When I first heard the term “blood-nerve barrier” at a neurology appointment, I'll be honest — I nodded along and pretended I understood. I went home, sat down with a cup of tea, and Googled it the way I Google most medical things these days: skeptically, slowly, and with one eye on whether the explanation made any actual sense.
What I found surprised me. There's a real, physical barrier inside your peripheral nerves — a kind of biological gatekeeper — and it does some very specific work to keep your nerve fibers safe from whatever happens to be floating around in your bloodstream. Most of the time, you'll never know it exists. But when it breaks down — and it breaks down in a lot of the conditions we talk about on this site — that quiet barrier failure is part of why nerves get hurt.
This article is the friendly, plain-language version of what I wish someone had handed me back then. We'll look at what the blood-nerve barrier actually is, how it normally protects you, and what goes wrong when it stops doing its job — especially in diabetic neuropathy, autoimmune conditions like Guillain-Barré and CIDP, and chemo-induced nerve damage.
What Is the Blood-Nerve Barrier?
The blood-nerve barrier — often shortened to BNB — is a specialized layer of cells inside your peripheral nerves that controls what's allowed to pass from your bloodstream into the protected environment around your nerve fibers.
Key Takeaway
The blood-nerve barrier (BNB) is the second most restrictive vascular system in your body — a microscopic gatekeeper that protects peripheral nerves from circulating toxins, immune cells, and inflammation. When it leaks, nerve damage follows. Understanding it changes how you think about neuropathy management.
If you've ever heard of the blood-brain barrier, the BNB is its less-famous cousin. They do similar work in different places. The blood-brain barrier protects the brain and spinal cord. The blood-nerve barrier protects the peripheral nerves — the ones that run out into your arms, legs, hands, and feet. After the blood-brain barrier, the BNB is the second most restrictive vascular system in the human body.
Why does the body bother with such a barrier at all? Because peripheral nerves are extraordinarily delicate. They need a very specific chemical environment to function — the right balance of ions, the right amount of water, the right nutrients, and crucially, an environment that's mostly walled off from the immune system. Your bloodstream is busy and chaotic. It carries everything from oxygen and glucose to immune cells, hormones, antibodies, and the occasional toxin. Most of that traffic should never come anywhere near a nerve fiber.
The BNB is the gatekeeper that decides what gets through.
How the BNB Protects Your Nerves Day to Day

On a normal Tuesday afternoon, when you're not thinking about your nerves at all, the BNB is doing several jobs at once.
It's regulating the flow of ions — sodium, potassium, calcium — because nerve signaling depends on a precise ionic balance inside the nerve fiber's protected space (called the endoneurium). It's controlling water movement so the nerve doesn't swell or shrivel. It's letting in the nutrients nerves need (like glucose and amino acids) while keeping out larger molecules that don't belong. And it's actively excluding most immune cells — the lymphocytes and macrophages that patrol the rest of your body — because nerves and the immune system have an uneasy relationship that works best when they stay apart.
This last part is important and often misunderstood. Nerves are what immunologists call “immune-privileged” tissue. That doesn't mean the immune system never visits — it does, in small numbers, for surveillance. It means that under normal circumstances, the BNB keeps the volume turned way down. Antibodies, complement proteins, and inflammatory cells stay mostly on the bloodstream side of the wall.
When the system works, you don't notice it. When it fails, you notice in the form of pain, numbness, weakness, or progressive nerve damage.
The Architecture: Tight Junctions, Endothelial Cells, and the Inner Sanctum
Let's get a little more specific about what the barrier actually is, because the architecture matters for understanding why it fails.
How the Blood-Nerve Barrier Is Built
1. Endoneurial Microvessels
Tiny capillaries thread through the inside of each peripheral nerve, supplying oxygen and nutrients to nerve fibers.
2. Endothelial Cells with Tight Junctions
Specialized cells line those vessels, sealed together by tight junction proteins like ZO-1 and claudins — the molecular weatherstripping of the barrier.
3. The Endoneurium: The Inner Sanctum
The protected nerve fiber environment inside, kept chemically stable and mostly isolated from immune-system traffic.
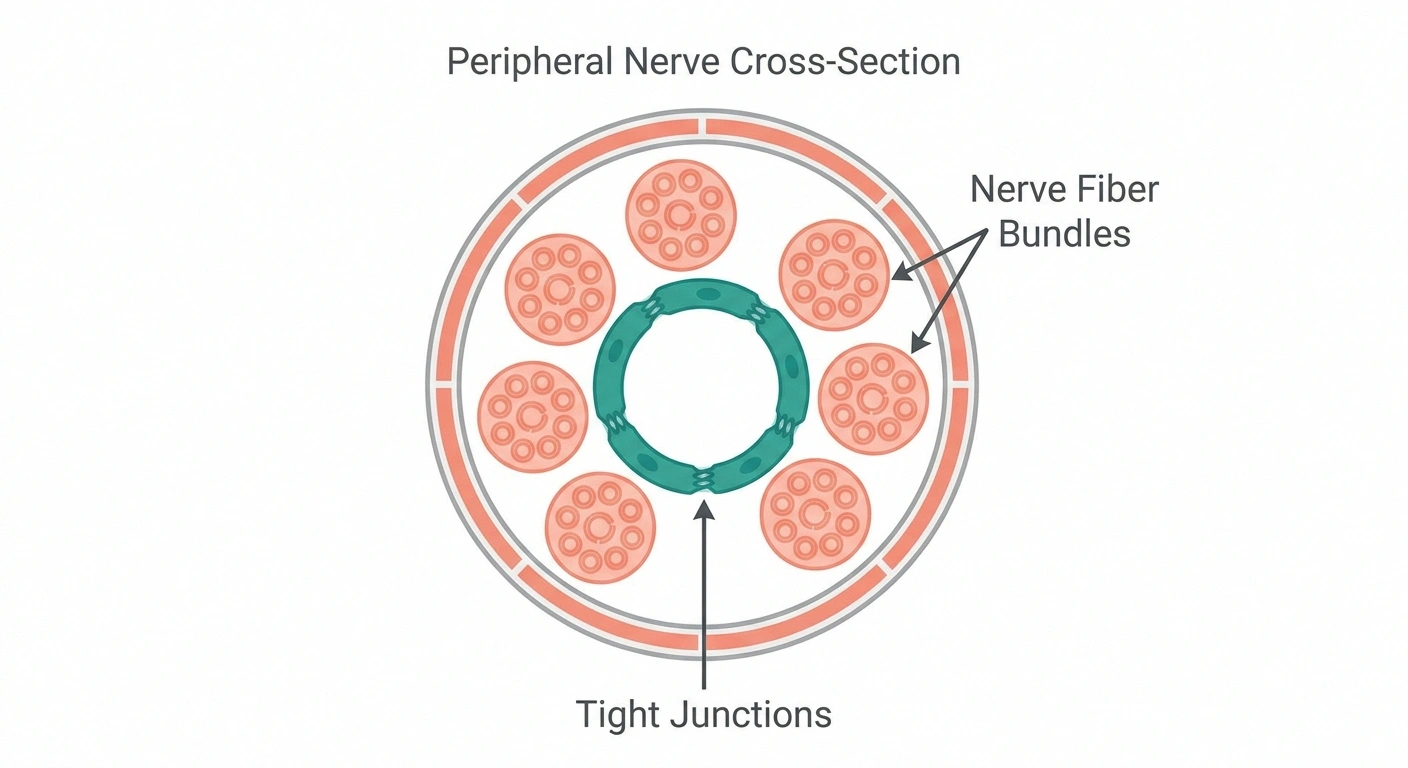
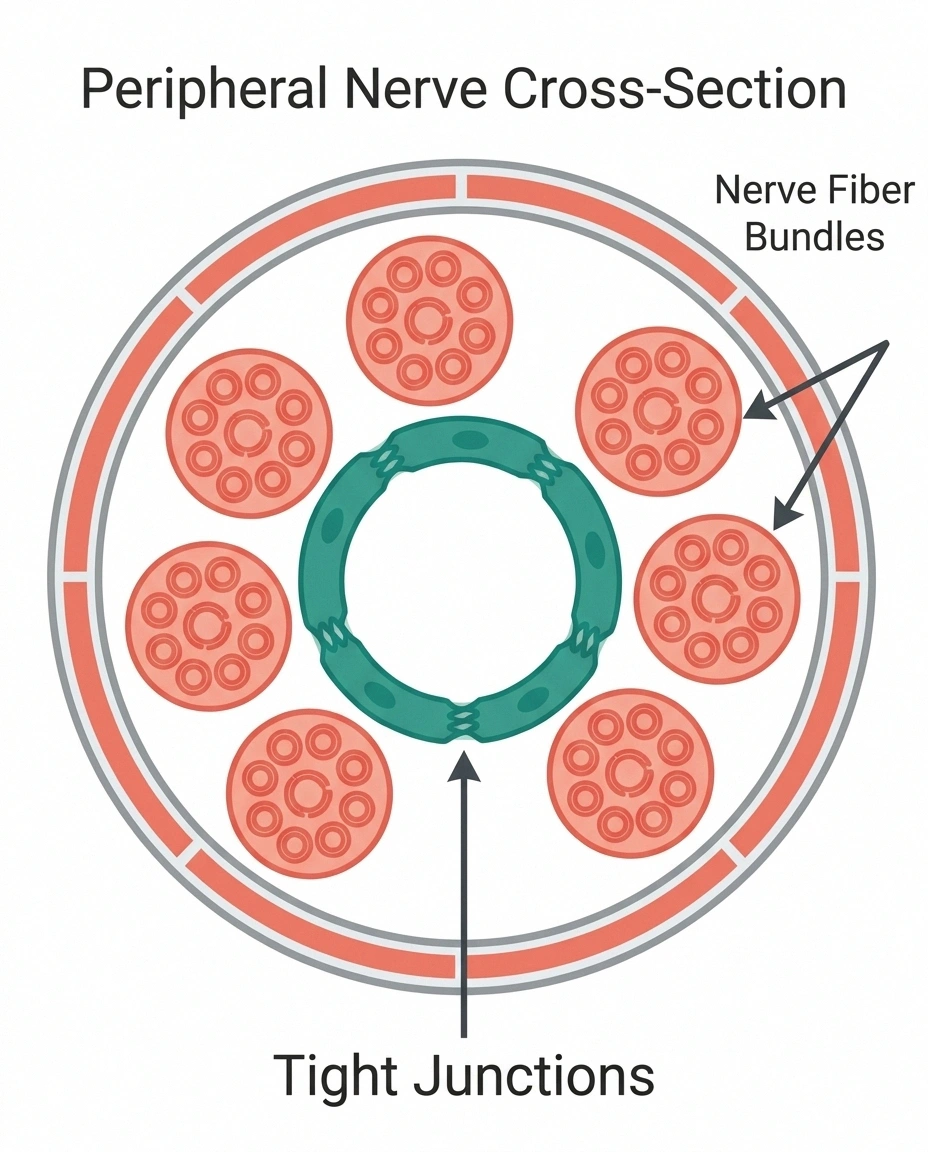
The BNB is built from specialized blood vessels called endoneurial microvessels — tiny capillaries that thread through the inside of each peripheral nerve. The cells lining these vessels (endothelial cells) are bound to each other by structures called tight junctions. Think of tight junctions as the molecular equivalent of weatherstripping — they seal the gaps between adjacent cells so that nothing can sneak through the spaces.
The proteins that build these tight junctions have names you may run across in research papers: ZO-1 (zonula occludens-1), the claudins, occludins, and a few others. When researchers talk about the BNB being “intact,” they mean these tight junction proteins are present, properly arranged, and doing their sealing work. When they talk about BNB “leakage” or “breakdown,” they mean those proteins have been damaged, downregulated, or pulled apart — and substances that should stay outside are now getting through.
One key thing to understand: the BNB is thinner than the blood-brain barrier. It has fewer protective layers and a less elaborate cellular architecture. That sounds like a small detail, but it has big consequences. It means peripheral nerves are more vulnerable to systemic insults than the brain is. When something nasty starts circulating in your blood — high blood sugar, autoantibodies, chemotherapy drugs — the BNB is the thinner wall that gives way first. This is part of why so many diseases that don't touch the brain still cause peripheral nerve damage.
How Diabetes Damages the Blood-Nerve Barrier

BNB breakdown plays a pivotal role in diabetic neuropathy, and it's one of the most studied examples of barrier failure causing nerve injury.
🔎 Research Says
Studies published in Frontiers in Neuroscience and other journals describe BNB breakdown as a pivotal mechanism in diabetic neuropathy. Tight junction protein downregulation and endothelial dysfunction allow glucose-derived toxins, inflammatory cytokines, and immune cells to reach nerve fibers directly — accelerating damage that begins long before symptoms appear.
Here's the simplified version of what the research describes. When blood sugar runs chronically high, several things start to happen to the small blood vessels of the body — and the endoneurial microvessels that form the BNB are no exception. The endothelial cells lining those vessels develop what's called endothelial dysfunction: they don't make as much nitric oxide (which normally keeps blood vessels relaxed and healthy), they accumulate damage from oxidative stress, and they become “stickier” to inflammatory cells.
Over time, the tight junction proteins that hold the barrier together get downregulated and disorganized. The wall develops gaps. Once that happens, things that should never have access to the nerve fiber environment — glucose-derived toxic compounds called advanced glycation end products (AGEs), inflammatory cytokines, and immune cells — start to leak through.
This is part of why diabetic neuropathy is so insidious. It's not a single sudden injury to a nerve. It's a slow, low-grade contamination of the protected nerve environment, day after day, for years. By the time symptoms become impossible to ignore, the BNB has often been leaky for a long time, and nerve fibers have been bathed in a more toxic environment than they were ever meant to handle.
Understanding this helps explain why blood sugar control matters so much, and why interventions aimed at reducing oxidative stress (like alpha-lipoic acid) and supporting vascular health are part of so many neuropathy management discussions. They're not just treating symptoms — they're targeting the upstream barrier failure.
Autoimmune Attacks: When the BNB Fails in GBS and CIDP

Diabetic BNB failure is slow and chronic. The autoimmune neuropathies — Guillain-Barré syndrome (GBS) and chronic inflammatory demyelinating polyneuropathy (CIDP) — show a different pattern: more dramatic, more rapid, and driven by the body's own immune system attacking its own nerves.
Blood-Nerve Barrier vs. Blood-Brain Barrier: A Quick Comparison
| Feature | Blood-Brain Barrier (BBB) | Blood-Nerve Barrier (BNB) |
|---|---|---|
| Protects | Brain and spinal cord | Peripheral nerves |
| Restrictiveness | Most restrictive | Second most restrictive |
| Wall thickness | Multiple protective layers | Thinner, fewer layers |
| Vulnerability | More resistant to systemic insults | More vulnerable to circulating toxins |
| Common failure causes | Stroke, MS, infection, trauma | Diabetes, autoimmunity, chemo, injury |
In these conditions, research published in journals like Frontiers in Neuroscience has shown that tight junction proteins (TJPs) get downregulated and the BNB becomes leaky. Once that happens, the immune system gains access to nerve tissue it was never supposed to reach. Autoantibodies — the immune system's misdirected weapons against the body's own tissues — flood through the breached barrier and attack the myelin sheath or the nerve fibers themselves.
In Guillain-Barré, this happens fast. A patient may go from feeling fine to severe weakness within days or a couple of weeks. In CIDP, the same kind of process happens more slowly and recurrently — symptoms develop over months, often relapsing. Researchers studying CIDP have found measurable changes in BNB structure and permeability, suggesting the barrier failure isn't just a side effect of the autoimmune attack — it's part of the mechanism that lets the attack happen at all.
This insight is why treatments for GBS and CIDP often involve calming down the immune system itself (with intravenous immunoglobulin or plasma exchange, for example). If you can quiet the autoimmune storm, you give the BNB a chance to repair itself and reseal the nerves' protected environment.
Other Causes of BNB Breakdown
Diabetes and autoimmune conditions aren't the only ways the blood-nerve barrier can fail. There's a longer list of insults that can punch through it.
Don't Self-Diagnose BNB Damage
There is no routine clinical test for blood-nerve barrier permeability. Doctors infer barrier involvement from the underlying condition and symptom pattern — not from a lab value. Use this concept to ask better questions at appointments, not to diagnose yourself or skip professional evaluation.
Chemotherapy-induced neuropathy. Several chemo drugs — particularly platinum-based agents like cisplatin and oxaliplatin, plus the taxanes and vincristine — can damage the endothelial cells of the BNB. This is part of why CIPN develops in so many patients. The drug doesn't have to enter the nerve directly; it can do its damage by compromising the barrier and letting the chemo (and other circulating substances) reach nerve fibers.
Traumatic nerve injury. When a nerve is physically damaged — by an accident, a surgical complication, or sustained compression — the BNB at the injury site is breached almost immediately. This is normal and even necessary for healing (immune cells need access to clear debris and coordinate repair). But it also means that during the recovery window, the nerve environment is unusually exposed.
Inflammatory and infectious neuropathies. Conditions where the body mounts a strong inflammatory response — including some viral and bacterial infections that can cause neuropathy — disrupt BNB function. The same is true of vasculitic neuropathies, where the small blood vessels themselves are inflamed.
Toxic exposures. Heavy metals, certain solvents, and some medications can damage BNB endothelial cells directly. Even chronic alcohol use, over many years, has effects on the small blood vessels that maintain the barrier.
What ties all of these together is the same basic story: the wall comes down, and substances that should stay out get in. Once that happens, nerve damage becomes much harder to prevent.
What This Means for Treatment and Prevention

The blood-nerve barrier is a relatively young area of neurology research, and treatments aren't yet packaged the way “take this pill for BNB repair” might suggest. But the concept has real implications for how we think about neuropathy management.
First, it reframes the question of whether neuropathy can be reversed. Some forms of nerve damage are extremely difficult to undo because the nerve fibers themselves have been lost. But BNB function can recover under the right conditions — when the underlying insult is removed and the inflammatory drivers are calmed. That's why early, aggressive management of the upstream cause (controlling blood sugar in diabetes, suppressing autoimmunity in CIDP, supporting recovery after chemo) matters so much.
Second, it explains why “vascular health” keeps coming up in neuropathy conversations even though the disease is about nerves. The BNB is a vascular system. Anything that supports endothelial health — managing blood pressure, reducing inflammation, maintaining good blood sugar control, not smoking, regular movement — supports the barrier that protects the nerves.
Third, it explains why supplements that target oxidative stress and endothelial function are part of so many neuropathy management strategies. Alpha-lipoic acid, B vitamins, acetyl-L-carnitine, and others have been studied not just for their direct effects on nerve fibers, but for their potential effects on the small blood vessels that feed and protect those nerves.
Living With This Knowledge: What You Can Actually Do

Reading about a microscopic structure failing inside your peripheral nerves can feel a little hopeless. Like, what am I supposed to do — fix my own tight junctions over breakfast? Of course not. But here's what understanding the BNB has helped me do, both for myself and in conversations with friends managing their own neuropathy.
Practical Steps That Support Barrier Health
Tighten blood sugar control — every spike contributes to slow barrier breakdown in diabetic neuropathy.
Manage blood pressure and inflammation — the BNB is a vascular system, so anything that supports vessel health supports the barrier.
Move daily, don't smoke, and limit alcohol — all three protect endothelial function across your whole vascular system.
Ask about the inflammatory side of your case — discuss with your doctor whether autoimmune or inflammatory factors are driving your neuropathy.
None of these replace medical care — they support the system around it.
I stopped thinking of nerve damage as just “the nerves” and started thinking about the system that supports them. When I'm reading about a new treatment or supplement, I now ask: does this support the vascular health that maintains the barrier? Or is it only addressing the downstream nerve fiber? Both matter, but the upstream interventions tend to be the ones that have the best long-term outlook.
I take blood sugar control more seriously, even on the days I don't feel like it. Knowing that every spike contributes to the slow breakdown of a real, physical barrier inside my nerves changes my relationship with my food choices. It's not abstract anymore.
I asked my doctor about the inflammatory side of my situation. Not in a pushy way — just an honest “is there anything we should be looking at on the inflammation side?” Sometimes the answer is yes, sometimes no, but it's a real and reasonable question for anyone with a neuropathy that has an inflammatory or autoimmune component.
I stopped looking for a single magic bullet. The BNB story makes it clear that nerve health is the result of many systems working together — vascular, immune, metabolic, neurological. That's also why the management plans that work tend to look like a combination: blood sugar plus blood pressure plus movement plus targeted supplements plus, sometimes, medication. It's frustrating to have no single answer. But it's also liberating, because it means there are many small levers to pull.
One last thing. The blood-nerve barrier is also part of why conditions affecting the myelin sheath and conditions affecting small nerve fibers can both stem from similar upstream barrier failures, even though the resulting symptoms feel completely different. And it's part of why the relationship between neuropathy and the immune system deserves careful attention. These aren't separate problems — they're different consequences of the same underlying gatekeeper losing its grip.
Knowing this hasn't fixed my nerves. But it has made me a more thoughtful patient, a better question-asker at appointments, and a slightly less anxious person when a new symptom shows up. And honestly? In a chronic condition, that's not nothing.
Frequently Asked Questions
What is the blood-nerve barrier in simple terms?
The blood-nerve barrier is a layer of specialized cells inside your peripheral nerves that controls what passes from your bloodstream into the protected environment around your nerve fibers. It works like a gatekeeper, letting nutrients in while keeping out most immune cells, large molecules, and toxins. After the blood-brain barrier, it is the second most restrictive vascular system in the human body, and it is essential for keeping your peripheral nerves working properly.
How does diabetes damage the blood-nerve barrier?
Chronically high blood sugar damages the small blood vessels that make up the blood-nerve barrier. The endothelial cells lining those vessels develop what is called endothelial dysfunction, the tight junction proteins that seal the barrier get downregulated, and the wall becomes leaky over time. Once the barrier fails, glucose-derived toxic compounds, inflammatory molecules, and immune cells reach nerve fibers directly, contributing to the slow nerve damage we see in diabetic neuropathy.
Can the blood-nerve barrier repair itself?
Yes, the blood-nerve barrier can recover under the right conditions. When the underlying insult is removed or controlled, such as bringing blood sugar into target range, calming an autoimmune attack, or finishing a course of chemotherapy, the endothelial cells can reorganize and tight junction proteins can be restored. Recovery is not always complete, especially after long-standing damage, but the barrier is not a one-way door. This is part of why early intervention in neuropathy matters so much.
What is the difference between the blood-brain barrier and the blood-nerve barrier?
The blood-brain barrier protects the central nervous system, including the brain and spinal cord, while the blood-nerve barrier protects the peripheral nerves that run to your arms, legs, hands, and feet. Both work the same way in principle, using tight junctions between specialized blood vessel cells. The key difference is that the blood-nerve barrier is thinner, with fewer protective layers, which makes peripheral nerves more vulnerable to circulating toxins, high blood sugar, and autoimmune attacks than the brain is.
Why does chemotherapy cause nerve damage through the blood-nerve barrier?
Several chemotherapy drugs, especially platinum-based agents like cisplatin and oxaliplatin, taxanes, and vincristine, can damage the endothelial cells that form the blood-nerve barrier. When the barrier is compromised, the chemo drug and other circulating substances can reach nerve fibers more directly than they normally would. This is part of why chemotherapy-induced peripheral neuropathy develops in so many cancer patients, sometimes during treatment and sometimes only after treatment ends.
How is the blood-nerve barrier involved in Guillain-Barré syndrome and CIDP?
In both Guillain-Barré syndrome and chronic inflammatory demyelinating polyneuropathy, research has shown that tight junction proteins are downregulated and the blood-nerve barrier becomes leaky. Once the barrier fails, autoantibodies and immune cells reach the nerves and attack the myelin sheath or the nerve fibers themselves. Treatments like intravenous immunoglobulin and plasma exchange work in part by calming the immune attack and giving the barrier a chance to repair, allowing nerves to recover.
Are there supplements that help the blood-nerve barrier?
No supplement is FDA-approved to treat blood-nerve barrier dysfunction directly, but several supplements that have been studied for neuropathy may support the vascular and antioxidant systems that maintain the barrier. Alpha-lipoic acid is the most studied for its effects on oxidative stress and endothelial function. B vitamins, acetyl-L-carnitine, and others have also been investigated. Always discuss supplements with your doctor or pharmacist before starting them, especially if you take prescription medications.
Can I get tested to see if my blood-nerve barrier is leaky?
There is no routine clinical test that measures blood-nerve barrier permeability the way you might measure blood pressure or cholesterol. Researchers can study the barrier using nerve biopsy and specialized imaging, but these are not part of standard care for most people with neuropathy. Doctors infer that the barrier may be involved based on the type of neuropathy, the underlying condition, and the pattern of symptoms. Self-diagnosing barrier dysfunction is not useful, but understanding the concept can help you have richer conversations with your medical team.