
If you're dealing with weird, burning, or stabbing sensations in your foot and you've landed here, the first useful question to ask yourself is this: is it one spot in one foot, or is it both feet, like a sock?
That single question separates two conditions that often get tangled together — Morton's neuroma and peripheral neuropathy. They feel similar from inside. They share words like burning, tingling, numbness, and electric. But they're different problems, with different causes, different specialists, and different treatments. Sorting them out matters because following the wrong path means months of treatment aimed at the wrong target.
I want to be honest up front: telling them apart from the couch is hard, and this article is not a self-diagnosis tool. What I can do is give you the cleanest distinguishing signals, walk you through what each condition actually is, name the (real) overlap when both are present, and route you to the right kind of doctor with the right questions. That last part is where most articles let you down.
Quick Differential at a Glance
Before we go deep, here's the compressed picture. If you only read one section, read this.
Morton's neuroma is a focal nerve problem in the ball of one foot — usually one specific spot between the third and fourth toes. It's mechanical. It hates tight shoes and weight on the ball of the foot. It loves taking the shoe off and rubbing the spot. It's almost always one-sided. Pain quality is sharp, electric, “walking on a marble” or “stepping on a bunched-up sock.”
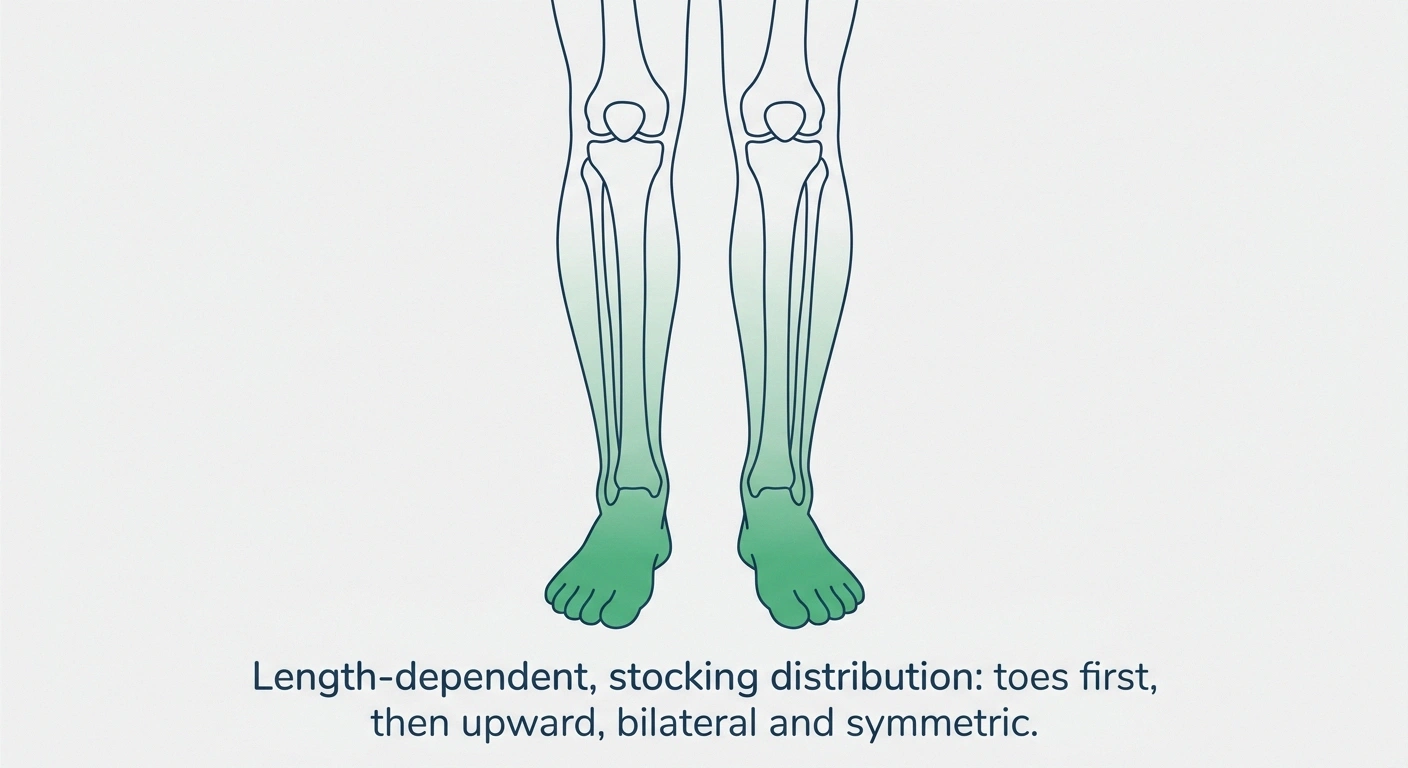
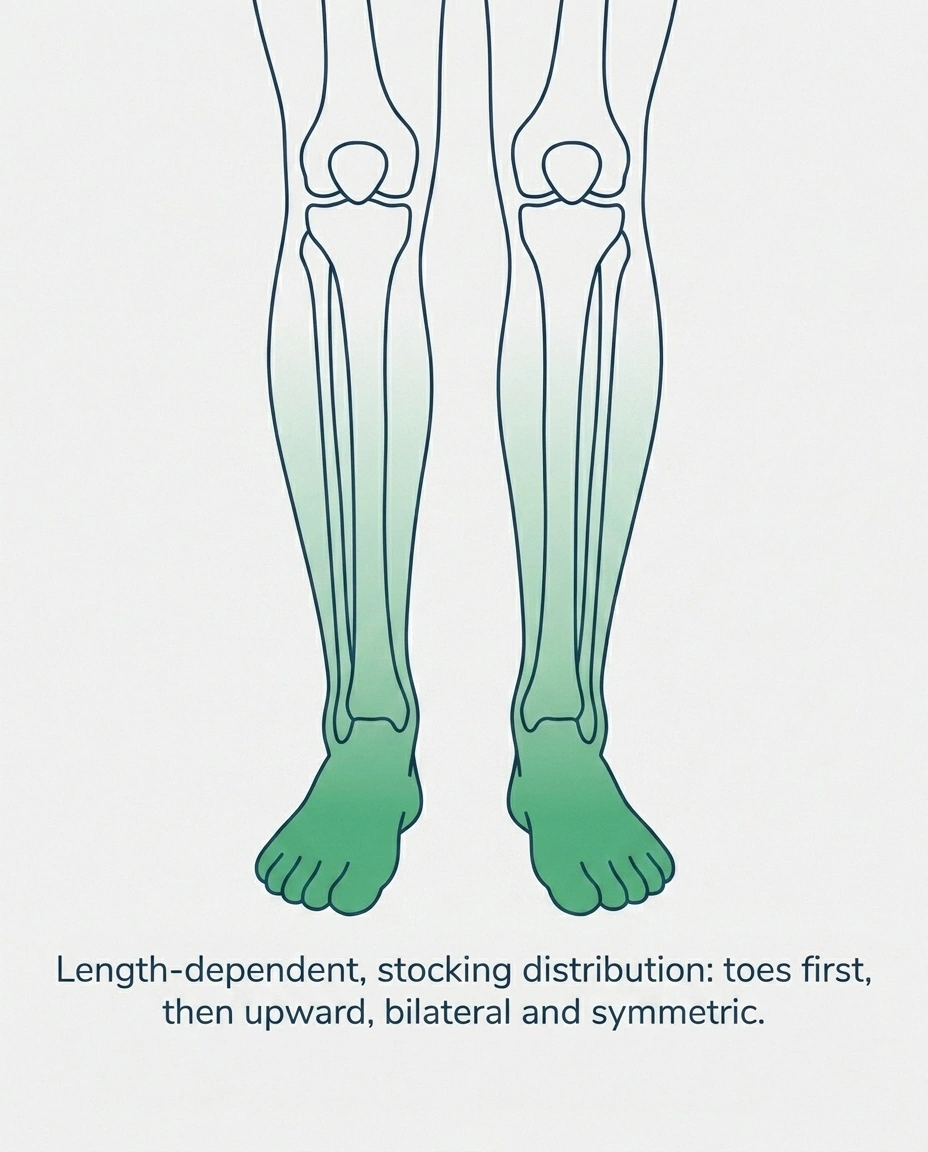
Peripheral neuropathy is a systemic nerve problem. It's almost always both feet, with a stocking-pattern distribution — toes first, then forefoot, then up the ankles and calves. It creeps in over months or years. It often doesn't care what shoes you wear. It can be worse at night, when you're lying still. Pain quality is burning, tingling, pins-and-needles, sometimes numbness, sometimes a “walking on cotton” disconnect from the floor.
The mechanical-versus-systemic distinction is the big one. Morton's neuroma comes from physical pressure on a specific nerve. Peripheral neuropathy comes from something affecting nerves throughout the body — diabetes, vitamin deficiency, chemotherapy history, alcohol, thyroid, autoimmune disease, or unknown causes. Different conditions, different evaluations, different fixes.
What Morton's Neuroma Actually Is
Morton's neuroma is technically not a tumor, despite the “-oma” ending that suggests one. It's a thickening of the tissue around one of the interdigital plantar nerves — the nerves that run between your metatarsal bones and supply sensation to your toes. The nerve itself develops perineural fibrosis (scar-like tissue) from chronic compression and irritation. The thickened bundle then sits in a tight space between two metatarsal heads and gets squeezed every time you bear weight on the ball of your foot or wear a narrow shoe.
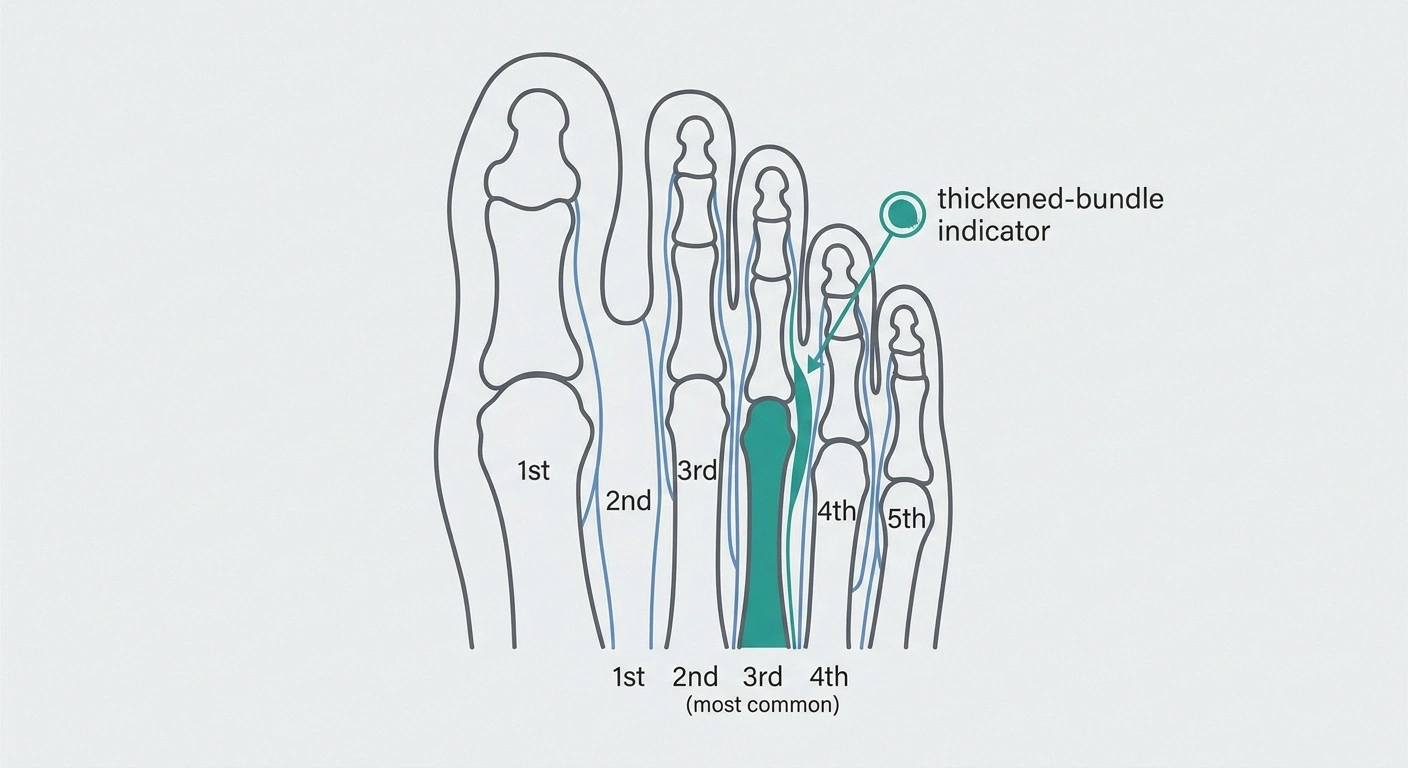
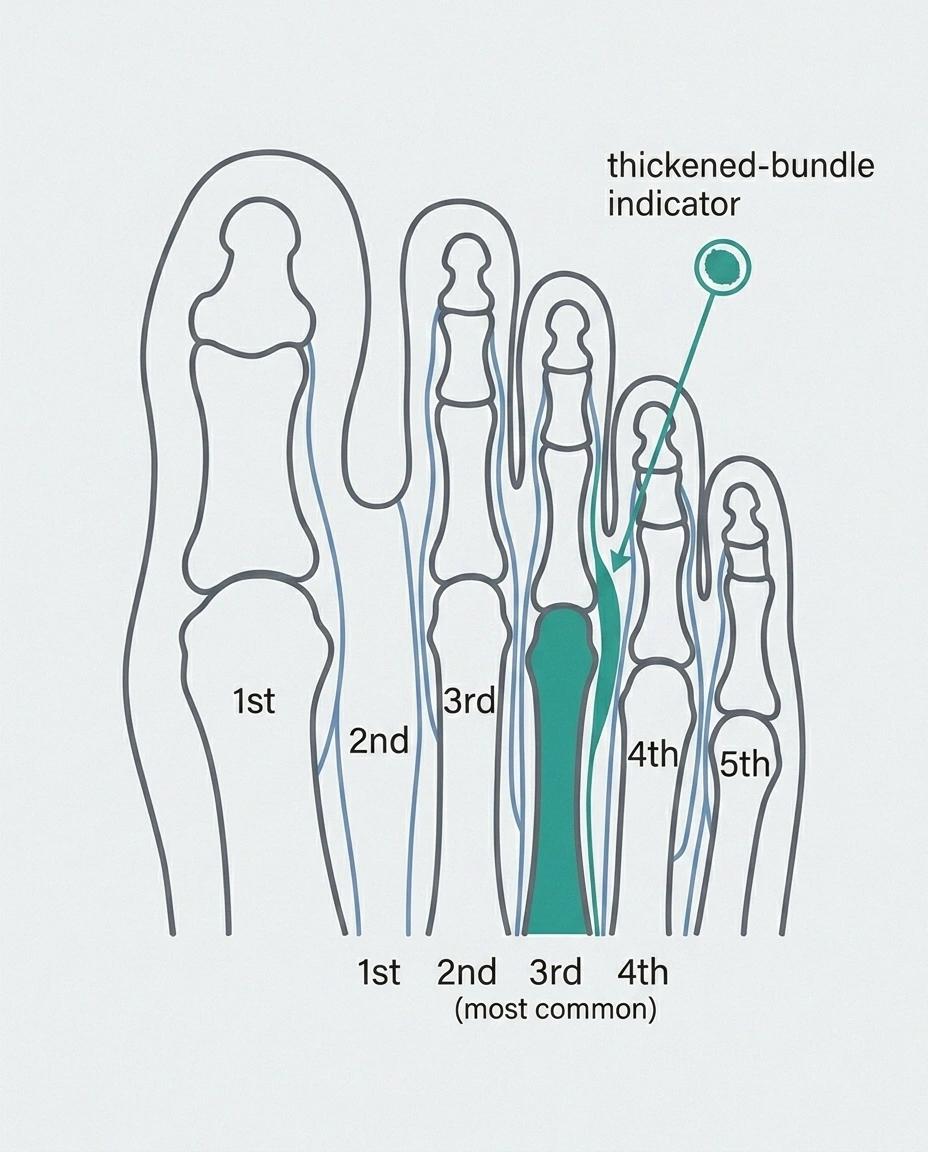
The condition has a strong location preference: the third interspace, between the third and fourth toes, is by far the most common site. There's an anatomical reason for this. The plantar nerve there receives a contribution from two sources, making the bundle larger than average, and the space it sits in is narrower than the neighboring interspaces. The combination — bigger nerve, smaller space — sets up perfect conditions for compression.
The classic Morton's neuroma patient is a middle-aged woman. Women are about five times more likely than men to develop it, partly because of footwear patterns (narrow toe boxes, heels), partly because of anatomy. People who run or do high-impact exercise, people who stand for long stretches on hard floors, and people whose work requires tight shoes are all at elevated risk.
The sensations are distinctive once you've heard them described. The most common complaint is a sharp, burning, or electric pain in the ball of the foot, often radiating into the third and fourth toes. Many people describe a feeling like there's a marble, a pebble, or a bunched-up sock under the front of their foot. Numbness in the affected toes is common, though less universal than pain. The pain dramatically worsens with tight shoes, running, prolonged standing, or any prolonged weight-bearing — and it dramatically improves when shoes come off, when the foot is rubbed, or when the toes are spread apart.
One thing worth knowing about Morton's neuroma: it doesn't resolve on its own. Symptoms can flare and settle, and conservative treatment can dramatically reduce or eliminate pain, but the underlying nerve thickening doesn't reverse without intervention or sustained pressure relief.
What Peripheral Neuropathy Actually Is
Peripheral neuropathy is a much broader category — really a family of conditions in which the peripheral nerves (the nerves outside the brain and spinal cord) are damaged or functioning poorly. Most adults who develop peripheral neuropathy have a length-dependent sensory or sensorimotor version, which means the longest nerves in the body get hit first. Since the longest nerves are the ones supplying your feet, that's where symptoms start. Over time the symptoms can creep up the legs and eventually reach the hands.
- Focal compression of one interdigital nerve
- Usually 3rd interspace (between toes 3 and 4)
- One foot, almost always
- Mechanical — tight shoes, weight on ball of foot
- Marble or pebble sensation in shoe
- 5× more common in women
- Systemic damage to many nerves
- Length-dependent — longest nerves first (feet)
- Both feet, symmetric
- Systemic — diabetes, B12, chemo, alcohol, thyroid, idiopathic
- Burning, tingling, numbness across stocking distribution
- Often worse at night, present at rest
The stocking-and-glove distribution — symptoms in the parts of your body that a sock or a glove would cover — is the classic pattern. Bilateral and symmetric. Both feet, both hands eventually. For more on this pattern in detail, our overview of neuropathy in feet covers what readers often recognize from their own experience.
The causes are many. Diabetes is by far the most common — diabetic peripheral neuropathy affects roughly half of long-standing diabetics. Other major causes include vitamin B12 deficiency, certain chemotherapy drugs (especially platinum-based agents and taxanes), heavy alcohol use, thyroid disease, autoimmune conditions, infections like Lyme and shingles, and a meaningful number of cases that remain idiopathic despite full workup. Our piece on types of neuropathy explained walks through the full landscape.
The symptoms vary by what kind of nerve fibers are affected. Large-fiber neuropathy tends to produce numbness, balance problems, loss of vibration sense, and a “walking on cotton” disconnect from the floor. Small-fiber neuropathy tends to produce burning, electric, pins-and-needles, sometimes itching or sunburn-like sensations. Most people with neuropathy have a mix.
Two patterns are worth highlighting because they're so common and so different from Morton's neuroma. First, peripheral neuropathy often doesn't change much when you take your shoes off. The symptoms aren't mechanically driven. Second, peripheral neuropathy classically gets worse at night and in bed — when the brain has fewer competing inputs and the burning or tingling moves to the foreground. If your foot symptoms are most intense at 2 AM in a quiet, dark bedroom and your shoes have nothing to do with it, you're looking at a neuropathy pattern.
The Signs That Point One Way or the Other
Here are the highest-yield distinguishing features, organized so you can mentally check off which side your symptoms fall on.
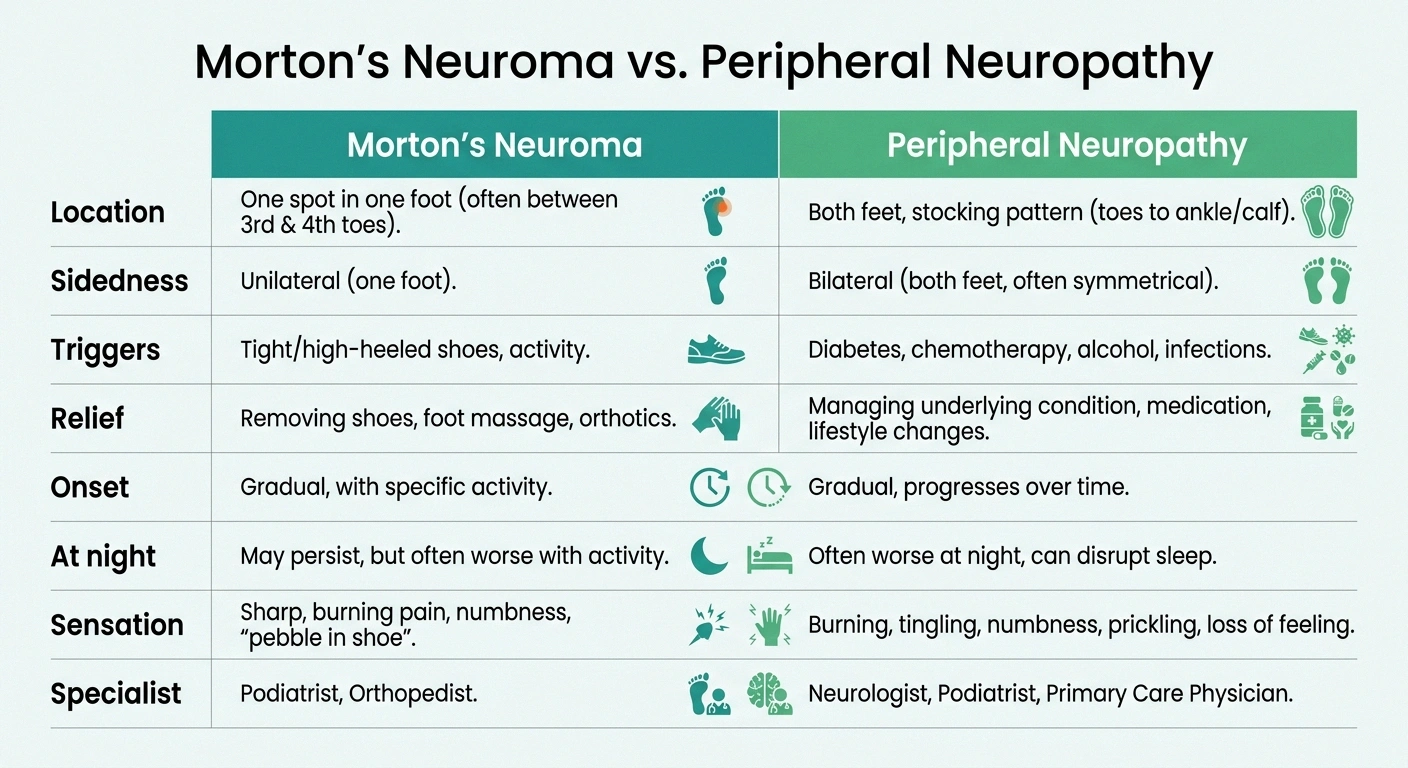
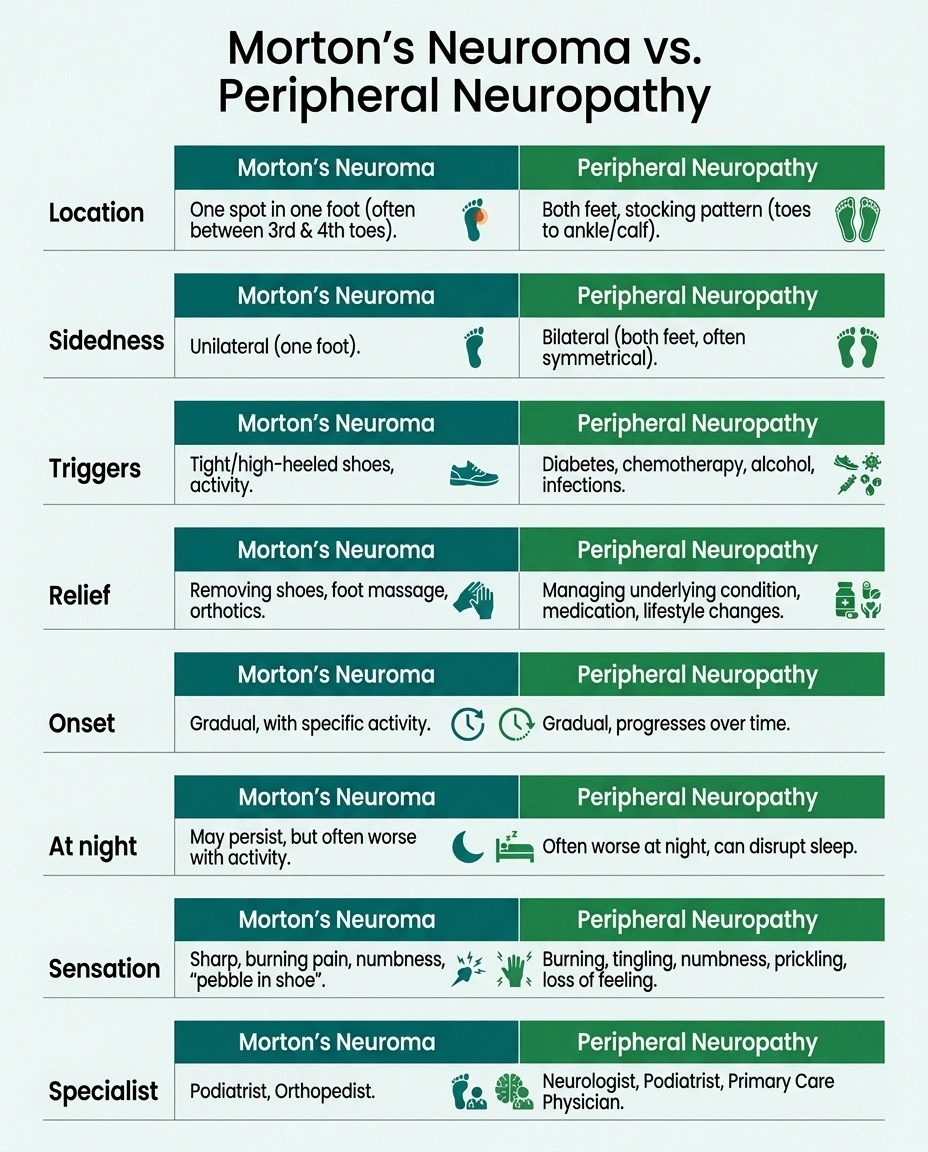
| Feature | Morton's Neuroma | Peripheral Neuropathy |
|---|---|---|
| Location | One focal spot, ball of foot | Diffuse, stocking pattern |
| Sidedness | Usually one foot | Both feet, symmetric |
| Triggers | Tight shoes, standing, running | Often unprovoked, present at rest |
| Relief | Remove shoes, rub spot | Often unchanged by sitting/lying |
| At night | Usually quiet | Classically worse |
| Sensation | Normal everywhere except the webspace | Broadly reduced in stocking pattern |
| First specialist | Podiatrist / Foot & Ankle | Primary care → Neurologist |
Where is the pain? Morton's neuroma is focal — usually one spot in the ball of one foot, often pointable with one finger. Peripheral neuropathy is diffuse — spread across both feet in a sock-like pattern.
One foot or both? Morton's neuroma is almost always one-sided. Peripheral neuropathy is almost always bilateral and symmetric.
What triggers it? Morton's neuroma is shoe- and weight-bearing-triggered. Tight shoes, running, prolonged standing, and high heels reliably flare it. Peripheral neuropathy often isn't movement-triggered at all — it can persist whether you're walking or lying still.
What relieves it? Morton's neuroma is dramatically relieved by kicking off shoes and rubbing the affected webspace. Peripheral neuropathy is often unchanged by sitting, lying down, or rubbing — and sometimes it's worse when you're horizontal in bed.
How did it start? Morton's neuroma often appears with a clear trigger — new shoes, more running, a new job that required standing for hours, a long day at a wedding in heels. Peripheral neuropathy creeps in over months or years, with no single starting point you can name.
How does it behave at night? Morton's neuroma usually quiets down at night when shoes are off and you're not bearing weight. Peripheral neuropathy classically gets worse at night, sometimes severely. Our piece on why neuropathy gets worse at night explains why this happens.
Sensation across the rest of the foot. A foot with Morton's neuroma usually has normal sensation everywhere except the affected webspace. A foot with peripheral neuropathy has reduced sensation across the whole sock-pattern distribution — testing vibration with a tuning fork, light touch with a monofilament, or sharp/dull discrimination shows broad changes.
Your medical history matters. Diabetes, longstanding alcohol use, chemotherapy history, known B12 deficiency, thyroid disease, autoimmune conditions, or family history of neuropathy all raise the probability that what you're dealing with is peripheral neuropathy. A history of narrow shoes, high heels, running, or repetitive forefoot loading raises the probability of Morton's neuroma.
Here's the honest disclaimer that has to come with this list: real people don't always fit clean categories. Symptoms overlap. Both conditions can produce burning, tingling, and numbness. And — critically — both conditions can be present in the same foot at the same time. The questions above are starting points for a conversation with a clinician, not a verdict you reach on your own.
What Happens at the Doctor's Office
Knowing what the workup looks like helps you go in less anxious and ask better questions.

For suspected Morton's neuroma, expect a podiatrist or orthopedic foot-and-ankle surgeon to do a hands-on exam. The signature test is called Mulder's click. The clinician squeezes your forefoot from the sides while pressing up into the painful webspace. If the test reproduces your pain — and especially if there's a palpable click as a thickened nerve gets pushed past the metatarsal heads — it's strongly suggestive of Morton's neuroma. They'll also press on individual webspaces to localize where the pain lives, examine your gait and footwear, and check for any deformities or callus patterns.
If imaging is ordered, ultrasound is the usual first choice — it's cheap, fast, and shows the characteristic dumbbell-shaped lesion well. MRI is sometimes used for surgical planning. There's an important honesty point here that no one tells patients: studies have shown that up to about 60 percent of people with no foot pain at all have a neuroma-shaped finding on imaging. The lesion can be present without being the source of pain. That's why imaging supports the clinical picture; it doesn't make the diagnosis on its own.
Nerve conduction studies (EMG/NCS) are usually normal in Morton's neuroma because the affected nerve is small, distal, and focal — too small to show up reliably on standard nerve testing.
For suspected peripheral neuropathy, the workup is entirely different. A neurologist (often after a primary-care referral) will start with a careful history — onset, progression, distribution, any risk factors — and a focused physical exam. They'll check vibration sense with a tuning fork on the bony parts of the toes, light touch with a 10-gram monofilament, pinprick sensation, joint-position sense, deep tendon reflexes (especially the Achilles, which is often diminished or absent in length-dependent neuropathy), and muscle strength.
Lab work hunts for treatable causes. The standard panel typically includes fasting glucose and hemoglobin A1c (diabetes), vitamin B12, thyroid function, complete blood count, comprehensive metabolic panel, and sometimes additional testing like serum protein electrophoresis, methylmalonic acid, copper, or autoimmune markers depending on the clinical picture. Our overview of neuropathy lab tests walks through what to expect.
Nerve conduction studies and EMG are the standard objective test for large-fiber neuropathy. If small-fiber neuropathy is suspected (burning predominant, normal nerve conduction studies, intact reflexes), additional testing like a skin punch biopsy for nerve fiber density or autonomic testing may be ordered.
The point of mapping these out side by side is that they answer different questions. The Morton's workup asks where is the focal problem? The neuropathy workup asks what systemic cause is driving the diffuse nerve damage, and how extensive is it?
What If It's Both?
This is the section that matters most to a lot of NeuropathyResource readers. Morton's neuroma and peripheral neuropathy are not mutually exclusive. A person with diabetic neuropathy can absolutely develop a Morton's neuroma — and the combination is uniquely confusing.
Several things make the overlap particularly tricky. Reduced sensation from neuropathy can let someone walk much longer in a poorly fitting shoe before the foot signals distress — increasing the mechanical insult that produces the neuroma in the first place. The background tingling or burning of neuropathy can mask the sharper, focal pain of a new neuroma, delaying recognition. And healing after corticosteroid injection or surgery can be slower and more complication-prone in people with diabetes, which affects how treatment options should be sequenced.
The clinical signal that a neuropathy patient may also have developed a neuroma is usually a new, focal, asymmetric change on top of the baseline. Something like: “My usual neuropathy has been steady for years, but over the last three or four months one specific spot in the ball of my left foot has gotten sharp, especially in my work shoes.” Or: “I have neuropathy in both feet, but for the first time the left foot has a spot that hurts in a different way.” When asymmetry shows up in a normally-symmetric condition, that's a flag to investigate.
If this describes you, the move isn't to self-diagnose. The move is to bring this exact framing to your podiatrist or neurologist: “I have neuropathy. Something new and different is happening in one spot in one foot. Can we evaluate for a Morton's neuroma?” That sentence routes the conversation correctly.
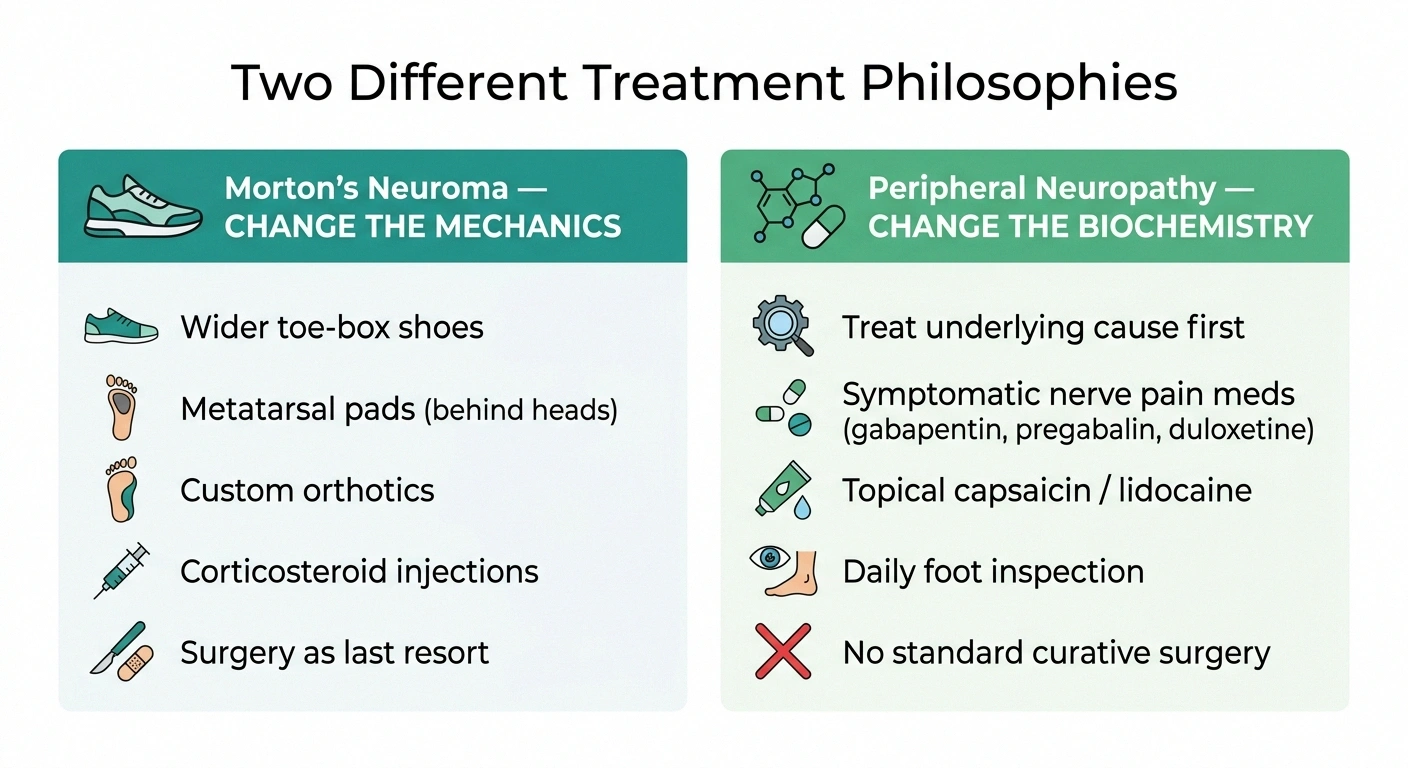
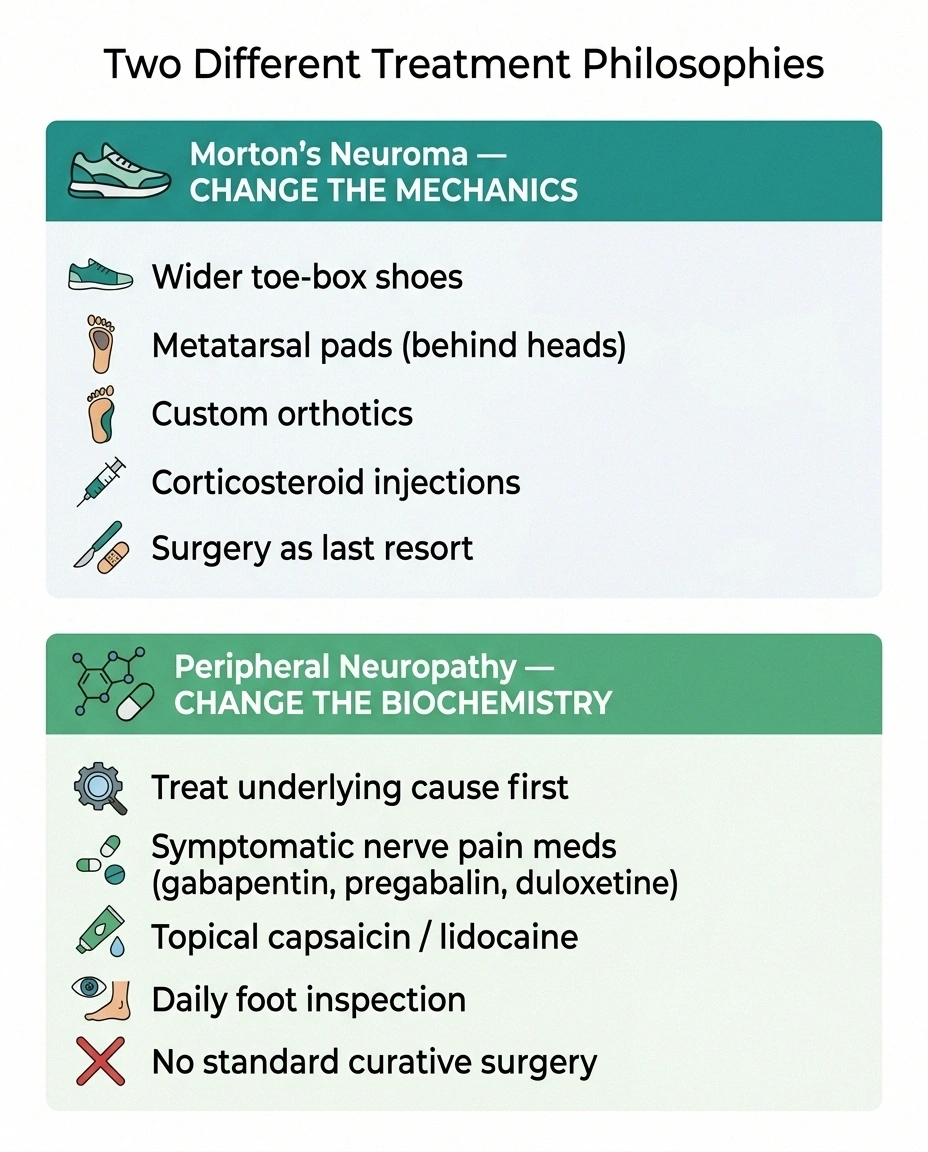
Treatments — Two Different Approaches
The treatment philosophies for these two conditions are fundamentally different, which is one more reason why getting the diagnosis right matters.
For Morton's Neuroma: Change the Mechanics
Morton's neuroma treatment is fundamentally about reducing the mechanical compression on the affected nerve. Most podiatrists recommend at least six months of conservative care before considering surgery. The progression goes something like this:
Footwear change first. Wide toe-box, low heel, soft-soled shoes. This is non-negotiable, free, and often produces the biggest single improvement. If you've spent decades in narrow shoes or heels, your feet have an opinion about that, and the opinion is louder when there's a neuroma involved. Our best shoes for neuropathy guide overlaps somewhat — though the specific neuroma priority on a wide toe box is sharper.
Metatarsal pad placement. A metatarsal pad sits behind the metatarsal heads (not directly under them) to lift and spread the metatarsals, opening up the space the nerve runs through. The placement detail matters and is frequently gotten wrong with over-the-counter pads stuck on without guidance. Your podiatrist can show you exactly where it goes.
Custom orthotics when over-the-counter approaches aren't enough.
Activity modification — reducing or modifying the high-impact or tight-shoe activities that flare it.
NSAIDs or ice for symptom management while the mechanical fixes do their work.
Corticosteroid injection if conservative care isn't enough. A meta-analysis of nearly 3,000 patients found that about 43 percent achieved complete pain relief with injection therapy. Effects can last weeks to months. Repeated injections carry risks — fat pad atrophy and skin discoloration — so most podiatrists are conservative about repeat doses.
Alcohol or sclerosing injections, typically given as a series of four to seven weekly injections, with reported response rates in the 60 to 80 percent range in published studies.
Radiofrequency ablation or cryoneurolysis as newer options between injection and surgery.
Surgery as last resort. The two main options are nerve decompression (releasing the deep transverse metatarsal ligament without removing the nerve) and neurectomy (surgically removing the affected nerve segment). Published outcomes suggest about 74 percent of neurectomy patients are pain-free and about 68 percent of decompression patients are pain-free. The honest trade-offs: permanent numbness in the affected webspace after neurectomy, risk of stump neuroma (a recurrent painful nerve regrowth at the cut end), and a meaningful recurrence rate. Surgery helps most people but doesn't guarantee a pain-free outcome forever.
For Peripheral Neuropathy: Change the Biochemistry
Peripheral neuropathy treatment is fundamentally different. You can't fix neuropathy with shoes.
Treat the underlying cause. This is the single highest-leverage move. Tight glycemic control for diabetes. B12 repletion for B12 deficiency. Alcohol cessation for alcoholic neuropathy. Thyroid treatment for hypothyroidism-related neuropathy. Discontinuing offending medications when possible. Treating an underlying autoimmune condition. For diabetic patients specifically, our diabetic neuropathy treatment guide covers this in detail.
Symptomatic medications for nerve pain. Gabapentin, pregabalin, duloxetine, and tricyclic antidepressants like amitriptyline or nortriptyline are the first-line options. None of these are perfect. All have side effects. Many patients try several before finding one that helps without intolerable side effects.
Topicals like capsaicin cream and lidocaine patches for localized burning or shooting pain.
Foot protection and daily inspection — critical when sensation is reduced. Look at the bottoms of your feet every day. Never go barefoot at home. Wear protective shoes even indoors. Our piece on going barefoot at home with neuropathy walks through why this matters.
Supportive measures — physical therapy, balance training, supplements (B-complex, alpha-lipoic acid) with appropriate caveats about what the evidence does and doesn't show.
There's no standard curative surgery for typical peripheral neuropathy. Nerve decompression in diabetic neuropathy remains a contested niche option, not first-line care.
The single biggest mental pivot: for neuroma, you change the mechanics of the foot. For neuropathy, you change the biochemistry of the body. Wrong target = wrong treatment.
Which Doctor Should You See?
This is the part most articles bury or skip. Here's the routing.
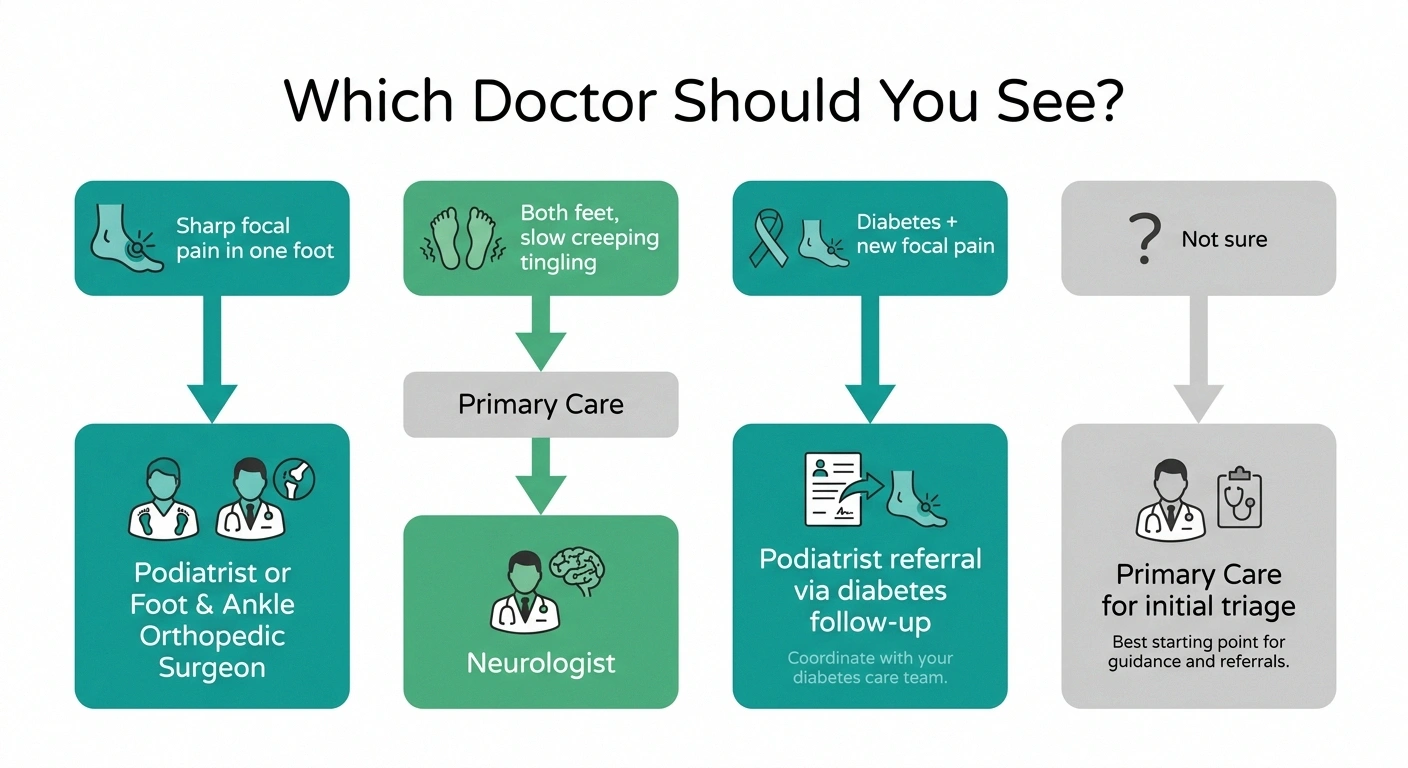
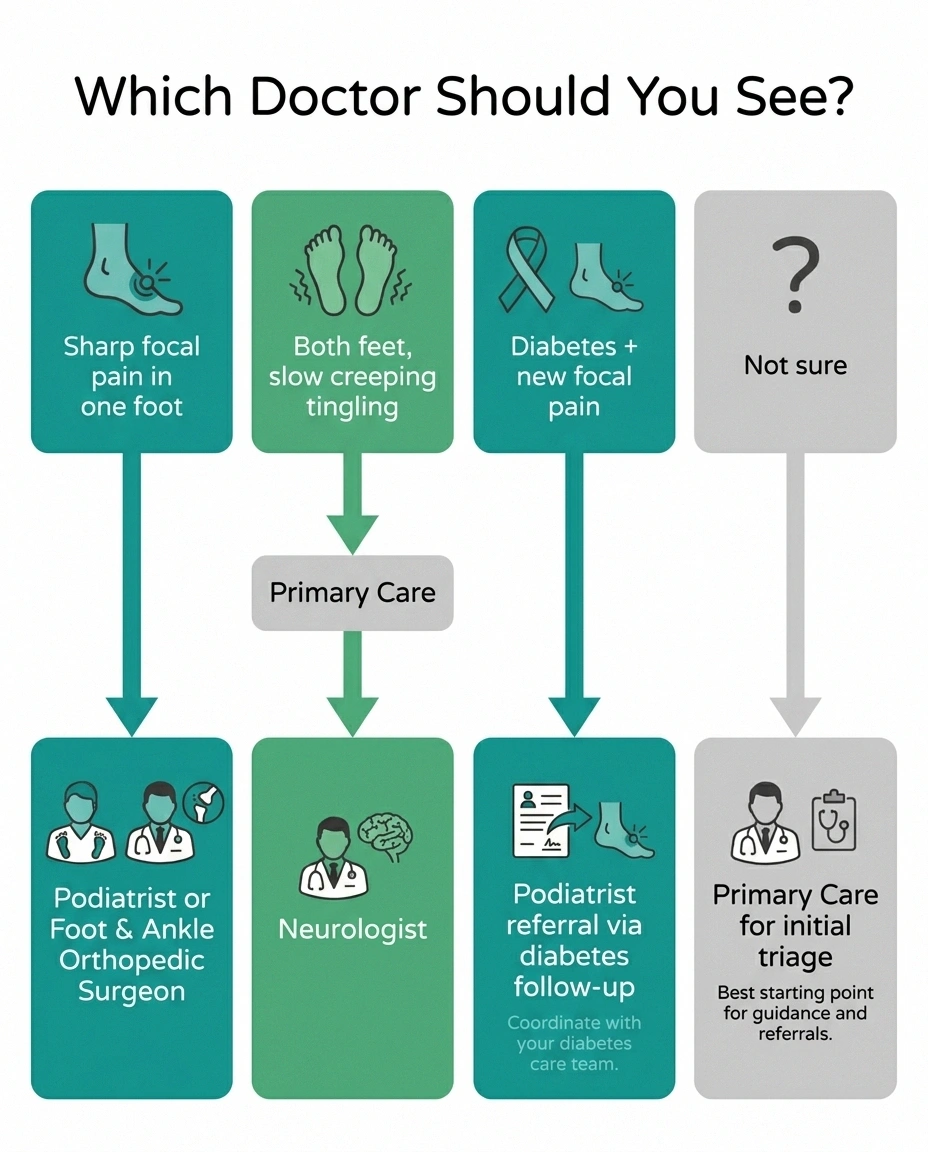
Sharp focal ball-of-foot pain in one foot, worse in shoes: start with a podiatrist or orthopedic foot-and-ankle surgeon. These specialists handle Morton's neuroma every day.
Both feet, gradual creeping tingling, numbness, or burning, often worse at night: start with your primary care doctor for the initial evaluation and labs, then a neurologist for the more specialized workup.
You have diabetes and a new focal pain has appeared on top of your usual symptoms: bring it up at your next diabetes follow-up and specifically ask for a referral to podiatry to evaluate for a possible neuroma. Don't let it get attributed to “your usual neuropathy” without evaluation.
You're not sure which it is: primary care is the right starting place. They can do an initial exam, order baseline labs, and refer you to the right specialist.
Pain is severe, waking you up, or you're rapidly losing function: don't wait. Get seen sooner — urgent care if needed.
Red flags that warrant prompt medical attention regardless of which condition you suspect: sudden onset of foot or leg weakness, loss of bowel or bladder control with foot symptoms (possible spine issue), a wound or ulcer or color change on the foot, fever with foot pain, rapidly ascending numbness moving up the leg, or foot symptoms following recent trauma. Any of those = urgent evaluation, not “wait and see.”
What to Bring to Your Appointment
A focused, prepared patient gets better care. Before your appointment, jot down answers to these:
Where exactly does it hurt? Point with one finger if you can. One spot, multiple spots, all over.
One foot or both? Same on both sides, or worse on one?
What does it feel like? Sharp, burning, electric, tingling, numb, “walking on a marble,” “walking on cotton” — your specific words matter.
When did it start? Months ago, years ago, after a specific event?
What triggers it? Tight shoes, walking, standing, running, nothing in particular?
What relieves it? Removing shoes, rubbing, elevation, rest, nothing?
How does it behave at night? Quiets down, doesn't change, gets dramatically worse?
What shoes do you mostly wear? Bring a pair if it's an outdoor problem (the wear pattern tells the doctor a lot).
Your full medication list, including over-the-counter supplements. Some medications are known to cause or worsen neuropathy.
Your medical history, especially diabetes, B12 issues, thyroid disease, chemotherapy history, autoimmune conditions, or any family history of nerve problems.
Five minutes of preparation upgrades the entire appointment.
The Bottom Line
Morton's neuroma and peripheral neuropathy can both produce burning, tingling, and numbness in the foot. They feel similar from inside. But the patterns differ in ways that matter: one spot in one foot versus both feet in a sock-shaped pattern; shoe-triggered and weight-bearing-driven versus often present at rest and worse at night; mechanical compression at a single nerve versus systemic damage across many nerves.
Getting the right diagnosis matters because the treatments don't overlap. Neuroma needs better shoes, metatarsal pads, sometimes injections, occasionally surgery. Neuropathy needs the underlying cause addressed — diabetes control, B12 repletion, whatever is driving it — plus symptomatic treatment for pain. Mixing them up means months of effort aimed at the wrong target.
If your symptoms sound more neuroma-like, a podiatrist is your starting point. If they sound more neuropathy-like, primary care into neurology is the path. If you have known neuropathy and something new and focal has appeared, ask about both. And if you're unsure, primary care can do the initial triage and send you the right direction.
The most useful thing this article can do is replace months of guessing with one clearer conversation with the right doctor. That's worth showing up for.
Frequently Asked Questions
What does Morton's neuroma feel like?
Most people describe a sharp, burning, or electric pain in the ball of the foot, usually between the third and fourth toes, often with the feeling of walking on a marble or a bunched-up sock. Numbness or tingling in the affected toes is common but not universal. The pain dramatically worsens with tight shoes, running, or prolonged standing, and dramatically improves when shoes come off and the foot is rubbed.
How is Morton's neuroma different from peripheral neuropathy?
Morton's neuroma is one spot in one foot, usually shoe- and weight-bearing-triggered, with sensation normal everywhere else on the foot. Peripheral neuropathy is typically both feet, with a stocking-pattern distribution, often present at rest, frequently worse at night, and accompanied by reduced sensation across the whole sock-pattern area. Neuroma is a focal mechanical problem; peripheral neuropathy is a systemic nerve problem.
Can you have Morton's neuroma and diabetic neuropathy at the same time?
Yes. They are not mutually exclusive, and diabetes both raises the risk of Morton's neuroma (because reduced sensation lets someone tolerate poorly fitting shoes longer) and complicates its evaluation (because background neuropathy symptoms can mask focal neuroma pain). The signal that a neuropathy patient may also have a neuroma is a new, focal, asymmetric pain on top of the usual baseline symptoms.
What is Mulder's sign?
Mulder's sign (or Mulder's click) is a physical exam test for Morton's neuroma. The clinician squeezes the forefoot from the sides while pressing up into the painful webspace. A palpable click as a thickened nerve is pushed past the metatarsal heads, combined with reproduction of the patient's typical pain, strongly suggests Morton's neuroma. It's a bedside test — not something to do on yourself.
Will an MRI definitively diagnose Morton's neuroma?
Not on its own. Ultrasound or MRI can show the characteristic dumbbell-shaped lesion in the affected interspace. But studies have shown that up to about 60 percent of people with no foot pain at all have a similar finding on imaging. The lesion can exist without causing symptoms. Imaging supports the diagnosis; the clinical picture — pattern of pain, location, exam findings — is what makes it.
Does Morton's neuroma go away on its own?
Generally no. Symptoms can flare and settle over time, and conservative treatment can dramatically reduce or eliminate pain. But the underlying thickening of the nerve doesn't reverse without intervention or sustained pressure relief. Most people who get persistent relief have done at least some combination of footwear change, metatarsal padding, and sometimes injection or other treatment.
What kind of doctor treats Morton's neuroma?
A podiatrist or an orthopedic foot-and-ankle surgeon. These specialists handle Morton's neuroma routinely. If you start with your primary care doctor, expect a referral to one of those specialists for evaluation and treatment.
What kind of doctor treats peripheral neuropathy?
A neurologist is the specialist for peripheral neuropathy, usually after an initial evaluation by primary care. Depending on the underlying cause, other specialists may be involved — endocrinology for diabetes, hematology for blood-related causes, rheumatology for autoimmune-driven neuropathy. Primary care is the right starting point if you're not sure what's driving your symptoms.


