There's a particular kind of evening I know well, because I've lived it and I've sat with dozens of people in my support group who have too. You've had your blood drawn for a neuropathy workup. The results land in your patient portal at 9 p.m., days before your follow-up appointment. And there it all is — a wall of three-letter abbreviations, numbers, and little flags that say “H” or “L” next to things you've never heard of. So you do what any of us would do: you start typing them into a search bar at midnight, and an hour later you're more frightened and no clearer.
This article is meant to be the thing I wish someone had handed me that night. I'm going to walk you through what's typically on a neuropathy blood panel, what each test is actually hunting for, and what an abnormal number might point toward — in plain language. One firm promise and one firm boundary up front: I'll help you understand the map, but I am a fellow patient and advocate, not a doctor. These results have to be interpreted in the context of your history and exam, by your clinician. Reading along here is meant to make that conversation sharper, not to replace it.
First, the Reframe That Changes Everything
Here is the single most important thing to understand before you look at a single number: blood tests do not diagnose neuropathy. They don't show nerve damage. The diagnosis of neuropathy itself comes from your symptoms, a neurological exam, and often nerve testing like an EMG and nerve conduction study — we explain that whole process in our guide to how neuropathy is diagnosed.
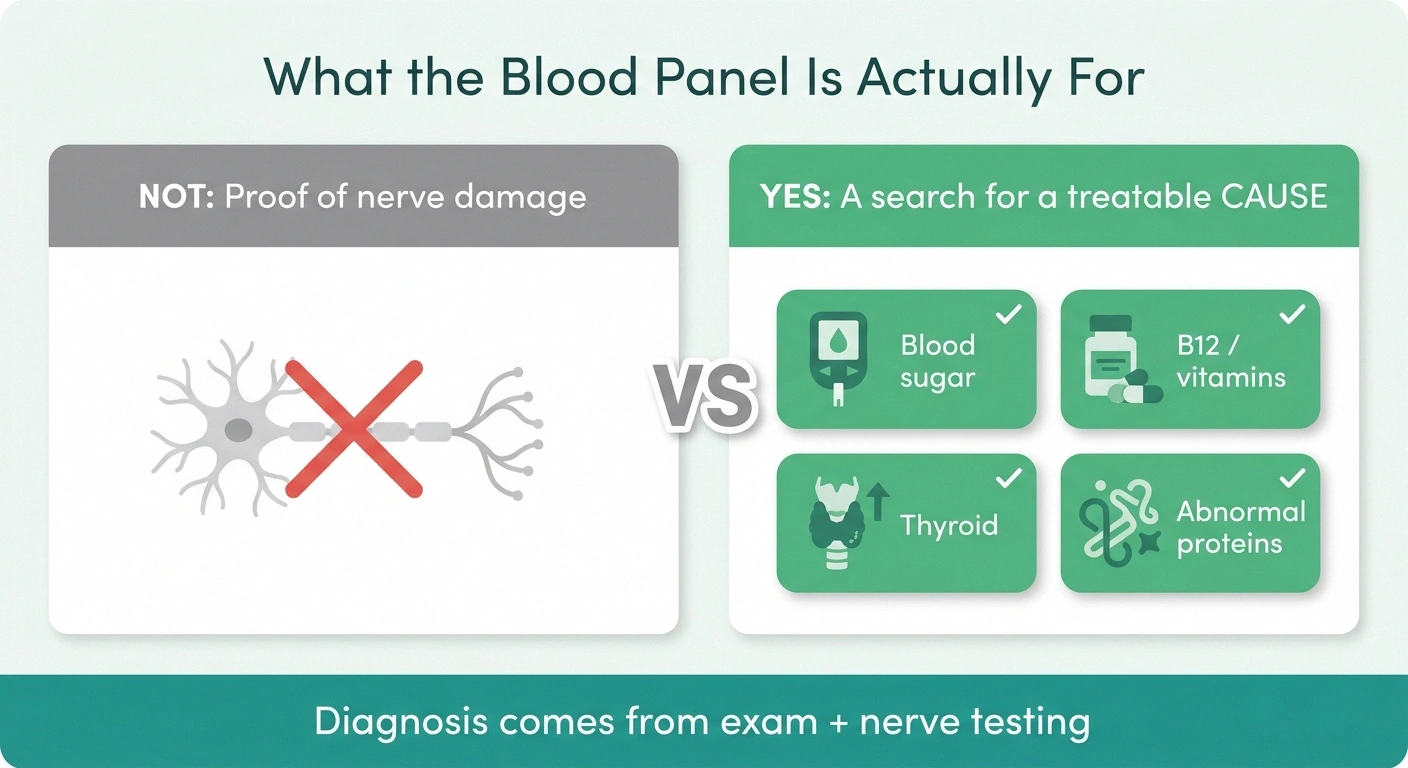
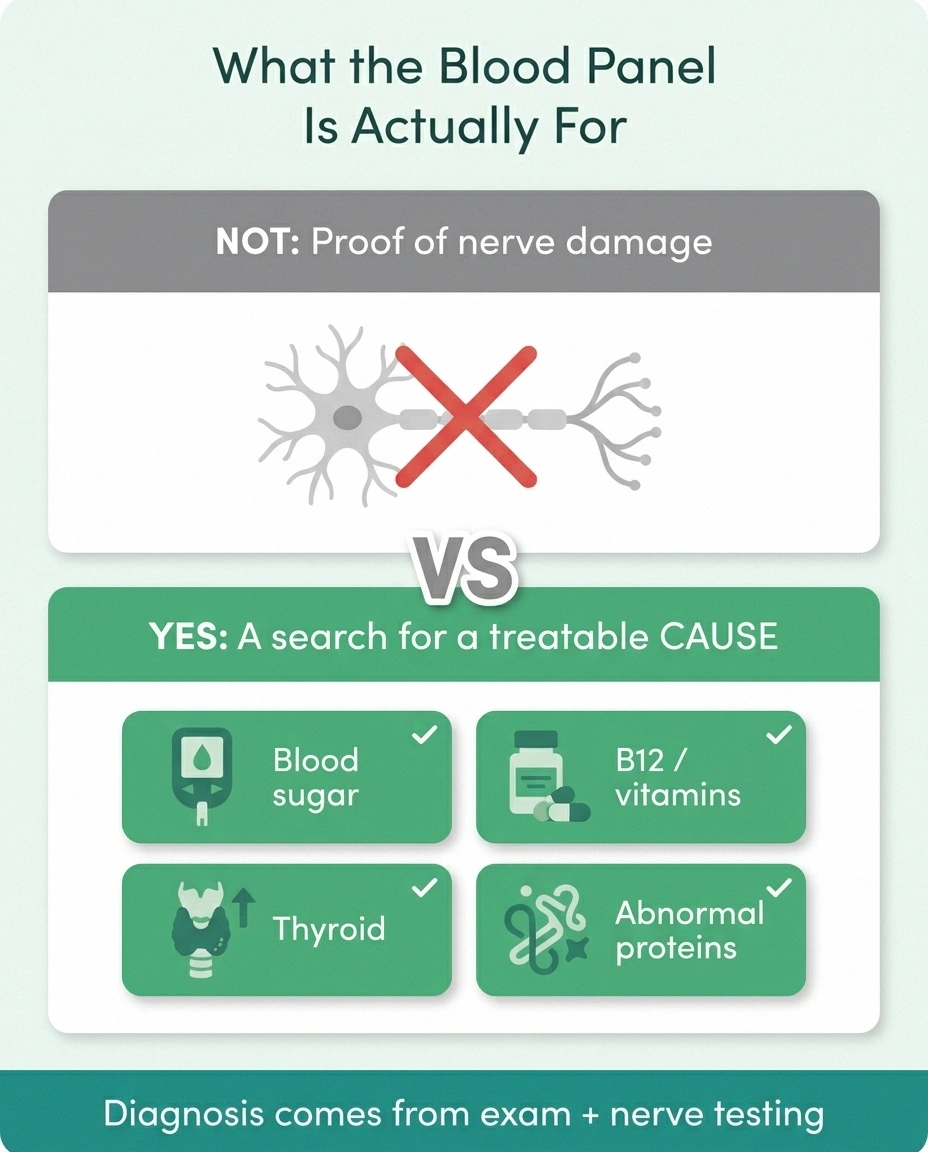
The panel hunts for a treatable cause — it doesn't diagnose neuropathy
Diagnosis comes from your symptoms, exam, and nerve testing. Ask of every line: “What treatable cause is this looking for?” That turns a wall of numbers into a checklist instead of a verdict.
So what is all this blood work for? It's a search for the cause. Many things that damage nerves leave a fingerprint in the blood — high blood sugar, a vitamin deficiency, a thyroid problem, an abnormal protein, an autoimmune signal. Some of those causes are treatable, and a few are reversible if caught early. That's the whole point of the panel: not to confirm you have neuropathy (you and your doctor likely already suspect that), but to find a reason that can be acted on. When you look at your results through that lens — “what treatable cause is this hunting for?” — the wall of numbers turns into a checklist instead of a verdict.
Blood Sugar: A1c, Fasting Glucose, and the Test That Catches What They Miss

Diabetes is the most common cause of peripheral neuropathy in countries like ours, so blood sugar tests are almost always front and center. You'll usually see two: a fasting glucose (a single snapshot of your blood sugar that morning) and hemoglobin A1c, which estimates your average blood sugar over roughly the past three months. An elevated A1c suggests diabetes or, in the borderline range, prediabetes.
Nerve damage can begin during the prediabetic stage, when A1c and fasting glucose still read normal. A 2-hour oral glucose tolerance test can catch the impaired glucose tolerance those tests miss. If your sugar tests are borderline and no one has mentioned it, that's a fair, specific question to bring.
Here's the nuance that genuinely matters and that a lot of people miss: a normal A1c and fasting glucose do not fully rule out blood sugar as the culprit. There's a well-recognized pattern where nerve damage appears during the prediabetic stage, when standard tests still look fine. That's why, when suspicion is high, some clinicians order a 2-hour oral glucose tolerance test — you drink a measured sugar solution and they check your blood sugar two hours later. It catches impaired glucose tolerance that A1c can sail right past. We dig into this exact gap in our article on prediabetes and neuropathy, and into the bigger picture in our overview of diabetic neuropathy. If your sugar tests are borderline and no one has mentioned a glucose tolerance test, that's a fair, specific question to bring to your appointment.
Vitamin B12 — and Why the Number Alone Can Fool You
B12 deficiency is one of the genuinely treatable causes of neuropathy, which is why it's on essentially every panel. But B12 is also the test most likely to mislead you if you read it in isolation, so this section is worth slowing down for.
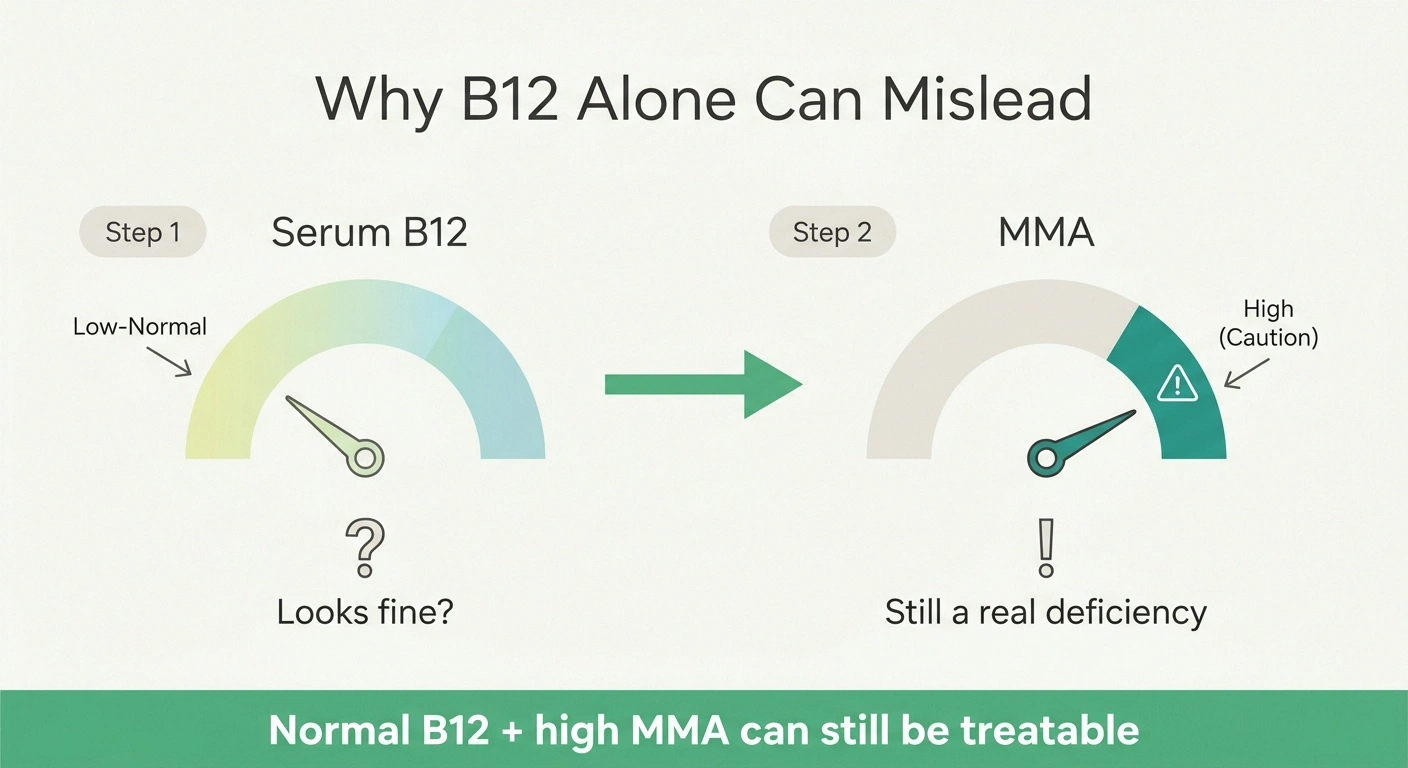
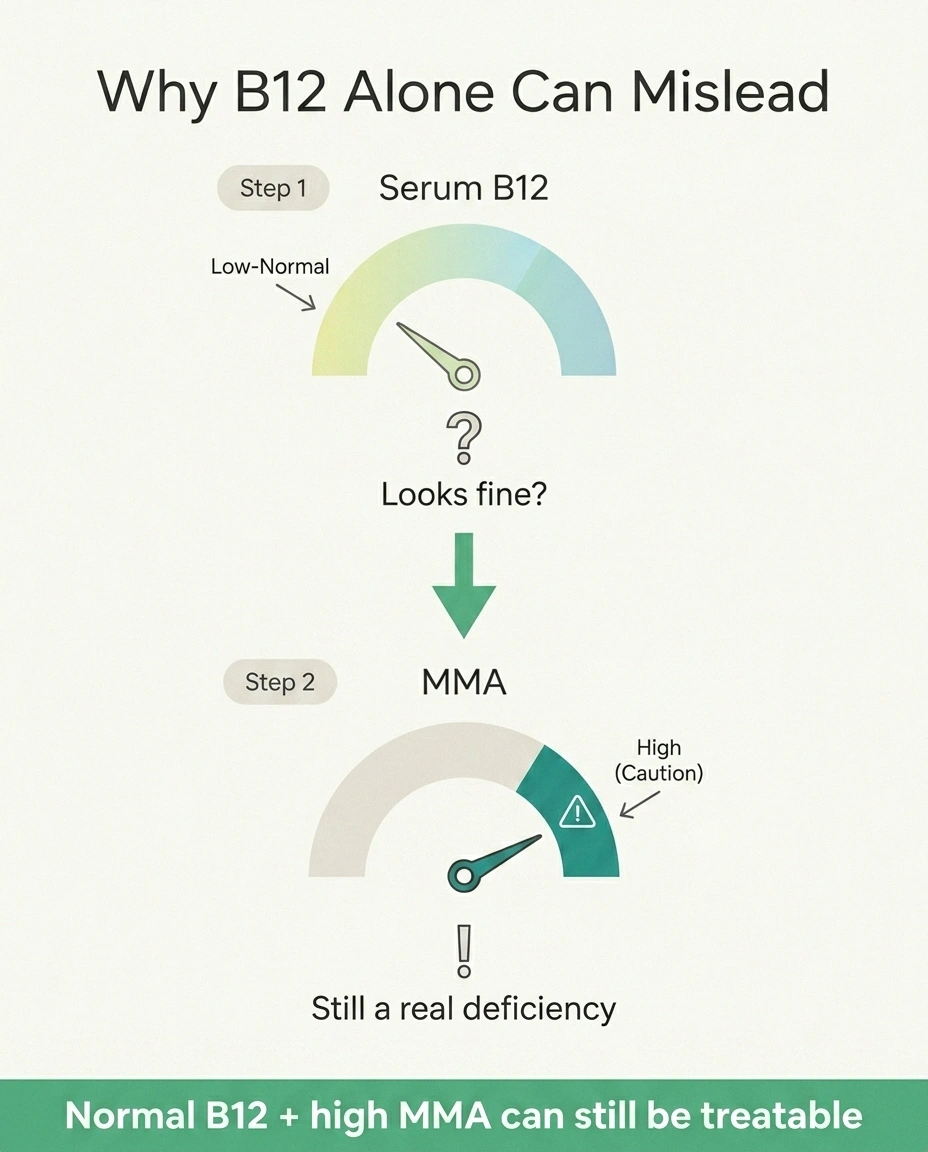
A “low-normal” serum B12 can still be a functional deficiency at the tissue level. An elevated methylmalonic acid (MMA) — and sometimes homocysteine — is what confirms it. A normal B12 with a high MMA can still mean a meaningful, treatable problem.
A serum B12 result that sits in the “low-normal” range can still represent a functional deficiency at the level where it matters — inside your cells and nerves. To see past that, doctors add a test called methylmalonic acid (MMA), and sometimes homocysteine. When B12 is truly insufficient at the tissue level, MMA rises. So a “normal” B12 with a high MMA can still mean a meaningful, treatable deficiency — and a low B12 backed up by a high MMA makes the case stronger. This is precisely why you can't judge your B12 status from the B12 line alone. Our guides to vitamin deficiencies that cause neuropathy and the practical question of B12 injections versus oral supplements go deeper here.
Two extra notes that matter for real people. If you take metformin for diabetes, long-term use can lower B12 — a double relevance when you also have neuropathy, which we cover in metformin and the B12 connection. And if your B12 is low, the next question is why — sometimes it's an absorption problem like pernicious anemia rather than diet, which changes the treatment entirely; our piece on pernicious anemia and neuropathy explains that fork in the road.
The Metabolic Screen: Thyroid, Kidney, and Liver
A chunk of your panel is checking the body systems whose dysfunction can quietly damage nerves. You'll typically see a TSH (thyroid), and a metabolic panel covering kidney markers (like creatinine and BUN) and liver enzymes. An out-of-range thyroid result is relevant because both an underactive and, less commonly, an overactive thyroid are associated with neuropathy — and thyroid problems are treatable, which is the recurring theme of why we test for these things. Our article on thyroid problems and neuropathy covers that link. Significant kidney or liver dysfunction can also be a driver, so abnormal values there aren't random extra information — they're part of the same search for a cause. A complete blood count (CBC) often rides along too, screening for anemia and other clues that can accompany some of these conditions.
Protein Tests: The Ones With the Intimidating Names

If you see serum protein electrophoresis (SPEP), immunofixation, or free light chains on your order, don't let the names spook you — but do understand why they're there, because this is one people often skip and shouldn't. A meaningful minority of peripheral neuropathies are linked to an abnormal protein made by the immune system, called a monoclonal protein. These tests screen for that. A finding here doesn't mean something dire by default — the most common result in this category is a condition called MGUS that is monitored over time — but it does mean the right next step is a referral to a specialist (often hematology) for follow-up. The reason this test earns its place on the panel is simple: it's a treatable-cause category you would not want missed, and the result tells your doctor a clear next move.
Autoimmune and Inflammation Markers
Depending on your symptoms and history, you may see inflammation markers like ESR and CRP, and autoimmune screens like ANA, rheumatoid factor, or ANCA. These are looking for autoimmune and inflammatory conditions — things like vasculitis, lupus, Sjögren's, or rheumatoid arthritis — that can attack nerves. One honest caveat to carry into your appointment: these tests are sensitive but not perfectly specific, meaning a mildly positive ANA, for example, is fairly common in the general population and does not automatically mean you have an autoimmune disease. This is a textbook example of why a number on a screen has to be read against your actual symptoms and exam by a clinician, not pattern-matched against the internet at midnight. A weakly positive result is a reason for a thoughtful conversation, not a reason to panic.
A Single Flag Is a Question, Not a Diagnosis
Tests like ANA are sensitive but not perfectly specific — mild positives are common in people without autoimmune disease. A result just outside the range is usually far less meaningful than one far outside it, and the lab's own printed range is the one that applies. Generate questions from this, not conclusions.
Infections Worth Ruling Out

Several infections can cause or contribute to neuropathy, so your panel may include screens for things like HIV, hepatitis C, syphilis (an RPR test), or Lyme disease, particularly if your history or geography points that way. These are on the list for the best possible reason: some are very treatable, and treating the infection can change the course of the neuropathy. If one of these is included, it's standard due diligence in a thorough workup, not a statement about your life — clinicians screen broadly because the upside of catching a treatable infectious cause is large.
The Second-Tier Tests, and the Ones to Question
Beyond the core panel, history-guided tests may appear: vitamin B6 (notable because both too little and too much — usually from over-supplementing — can cause neuropathy), folate, copper, vitamin D, celiac screening (tissue transglutaminase antibodies), and genetic testing when there's a family pattern suggesting a hereditary neuropathy. The vitamin D angle is covered in our article on vitamin D and neuropathy.
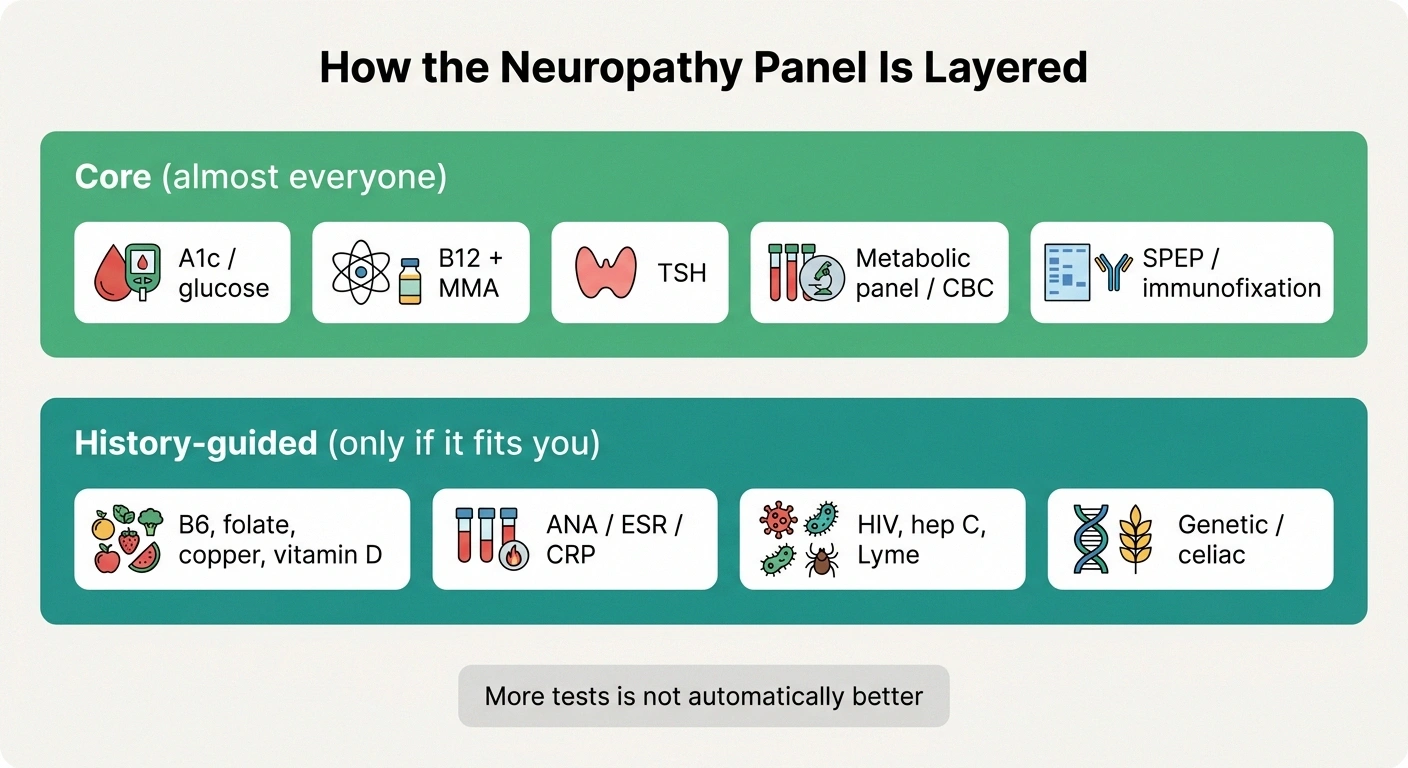
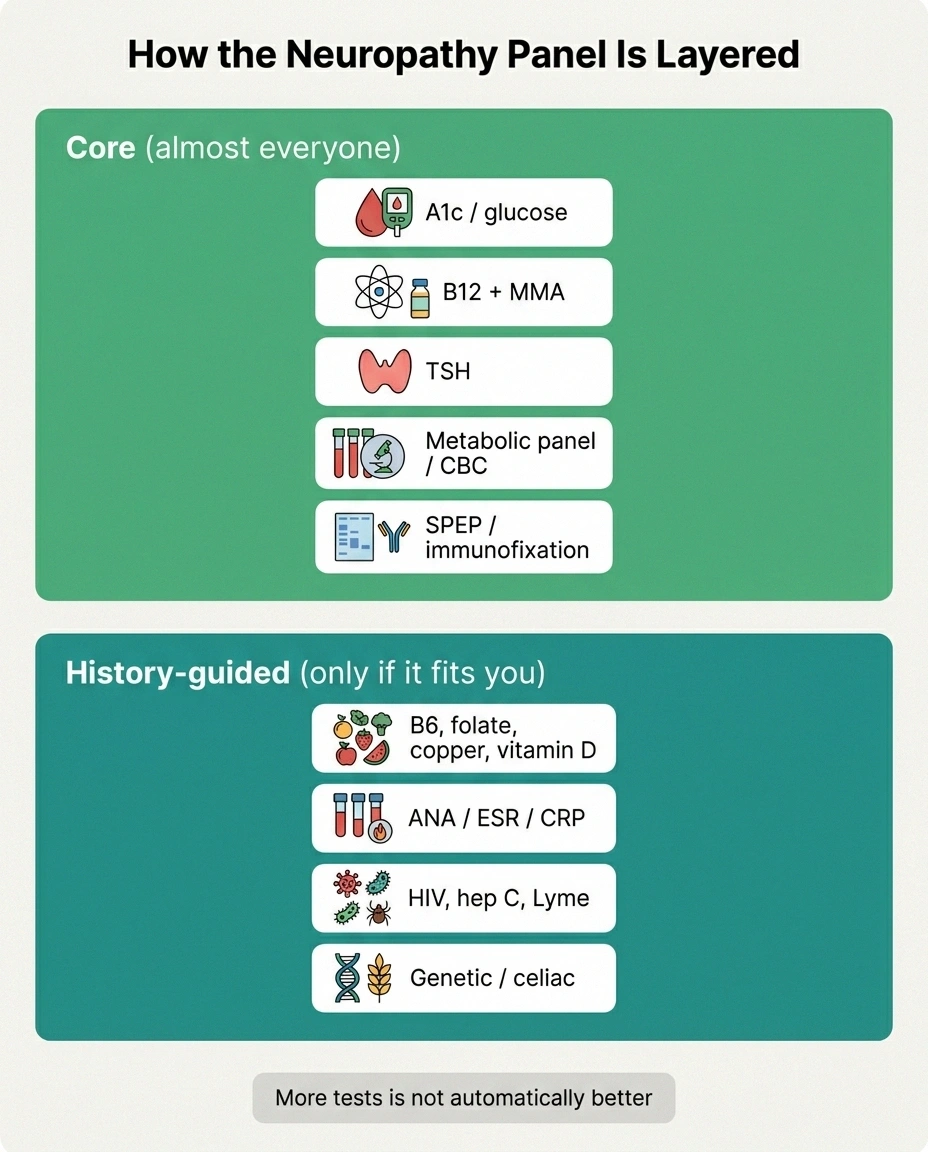
How the Panel Is Layered
A1c / glucose, B12 + MMA, TSH, a metabolic panel and CBC, and protein studies (SPEP / immunofixation). High-yield, treatable-cause tests.
B6 / folate / copper / vitamin D, autoimmune and inflammation markers, infection screens, genetic or celiac testing. Order to fit history — more is not automatically better.
It's also worth knowing the flip side, because it's empowering rather than alarming: more testing is not automatically better. Expert guidelines specifically advise against routinely ordering things like heavy-metal panels without a real exposure history, because in low-probability situations a “positive” is far more likely to be a false alarm that triggers anxiety and more testing than a true finding. If you're handed a huge battery of exotic tests, it's perfectly reasonable to ask your doctor, “Which of these fit my history, and which are we doing just to be exhaustive?” Our companion guide on which blood work to request covers the high-yield list so you can have that conversation as a partner.
“Everything Came Back Normal” — What That Does and Doesn't Mean

This is the result a lot of people are quietly dreading, so let's meet it directly. A normal panel can feel like a door closing — “they couldn't find anything, so there's nothing to be done.” That interpretation is understandable and, importantly, wrong.
A normal workup means something specific and limited: the common identifiable, treatable causes that show up in blood were not found. After a thorough evaluation, a sizable share of neuropathy — often roughly a quarter to a third of cases — has no identified cause and is called idiopathic neuropathy. That is a recognized category, not a dead end, and it does not mean nothing can help your symptoms. Symptom management, lifestyle factors, and follow-up over time (sometimes a cause declares itself later) are all still very much on the table. Our article on idiopathic neuropathy is written specifically for the person staring at a “normal” panel, and our honest look at whether neuropathy can be reversed separates what's realistic from what isn't. “We didn't find a cause in the blood” and “there's nothing we can do for you” are two completely different sentences. Don't let the first one masquerade as the second.
How to Read Your Own Results Without Spiraling
If you're going to look before your appointment — and most of us will — do it with a few guardrails. First, focus on the flagged values, but remember a single flag is a question, not a diagnosis. Second, reference ranges vary between laboratories, and a result just outside the range is often far less meaningful than a result far outside it; the lab's own range printed next to your number is the one that applies. Third, resist the urge to assemble a self-diagnosis from individual lines — these tests are designed to be read together and against your exam, and the same number can mean very different things in different people. Use what you've read here to generate good questions, not conclusions. The goal of looking early isn't to beat your doctor to the answer; it's to walk in able to have a faster, clearer conversation.
Questions Worth Bringing to Your Appointment

This is where understanding your results actually pays off. A few questions that consistently move these conversations forward: “Based on these results, what do you think is the most likely cause — or are we in idiopathic territory?” “My B12 was normal but did we check MMA, and what did it show?” “My sugar tests were borderline — should we do a glucose tolerance test?” “Is anything here a ‘treatable cause,' and if so, what's the plan?” “Which of these flagged values are you actually concerned about, and which are background noise?” Our guide on how to talk to your doctor about neuropathy has more scripts like these. Walking in with three or four specific questions, instead of a folder of printouts and a knot in your stomach, genuinely changes the appointment — I've watched it do exactly that for people in my group, and it did it for me.
Four Questions That Move the Appointment
“Based on these results, what's the most likely cause — or are we in idiopathic territory?”
“My B12 was normal — did we check MMA, and what did it show?”
“My sugar tests were borderline — should we do a glucose tolerance test?”
“Which flagged values are you actually concerned about, and which are background noise?”
Frequently Asked Questions
What blood test shows neuropathy?
No blood test shows neuropathy itself. Neuropathy is diagnosed from your symptoms, a neurological exam, and often nerve testing such as an EMG and nerve conduction study. Blood tests are ordered to search for an underlying cause — things like high blood sugar, vitamin B12 deficiency, thyroid problems, or abnormal proteins — many of which are treatable. Reading your results as a hunt for a treatable cause, not a test for nerve damage, is the key to making sense of them.
What does it mean if my neuropathy blood tests are all normal?
It means the common identifiable causes that show up in blood were not found. It does not mean nothing is wrong or nothing can help. After a thorough workup, roughly a quarter to a third of neuropathy has no identified cause and is called idiopathic, which is a recognized category, not a dead end. Symptom management, lifestyle factors, and ongoing follow-up are still available, and a cause sometimes becomes clear later.
My vitamin B12 was normal — could it still be a B12 problem?
“No cause found in the blood” is not “nothing can help”
A normal panel means the common treatable causes that show in blood weren't found. A quarter to a third of neuropathy is idiopathic — a recognized category, not a dead end. Symptom care, lifestyle factors, and follow-up are all still on the table.
Possibly. A serum B12 in the low-normal range can still reflect a functional deficiency at the tissue level. Doctors add a methylmalonic acid (MMA) test, and sometimes homocysteine, to detect this. A normal B12 with an elevated MMA can still indicate a meaningful, treatable deficiency. This is why B12 status should not be judged from the B12 number alone, and it is a good specific question to raise with your doctor.
Can a blood test tell what type of neuropathy I have?
Blood tests point toward a possible cause rather than classifying the type of neuropathy directly. The type and pattern of nerve involvement come from your exam and nerve testing. A blood result can support a particular cause — for example, abnormal blood sugar pointing toward diabetic neuropathy — but the full picture combines blood work, exam findings, and nerve studies interpreted together by your clinician.
Why did my doctor order a glucose tolerance test when my A1c was normal?
Because nerve damage can begin during the prediabetic stage, when A1c and fasting glucose still look normal. A 2-hour oral glucose tolerance test can detect impaired glucose tolerance that those tests miss. Ordering it when blood sugar is borderline but suspicion is high is a thorough, appropriate step rather than an unnecessary one, and it can uncover a treatable contributor.
Should I be worried about a slightly positive ANA or a single flagged value?
Not on its own. Tests like ANA are sensitive but not perfectly specific, and mild positives are fairly common in people without autoimmune disease. A single flagged value is a question to discuss, not a diagnosis. Results just outside the reference range are often far less significant than results far outside it, and everything has to be interpreted against your symptoms and exam by your clinician rather than pattern-matched in isolation.
Is more testing always better?
No. Expert guidance recommends targeting tests to your history rather than ordering everything. In low-probability situations, broad exotic panels like routine heavy-metal screening without an exposure history are more likely to produce false alarms than true findings, leading to anxiety and more testing. It is reasonable to ask your doctor which tests fit your specific history and which are being done only to be exhaustive.