
The first member of our support group I ever heard describe Charcot foot did so in a sentence I have never forgotten. “My foot was warm and a little puffy for about three weeks,” she said, “and I just thought I'd done too much on it. By the time I got it looked at, the bones inside had collapsed and I had to spend the next six months in a cast.” Her foot eventually stabilized, but it never looked the same again. She walked the rest of her life with a custom-built shoe and a slow, careful gait.
I share that story not to scare you. I share it because Charcot foot is one of the genuinely dangerous complications of diabetic neuropathy, and the difference between a good outcome and a devastating one almost always comes down to how quickly it gets caught. There is a window — sometimes a few weeks, sometimes a couple of months — where simple offloading can stop the bones from collapsing. Miss that window and the foot reshapes itself in ways that cannot be undone.
I'm Janet, and I write here as a patient advocate, not a medical professional. What I want to give you in this article is what I wish every diabetic patient with foot numbness already knew: what Charcot foot actually is, what its early warning signs look like, why it gets missed, and exactly what to do if you see those signs in yourself or a loved one. If you are a person with diabetes — or you love someone who is — please don't skim this one. The five minutes you spend reading it could be the most important medical reading of your year.
What Charcot Foot Actually Is
Charcot foot — full medical name Charcot neuroarthropathy, sometimes Charcot arthropathy — is progressive destruction of the bones and joints in the foot or ankle in a person who has lost protective sensation. The bones fracture. The joints dislocate. The arch of the foot can collapse or invert into a shape clinicians call a “rocker bottom” because the foot looks bowed downward like the bottom of a rocking chair. And the patient, in many cases, feels almost none of this happening.
A warm, swollen, red foot in a diabetic patient with neuropathy is Charcot foot until proven otherwise. The phrase exists because the cost of delay is so high — bones can fracture and collapse before the patient feels meaningful pain.
That last sentence is the part that surprises everyone. We are used to thinking of broken bones as some of the most painful injuries the body can produce. Walk on a sprained ankle for ten steps and you'll be limping. Walk on a small foot fracture for an hour and you'll be off your feet for a week. Now imagine a foot where the bones can fracture and the body's pain alarm is muted to a whisper. The foot keeps being walked on. The fractures progress. The joints displace. The deformity grows.
That is Charcot foot. It is not a separate disease. It is what happens when severe neuropathy meets ongoing weight-bearing on a vulnerable foot, and it is one of the most preventable serious complications of diabetes.
Why It Happens, Mechanically
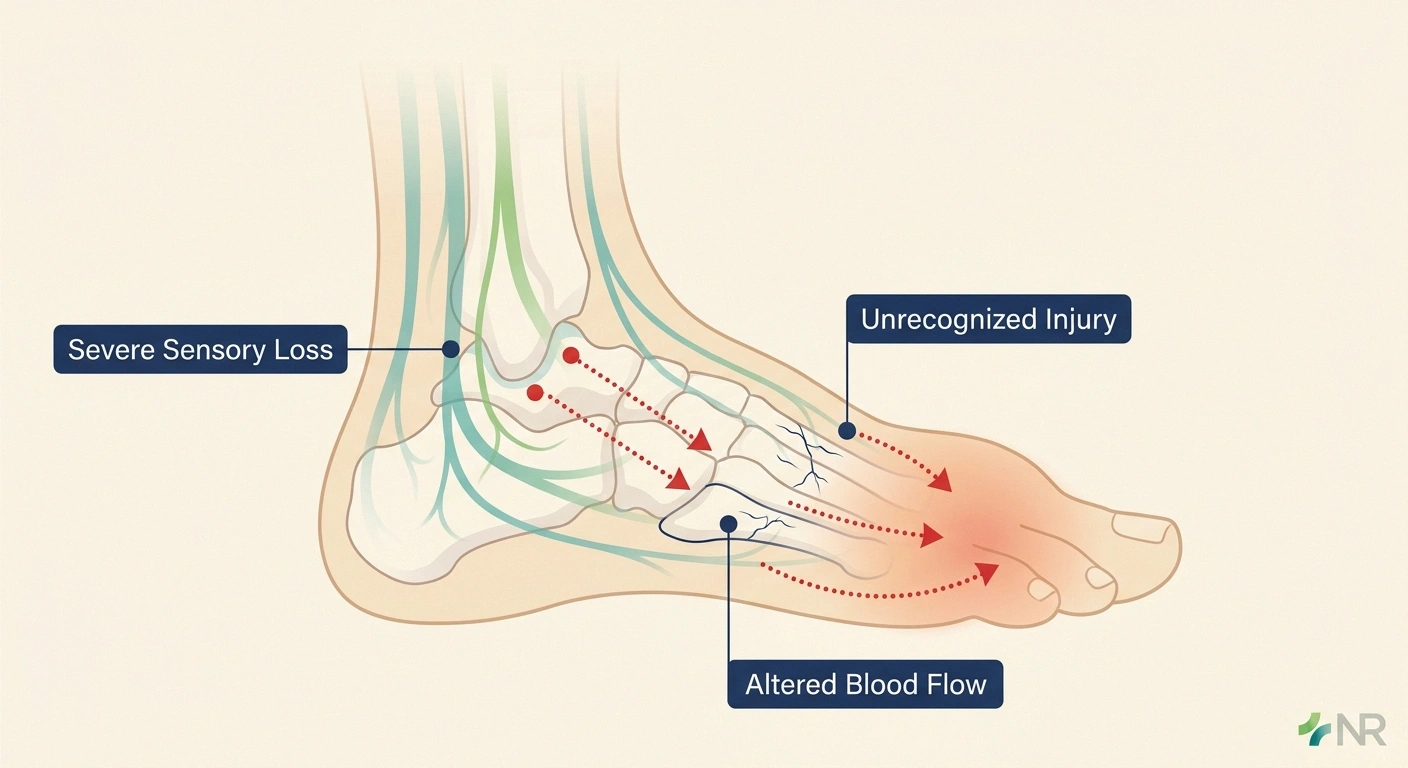
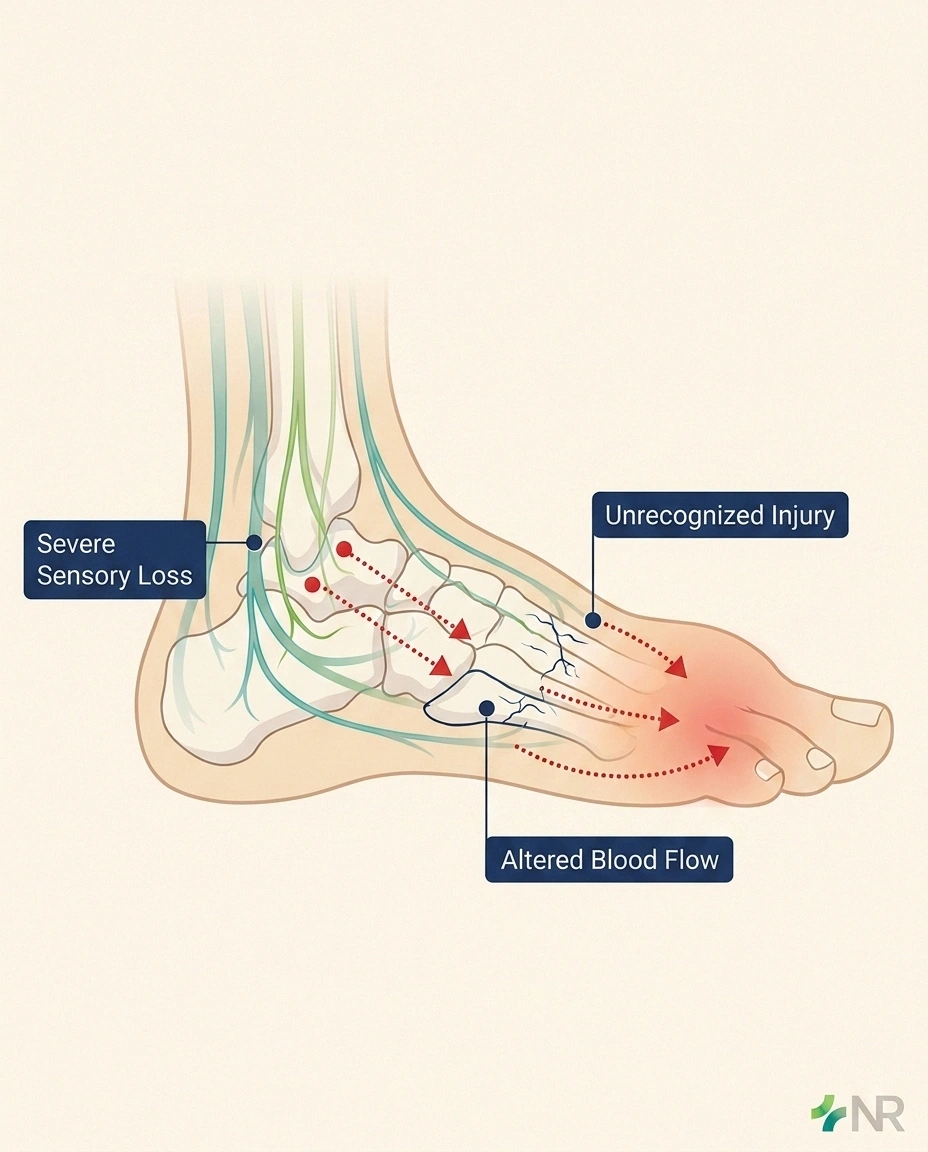
Doctors still debate some of the finer details, but the broad mechanism of Charcot foot is reasonably well understood. Three things have to come together.
Studies have shown that a consistent foot-temperature difference of more than four degrees Fahrenheit between feet often precedes a visible Charcot episode by days or weeks. Daily home temperature checks with a simple infrared thermometer are one of the highest-leverage prevention habits for high-risk patients.
The first is severe sensory neuropathy. The kind where protective sensation in the foot is significantly reduced — where you cannot feel the small pebble in your shoe, where the bath water doesn't feel as hot as it actually is, where touching the floor with your bare feet feels muffled or distant. This is the foundation. Without significant sensory loss, Charcot foot does not develop because pain stops the patient before damage accumulates.
The second is a triggering injury that the patient does not recognize. It might be an actual fall or twist. It might be a long day of walking that produced micro-fractures. It might be a piece of furniture stubbed in the night. It might be nothing the patient can remember at all. In many cases, the initial injury is genuinely minor — the kind a person with normal sensation would walk off in an hour. But because the foot has no functioning pain alarm, the patient keeps loading the injured tissue.
The third is the body's vascular and inflammatory response in diabetes. Autonomic neuropathy alters blood flow patterns in the feet, increasing local blood supply and accelerating bone resorption. The bones become more fragile than they appear. Small fractures progress to bigger fractures, joints become unstable, and the architecture of the foot begins to fail.
The result over a few weeks to a few months is a foot that may look swollen and red on the outside while the bones inside are quietly disintegrating. The patient feels mild discomfort that they may dismiss as a sprain or strain. The condition advances. By the time the picture is clear — visible deformity, ulceration over bony prominences, X-ray findings of fragmentation — the most reversible window has already closed.
The Early Warning Signs That Save Feet
If there is one section of this article I want you to memorize, it is this one. The early Charcot foot — what specialists call Stage 0 — is the version that can usually be stopped before serious damage occurs. The trouble is that the early signs are subtle, and they look like several less serious things.
A temperature difference between feet of four degrees Fahrenheit or more in a diabetic with neuropathy is a warning sign — get evaluated this week, not next month.
The classic Stage 0 picture in someone with diabetic neuropathy includes most or all of the following:
- Warmth. The affected foot is noticeably warmer to the touch than the other foot. A difference of four degrees Fahrenheit or more is significant. Many specialists teach high-risk patients to check foot temperature daily with a simple infrared thermometer for exactly this reason.
- Swelling. The foot looks puffy, often most prominently around the midfoot or the ankle. Swelling that doesn't go down overnight is more concerning than swelling that resolves after sleep.
- Redness. The affected foot has a reddish or pink discoloration that may extend partway up the leg. The redness often fades when the foot is elevated above heart level for several minutes and returns when the foot is dependent.
- Mild discomfort, not severe pain. This is the most important diagnostic clue and the one that misleads patients and clinicians alike. The pain is less than you would expect for the swelling and warmth. Many patients describe a vague ache or a sense of fullness rather than sharp pain. Severe pain points more toward infection or vascular problems; mild pain with major warmth and swelling in a diabetic foot points toward Charcot.
- No clear injury history. Patients usually cannot recall a specific moment when something happened.
If you are a person with diabetic neuropathy and you notice these signs in one of your feet, the rule that podiatrists and endocrinologists teach is simple and absolute: a warm, swollen, red foot in a diabetic with neuropathy is Charcot foot until proven otherwise. Not maybe Charcot. Not probably something else. Charcot until proven otherwise. That phrasing exists because the cost of delay is so high.
What you do next depends on access, but it does not depend on whether the symptoms seem bad enough to warrant the trouble. The answer is yes. Always.
What to Do If You Notice the Signs
Three actions, in order.

The 3 Actions That Save Feet
First, get off the foot. Stop walking on it. Use a chair, a couch, a bed. If you must move, use a walker or crutches that keep the affected foot from bearing weight. This is not optional and it is not “see how it feels tomorrow.” Every additional hour of weight-bearing on a foot in early Charcot adds to the damage. The single most important treatment for early Charcot foot is mechanical: stop loading it.
Second, get evaluated this week. Not next month. Not at your next regular appointment. This week. Call your podiatrist or your primary care doctor and use the words “I have a warm, swollen, red foot and I have neuropathy. I'm worried about Charcot foot.” Those specific words tend to move you up the schedule because every clinic-staff person trained in diabetic care recognizes the urgency. If you cannot reach your usual doctors, an emergency department visit is appropriate.
Third, advocate for proper imaging if the first X-ray looks normal. Stage 0 Charcot foot is often invisible on a standard X-ray. The bones haven't fragmented yet. An MRI of the foot is the test most likely to catch the condition at the earliest, most treatable stage. If your clinician orders an X-ray that comes back unremarkable and is ready to send you home with “probably a sprain,” it is reasonable to ask, politely but firmly, whether an MRI is appropriate given the diabetes, the neuropathy, and the asymmetric warmth.
The Conditions Charcot Foot Gets Confused With
Part of why Charcot foot is missed so often is that several common conditions look similar at first glance. Each one is worth ruling in or out, and most of them require treatments that are completely different from what Charcot foot needs.
Cellulitis — a bacterial skin infection — also produces warmth, redness, and swelling. The differentiating clues: cellulitis usually hurts more, often comes with fever or chills, has redness that does not significantly fade with elevation, and may have a visible entry point such as a wound or a crack between the toes. Treatment is antibiotics. The trouble is that Charcot foot patients sometimes have a foot ulcer too, and a foot can have both cellulitis and Charcot at the same time.
Deep vein thrombosis (DVT) — a blood clot in a deep vein — produces leg swelling, sometimes with warmth and redness. DVT is usually evaluated with a Doppler ultrasound, which is fast, painless, and widely available. A negative ultrasound rules it out reasonably well.
Gout — a crystal arthritis — produces severe pain, redness, and warmth, classically at the base of the big toe. Gout usually hurts a lot more than Charcot foot at presentation. A serum uric acid level and sometimes joint fluid analysis help confirm.
Ankle sprain — soft-tissue injury — has a clear injury history, sharp pain at the time of injury, and predictable location of tenderness. The mismatch between the visible swelling and the patient-reported pain is much less than in Charcot foot.
If your initial evaluation focused on one of these and did not produce a clear diagnosis, please go back. The default assumption in a diabetic foot with persistent warmth, swelling, and redness — without a clearly identified alternative cause — should be Charcot foot.
The Stages, So You Know What Doctors Are Talking About
Charcot foot is traditionally described in stages based on a system developed by Dr. Sidney Eichenholtz. Knowing the stages helps you understand what your specialists are seeing on imaging and what treatments are appropriate.
Treatment requires three to six months of casting on average — sometimes nearly a year. The duration shocks most patients, but the offloading is what stops the bone destruction. Patients who follow the cast schedule strictly have dramatically better outcomes than those who shorten it.
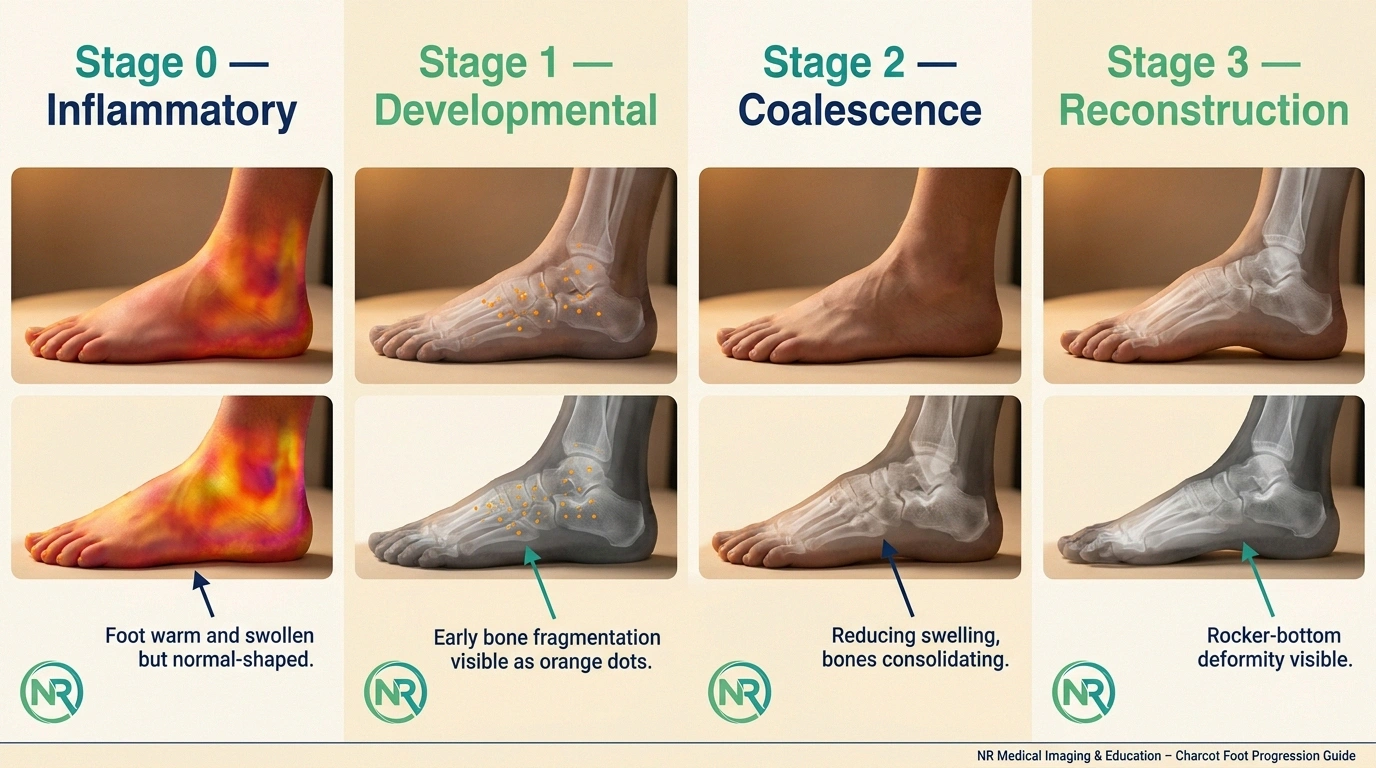
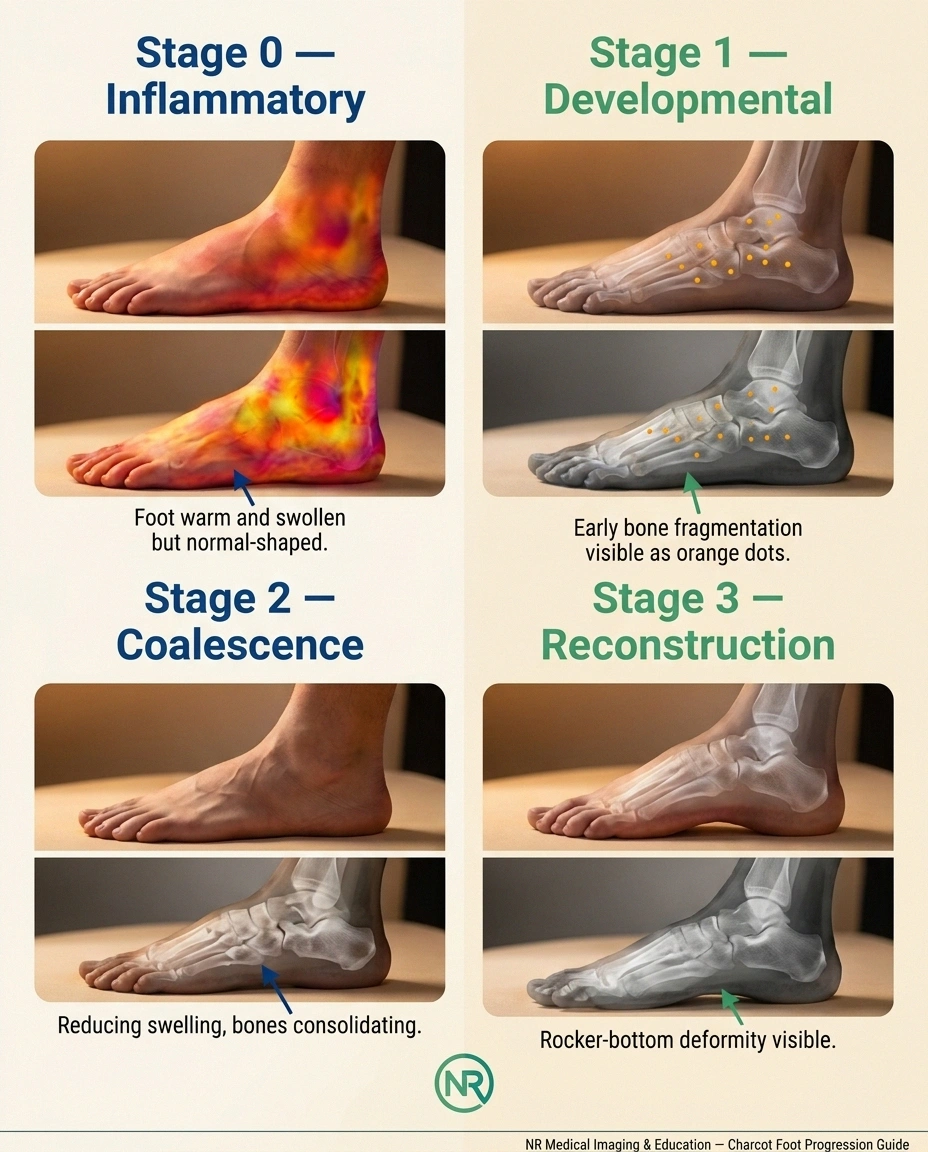
- Stage 0 — Pre-Charcot or Inflammatory Stage. The foot is warm, swollen, and red. X-rays may look normal. MRI shows bone marrow edema — microscopic injury within the bone. This is the most treatable stage. Aggressive offloading can stop progression before visible bone destruction.
- Stage 1 — Acute or Developmental Stage. Bone fragmentation is visible on X-ray. Joints may be dislocating. The foot remains warm and swollen. Offloading at this stage can still preserve foot shape, though some change is usually permanent.
- Stage 2 — Coalescence or Subacute Stage. Swelling decreases. Bone fragments begin to fuse and consolidate. The foot is becoming more stable but the shape is being set.
- Stage 3 — Reconstruction or Chronic Stage. The foot is no longer warm. The bones have healed in their new positions. The classic “rocker bottom” deformity, if it's going to develop, is visible by now. The foot is stable but often misshapen, vulnerable to ulceration where bone protrudes against the inside of the shoe.
The arithmetic of these stages explains why early recognition matters so much. A Stage 0 foot caught and offloaded promptly often returns to a near-normal shape. A Stage 3 foot is locked into whatever deformity has developed, and the patient lives with the consequences for the rest of their life.
Treatment: The Long Months in a Cast
The foundation of Charcot foot treatment, regardless of stage, is mechanical offloading. The most common approach is something called a total contact cast — a custom-fitted cast that conforms closely to the entire foot and lower leg, distributing pressure across the whole surface rather than concentrating it on injured areas. Total contact casts are changed every one to two weeks initially, then less frequently as the foot stabilizes.

The duration of casting is longer than most patients expect. Typical Charcot foot treatment runs eight to twelve weeks minimum, frequently extending to three or six months. Some patients spend nearly a year in some form of cast or boot. The endpoint is determined by clinical signs — the warmth and swelling resolving — and by imaging showing bone healing.
As the foot moves into later stages, a custom brace called a Charcot Restraint Orthotic Walker, often called a CROW boot, replaces the cast. A CROW boot is a removable, hard-shelled boot that protects the foot during weight-bearing while allowing the patient to take it off for hygiene and skin checks.
Long-term management almost always includes custom shoes. The reshaped Charcot foot does not fit standard footwear safely. Custom diabetic shoes with deep toe boxes, accommodative insoles, and sometimes added support structures distribute pressure and prevent ulceration over the prominent bones that develop.
Surgery enters the picture in a minority of cases — when conservative treatment has failed, when ulcers won't heal because of severe deformity, when the foot is grossly unstable, or when amputation is being considered. Reconstructive surgery for Charcot foot is complex and is typically performed by a foot and ankle surgeon with specific experience in this condition. Outcomes vary; the decision to operate is rarely simple.
Why Daily Foot Temperature Checks Matter
Of all the practical things I have learned writing about diabetic neuropathy, the daily home foot temperature check is one of the highest-leverage habits I know of. The principle is simple. Buy an inexpensive infrared thermometer — the kind sold for checking children's foreheads or food temperatures works fine. Each morning, measure the temperature on the top of each foot at the same location, with the same technique. Write the numbers down. Compare them.
A consistent temperature difference of more than four degrees Fahrenheit between the two feet is a warning sign. Research has shown that this kind of asymmetric warming often precedes a visible Charcot episode by days or weeks. If you catch the warming before the foot looks obviously different, you have bought yourself precious time to get evaluated while the damage is still minimal.
This habit is especially worth the small effort for patients who have already had one Charcot episode in either foot. Recurrence — either in the same foot or the other one — is a real risk, and the early-detection approach is the most reliable defense.
Living With a Charcot Foot After Treatment
The patients I have known who came through Charcot foot well share a few common practices. They keep their diabetes control as steady as it can reasonably be. They get their feet examined by a podiatrist at least quarterly, sometimes monthly. They wear their custom shoes consistently — not just for going out, but at home and on quick errands too. They never walk barefoot indoors. They check their own feet visually every single day, often using a small mirror to see the bottoms. They have a low threshold for calling their doctor if anything changes.

Skip the routine appointment and go to the emergency room for any of these:
- Open wound with red streaking up the leg, fever, or pus
- Any black or dead-looking tissue, regardless of pain
- Sudden severe pain in a previously numb foot
- Foot shape changing dramatically in days
- Foul-smelling or visibly contaminated wound
The patients who do less well tend to share a different set of habits. They take off the custom shoes at home. They walk barefoot to the bathroom at night. They skip the daily foot check because they “know” their feet. They wait to schedule appointments when something seems wrong. They downgrade their podiatry visits to “as needed.” They lose track of small changes until those changes become big problems.
I am not saying this to lecture. I am saying it because I have watched both groups over the years, and the difference in outcomes is striking. Charcot foot is the kind of condition where the small habits genuinely matter. The patients who treat them as non-negotiable do better.
When to Skip This Article and Go to the Emergency Room
A few signs in a foot of a diabetic patient with neuropathy are emergencies, not appointments-for-next-week:
- An open wound with redness streaking up the leg, fever, or pus
- Any black or dead-looking tissue, regardless of pain
- Sudden severe pain in a previously numb foot
- A foot that has changed shape dramatically in days
- A wound that is foul-smelling or visibly contaminated
- Inability to bear weight at all when you previously could
These are limb-threatening signs and need same-day emergency evaluation. Charcot foot itself is an urgent outpatient situation, not a 911 situation — but the infections and vascular complications that can accompany it absolutely are.
The Story I Want You to Tell Differently
When the woman from our support group described her warm, slightly swollen foot that she had walked on for three weeks, she did not know about Charcot foot. Nobody in her circle had ever mentioned it. By the time her diagnosis was made, the moment for prevention had passed and the conversation was about managing the deformity that was already forming.
I am telling you about this so that, if it happens to you, the story has a different ending. A warm, swollen foot in a diabetic with neuropathy is not a sprain you walk off. It is not something you wait out. It is the earliest version of one of the most preventable serious complications of your disease, and the action that stops it is simple and available: get off the foot, get to a doctor this week, and ask specifically about Charcot foot.
That conversation, started early, has saved many feet. I hope yours is one of them.
Frequently Asked Questions
What does Charcot foot look like in the early stages?
Early Charcot foot — Stage 0 — looks like a warm, swollen, mildly reddened foot in a person with diabetic neuropathy. The skin temperature on the affected side is noticeably higher than the other foot. Swelling typically does not resolve overnight. Discomfort is often mild relative to how the foot looks, and there is usually no clear injury history. At this stage, an X-ray may appear normal; MRI is the most sensitive test for catching the condition before bone fragmentation begins.
Is Charcot foot reversible?
The earliest stage of Charcot foot is largely reversible if recognized and offloaded promptly — meaning the foot returns to nearly its original shape and function. Once visible bone fragmentation has begun, complete reversal becomes impossible, but progression can usually be halted with proper treatment. Late Charcot foot, with established deformity, is not reversible; the goal at that stage shifts to stabilizing the foot in its new shape and preventing ulceration over bony prominences.
What causes Charcot foot?
Charcot foot develops when severe neuropathy meets ongoing weight-bearing on an injured foot. The patient cannot feel the small fractures or strains that occur, keeps walking, and the damage progresses. Altered blood flow from autonomic neuropathy and accelerated bone resorption in diabetes contribute as well. The most common underlying condition is long-standing diabetes with neuropathy, but Charcot foot can develop in anyone with significant sensory loss in the feet — from leprosy, alcoholic neuropathy, syphilis, or hereditary neuropathies.
How long does Charcot foot take to heal?
Most patients spend three to six months in some form of cast or immobilizing boot during the active phase of Charcot foot. Some patients require closer to a year of immobilization. Bone healing on imaging is the most reliable signal for transitioning out of casting. After active healing, lifelong use of custom shoes is typically required to protect the reshaped foot and prevent ulceration.
Can you walk on a Charcot foot?
You should not. Continuing to bear weight on a Charcot foot accelerates the destruction and makes the eventual deformity worse. During the active phase, the foot must be immobilized in a total contact cast and weight kept off it as completely as possible. After healing, walking returns gradually in protective footwear. Walking barefoot or in poorly protective shoes on a healed Charcot foot is one of the surest ways to develop ulcers and start the cycle over again.
What is the difference between Charcot foot and cellulitis?
Cellulitis is a bacterial skin infection that produces warmth, redness, and swelling. It tends to be more painful, often comes with fever, and may have a visible entry point such as a small wound or cracked skin. Cellulitis redness does not fade significantly when the foot is elevated. Charcot foot is bone and joint destruction, produces less pain than expected for its appearance, often has no fever, and the redness frequently fades with several minutes of elevation. The two conditions can coexist, which is why proper evaluation by a physician is essential.
Does Charcot foot always lead to amputation?
No. With early recognition, prompt offloading, and consistent long-term foot care, most patients keep their feet. Amputation rates in published series of Charcot foot patients are roughly fifteen percent, occurring mostly in patients with late diagnosis, severe deformity, recurrent ulceration, or significant vascular disease in addition to neuropathy. The single most powerful predictor of keeping the foot is how early the condition is caught and how strictly the offloading protocol is followed.
What kind of doctor treats Charcot foot?
Podiatrists with experience in diabetic foot care are the most common primary providers for Charcot foot. Foot and ankle orthopedic surgeons are often involved, especially when reconstructive surgery is considered. Endocrinologists or primary care doctors manage the underlying diabetes alongside the foot specialist. For complex or recurrent cases, multidisciplinary diabetic foot centers — staffed by podiatrists, surgeons, wound care nurses, and prosthetists working together — provide the highest level of care.


