
You sit down for dinner. The first bite of food touches your tongue. Within seconds, the sweat starts. It's not on your back or your chest — it's on your face, your forehead, your neck. By the time you've finished a plate of pasta, you've blotted your brow three times and you're hoping no one across the table noticed. Then it stops. Until the next meal.
This is gustatory sweating. It's strange, it's embarrassing, and for many people who have it, no one has ever named it for them. They've spent years assuming they're just “a sweater” or that something is wrong with the food. The truth is more specific. Gustatory sweating is a known sign of autonomic nerve damage — most often from diabetes, but also from a handful of other conditions — and once you understand what's happening, the path forward makes a lot more sense.
I want to walk through what gustatory sweating actually is, why it happens, why it shows up at one cheek or one side of the head sometimes and the whole face other times, and what your real options are. I'll also be honest about which treatments help most people and which ones get oversold.
What Gustatory Sweating Actually Is
Gustatory sweating, sometimes called “sweating while eating” or referred to under the older medical name Frey syndrome (for one specific type), is a condition where eating triggers visible, often profuse sweating on the face, scalp, or neck. The sweat typically appears within seconds of food entering the mouth. It can come from any food, but spicy, hot, sour, or strongly flavored foods tend to provoke it most.
Gustatory sweating is profuse facial, scalp, or neck sweating triggered within seconds of eating. It is not “being a sweater” — it is a sign of autonomic nerve damage, most often from long-standing diabetes or after parotid (salivary gland) surgery. Many people who have it also have reduced sweating on the feet and legs (anhidrosis) — the same nerve damage, different geography.
The medical term for it in the diabetes literature is gustatory hyperhidrosis. The name simply describes excessive sweating triggered by gustation — the act of tasting.
What makes it strange is the geography. Most people who have it sweat in places where they wouldn't normally sweat much — the forehead, temples, scalp, cheeks, upper lip, sometimes the neck. Meanwhile their underarms, back, and torso may sweat less than they used to. This odd geographic mismatch — sweating where you shouldn't, not sweating where you should — is the central clue that the autonomic nervous system is involved.
Why It Happens — The Autonomic Nervous System Backstory
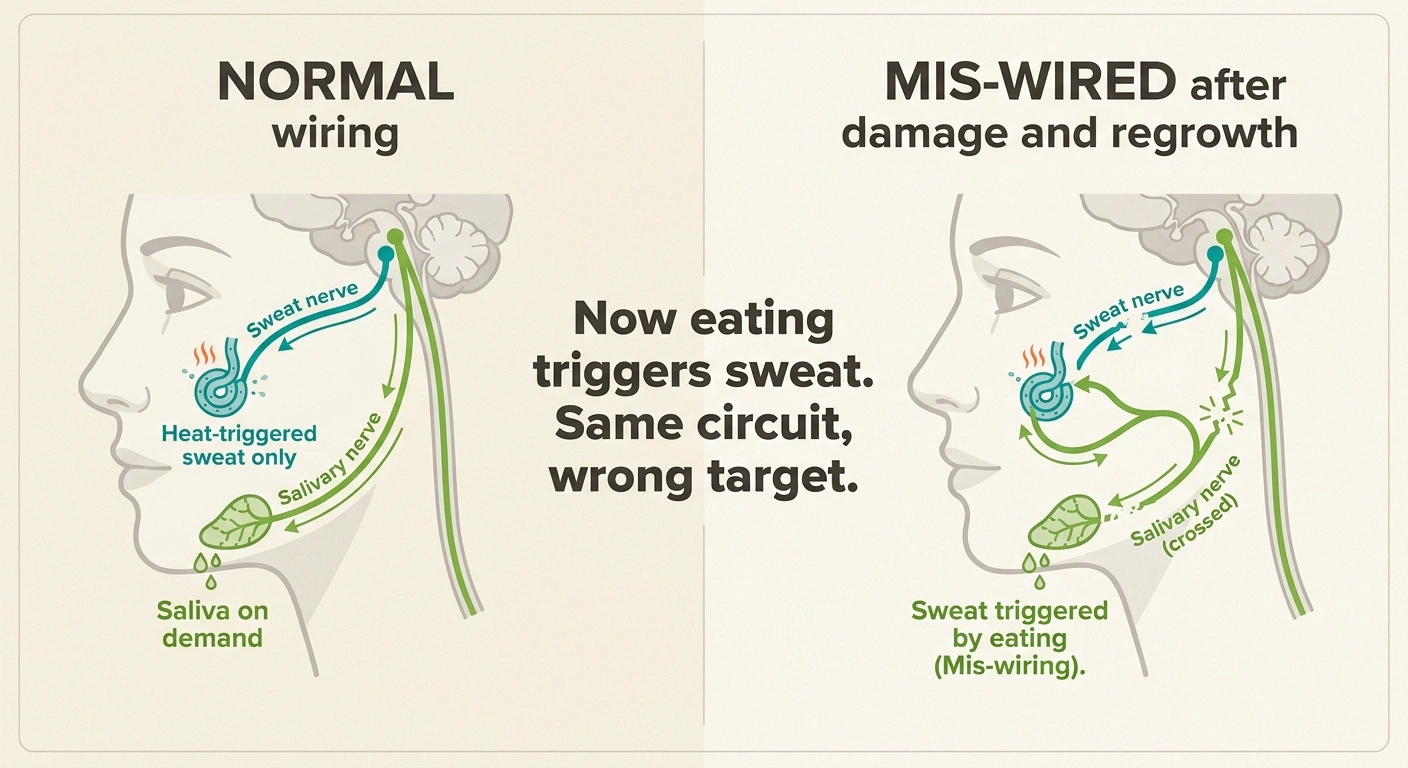
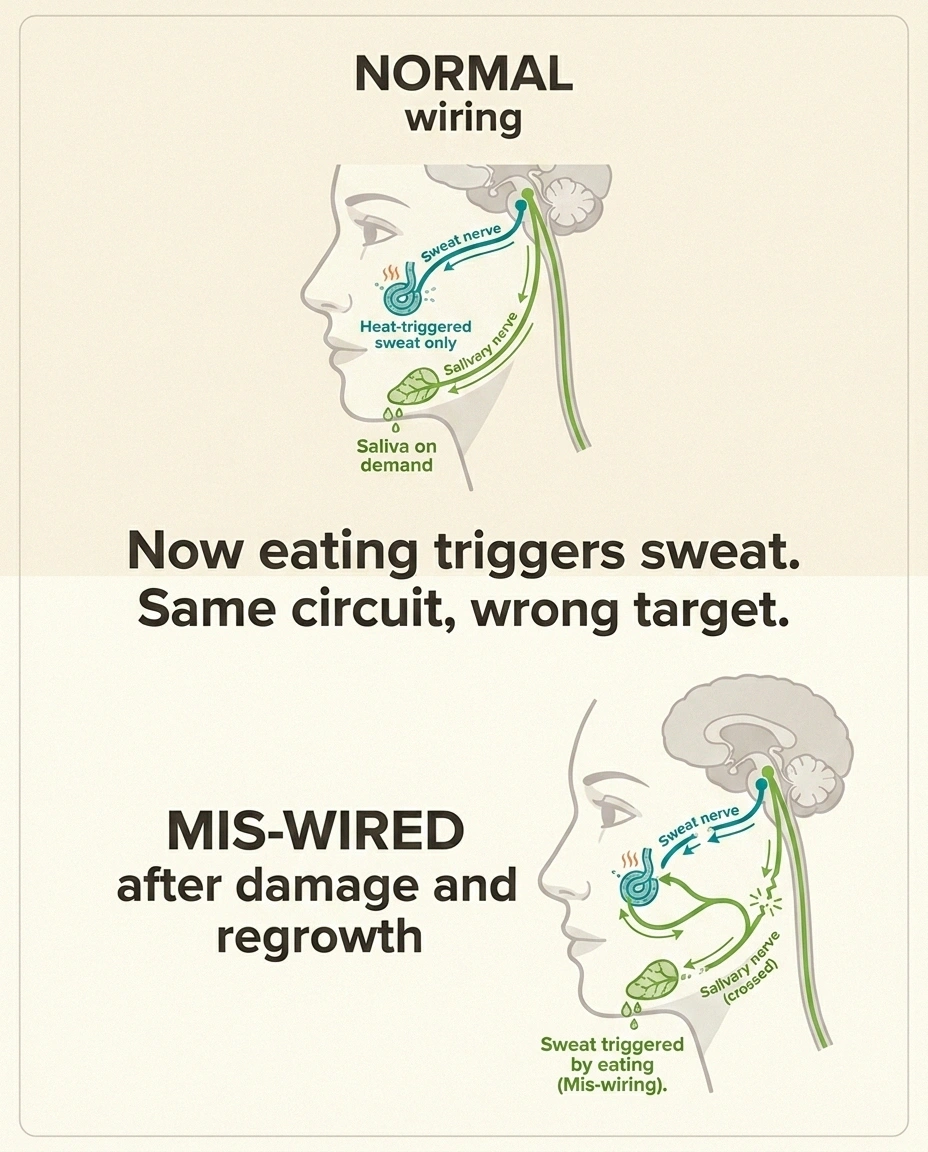
Your body's sweat glands are controlled by the sympathetic branch of the autonomic nervous system — the same wiring that controls your heart rate, blood pressure, digestion, and a dozen other “background” body functions. Normally, the nerve fibers going to your sweat glands stay quiet during eating. The nerve fibers going to your salivary glands fire actively during eating, which is why your mouth waters.
The mis-wiring story (aberrant regeneration):
- Autonomic nerve fibers controlling facial salivary and sweat glands get damaged
- As they regenerate, some fibers grow to the wrong target — a salivary-gland fiber ends up wiring into a sweat gland
- Now eating, which normally triggers saliva, also triggers sweat at the rerouted gland
- Result: instant sweat on the face the moment food enters the mouth
Same mechanism explains classical Frey syndrome after parotid surgery and diabetic gustatory sweating.
Now imagine that some of those autonomic nerve fibers get damaged. In diabetes — the most common cause of widespread gustatory sweating — small, unmyelinated autonomic fibers in many parts of the body slowly die off. The body, doing what it does, sometimes tries to repair. When the damaged nerves try to regrow, they don't always grow back to their original targets. Sometimes a regenerating fiber that was supposed to go to a salivary gland ends up wiring itself, by accident, to a nearby sweat gland.
Once that mis-wiring is in place, every time you eat — and the brain sends the normal “make saliva” signal — the rerouted nerve also triggers the sweat gland it accidentally connected to. That's why the sweat starts the moment food hits the mouth, not later. Your brain is asking for saliva. Your face is delivering sweat.
This is what neurologists call “aberrant nerve regeneration.” It's the same general mechanism behind Frey syndrome (which classically follows parotid gland surgery) and is increasingly understood as the explanation for diabetic gustatory sweating as well.
The Other Side of the Same Coin: Anhidrosis
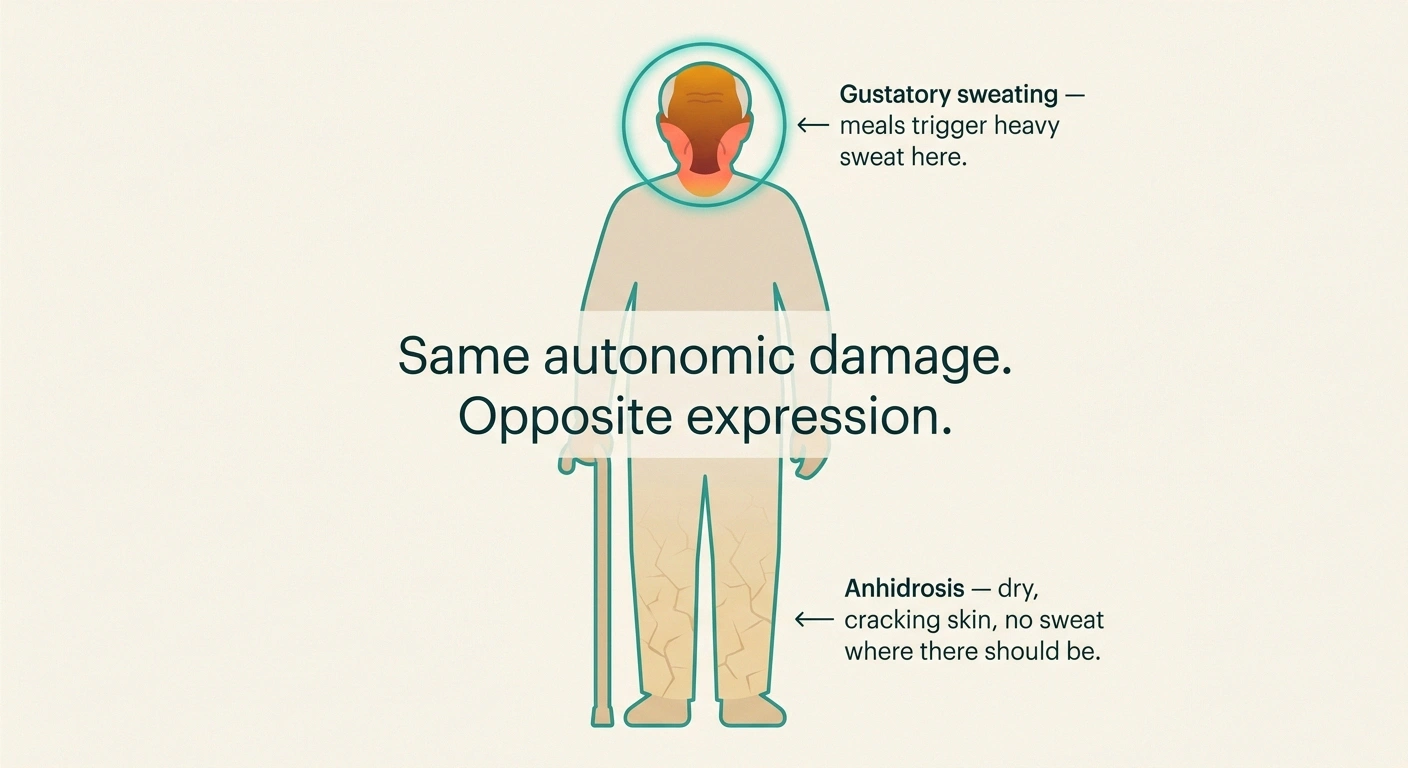
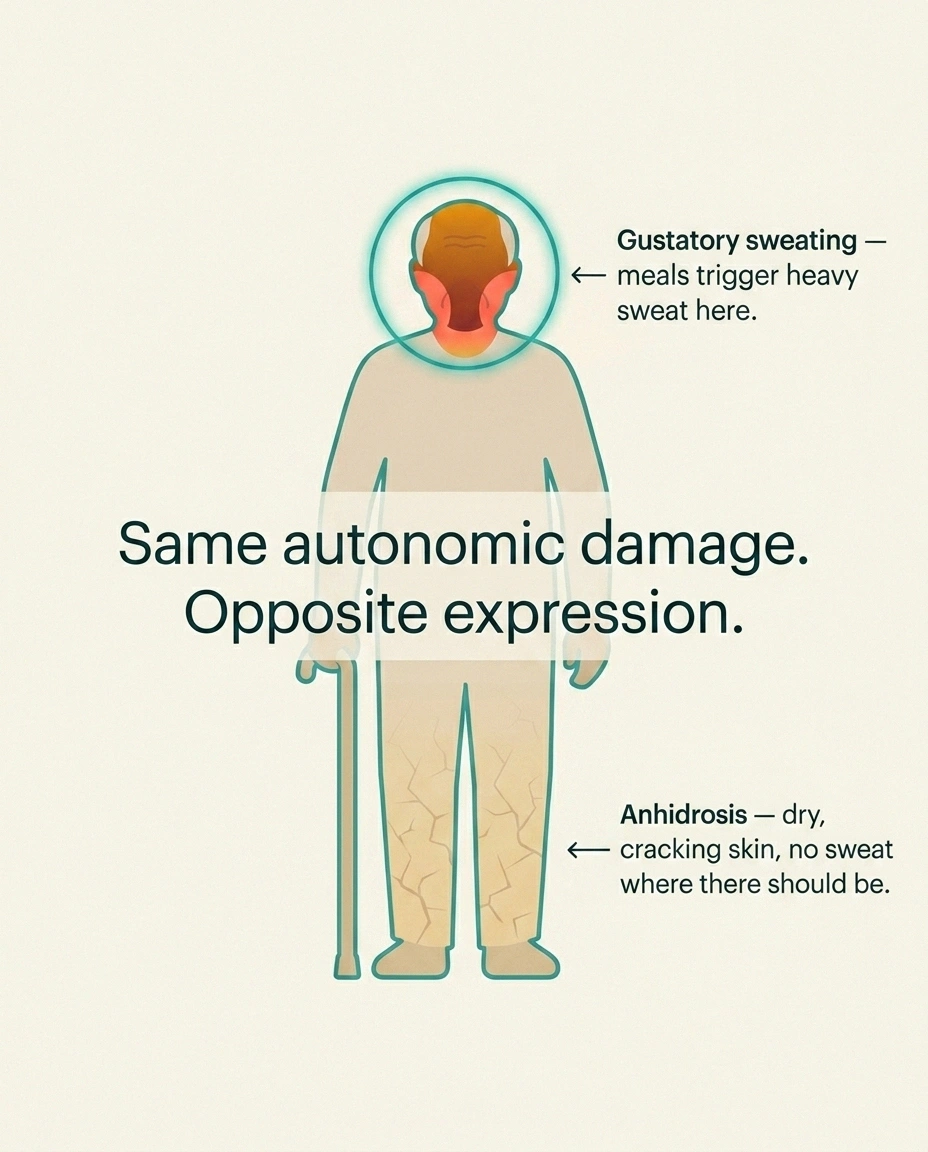
If gustatory sweating is the face turning on the sweat at the wrong time, anhidrosis — reduced sweating — is the body turning sweat off in the places it's needed. Both happen for the same reason: damage to the autonomic nerve fibers that control sweat glands.
Many people with gustatory sweating also have anhidrosis somewhere else on the body — often the feet, lower legs, and sometimes the lower torso. The skin in those areas may feel notably dry, crack easily, take a long time to heal, and never get the slick of sweat you'd expect after a hot day or hard exercise.
This combination — sweating where you shouldn't, not sweating where you should — is one of the most reliable signs of autonomic neuropathy. If you've noticed both, you're not imagining the contradiction. They share a single cause.
And the anhidrosis matters in a way the gustatory sweating doesn't, because dry skin on the feet is a setup for cracks, calluses, and infections — the same chain of problems that drives many of the worst diabetic foot complications. Anhidrosis is, quietly, one of the reasons daily foot care matters so much in people with longstanding diabetes.
Who Gets Gustatory Sweating
The two main paths to gustatory sweating are very different and worth distinguishing.
Diabetes-related (most common). Long-standing type 1 or type 2 diabetes, especially with other signs of autonomic involvement (silent heart-rate changes, dizziness on standing, gastroparesis, bladder issues). The sweating is usually bilateral — both sides of the face equally — and often involves the forehead, scalp, and neck. It tends to come on gradually over years and may worsen as autonomic neuropathy progresses.
Frey syndrome (rarer, surgical or traumatic). Sweating after parotid (salivary gland) surgery, facial trauma, or sometimes after radiation to the head and neck. Classically one-sided — affecting only the cheek and temple over the surgical area — because the nerve damage is local. Onset is usually within months to a couple of years of the surgery. The mechanism is the same aberrant regeneration, just in a smaller, more localized field.
Other less common causes. Some autoimmune autonomic neuropathies, certain spinal cord injuries, viral autonomic damage, and rare structural problems can produce gustatory sweating. These are uncommon enough that they shouldn't be the first thought, but they exist.
For most readers of this site, the conversation is about diabetes-related gustatory sweating in the broader context of diabetic neuropathy.
How It's Diagnosed

For most people, the diagnosis is clinical — meaning your doctor listens to your description, looks at the pattern, asks the right questions about diabetes and surgical history, and arrives at a confident answer without any test. The history is usually distinctive enough that gustatory sweating is rarely confused with general hyperhidrosis or hot flashes.
Some doctors will use a Minor's iodine-starch test for documentation — paint the area with an iodine solution, dust with starch, give the patient a strong-flavored food (lemon slice, cracker), and watch the iodine-starch turn blue-black where sweat appears. It's old technology but it works and gives a clear visual record.
If there's any doubt about whether the sweating reflects broader autonomic neuropathy, an autonomic test battery can be useful. This might include orthostatic blood pressure measurement (lying vs. standing), heart rate variability with breathing, the QSART test (quantitative sudomotor axon reflex testing) that directly measures sweat-gland function in the limbs, and a tilt table study in some centers. These tests can pin down whether autonomic neuropathy is broader than just the gustatory presentation.
For someone with diabetes and gustatory sweating, the more useful workup is often less about the sweating itself and more about catching other autonomic involvement — heart rate changes, blood pressure regulation, stomach motility, bladder function — that may need its own management.
Why It's More Than Just Embarrassing
It would be tempting to dismiss gustatory sweating as a social nuisance — a problem of restaurant napkins, not health. That misses something important.
The sweating itself is rarely dangerous. The autonomic neuropathy it points to often matters more than the sweating does. People with diabetic autonomic neuropathy have higher rates of cardiovascular events, more silent heart attacks, more falls from orthostatic blood pressure drops, more hospitalizations for dehydration and electrolyte imbalances, and a higher overall mortality risk than people with diabetes who don't have autonomic neuropathy.
The gustatory sweating is, in this sense, a signal flare. It's visible. It's distinctive. And it tells you and your doctor that the autonomic nervous system has accumulated enough damage to be doing strange things. That's a reason for a broader autonomic assessment, not a reason to just blot your face and move on.
This doesn't mean every person with gustatory sweating has serious autonomic disease. Some have a relatively focal, isolated finding. But the conversation worth having with your doctor is: “I'm sweating during meals on my face — should we be looking at the rest of my autonomic system?”
What Helps the Sweating Itself

Once the underlying autonomic neuropathy is identified and addressed (in diabetes, this means the standard work of blood sugar optimization, blood pressure control, and the broader neuropathy toolkit), the question of what to do specifically about the sweating becomes practical.
Trigger avoidance. The simplest first move. Most people can identify a handful of foods that consistently provoke heavier sweating — spicy foods, hot temperature foods, certain strong flavors, sometimes acidic ones. Cutting back on the worst offenders, especially in social settings, can substantially reduce the daily impact.
Topical antiperspirants. Standard over-the-counter and prescription antiperspirants (aluminum chloride) applied to the face or scalp can reduce gustatory sweating. The over-the-counter strengths often help; the prescription strengths (20% aluminum chloride hexahydrate, sold as Drysol or similar) work better but can irritate facial skin and are usually used carefully — at night, on dry skin, with petroleum jelly to protect sensitive areas around the eyes.
Topical glycopyrrolate (anticholinergic cream or wipes). Glycopyrrolate is an anticholinergic — it blocks the chemical signal (acetylcholine) that triggers the sweat gland. Topical formulations (a 1–2% cream or a 2.4% wipe, sold under names like Qbrexza) can dramatically reduce gustatory sweating on the area where they're applied. This is one of the most effective interventions for facial gustatory sweating specifically, and a dermatologist familiar with hyperhidrosis can prescribe it.
Oral anticholinergic medications. Drugs like oral glycopyrrolate (Robinul) or propantheline taken by mouth can reduce sweating throughout the body. They work, but the side effects — dry mouth, blurred vision, constipation, urinary retention, dizziness — limit their day-to-day use, especially in older patients who may already be sensitive to anticholinergic effects. They're worth considering for severe cases, not for everyday management.
Botulinum toxin injections (Botox). For severe localized gustatory sweating — especially classical Frey syndrome — botulinum toxin injections into the affected skin can reduce sweating for 6 to 12 months at a time. Botox blocks the nerve signal at the sweat gland directly. It's typically administered by a dermatologist or specialist in a grid pattern across the affected area. The procedure is straightforward but not painless, and insurance coverage varies depending on the cause and the documentation of severity.
Practical daily strategies. Keep absorbent handkerchiefs or small cotton cloths handy (more absorbent than restaurant paper napkins). Position yourself at meals where airflow is good. Choose cooler-temperature foods when in formal settings. Wear breathable fabrics. Stay well-hydrated — counterintuitively, dehydration can make the gustatory sweating feel worse because the body's overall thermoregulation is more strained.
What Probably Doesn't Help
It's worth being clear about the things that get suggested but don't have good evidence in gustatory sweating specifically.
Most over-the-counter “anti-sweat” supplements don't have meaningful effects on autonomic nerve-mediated sweating. The same goes for general herbal sage extracts that are sometimes marketed for hyperhidrosis. They may reduce overall thermoregulatory sweating modestly in some people, but they don't target the gustatory mechanism.
Iontophoresis — the electrical-water treatment for hands and feet — doesn't translate well to facial sweating both because of the impracticality and because the underlying nerve mechanism is different.
Diet changes beyond avoiding specific personal triggers haven't been shown to alter gustatory sweating. It's not a food sensitivity problem. It's a wiring problem.
Sympathectomy — surgery to cut sympathetic nerves — is occasionally raised but is rarely appropriate for gustatory sweating. It carries significant risks (including compensatory sweating elsewhere on the body, which can be worse than the original problem) and is generally reserved for severe palmar or axillary hyperhidrosis, not the gustatory presentation.
The Connection to Bigger Autonomic Issues
If you've come this far and gustatory sweating fits your experience, the most useful next step is often a wider conversation about autonomic function with your primary care doctor or endocrinologist (if diabetes) or neurologist.
Gustatory sweating + any of these = ask for autonomic testing:
- Lightheadedness on standing (orthostatic hypotension)
- Resting heart rate over 90 bpm or unusually steady (low variability)
- Early fullness, nausea, or unpredictable post-meal blood sugar (gastroparesis)
- Difficulty starting urination or recurrent UTIs
- Erectile dysfunction or vaginal dryness
- Glare sensitivity, trouble seeing at night
- Dry, cracking skin on the feet (anhidrosis) — foot infection risk
Worth asking about:
- Orthostatic hypotension. Have you noticed lightheadedness or dizziness when standing up from sitting or lying down? Blood pressure should be measured both sitting and immediately after standing — a drop of 20 mm Hg systolic or 10 mm Hg diastolic suggests autonomic involvement.
- Resting heart rate. Has your resting heart rate crept up? Autonomic neuropathy often produces a higher-than-expected resting heart rate (over 90 bpm) with reduced variability.
- Gastroparesis. Are you feeling unusually full after small meals, having unpredictable blood sugar after eating, experiencing nausea? Slowed stomach emptying is a common autonomic finding.
- Bladder symptoms. Difficulty starting urination, incomplete emptying, urinary tract infections?
- Sexual dysfunction. Erectile dysfunction or vaginal dryness can have autonomic-neuropathic origins.
- Pupil response. Poor adaptation to changing light, glare sensitivity, difficulty driving at night?
Any cluster of these alongside gustatory sweating is a reason for proper autonomic testing and a thoughtful management plan that goes beyond just the cosmetic sweating.
What I'd Tell a Friend
If a friend told me they were sweating heavily on their face every time they ate, here's what I'd say. First, this is a known thing. You're not making it up, and you're not alone — it's well-documented in people with long-standing diabetes and after certain surgeries. Second, the sweating itself is treatable. There are real options, from antiperspirants to topical glycopyrrolate to Botox, and most people get meaningful relief with one or two of them. Third — and this is the part most people miss — the sweating is a signal worth following. Your autonomic nervous system is doing something measurable, and that's worth your doctor's attention even if the sweating is your only symptom.
You don't need to live with it as a permanent feature of every meal. You also shouldn't write it off as just an embarrassing quirk. It's specific, it's nameable, and it has a story behind it that fits into the larger picture of how your nerves are doing.
That, in the end, is the most useful thing about understanding gustatory sweating. It's a reminder that the body sends signals even when nothing visible is wrong yet. The trick is learning to read them.
Frequently Asked Questions
Is gustatory sweating a sign of diabetes? It can be a sign of long-standing diabetes with autonomic involvement, particularly in people with type 1 or longer-duration type 2 diabetes. It is not typically an early sign — gustatory sweating tends to appear after years of diabetes when other autonomic features (resting tachycardia, orthostatic changes, gastroparesis) are also developing. In someone without known diabetes who develops gustatory sweating, it is reasonable to check fasting glucose and an A1C to rule out undiagnosed diabetes, but other causes should also be considered.
Why does my face sweat but my body doesn't? This is the classic pattern of autonomic neuropathy with mis-wired regeneration. Damaged sympathetic nerves that should reach sweat glands in the trunk and legs can die off, while regenerating fibers in the head and neck can accidentally connect to facial sweat glands and get triggered by eating signals instead of heat signals. The result is dry skin on the legs and feet alongside heavy sweating on the face during meals.
Can gustatory sweating be reversed? The underlying nerve damage is usually not reversed once it's established, but the sweating itself can be substantially reduced with topical treatments, antiperspirants, glycopyrrolate, or Botox. In some cases of newer-onset gustatory sweating with good diabetes control, the sweating may stabilize or even improve modestly over years, though this is less common than persistent or progressive symptoms.
Does Botox really work for gustatory sweating? Yes, for many people. Botulinum toxin injected into the affected facial or scalp area blocks the chemical signal at the sweat gland and can dramatically reduce sweating for 6 to 12 months per treatment. It is particularly effective for localized Frey syndrome after parotid surgery and can also help diabetic gustatory sweating when other approaches fall short. Treatment is typically done by a dermatologist or specialist familiar with hyperhidrosis protocols.
Is it normal to sweat from spicy food? A modest amount of facial flushing and light sweating in response to capsaicin (spicy food) is normal in everyone — that's a vasodilation response, not autonomic neuropathy. What is not normal is profuse, drenching sweating from any food, including bland foods, that starts within seconds of eating and centers on the forehead, cheeks, and scalp. That pattern points to gustatory sweating from autonomic nerve involvement.
Can gustatory sweating be one-sided? Yes, particularly after parotid gland surgery or trauma on one side of the face. This is the classic Frey syndrome pattern. One-sided gustatory sweating in someone without a surgical history should still prompt a careful look for a localized cause, including a thoughtful neurological exam. Diabetes-related gustatory sweating, in contrast, is typically symmetric across both sides of the face.
What deodorant or antiperspirant works best for facial sweating? The most effective over-the-counter options contain aluminum chloride. For more significant gustatory sweating, dermatologist-prescribed strengths (such as 20% aluminum chloride hexahydrate) or topical glycopyrrolate wipes are usually more effective than retail antiperspirants. Use on dry skin, often at night, and avoid the eye area. Many people find a combined approach — an antiperspirant for daily use and reserving glycopyrrolate or Botox for special occasions — works best.
Should I see a neurologist for gustatory sweating? A neurologist is a reasonable referral if the sweating is severe, if there are other signs of autonomic neuropathy (lightheadedness on standing, slow stomach emptying, bladder symptoms), if the diagnosis is unclear, or if you want formal autonomic testing. For someone with known diabetes and isolated mild gustatory sweating, the conversation can often start with your primary care doctor or endocrinologist, who can refer to neurology or dermatology as needed.


