
If you or someone you love has been on amiodarone for atrial fibrillation, ventricular tachycardia, or another stubborn heart rhythm problem, you already know the drug occupies a strange place in medicine. It works when nothing else does. It also has one of the longest side-effect lists of any common cardiac drug — the lungs, the thyroid, the liver, the eyes, the skin. And in a smaller but real number of patients, the nerves.
Amiodarone-induced neuropathy is one of those side effects that doesn't always make the conversation when the drug is started. The lung warning gets mentioned. The thyroid blood work gets ordered. The nerves often go unaddressed until a patient starts noticing burning feet, weak ankles, or hands that don't quite grip the way they used to. By then, the drug has often been on board for many months, and the question becomes a hard one — what do we do now?
I've written this piece for people who are either on amiodarone and worried about nerve symptoms, or who have already developed neuropathy on the drug and are trying to figure out the path forward. The good news is that amiodarone neuropathy, unlike some drug-induced neuropathies, is often partly reversible if it's caught and addressed. The harder news is that the conversation with your cardiologist has to be a careful one, because for many people, the alternative to amiodarone is worse than the neuropathy.
What Amiodarone Is and Why It's Prescribed
Amiodarone is an antiarrhythmic drug — it slows and steadies abnormal heart rhythms. It was first approved in the 1980s and has become one of the most widely used medications for atrial fibrillation and life-threatening ventricular arrhythmias.
Amiodarone is a fat-loving, iodine-containing antiarrhythmic that accumulates in tissues throughout the body — including peripheral nerves. About 2–5% of long-term users develop symptomatic neuropathy; closer to 10–15% develop subtle subclinical nerve changes. The neuropathy is often partly reversible if the drug is reduced or stopped early. The hard part is that for many patients, amiodarone is genuinely irreplaceable.
What makes amiodarone unusual is its chemistry. It's a fat-soluble iodine-containing molecule that accumulates in tissues throughout the body — fat, muscle, lung, liver, thyroid, skin, and yes, peripheral nerves. It has an extraordinarily long half-life, often measured in weeks to months. A single dose persists in the body for a long time, which is part of why it's so effective for rhythm control and also part of why its side effects can be slow to develop and slow to resolve.
For many people with serious arrhythmias, amiodarone is genuinely lifesaving. There aren't always good alternatives. That context matters when we talk about side effects — this isn't a drug to stop casually, and any decisions about it belong with a cardiologist who knows the full clinical picture.
How Often Does Amiodarone Cause Neuropathy?
The honest answer is that the published rates vary widely depending on how carefully you look. Older estimates put symptomatic peripheral neuropathy at around 2–5% of patients on long-term amiodarone. More careful prospective studies that look for subclinical nerve changes with formal nerve conduction studies have found rates closer to 10–15% with subtle signs that don't always cause obvious symptoms.
That gap matters. It means amiodarone neuropathy is more common than the typical drug label suggests, but the more severe presentations are rarer than the subtle ones. Many people on amiodarone have mild slowing of nerve conduction that they never notice. A smaller subset develops the classic symptoms — numbness, burning, tingling, weakness — that disrupt their daily life.
Risk goes up with three things. First, dose. The risk is concentrated in patients on higher daily doses (typically over 400 mg/day, especially during loading) or who have been on the drug for many years on lower maintenance doses. Second, total cumulative exposure. Because amiodarone accumulates, the longer you're on it, the more is sitting in tissues. Third, individual susceptibility — including age, baseline nerve health, and concurrent risk factors like diabetes, B12 deficiency, or alcohol use that put nerves on a thinner margin.
What the Neuropathy Looks Like
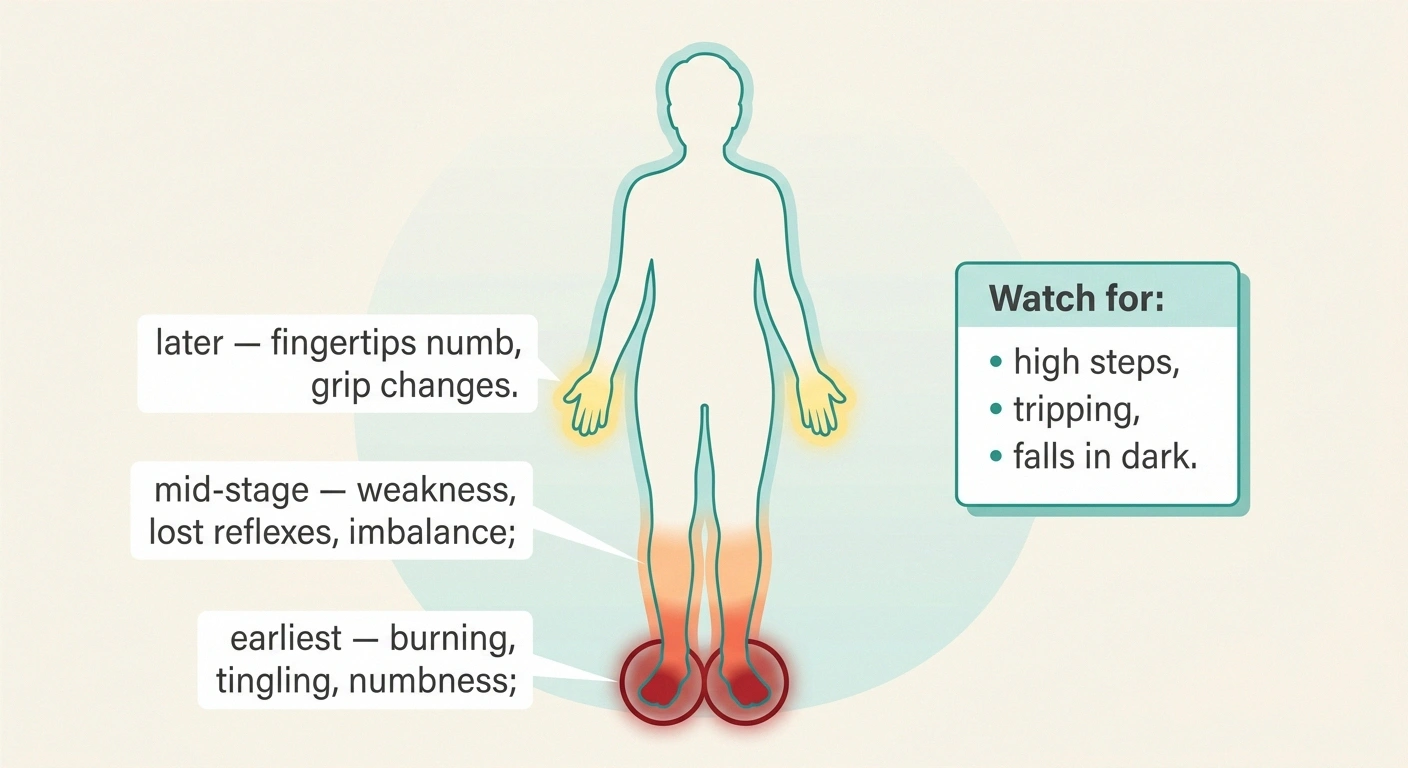
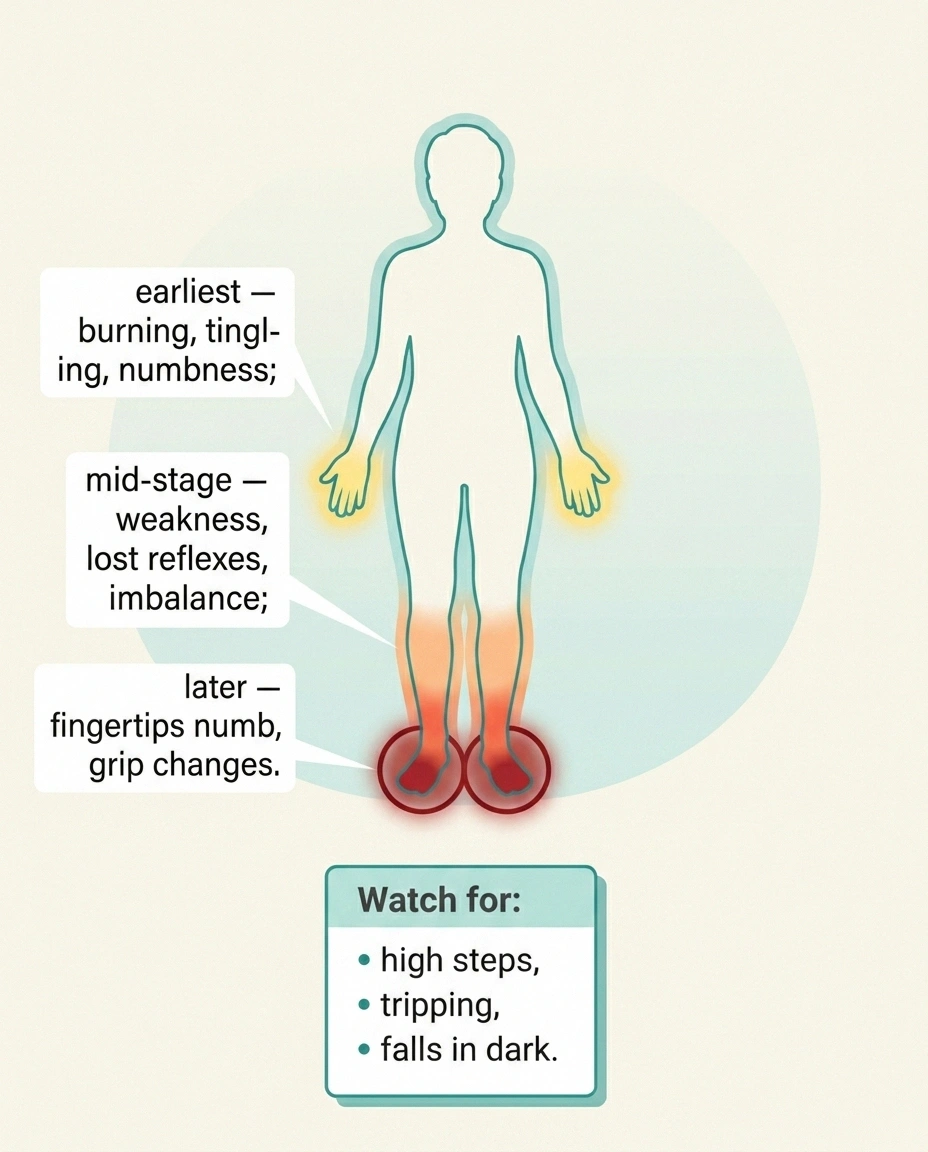
Amiodarone neuropathy usually shows up as a length-dependent sensorimotor polyneuropathy. That's the same general pattern as diabetic neuropathy or many other adult-onset neuropathies — it starts in the feet, moves up the legs, and only later involves the hands. It tends to be slow and gradual, not sudden.
The typical symptoms include:
- Burning, tingling, or “pins and needles” in the toes and balls of the feet, often worse in the evening and at night
- Numbness in a stocking-glove distribution — the parts of the body farthest from the spinal cord lose sensation first
- Loss of vibration sense in the toes, often detectable on exam before the patient notices it themselves
- Weakness in the small foot and lower leg muscles — high steps, occasional tripping, difficulty walking heel-to-toe
- Reduced or absent ankle reflexes
- Imbalance, especially in the dark or on uneven ground, as proprioception (the body's position sense) is lost
One feature that sometimes distinguishes amiodarone neuropathy from purely sensory neuropathies is that motor involvement (weakness) often shows up earlier in the course than you'd expect. Some patients also develop a coarse tremor in the hands, which can confuse the picture because tremor is one of amiodarone's known central nervous system side effects and isn't itself a sign of peripheral neuropathy.
In severe cases, the neuropathy can resemble chronic inflammatory demyelinating polyneuropathy closely enough that a neurologist may need nerve conduction studies and sometimes a nerve biopsy to be confident about the diagnosis.
How Amiodarone Damages Nerves
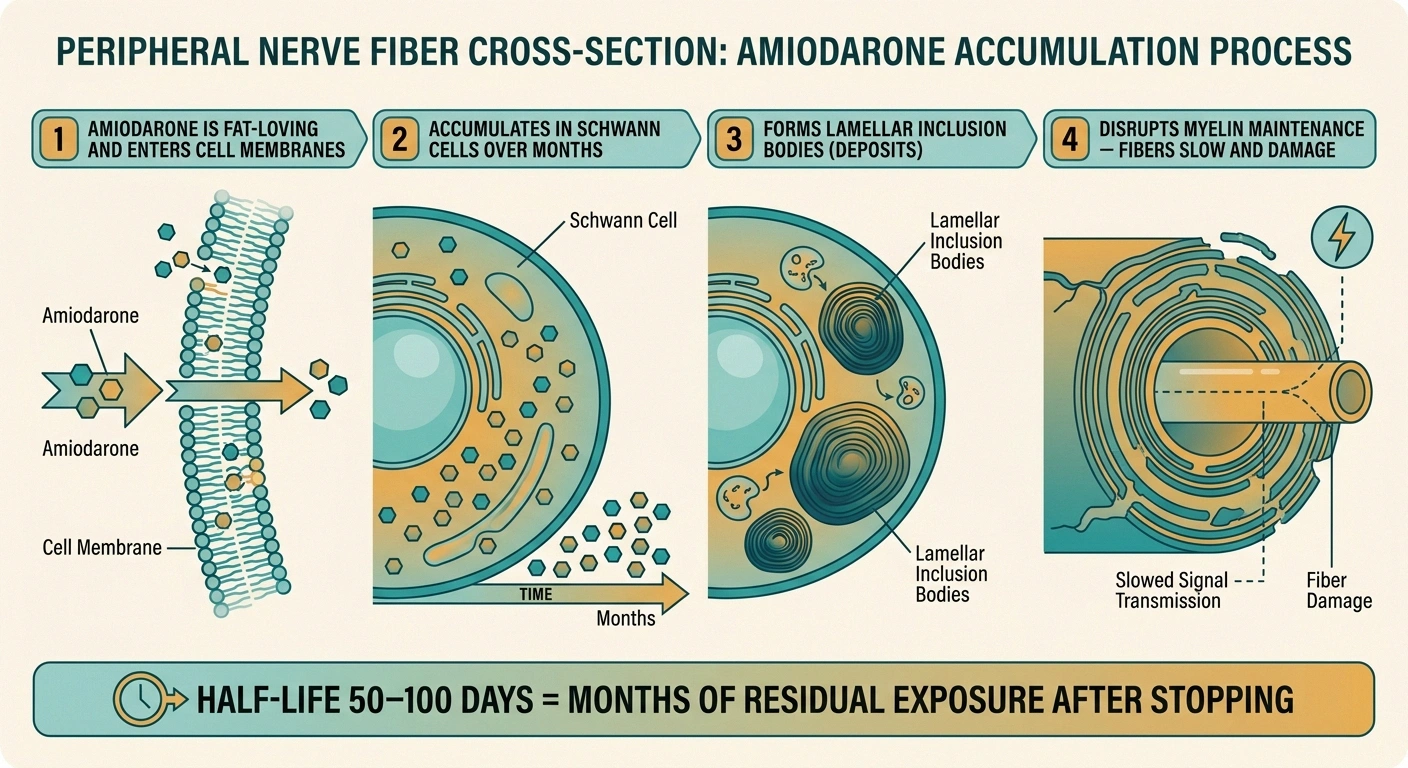
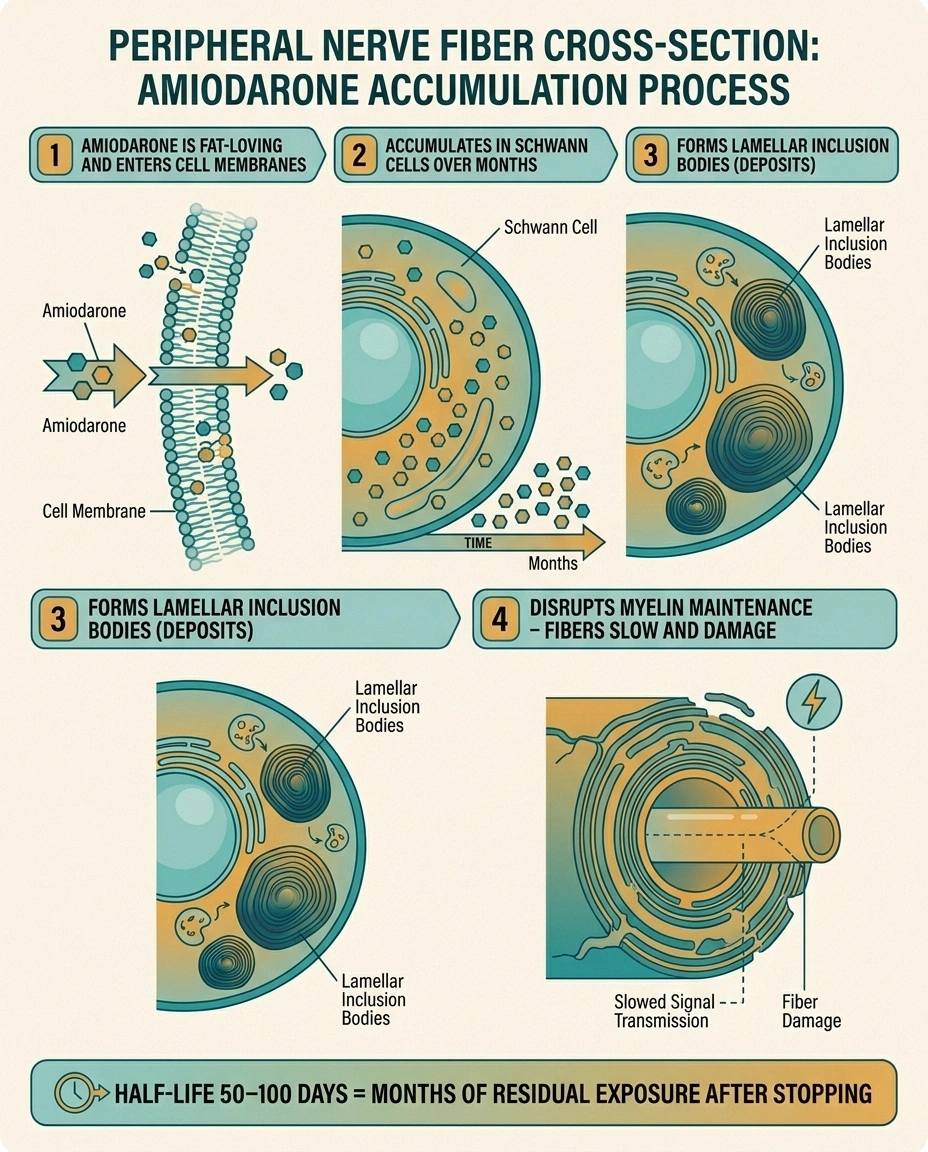
The mechanism isn't fully nailed down, but the prevailing theory has been consistent for decades. Amiodarone is a strongly lipophilic, or fat-loving, drug. It accumulates in cell membranes, and especially in the myelin-rich membranes of peripheral nerves. There it disrupts membrane lipid metabolism in ways that interfere with the normal turnover of myelin, the insulating sheath around large nerve fibers.
- Lamellar inclusion bodies inside Schwann cells — deposits of amiodarone and its metabolites built up over months to years
- Patchy demyelination — disrupted insulation around nerve fibers, slowing conduction
- Axonal degeneration in more advanced cases — actual nerve fiber damage that heals more slowly
- Mixed pattern distinguishes amiodarone neuropathy from the predominantly axonal pattern of diabetic neuropathy
The demyelinating component is the part that recovers; the axonal part is the part that often doesn't.
Nerve biopsies from amiodarone patients have shown characteristic findings — lamellar inclusion bodies inside Schwann cells (the cells that make myelin) and other peripheral cells. These are essentially deposits of amiodarone and its metabolites that have built up over months or years. The result is a mixed picture of demyelination (loss of insulation around the fibers) and axonal damage (damage to the actual nerve fibers themselves).
The dual demyelinating-plus-axonal mechanism is why amiodarone neuropathy can be partly but not always fully reversible. The myelin part can repair if the drug is removed and the nerves are given time. The axonal part heals more slowly and incompletely, which is why catching it earlier rather than later matters.
When to Suspect Amiodarone as the Cause
Not every neuropathy that develops in someone on amiodarone is caused by the drug. Diabetes is far more common than amiodarone neuropathy, and the average patient on amiodarone tends to be older, often diabetic, often with some baseline nerve risk from other sources. Sorting causation can be genuinely difficult.
Stopping amiodarone abruptly without a plan can trigger life-threatening arrhythmias in some patients. The decision belongs to your cardiologist.
Bring this to your next cardiology visit: when the symptoms started, what they feel like, how they're affecting daily function, whether you've had any falls, any other new amiodarone-related symptoms (cough, shortness of breath, vision changes).
Some features make amiodarone more likely as the driver:
- Symptom onset clearly after starting the drug, with no obvious neuropathy beforehand. Onset typically occurs 6 months to several years into treatment.
- Higher doses or higher cumulative exposure. If you started on 400 mg/day for loading and have been on 200 mg/day for years, the cumulative dose is substantial.
- Mixed motor and sensory involvement with relatively early weakness, rather than pure sensory burning.
- Other amiodarone side effects appearing at the same time — corneal microdeposits, mild thyroid changes, skin photosensitivity, slowly developing pulmonary issues. These tend to cluster.
- Nerve conduction studies showing a mixed demyelinating-axonal pattern. Pure diabetic neuropathy tends to look more uniformly axonal.
A formal evaluation by a neurologist usually includes nerve conduction studies and electromyography, blood work to rule out other treatable causes (B12, glucose, thyroid, kidney function), and a careful medication history that catches not just amiodarone but other contributors. Other medications that damage nerves can stack with amiodarone in ways that make each one worse.
The Hard Conversation: Stopping or Continuing
If amiodarone is the likely cause of a developing neuropathy, the decision about whether to stop the drug is rarely simple. This is genuinely your cardiologist's call, not mine and not your neurologist's alone, because the consequences of stopping amiodarone can be severe.
The realistic options usually look like this.
Lower the dose. For many patients on chronic amiodarone, the dose used for rhythm maintenance is well above what they actually need. A dose reduction — say from 200 mg/day to 100 mg/day or every other day — can sometimes stabilize or even partly reverse the neuropathy while keeping rhythm control. This is often the first move when the neuropathy is mild and the cardiac indication is strong.
Switch antiarrhythmic. Other antiarrhythmic drugs exist (dofetilide, sotalol, propafenone, flecainide, dronedarone) and depending on the cardiac diagnosis, they may be appropriate substitutes. Dronedarone is structurally similar to amiodarone but without the iodine and with a much lower neuropathy risk — for some patients, it's a useful step-down. The catch is that none of these alternatives is universally as effective as amiodarone, and not all are safe in every cardiac situation. This is a complex risk-benefit decision.
Catheter ablation. For atrial fibrillation in particular, the technology and outcomes of catheter ablation have improved enough that many patients who were on amiodarone for years are now candidates for an ablation procedure that eliminates the need for the drug. Success rates vary by AFib type, age, and atrial size, but for younger patients with paroxysmal AFib, success rates over 70–80% are realistic.
Implantable cardioverter-defibrillator (ICD) optimization. For patients on amiodarone primarily to reduce ICD shocks, sometimes ICD programming can be optimized, or other adjunctive measures used, to allow the amiodarone dose to come down.
Stay on amiodarone and manage the neuropathy. For some patients — particularly those with refractory ventricular arrhythmias where amiodarone is genuinely lifesaving and no alternative is safe — the right answer is to stay on the drug, monitor the neuropathy closely, and treat the symptoms aggressively with the standard neuropathic pain toolkit.
The point is that there is almost always something to discuss with the cardiologist. The worst outcome is the patient who develops neuropathy, doesn't mention it, and stays on the drug at the same dose for years while the nerve damage slowly accumulates beyond the reversible range.
What Happens When You Stop Amiodarone
This is the question I get most often from patients who have stopped or reduced amiodarone because of neuropathy concerns. How fast does the nerve damage reverse, and how much can I get back?
The honest answer is “slowly, and partly.” Because amiodarone accumulates so heavily in tissues and has such a long half-life, blood levels remain elevated for months after stopping the drug. The nerve recovery curve is correspondingly slow. Most patients see some improvement within 3 to 6 months of dose reduction or discontinuation. Maximum recovery often takes 12 to 24 months. The improvement is generally more in pain symptoms (burning, tingling) than in pure numbness or weakness, because pain is mediated by smaller fibers that regrow more readily than the larger motor and proprioceptive fibers.
Some residual neuropathy almost always remains, especially if the drug was on board for years before discontinuation. This is why early recognition matters so much — the longer the cumulative exposure, the more axonal damage there is, and the less complete the recovery.
During the recovery period, the standard neuropathy management tools — symptom tracking, supportive footwear, gentle movement, nutritional adequacy — all still apply. So does pain management when needed.
Managing Symptoms While the Cause Is Being Sorted Out
While you and your cardiology team are working out the long-term plan, the day-to-day symptoms still need managing. The toolkit is essentially the same as for any other peripheral neuropathy, and most of it doesn't interact with amiodarone.
For pain symptoms, the standard first-line medications — gabapentin, pregabalin, duloxetine, and tricyclic antidepressants — can all be used in patients on amiodarone, with one important caution. Several antiarrhythmic and neuropathic pain drugs can affect the heart's QT interval, and amiodarone already prolongs QT. A cardiologist should weigh in on any QT-prolonging medication. Gabapentin and pregabalin don't carry this risk and tend to be the safer choice from a cardiac perspective.
For non-drug symptom relief, the gate-closing therapies all remain available. TENS units, foot massage, compression socks, warm foot soaks, and gentle daily movement can all help and don't interact with the drug. Topical options include capsaicin cream, lidocaine patches, and menthol-based products.
For nutritional support, addressing B12, folate, and other relevant deficiencies matters more in amiodarone neuropathy than in many other types, because a nerve already under metabolic stress benefits from removing any other limiting factors. Alpha-lipoic acid and other antioxidants don't have specific evidence in amiodarone neuropathy, but they're reasonable adjuncts for someone with mixed mechanisms.
For balance and safety, the loss of proprioception is the single most underrated risk in amiodarone neuropathy. Older patients with reduced foot sensation are at meaningfully higher risk of falls. Targeted balance training, supportive footwear, removal of household trip hazards, and night-lights for bathroom trips matter at least as much as pain control.
What to Watch For Long-Term
If you stay on amiodarone — at any dose — the long-term monitoring matters. Most cardiologists order baseline pulmonary function tests, liver enzymes, thyroid function, and an eye exam, and repeat several of these annually. Add to that list, in patients with any neuropathic symptoms or known risk factors, a baseline neurological exam and consideration of nerve conduction studies if symptoms develop.
What you can do as the patient is keep a running symptom diary — a simple daily log of any sensory changes, balance issues, falls, or new pain. The pattern over weeks and months is what matters, and you'll see it more clearly in a written record than in memory. Bring that record to every cardiology and primary care visit. It's the single most useful thing a patient can do to make sure the neuropathy doesn't quietly accumulate.
Watch for the cluster — if you're noticing the neuropathy, also pay attention to any new shortness of breath, dry cough, fatigue, weight changes, eye symptoms (halos around lights, light sensitivity), or skin discoloration. These can all be amiodarone-related, and a cluster of side effects often shifts the cardiology calculus toward switching the drug.
The Honest Bottom Line
Amiodarone neuropathy is real, more common than the drug label suggests, and often partly reversible if caught early. The drug is also, for many of the people who take it, genuinely irreplaceable. Those two facts have to sit side by side in any conversation about it.
If you're on amiodarone and starting to notice nerve symptoms, the move is not to stop the drug on your own. The move is to bring it up at your next cardiology visit with specifics — when did the symptoms start, what do they feel like, how have they progressed, what's making your daily life harder. Ask whether dose reduction, switching to a different antiarrhythmic, or evaluation for ablation makes sense in your particular case. Get neurology involved if the cardiologist hasn't already.
The patients who do best with amiodarone neuropathy are the ones who treat it as a known risk to monitor, not as a vague possibility to ignore. They catch the symptoms early, have the conversation early, and either get the drug adjusted while the nerves can still recover or accept the trade-off with clear eyes and good symptom management.
Frequently Asked Questions
Is amiodarone neuropathy reversible? Partly, in most cases. The demyelinating component — damage to the insulation around nerve fibers — often improves over 6 to 24 months after the drug is reduced or stopped. The axonal component — damage to the actual nerve fibers — recovers more slowly and incompletely. Patients who caught the neuropathy early and reduced exposure quickly tend to recover most fully. Those who stayed on full doses for years after symptoms developed often have permanent residual damage.
How long does it take for amiodarone to leave the body? A long time. Amiodarone has an extraordinarily long elimination half-life — typically 50 to 100 days, sometimes longer. That means after stopping the drug, levels in your blood and tissues are still measurable for many months. This is why nerve recovery is gradual, not immediate.
Can I take gabapentin or pregabalin while on amiodarone? Yes, both are generally considered safe to combine with amiodarone. Neither significantly affects the QT interval, and there are no major drug interactions. As with any change, your prescribing doctor and pharmacist should confirm based on your full medication list — but in the absence of other complications, gabapentin and pregabalin are the more cardiac-friendly choices for amiodarone-related nerve pain.
Does dronedarone have the same neuropathy risk as amiodarone? No. Dronedarone is a related but structurally distinct drug that does not contain iodine and does not accumulate in tissues the way amiodarone does. The peripheral neuropathy risk with dronedarone is much lower. The trade-off is that dronedarone is less effective than amiodarone for some arrhythmias and is contraindicated in certain heart failure and atrial fibrillation populations. Whether you can switch is a cardiology-specific decision.
Will the neuropathy keep getting worse if I stay on amiodarone? If nothing changes, it often does — slowly. Continued accumulation of the drug in nerve tissue without compensating recovery time tends to progress the damage. This is why dose reduction is usually the first move when neuropathy develops, even if the patient stays on some amiodarone. Even modest reductions in cumulative dose can stabilize the neuropathy.
How is amiodarone neuropathy different from diabetic neuropathy? Both present in a similar stocking-glove pattern. The differences are subtle and often require nerve conduction studies to clarify. Amiodarone neuropathy more often has prominent demyelinating features (slow nerve conduction with relatively preserved axon counts) and earlier motor involvement, while diabetic neuropathy tends to be predominantly axonal and predominantly sensory in the early years. Mixed pictures are common in patients who have both conditions.
Should I stop amiodarone if I develop neuropathy? Not on your own. The decision belongs to your cardiologist, who has to weigh the seriousness of your underlying arrhythmia against the neuropathy. Some patients can safely stop or switch. Others genuinely can't. What you should do is bring the symptoms to your cardiologist's attention as early as possible so the conversation can happen while you still have options.
Are there blood tests that can tell me how much amiodarone has built up? Amiodarone and its main active metabolite (desethylamiodarone) can be measured in blood, and some monitoring centers use these levels. They're not routine in most outpatient cardiology practices, and the levels don't always correlate cleanly with side effects. Cumulative dose and time on the drug, in practice, are better proxies for tissue accumulation than blood levels alone.


