One of the most heartbreaking conversations I have, again and again, in my support group goes something like this: “Janet, I was perfectly fine. I took an antibiotic for a sinus infection or a UTI, and within a few days my feet were burning and tingling — and nobody warned me, and now my own doctor seems unsure whether to believe me.” If that is your story, or close to it, I want you to read the next sentence slowly: you are not imagining it, and you are not alone.
The class of antibiotics called fluoroquinolones — drugs like Cipro and Levaquin — carries a recognized risk of peripheral nerve damage, and the U.S. Food and Drug Administration has formally warned about it for years. This article walks through what that warning actually says, how the nerve injury behaves, and most importantly what to do if you suspect it happened to you. I'll be honest about what's known and what isn't, because you deserve that more than you deserve reassurance.
First, You're Not Imagining It — and It's Not Your Fault
I lead with this because the disbelief hurts almost as much as the symptoms. When nerve trouble starts right after a short course of antibiotics, it's common for it to be dismissed — by others and even by yourself — as coincidence or anxiety. But the connection between fluoroquinolone antibiotics and peripheral neuropathy is not a fringe theory or an internet rumor. It is documented in the medical literature and acknowledged by the FDA in official drug safety communications. You did nothing wrong by taking a medication your doctor prescribed for a real infection. Naming the cause accurately isn't about blame; it's about getting you taken seriously and pointed toward the right next steps.
You are not imagining it, and it is not your fault
The link between fluoroquinolone antibiotics and peripheral neuropathy is documented in the medical literature and acknowledged by the FDA — not a fringe theory. You did nothing wrong by taking a medication your doctor prescribed.
What Fluoroquinolones Are (and Why They're Still Prescribed)
Fluoroquinolones are a powerful, broad-spectrum class of antibiotics. The ones taken by mouth or by injection that carry this risk include ciprofloxacin (Cipro), levofloxacin (Levaquin), moxifloxacin (Avelox), ofloxacin (Floxin), gemifloxacin (Factive), and a few others. They have been prescribed very widely — often for sinus infections, bronchitis, and urinary tract infections.
It's important to be fair here: these drugs are not “bad.” For certain serious infections — and in some cases life-threatening ones — they are genuinely valuable and sometimes irreplaceable. The concern that regulators raised is not “never use them.” It's that for many minor, uncomplicated infections, the risk-benefit math doesn't favor a fluoroquinolone when safer alternatives exist. That distinction — reserve, don't demonize — is the honest frame, and it matters when you talk with your own prescriber.
What the FDA Actually Warned — and When
Here are the facts, anchored so you can stand on them. In August 2013, the FDA strengthened its labeling warning that fluoroquinolone antibiotics taken by mouth or by injection may cause peripheral neuropathy that can be rapid in onset and, in some patients, may be permanent. The agency required the warning to be made more prominent. In later safety communications, the FDA went further, advising that fluoroquinolones be reserved for patients who have no alternative treatment options for several common, uncomplicated infections, because the risk of serious side effects generally outweighs the benefit in those situations.
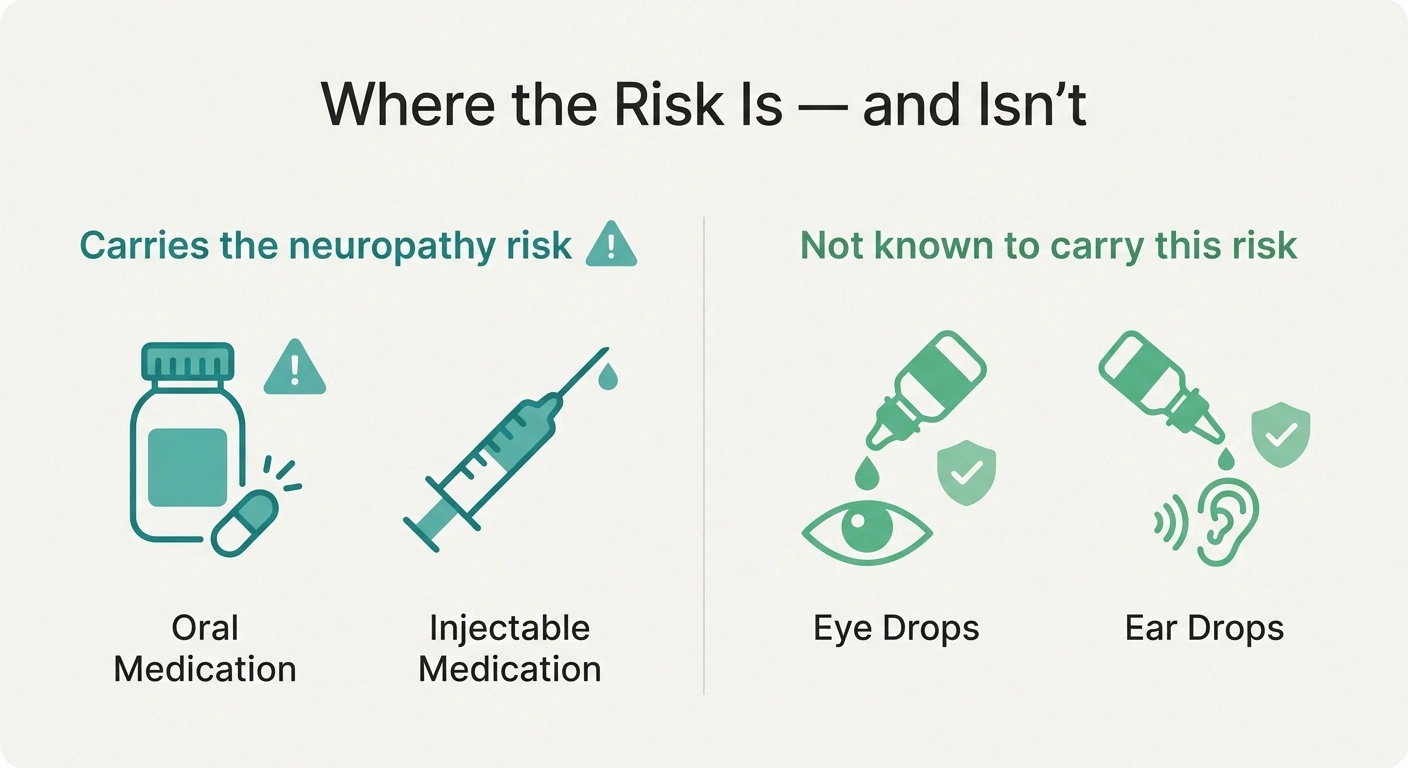
In August 2013 the FDA strengthened its warning that oral and injectable fluoroquinolones may cause peripheral neuropathy that can be rapid in onset and, in some patients, permanent. Later communications advised reserving these drugs for patients with no other option for several common, uncomplicated infections. Topical eye/ear drops are not known to carry this risk.
One detail brings real relief to a lot of people: this neuropathy risk is associated with the oral and injectable forms. Topical fluoroquinolones — the kind used as eye drops or ear drops — are not known to carry this peripheral neuropathy risk. So if your only exposure was an ear or eye drop, this particular concern is very unlikely to apply to you.
How Fast It Can Happen and What It Feels Like

This is the part that catches people off guard. With many side effects, there's a slow build. With fluoroquinolone-associated neuropathy, the onset can be fast — sometimes within a few days of starting the drug, and in some reports after a single course. It doesn't always wait politely.
A Fast Onset Is a Reason to Call, Not to Wait
Burning, tingling, numbness, or weakness that begins within days of starting one of these antibiotics is the pattern that should prompt a prompt call to the prescriber — not a wait-and-see. Do not stop a prescribed antibiotic on your own; raise it quickly so the decision is made with you.
The symptoms are the familiar vocabulary of nerve injury: pain, burning, tingling, numbness, weakness, and altered sensation — changes in how light touch, pain, or temperature feel, and sometimes a loss of the sense of where your body is in space. If those words match your experience, our plain-language guide to what neuropathy actually feels like may help you put language to it, and because the small nerve fibers are often involved, our overview of small fiber neuropathy is worth reading too. What makes the timing so important is practical: a fast onset right after starting an antibiotic is exactly the pattern that should prompt a prompt call to your prescriber, not a wait-and-see.
Why This One Is Different: It Can Be Long-Lasting
I won't soften this, because false comfort doesn't help anyone plan. Many medication side effects fade once the drug is stopped. Fluoroquinolone-associated peripheral neuropathy is concerning specifically because, in some patients, it has been reported to be long-lasting or even permanent. That is the feature that sets it apart from a routine, reversible reaction and the reason the FDA treated it so seriously.
That said, “can be permanent in some patients” is not the same as “is permanent in everyone.” Outcomes vary widely, some people do improve over time, and how much recovery is possible often depends on how early the drug is stopped and how the nerves respond. The realistic, honest stance is somewhere between panic and dismissal: this is a serious possibility worth acting on quickly, not a guaranteed life sentence. Our broader discussion of whether neuropathy can be reversed applies the same balanced lens.
What Researchers Think Is Going On

You may want to understand the “why,” so here it is — with appropriate humility. The exact mechanism is not fully settled, but the leading hypotheses involve oxidative stress and mitochondrial toxicity (interference with the energy machinery inside nerve cells) and effects on magnesium and connective tissue. This is also why fluoroquinolones are linked to a broader pattern of effects beyond nerves — tendon problems and others — that some patients describe collectively.
Fluoroquinolone-associated neuropathy can begin within a few days of starting the drug — sometimes after a single course — which is what makes the timeline you bring to your appointment so valuable.
I'm deliberately presenting this as a working scientific explanation rather than established fact, because being accurate about the limits of knowledge is part of being trustworthy. What you do not need is a complete mechanistic theory in order to act. The practical steps below don't depend on which hypothesis turns out to be correct.
What to Do If You Think an Antibiotic Triggered Your Neuropathy

Here is the part to act on. First, do not simply stop a prescribed antibiotic on your own without guidance — instead, contact the prescriber promptly and describe exactly what you're feeling and when it started relative to the medication. The FDA's guidance is that if peripheral neuropathy symptoms develop, the fluoroquinolone should generally be stopped and switched to a different, non-fluoroquinolone antibiotic, unless the benefit of continuing clearly outweighs the risk in a serious infection. That decision is your clinician's to make with you — but you raising it promptly is what starts it.
If You Suspect It — Four Steps
Contact the prescriber promptly — don't stop a prescribed antibiotic unguided.
Document the drug, dose, and exact dates vs. your first symptoms.
Ask for a proper evaluation — not “let's just watch it.”
Consider reporting the reaction to the FDA MedWatch program.
Second, document everything: the drug name, dose, the exact dates you took it, and the date and nature of your first symptoms. This timeline is the single most useful thing you can bring to an appointment. Third, ask for a proper evaluation rather than accepting “let's just watch it” — our guide to neuropathy diagnosis and the tests that may be ordered shows what a real workup looks like, and our piece on talking to your doctor about neuropathy can help you be heard if you're being brushed off. You can also report the reaction to the FDA's MedWatch program; it both creates a record and contributes to the safety data that protects others.
Is There a Treatment? An Honest Answer
I wish I had a clean answer, and I respect you too much to invent one. There is no proven, targeted “antidote” that specifically reverses fluoroquinolone-associated nerve damage. Stopping the drug is the key protective step. Beyond that, management follows the same supportive path as other neuropathies: addressing symptoms, correcting any nutritional deficiencies, physical therapy to protect function and balance, time, and patience.
You will encounter online communities recommending high-dose magnesium, antioxidants, and various supplements. I want to be straight with you: these are largely unproven for this specific purpose, even though the reasoning sometimes connects to the proposed mechanism. That doesn't automatically make them worthless, but it does mean they should be discussed honestly with your clinician as experiments, not relied on as cures — and never instead of a proper medical evaluation. Our evidence-lens look at natural remedies for neuropathy pain applies that same honest standard.
How to Be a Smart Patient Going Forward

Whether or not a fluoroquinolone is behind your symptoms, this knowledge makes you a more powerful patient. For a future infection, it is entirely reasonable and appropriate to ask your prescriber: “Is a fluoroquinolone necessary here, or is there an equally good alternative for this particular infection?” For a minor, uncomplicated infection with safe alternatives, that's exactly the question regulators have effectively encouraged patients and clinicians to ask. You are not being difficult; you are participating in your own care.
Reserve, don't demonize — and document everything
Fluoroquinolones still matter for serious infections. For minor ones, it's reasonable to ask “is this necessary, or is there a safer alternative?” Keep a written reaction list in your chart so no prescriber re-exposes you. Information, calmly applied, is how you take back control.
Keep a written list of medications you've reacted to and make sure it's in your chart and known to every prescriber and pharmacist you see. If you've had fluoroquinolone-associated neuropathy, that history is critical information for avoiding re-exposure. Fluoroquinolones belong to a broader group of drugs that can affect the nerves — our overview of medications that can cause neuropathy is worth knowing, and understanding the general stages of neuropathy helps you track your own course over time. Information, calmly applied, is how you take back some control.
Frequently Asked Questions
Which antibiotics are linked to peripheral neuropathy?
The fluoroquinolone class is the group the FDA specifically warned about for peripheral neuropathy. Oral and injectable fluoroquinolones include ciprofloxacin (Cipro), levofloxacin (Levaquin), moxifloxacin (Avelox), ofloxacin (Floxin), and gemifloxacin (Factive), among others. The risk is associated with the oral and injectable forms. Topical fluoroquinolones used as eye or ear drops are not known to carry this peripheral neuropathy risk.
How quickly can fluoroquinolone neuropathy start?
It can start rapidly. Unlike side effects that build slowly, fluoroquinolone-associated peripheral neuropathy has been reported to begin within a few days of starting the medication, and in some cases after a single course. A fast onset of burning, tingling, numbness, or weakness shortly after starting one of these antibiotics is the pattern that should prompt a prompt call to the prescriber rather than waiting to see if it passes.
Is fluoroquinolone-induced neuropathy permanent?
It can be long-lasting or permanent in some patients, which is exactly why the FDA strengthened its warning, but it is not permanent in everyone. Outcomes vary, and some people improve over time. How much recovery is possible often depends on how early the drug is stopped and how the nerves respond. The accurate stance is between panic and dismissal: a serious possibility worth acting on quickly, not a guaranteed permanent outcome for every person.
What should I do if I think an antibiotic caused my nerve symptoms?
Contact the prescriber promptly rather than stopping a prescribed antibiotic on your own without guidance, and describe exactly what you feel and when it started relative to the drug. Current guidance is that the fluoroquinolone should generally be stopped and switched to a non-fluoroquinolone antibiotic if neuropathy symptoms develop, unless the benefit clearly outweighs the risk. Document the drug, dose, and dates, ask for a proper evaluation, and consider reporting the reaction to the FDA MedWatch program.
Is there a treatment that reverses it?
There is no proven targeted treatment that specifically reverses fluoroquinolone-associated nerve damage. Stopping the drug is the key protective step, and management otherwise follows the same supportive approach as other neuropathies: symptom management, correcting nutritional deficiencies, physical therapy, time, and patience. Supplements promoted in online communities are largely unproven for this specific purpose and should be discussed honestly with a clinician rather than relied on as a cure.
Should I refuse fluoroquinolones in the future?
That is a decision to make with your clinician, not a blanket rule. Fluoroquinolones remain genuinely valuable for certain serious infections. The reasonable approach is to ask whether a fluoroquinolone is necessary for your specific situation or whether an equally effective, safer alternative exists, especially for minor uncomplicated infections. If you have already had fluoroquinolone-associated neuropathy, that history is critical and should be clearly documented so prescribers can avoid re-exposing you.