absolute, but they're often wrong — and the only way to weaken them is to test them.
Graded exposure means deliberately, incrementally testing your catastrophizing predictions. Walk for twelve minutes instead of ten. Go to the party for thirty minutes. Each time the predicted catastrophe doesn't materialize, the catastrophizing thought loses power.
Start small. The goal isn't to prove your pain is fake — it's very real. The goal is to prove that your worst-case predictions are consistently more extreme than what actually happens.
Mindfulness-Based Pain Management
Mindfulness interrupts catastrophizing at its root by training your brain to observe sensations without adding a narrative. Pain without catastrophizing is “intense burning in my feet right now.” Pain with catastrophizing is “intense burning in my feet right now AND this means something terrible AND it's going to get worse AND I can't handle it AND my life is ruined.”
Mindfulness-Based Stress Reduction (MBSR), specifically adapted for chronic pain, has strong evidence. A meta-analysis found that MBSR reduced pain catastrophizing scores significantly, with effects lasting months after the program ended. The body scan meditation technique is particularly effective for neuropathy — learning to observe tingling, burning, or numbness as sensations rather than threats.
Start with five minutes daily. Sit or lie comfortably. Focus on the sensations in your feet or hands — not trying to change them, not labeling them as good or bad, just noticing. “There's tingling. There's warmth. There's a prickling feeling.” When your mind jumps to interpretation (“this means my nerves are dying”), gently return to observation.
The Pain Toolkit: Building Your Emergency Kit
Catastrophizing thrives when you feel helpless. Having a concrete, pre-made plan for pain flares reduces helplessness and breaks the cycle before it starts. Your pain toolkit might include:
- A written card with your balanced thoughts (from thought records) that you can read during a flare
- A specific physical comfort routine (foot soak, topical cream, TENS unit, positioning)
- An audio file of a guided body scan meditation on your phone
- A distraction activity that works even during flares (podcast, audiobook, gentle hand exercises)
- Emergency contact information for a support person you can text or call
The toolkit works not just because of the individual items, but because having it means you're not scrambling during a crisis. The catastrophizing thought “there's nothing I can do” has a harder time taking hold when your pain toolkit is sitting on the nightstand.
When Catastrophizing Requires Professional Help
Self-help strategies work well for mild to moderate catastrophizing, but some situations call for professional support. Consider seeking help if:
When to Seek Professional Help
If catastrophizing thoughts dominate most of your day, you've stopped activities you could physically do because of fear, or you're using substances to manage the mental distress — a pain psychologist can provide targeted CBT or ACT training. Studies show catastrophizing scores drop significantly with 6-8 structured sessions.
- Catastrophizing thoughts are your dominant mental state most of the day
- You've stopped activities you could physically do because you're afraid of pain
- The catastrophizing is significantly affecting your relationships
- You're using alcohol, excessive medication, or other substances to manage the mental distress
- You experience panic attacks related to pain
- Depression or anxiety has become severe
A pain psychologist who understands neuropathy can provide structured CBT or ACT specifically tailored to your situation. This isn't about “talking about your feelings” in a vague way — it's targeted, skill-based training that changes measurable outcomes. Studies show that pain catastrophizing scores drop significantly with even 6-8 sessions of structured therapy, with corresponding improvements in pain intensity, sleep quality, and daily functioning.
What Your Support Network Needs to Know
Catastrophizing isn't something you chose, and “just think positive” isn't a solution — it actually makes things worse by adding guilt to the equation. If someone in your life tells you to “stop overthinking it,” they mean well but they don't understand the neuroscience involved.
❌ What Doesn't Help
“Just think positive” • “Stop overthinking it” • “Oh no, that's terrible!” • Trying to fix everything • Minimizing the pain experience
✓ What Actually Helps
“That sounds really hard” • Gentle reality-checking with evidence • Practical toolkit support • Patience with the unlearning process • Simply being present
What actually helps from the people around you:
- Validation without amplification: “That sounds really hard” acknowledges the experience without feeding the spiral. “Oh no, that's terrible, you must be so scared!” feeds it.
- Gentle reality-checking: “Remember how the last flare like this settled down after a few days?” This provides evidence against the catastrophizing thought without dismissing the pain.
- Practical support: Helping with the pain toolkit, reminding about coping strategies, or simply being present without trying to fix everything.
- Patience with the process: Unlearning catastrophizing takes time. The spiral will recur even after significant progress.
The Real Power: Changing Your Relationship with Pain
I want to be clear about what breaking the catastrophizing cycle does and doesn't mean. It doesn't mean your pain goes away. It doesn't mean you should ignore symptoms or stop reporting changes to your doctor. It doesn't mean the pain is “all in your head” — your nerve damage is real and your pain is real.

The Key Insight
Pain catastrophizing is one of the strongest predictors of how well someone functions with chronic pain — stronger than pain severity itself. That means the single most powerful lever you have for improving your life with neuropathy may be learning to think differently about what your nerves are telling you. Your pain is real. And so is your power to change your relationship with it.
What it means is this: without catastrophizing layered on top, your experience of neuropathy becomes more manageable. The pain itself may even decrease, because you've interrupted the neurological amplification loop. The anxiety that comes with every new sensation calms down. Sleep improves. You start doing things you'd been avoiding. Your world, which had been shrinking around the pain, begins to expand again.
Pain catastrophizing is one of the strongest predictors of how well someone functions with chronic pain — stronger than the severity of the pain itself. That means the single most powerful lever you have for improving your life with neuropathy may not be a medication or a supplement. It may be learning to think differently about what your nerves are telling you.
Frequently Asked Questions
Is pain catastrophizing my fault?
No. Pain catastrophizing is a natural neurological response to chronic pain, not a character flaw or a choice. Your brain developed these thought patterns as a threat detection strategy. While it is a learned response that can be modified with practice, blaming yourself for catastrophizing only adds another layer of distress. The goal is to recognize the pattern and develop tools to interrupt it, not to judge yourself for having it.
Can catastrophizing actually make my nerve damage worse?
Catastrophizing may not directly worsen nerve damage, but it worsens everything around it. The stress response triggered by catastrophizing increases cortisol and systemic inflammation, which can impede nerve healing and worsen pain sensitivity. It also leads to poor sleep, reduced physical activity, and social withdrawal — all of which are independently associated with worse neuropathy outcomes. So while it may not damage nerves directly, it creates conditions where nerve damage is harder to manage and recovery is slower.
How is this different from anxiety about my neuropathy?
There is significant overlap, but they are distinct. Anxiety is a general state of worry and hyperarousal that may cover many topics beyond pain. Pain catastrophizing is specifically focused on magnifying, ruminating about, and feeling helpless about pain. You can have neuropathy-related anxiety without catastrophizing, and you can catastrophize about pain without meeting criteria for an anxiety disorder. However, they frequently co-occur and feed each other. The treatment approaches overlap too — CBT and mindfulness help with both.
Will my doctor take me seriously if I bring up catastrophizing?
Any good pain doctor or neurologist will take this very seriously. Pain catastrophizing is one of the most studied and validated concepts in pain medicine. Bringing it up shows you are informed and engaged in your treatment. If your doctor dismisses it or suggests it means your pain is not real, that is a red flag about their understanding of modern pain science. Pain catastrophizing is a neurological pattern that amplifies real pain — it does not mean the pain is imaginary.
What is the best first step to reducing catastrophizing?
Start by noticing the pattern without trying to change it. For one week, simply observe when catastrophizing thoughts arise and write them down. Note what triggered them, what time of day they happen, and how intense the pain was at the time. This observation alone begins the process of defusion — separating you from the thought. After a week of tracking, you will likely see patterns that make the thoughts feel more predictable and less overwhelming, which is the foundation for every other strategy.
Can medications help with catastrophizing?
No medication directly targets catastrophizing, but medications that reduce overall pain intensity or treat co-occurring depression and anxiety can lower the fuel that feeds catastrophizing. Duloxetine and pregabalin, commonly prescribed for neuropathic pain, also have mood-stabilizing effects that may help. However, the most effective approach according to research is a combination of medication for pain management AND psychological strategies like CBT or ACT for the catastrophizing pattern itself. One without the other leaves part of the problem unaddressed.


