Neuropathy and PTSD: When Chronic Pain Becomes Trauma
There's a conversation that doesn't happen enough in neuropathy communities, and it's time we had it. When you live with relentless nerve pain — the kind that steals your sleep, limits your independence, and reshapes your identity — something can shift inside you that goes beyond frustration or sadness. For some people, chronic neuropathy pain crosses a line into something that looks and feels a lot like trauma.
I've sat across from people in support groups who describe hypervigilance about their symptoms, nightmares about pain flares, emotional numbness, and avoidance of activities they once loved — not because they physically can't do them, but because they're terrified of triggering more pain. These aren't just “bad days.” These are signs that chronic pain has left psychological wounds that deserve attention and treatment.
This article explores the complex relationship between neuropathy and PTSD — a connection that's backed by growing research but still rarely discussed in doctor's offices.
Understanding the Two-Way Street Between Pain and Trauma
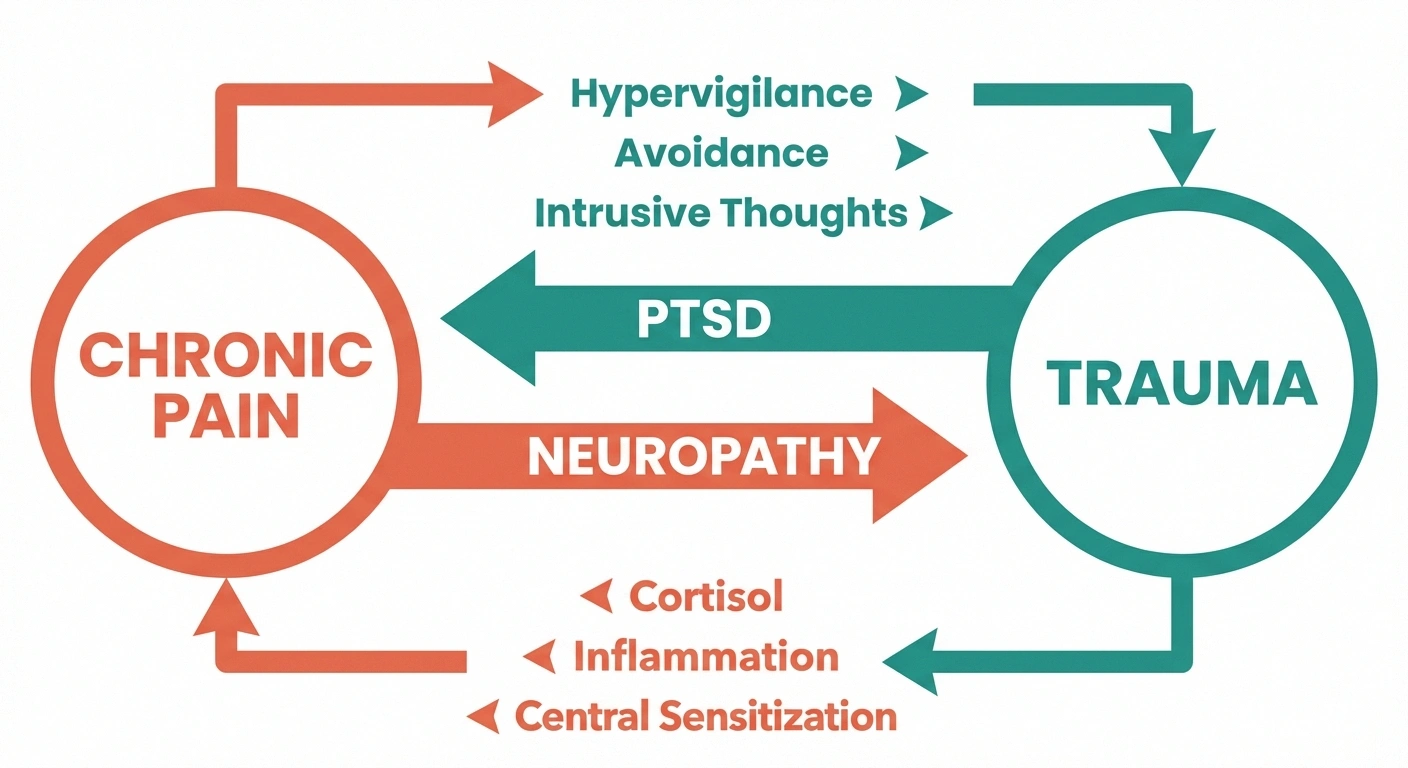
The relationship between neuropathy and PTSD isn't a one-way road. It flows in both directions, and understanding this is essential for getting the right help.
Path 1: When Chronic Pain Leads to Trauma
Most people think of PTSD as something caused by a single catastrophic event — combat, an accident, assault. But the diagnostic criteria for PTSD have expanded, and mental health professionals increasingly recognize that prolonged exposure to severe, uncontrollable pain can produce trauma responses that mirror traditional PTSD.
Think about what chronic neuropathy actually involves: unpredictable pain flares that can feel like electric shocks. The loss of abilities you once took for granted. Medical procedures that may have been painful or frightening. Feeling trapped in a body that seems to be working against you. The slow erosion of your social life, career, and sense of self.
These experiences, accumulated over months and years, can overwhelm your nervous system's ability to process them. The result may look like:
- Hypervigilance about symptoms: Constantly monitoring your body for signs of a pain flare, unable to relax
- Avoidance behaviors: Refusing to do activities, visit places, or even think about experiences associated with pain
- Intrusive thoughts: Unwanted, recurring thoughts about pain episodes or fears about your condition worsening
- Emotional numbing: Feeling disconnected from emotions, relationships, or activities that used to matter
- Sleep disruption: Nightmares or insomnia driven by anxiety about nighttime pain
- Exaggerated startle response: Jumping at unexpected sensations, including innocuous touches
If you're experiencing these symptoms alongside your neuropathy, you're not “overreacting” to your pain. Your nervous system is responding to a real, sustained threat in the way it's designed to — it just hasn't been able to turn off the alarm.
Path 2: When PTSD Worsens or Triggers Neuropathy
Research has also revealed a pathway running in the opposite direction. People with PTSD — whether from combat, abuse, accidents, or other traumatic experiences — are significantly more likely to develop chronic pain conditions, including peripheral neuropathy.
A study published in the Journal of Traumatic Stress found that veterans with PTSD had a significantly higher prevalence of peripheral neuropathy compared to veterans without PTSD. This isn't coincidence — there are specific biological mechanisms at work.
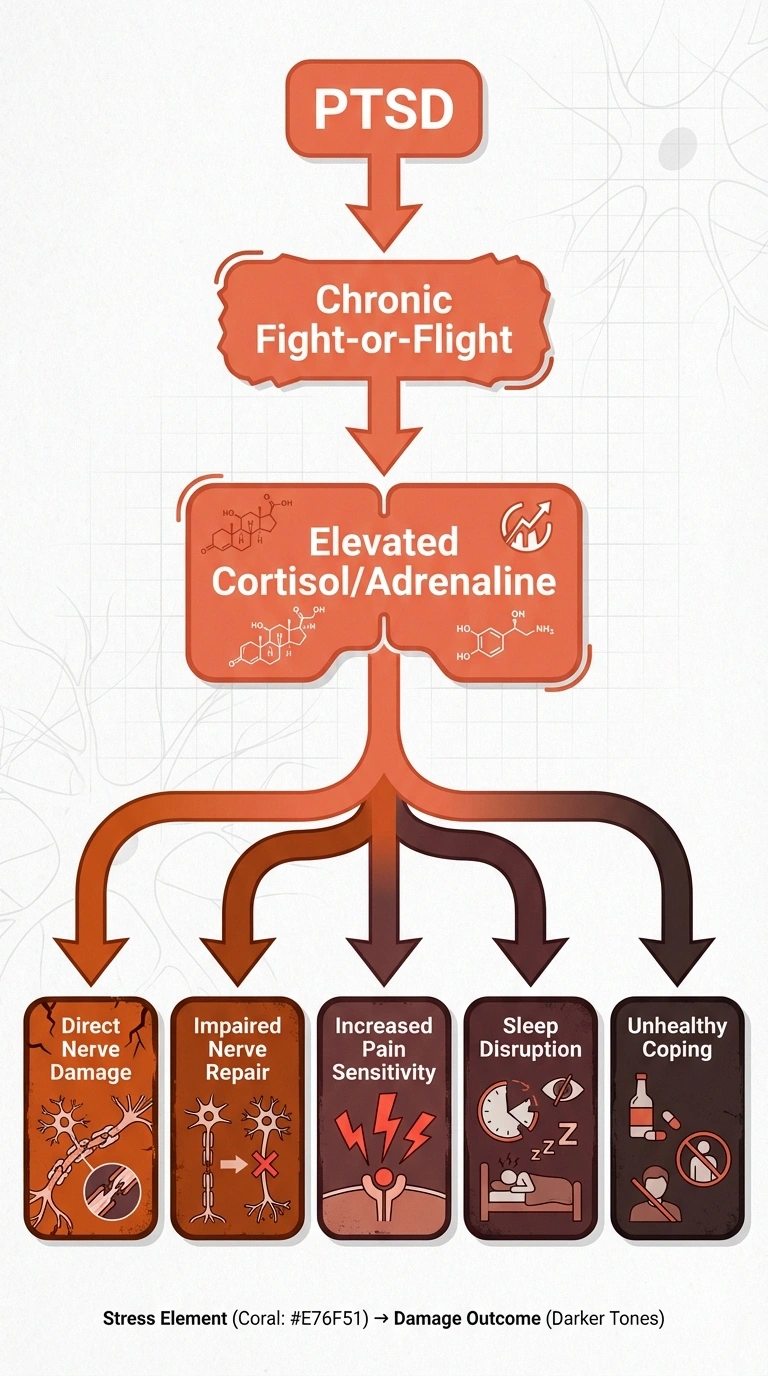
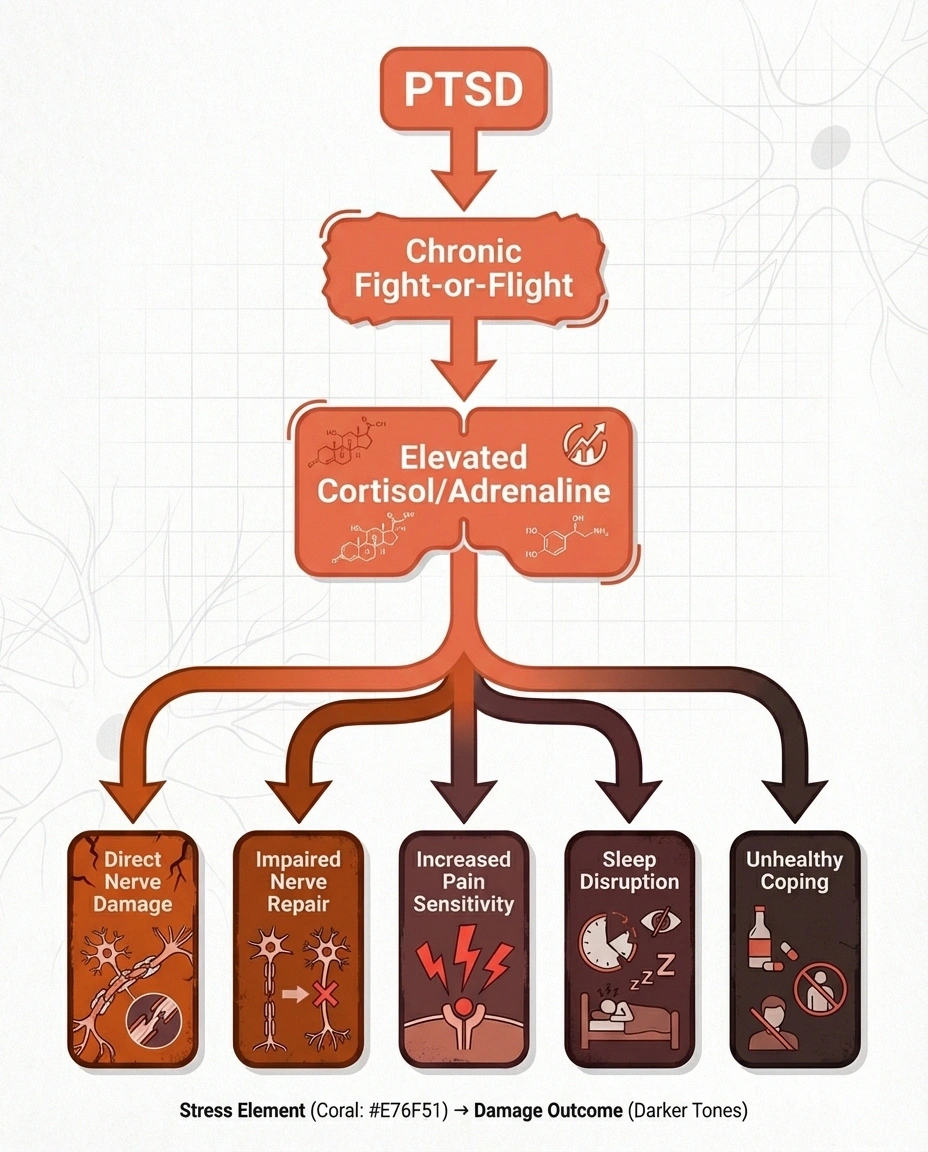
PTSD keeps your body in a chronic state of “fight or flight.” This means persistently elevated levels of stress hormones, particularly cortisol and adrenaline. Over time, these hormones can:
- Directly damage peripheral nerves through sustained inflammation
- Impair nerve repair processes by diverting the body's resources toward maintaining the stress response
- Increase pain sensitivity through a process called central sensitization
- Disrupt sleep, which is critical for nerve health and pain management
- Promote unhealthy coping behaviors (alcohol use, poor diet, inactivity) that independently worsen neuropathy
If you developed neuropathy symptoms after a traumatic event or period, or if your neuropathy seemed to worsen significantly during a time of extreme stress, the PTSD-neuropathy connection may be relevant to your experience.
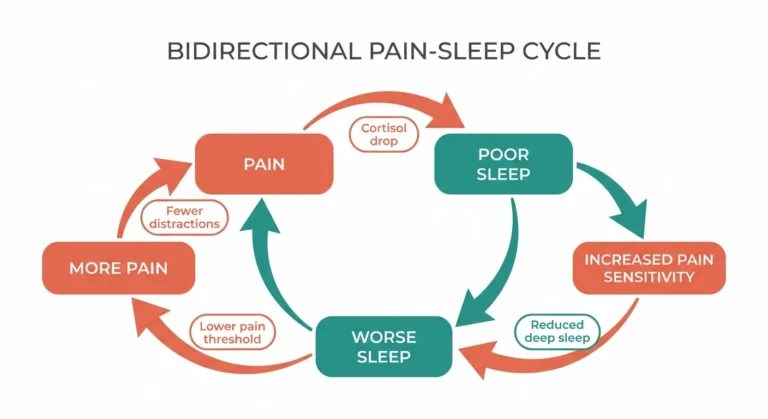
Central Sensitization: When Your Nervous System Gets Stuck on High Alert
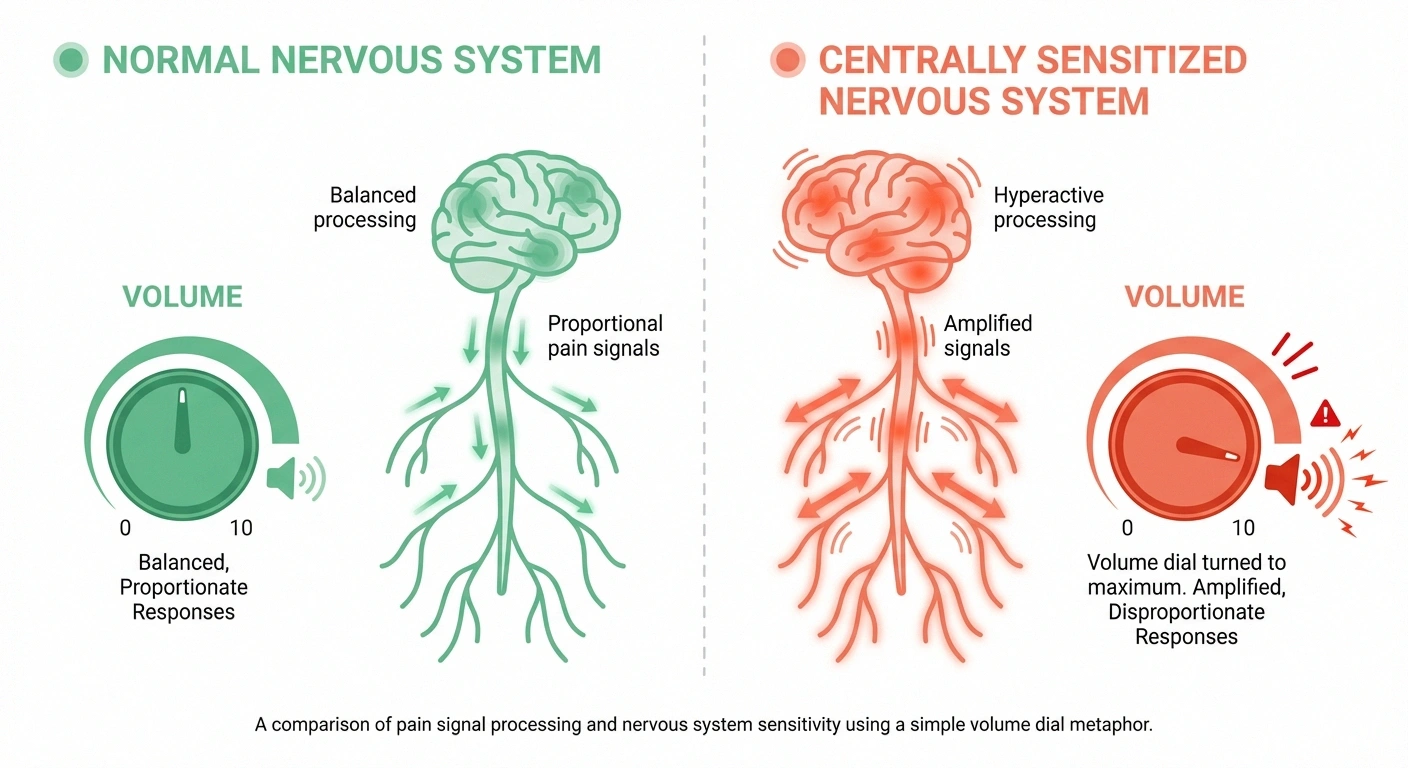
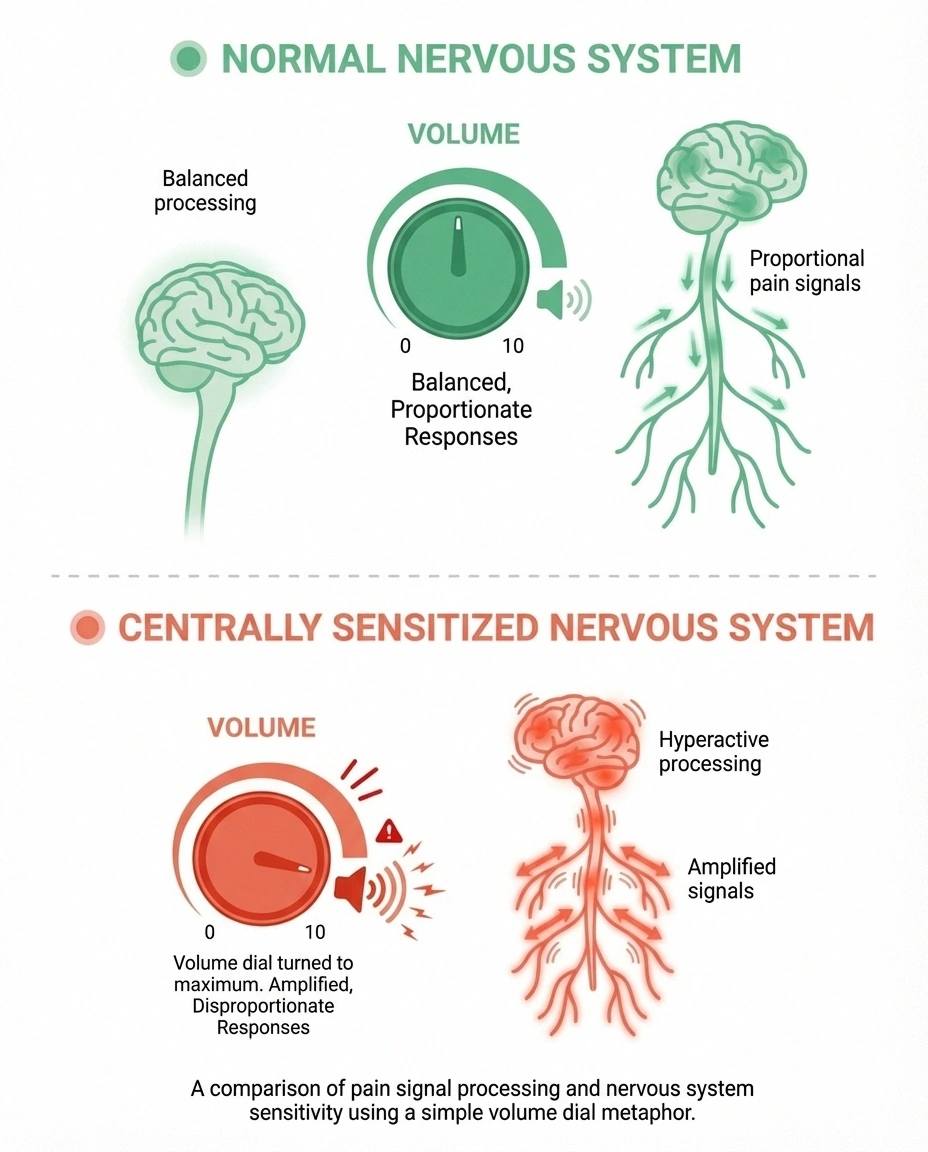
One of the most important concepts for understanding the PTSD-neuropathy overlap is central sensitization. This is the process by which your central nervous system — your brain and spinal cord — becomes hypersensitive to pain signals.
In a healthy nervous system, pain signals are processed proportionally. A mild stimulus produces a mild pain signal. But in central sensitization, the volume dial gets turned way up and stuck there. Normal sensations — a light touch, clothing against your skin, a temperature change — may register as painful. Pain from actual nerve damage gets amplified far beyond what the physical damage alone would produce.
Both chronic pain and PTSD independently contribute to central sensitization, and when they coexist, they compound each other's effects. Your trauma keeps your nervous system hypervigilant, which amplifies pain signals, which creates more distress, which further sensitizes your nervous system.
This isn't a psychological weakness — it's a measurable neurological change. Brain imaging studies show altered activity in pain-processing regions in people with both chronic pain and PTSD. Understanding this can be incredibly validating if you've ever been told your pain is “just in your head” or that you should be able to handle it better.
The connection to pain catastrophizing is important here too. Catastrophizing — those spiraling thoughts of “this will never end” and “I can't take anymore” — is a feature of both PTSD and chronic pain, and it directly fuels central sensitization.
Recognizing PTSD Symptoms in Yourself

One of the challenges with PTSD in chronic pain patients is that many symptoms overlap. Difficulty sleeping, irritability, difficulty concentrating, and withdrawal from activities can all be attributed to “just having neuropathy.” But there's value in asking yourself some honest questions:
- Do you feel constantly “on edge” about your pain, even during periods when symptoms are manageable?
- Do you avoid activities, places, or people because of fear of pain (not because of actual pain in that moment)?
- Do you have recurring, unwanted memories of particularly bad pain episodes or frightening medical experiences?
- Have you noticed feeling emotionally “flat” or disconnected from things you used to care about?
- Do you react intensely to unexpected physical sensations?
- Do you feel a sense of hopelessness about your future that goes beyond realistic concern about your condition?
If several of these resonate, it doesn't mean you definitely have PTSD, but it does suggest that the emotional impact of your neuropathy deserves professional attention. And there's absolutely no shame in that. Living with chronic nerve pain is genuinely hard, and acknowledging the psychological toll is a sign of strength, not weakness.
This kind of self-awareness is closely related to understanding the anxiety that often accompanies neuropathy. Anxiety and PTSD exist on a spectrum, and both are treatable.
How PTSD and Neuropathy Affect Daily Life Together
When these two conditions coexist, their combined impact on daily functioning can be far greater than either condition alone. Here's how this plays out in real life:
Social Withdrawal
Pain makes you cancel plans. Trauma makes you stop making plans in the first place. The combination can lead to profound isolation. You may pull away from friends and family — not because you don't care about them, but because the effort of socializing while managing pain and emotional distress feels impossible. Over time, your world can shrink dramatically.
If this sounds familiar, connecting with a neuropathy support group may help break the cycle. Being around people who understand your experience can feel less threatening than general social situations.
Medical Avoidance
Some people with pain-related PTSD begin avoiding medical appointments, tests, or procedures — even ones that could help them. Past experiences with painful or dismissive medical encounters can create trauma responses that make the doctor's office feel unsafe. This means conditions go unmonitored and treatment opportunities are missed.
Identity and Self-Worth
Neuropathy can force you to give up activities, careers, and roles that defined who you were. PTSD adds a layer of grief and loss that can feel paralyzing. The person you were before neuropathy may feel unreachable, and the person you are now may feel diminished. This is a profound loss that deserves to be acknowledged and processed — ideally with professional support.
Understanding how neuropathy affects not just your body but your sense of self connects to the broader experience of grief and loss in neuropathy.
Treatment Approaches That Address Both Conditions
The most important thing to understand about treating coexisting neuropathy and PTSD is that both conditions need attention. Treating only the pain while ignoring the trauma — or vice versa — is unlikely to produce lasting improvement.
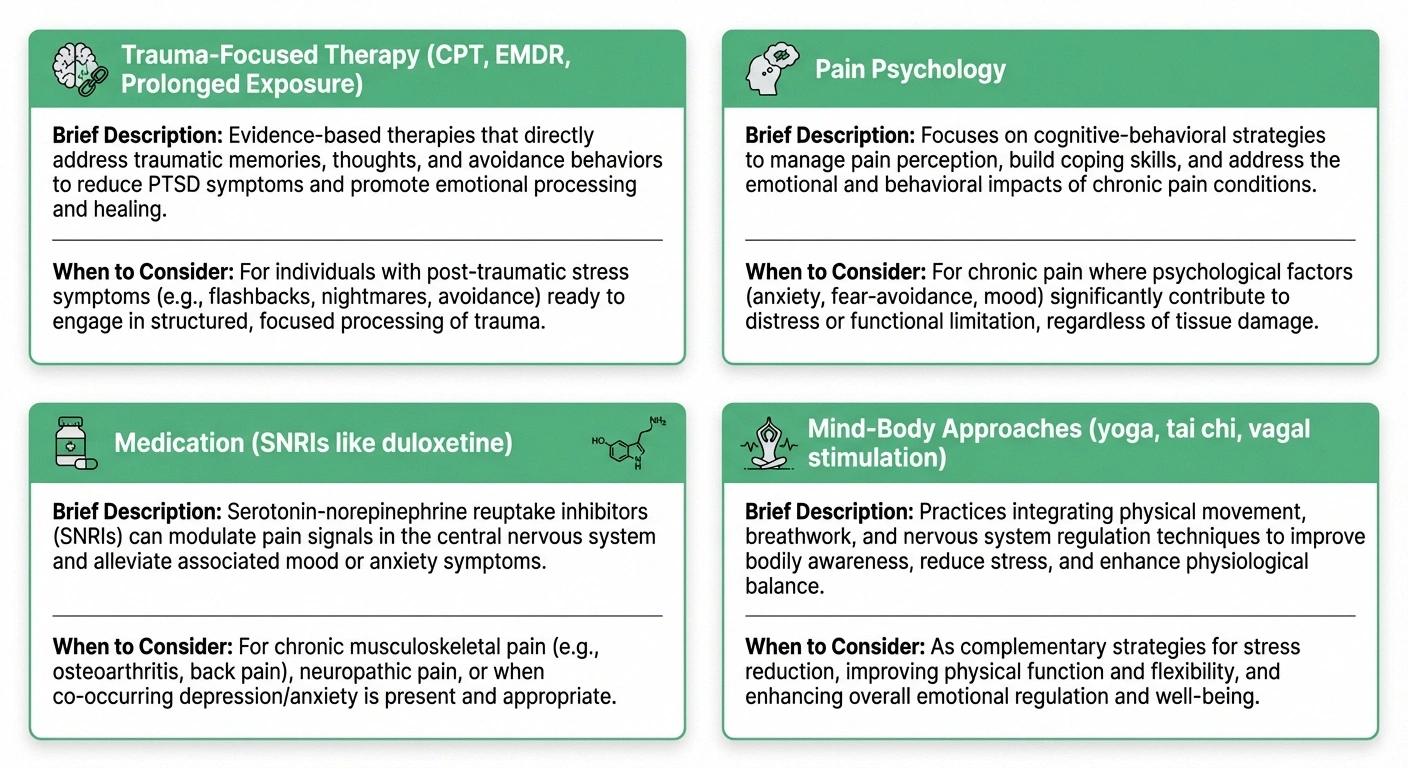
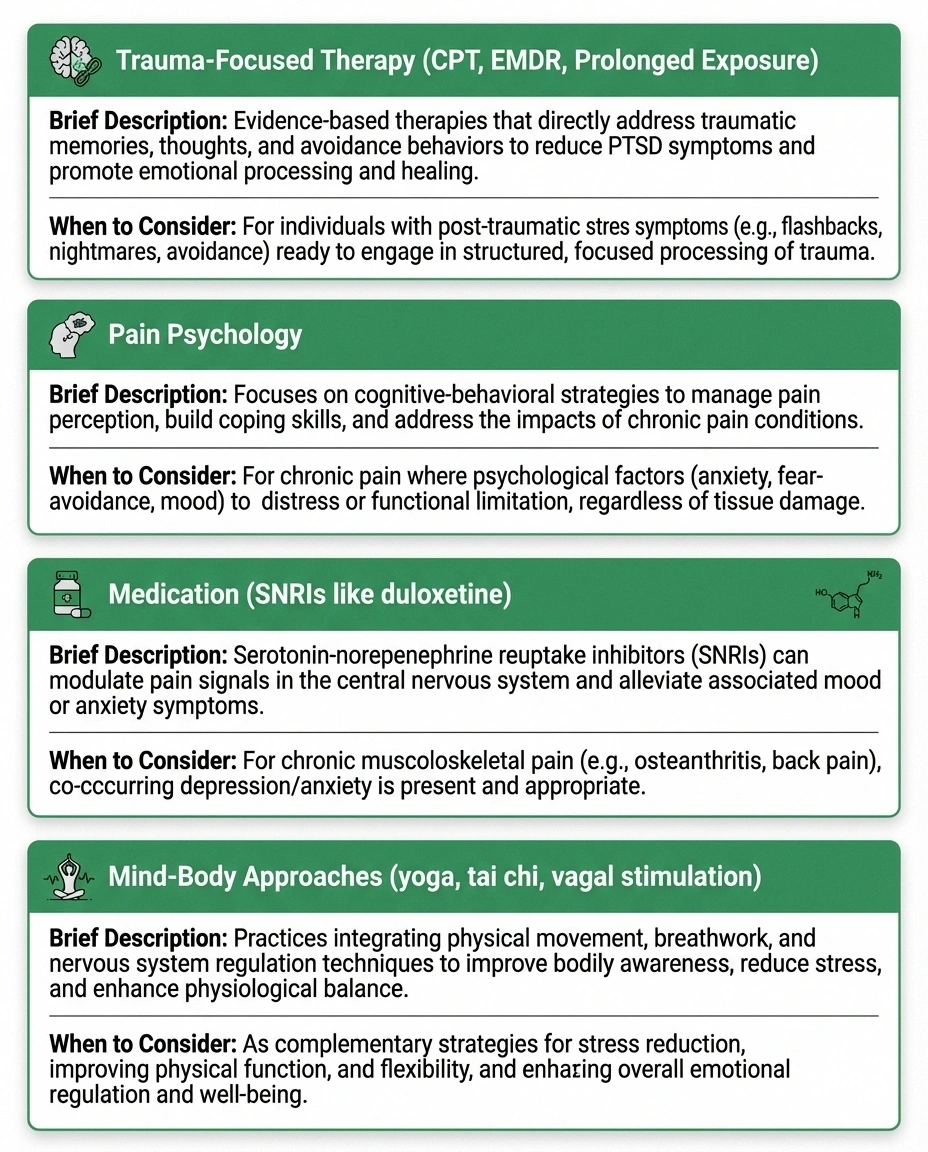
Trauma-Focused Psychotherapy
Several evidence-based therapies can help process the trauma associated with chronic pain:
Cognitive Processing Therapy (CPT) helps you examine and restructure the thoughts and beliefs that developed around your pain experience. If you believe “my life is over” or “no one understands what I'm going through,” CPT can help you develop more balanced, accurate perspectives without minimizing your real experience.
Eye Movement Desensitization and Reprocessing (EMDR) uses bilateral stimulation (typically eye movements) to help your brain reprocess traumatic memories. Several studies have shown that EMDR can reduce both PTSD symptoms and chronic pain levels. It's particularly helpful for people whose pain is connected to specific traumatic events or medical experiences.
Prolonged Exposure Therapy gradually and safely helps you face the memories, situations, and feelings you've been avoiding. For pain-related PTSD, this might involve gradually reengaging with activities you've avoided due to fear of pain.
Integrated Pain Psychology
Pain psychologists specialize in the intersection of chronic pain and mental health. They understand that your pain is real AND that psychological factors influence how you experience it. This “both/and” approach — rather than the dismissive “it's all in your head” — is crucial for building trust and making progress.
Look for psychologists who specialize in chronic pain management, as they'll be familiar with the specific challenges of neuropathy-related trauma. Your neurologist or pain management doctor can often provide referrals.
Medication Considerations
Some medications may help with both conditions simultaneously. SSRIs and SNRIs (like duloxetine, which is FDA-approved for diabetic neuropathy) can address both PTSD symptoms and neuropathic pain. Discuss with your doctor whether your current medication regimen is optimally addressing both your pain and your psychological symptoms.
It's worth noting that understanding where you are in the stages of neuropathy can help your treatment team calibrate both your pain management and psychological support appropriately.
Mind-Body Approaches
Practices that engage both physical and psychological healing may be particularly valuable when both systems are affected:
- Yoga: Yoga adapted for neuropathy combines gentle movement with breath work and mindfulness, addressing both the physical deconditioning and the nervous system hyperactivation that come with chronic pain and trauma.
- Tai Chi: This slow, intentional movement practice has shown benefits for both PTSD and chronic pain in clinical studies.
- Vagal nerve stimulation: Techniques that activate the vagus nerve — deep breathing, cold water on the face, humming — can help shift your nervous system out of fight-or-flight mode. This is particularly relevant because vagal dysfunction has been documented in both PTSD and neuropathy.
Talking to Your Doctor About the Emotional Impact of Pain

One of the biggest barriers to getting help is the conversation itself. Many people worry that mentioning emotional or psychological symptoms will lead their doctor to take their physical pain less seriously. This fear is understandable — too many people with chronic pain have had their symptoms dismissed.
Here are some approaches that may help:
Be direct: “I've noticed that my chronic pain is affecting my mental health in ways that go beyond feeling frustrated. I'm experiencing [specific symptoms]. I think I may need support for the emotional impact of living with this condition.”
Frame it medically: “I've read that chronic pain and PTSD are connected and can make each other worse. I want to make sure we're addressing both the physical and psychological aspects of my condition.”
Ask for referrals: “Can you refer me to a pain psychologist or a therapist who specializes in chronic illness? I think that could complement my pain management.”
If your doctor dismisses your concerns, that's information about your doctor, not about the validity of your experience. Consider seeking a second opinion or asking for a referral to a comprehensive pain management program that includes psychological support.
Helping Loved Ones Understand
The intersection of neuropathy and trauma can be particularly difficult for family members and friends to understand. They may see your physical pain but miss the psychological wounds underneath. Or they may recognize that you're struggling emotionally but attribute it to depression without understanding the trauma component.
Some things that may help:
- Share information about the pain-trauma connection (you could share this article)
- Be specific about what you need: “I need you to understand that when I cancel plans, it's not that I don't want to see you — it's that my body and mind are overwhelmed”
- Invite them to a therapy session if your therapist supports it
- Connect them with resources for understanding the mental health impact of neuropathy
A Note on Veterans and Military Trauma
Veterans deserve special mention here because the PTSD-neuropathy connection is particularly well-documented in this population. Combat-related PTSD, combined with exposures to environmental toxins, physical injuries, and the wear of military service, creates a high-risk profile for developing both conditions.
If you're a veteran dealing with both PTSD and neuropathy, the VA offers integrated care programs that address both conditions. VA healthcare providers are increasingly trained in the pain-trauma connection, and you may be eligible for specialized programs. Don't hesitate to ask your VA care team about integrated pain and mental health treatment.
Moving Forward: There Is Hope

If you recognized yourself in this article — if the words “hypervigilance,” “avoidance,” and “emotional numbness” hit close to home — please know that these responses to chronic pain are understandable, they're treatable, and they don't have to define your future.
Recovery from pain-related trauma doesn't mean becoming pain-free. It means reaching a place where pain is one part of your life rather than the thing that controls all of it. It means being able to make plans without paralyzing fear. It means reconnecting with emotions, relationships, and activities that give your life meaning.
I've seen people in our community make this journey, and while it's not quick or easy, the transformation is real. It starts with acknowledging that your suffering is valid and that you deserve help for all of it — not just the nerves, but the whole person.
If you're in crisis, please reach out to the 988 Suicide and Crisis Lifeline by calling or texting 988. You don't need to be suicidal to call — they support anyone in emotional distress.
Frequently Asked Questions
Can living with neuropathy pain actually cause PTSD?
Yes. While PTSD has traditionally been associated with single catastrophic events, mental health professionals increasingly recognize that prolonged exposure to severe, uncontrollable chronic pain can produce trauma responses that meet the diagnostic criteria for PTSD. The constant pain, loss of function, frightening medical experiences, and erosion of identity that accompany chronic neuropathy can overwhelm the nervous system's ability to process these experiences.
How does PTSD make neuropathy symptoms worse?
PTSD keeps the body in a chronic state of fight or flight, with elevated levels of stress hormones like cortisol and adrenaline. Over time, these hormones increase inflammation, impair nerve repair, and contribute to central sensitization, a process where the nervous system becomes hypersensitive to pain signals. This means the same level of nerve damage produces more perceived pain in someone with PTSD than in someone without it.
What is central sensitization and how does it relate to trauma and nerve pain?
Central sensitization is a condition in which the central nervous system, the brain and spinal cord, becomes hypersensitive to pain signals. Normal sensations may register as painful, and existing pain gets amplified beyond what the physical damage alone would produce. Both chronic pain and PTSD independently contribute to central sensitization, and when they coexist, they compound each other's effects through shared neurological pathways.
Should I see a therapist if my chronic pain is affecting my mental health?
Yes. If you are experiencing hypervigilance about symptoms, avoidance of activities due to fear of pain, intrusive thoughts about pain episodes, emotional numbness, or a sense of hopelessness, professional psychological support can make a meaningful difference. Look for a pain psychologist or therapist who specializes in chronic illness. Addressing the psychological impact of pain often improves the pain experience itself.
What treatments help when you have both PTSD and neuropathy?

The most effective approach addresses both conditions simultaneously. Evidence-based options include trauma-focused psychotherapy such as CPT, EMDR, or prolonged exposure therapy, combined with appropriate pain management. Some medications like duloxetine treat both neuropathic pain and PTSD symptoms. Mind-body practices including yoga and tai chi address both physical and psychological aspects. Integrated pain management programs that include psychological support often produce the best outcomes.
Can trauma-focused therapy reduce physical nerve pain?
Research suggests it can. Studies on EMDR and cognitive processing therapy have shown reductions in both PTSD symptoms and chronic pain levels. By reducing the stress response and central sensitization that amplify pain signals, trauma therapy can lower the overall pain experience even though the underlying nerve damage remains. This is not because the pain was imaginary but because the nervous system amplification of pain signals decreases when trauma is addressed.
How do I talk to my doctor about the emotional impact of chronic pain?
Be direct and specific about your symptoms. Frame your concerns medically by referencing the documented connection between chronic pain and PTSD. Ask specifically for a referral to a pain psychologist or therapist who specializes in chronic illness. If your doctor dismisses your concerns, seek a second opinion. You deserve a care team that addresses both the physical and psychological aspects of your condition.
Living with neuropathy is hard enough without carrying unaddressed trauma alongside it. If anything in this article resonated with you, please reach out for help. You deserve support for the whole experience — body and mind.
As always, this information reflects my perspective as a patient advocate and is not a substitute for professional medical or psychological advice.