You know that reflex you have when you stub your toe? You don't think about it. You grab it, squeeze it, rub it. The pain dulls for a moment. Then it surges back. Then you rub again.
That instinct — rubbing the spot that hurts — is one of the oldest pain remedies in human history. Your grandmother did it. Her grandmother did it. And up until about sixty years ago, no one had any real idea why it worked.
Then in 1965, two scientists named Ronald Melzack and Patrick Wall published a paper in Science that changed everything we thought we knew about pain. They called their idea the Gate Control Theory. It was elegant, it was testable, and it suddenly made sense of dozens of strange observations about pain that had been piling up for years. Why does ice help? Why does a TENS unit work? Why does a massage feel good on a sore back? Why does scratching relieve an itch? The gate control theory gave doctors and patients a way to think about all of it.
For those of us living with neuropathy, this theory matters more than it might for someone with a sprained ankle. It's the reason behind several of our most useful tools — TENS, foot massage, vibration plates, compression — and it's also why some of those tools work brilliantly for one person and barely at all for another. I want to walk you through it the way I wish someone had walked me through it. No jargon you don't need. No equations. Just the picture.
The Old Way of Thinking About Pain
Before 1965, the textbook model of pain went something like this. You touch a hot stove. Pain receptors in your skin fire. A signal travels up a wire — a nerve — to your brain. Your brain reads the signal. You feel pain. Pull your hand away.
That model treated pain like a doorbell. Push the button at one end, hear the bell at the other. Pain was a one-way street with a fixed volume. The more damage, the louder the bell.
The problem was that this model couldn't explain reality. Soldiers wounded in battle sometimes felt almost no pain in the moment. Patients with arthritis felt worse on rainy days and better on dry ones, with no change in the joints themselves. People with phantom limb pain felt agony in arms and legs that no longer existed. And every nurse, every mother, every massage therapist knew the central oddity — when one part of you hurts, touching another part nearby often helps.
The doorbell model couldn't explain any of it. Something more was going on between the skin and the brain. Melzack and Wall set out to find it.
What Melzack and Wall Actually Proposed
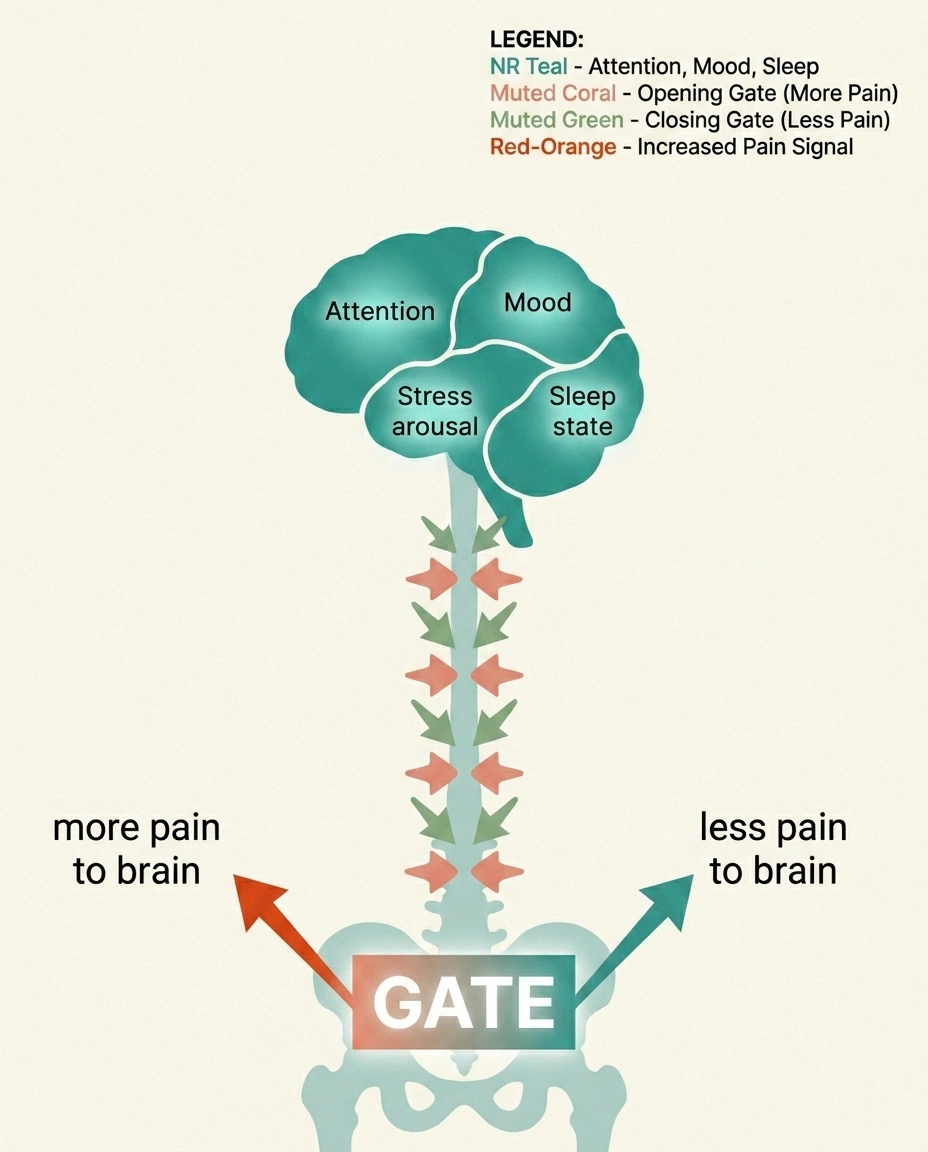
Their idea, in plain language, is this. Pain signals don't travel directly from your skin to your brain on a single express line. They pass through a relay station in your spinal cord — specifically a thin sliver of tissue called the substantia gelatinosa, in the dorsal horn of the cord. At that relay station, pain signals can be amplified, dampened, or stopped entirely, depending on what else is coming in at the same time.
Pain signals don't travel straight to your brain. They pass through a relay station in your spinal cord — a “gate” — that can be opened or closed by other sensory input from your skin and by signals coming down from your brain. Large-fiber input (touch, pressure, vibration) closes the gate. Small-fiber input (pain, temperature) opens it. That's why rubbing the spot that hurts actually helps.
Think of it as a gate. If the gate is open, pain signals flow through and reach the brain. If the gate is partly closed, fewer signals get through, and the pain you feel is less intense. If the gate is fully closed, you feel almost nothing — even when the original injury hasn't changed.
What decides whether the gate is open or closed? Two main things. First, the kind of nerve signals arriving from the body. Second, signals coming down from the brain.
Here's where the elegance of the theory shows up. You don't have just one kind of nerve fiber in your skin. You have several, and they don't all carry the same information.
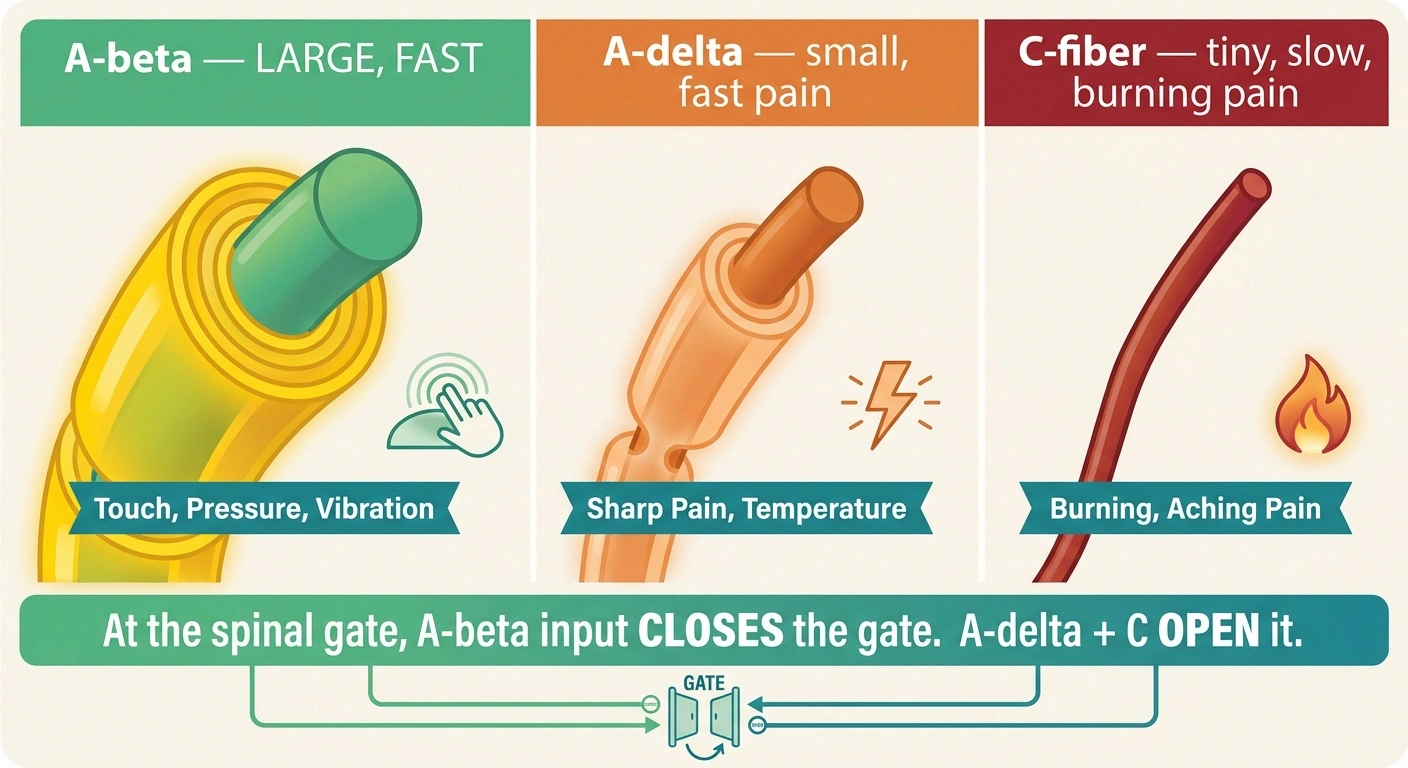
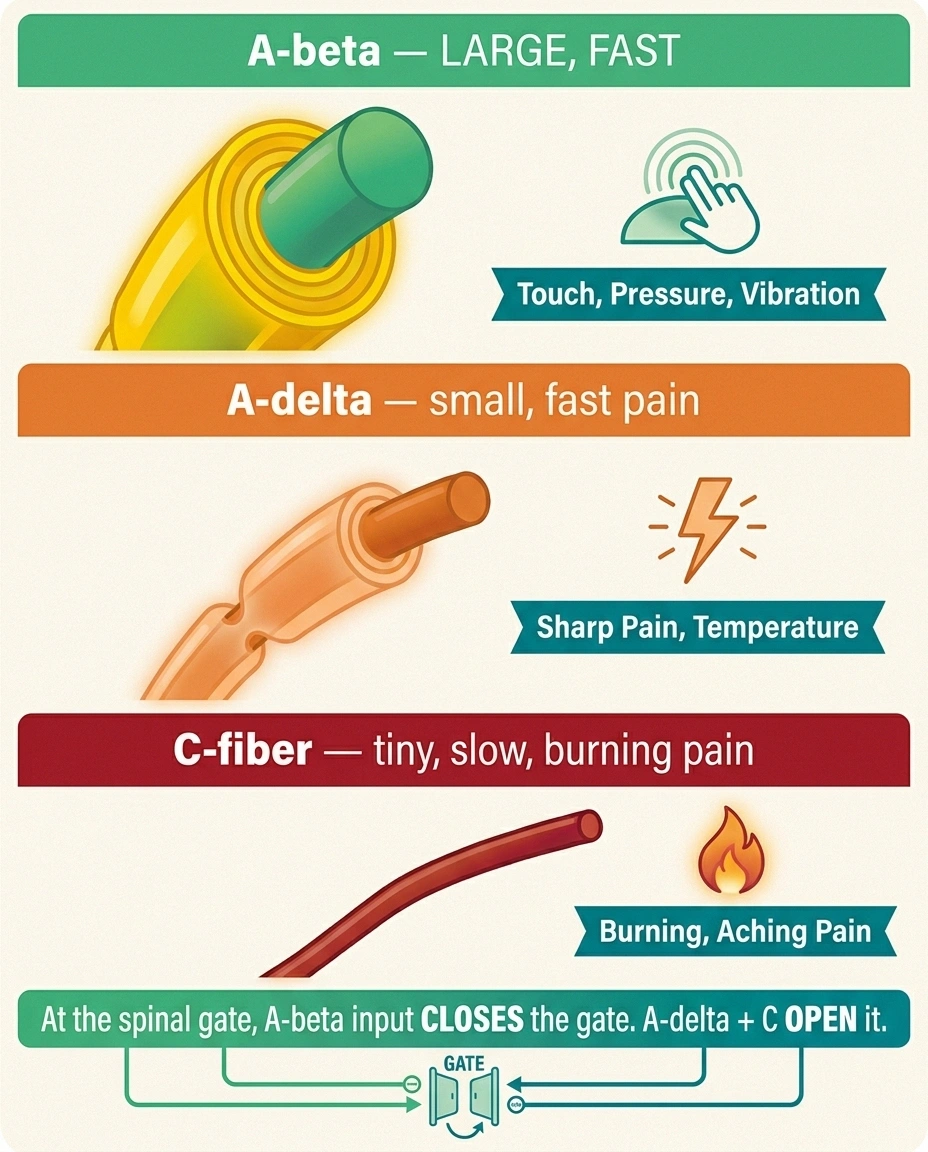
- Large fibers (called A-beta fibers) are thick, fast, and well-insulated with myelin. They carry information about light touch, vibration, and pressure. They fire when something brushes your arm, when you run your fingers across a surface, when you press on a sore spot.
- Small fibers (called A-delta and C fibers) are thinner, slower, and either lightly insulated or not insulated at all. They carry pain and temperature information. The sharp first pain when you cut yourself is mostly A-delta. The dull, burning, lingering pain that follows is mostly C-fiber.
Melzack and Wall proposed that large-fiber input closes the gate, and small-fiber input opens it. When you rub a sore spot, you flood the relay station with large-fiber input. That input crowds out the small-fiber pain signals trying to reach the brain. The gate closes. You feel less pain.
That's the whole core of it. Once you have the picture, almost every other observation about pain starts to make sense.
Why Rubbing the Spot Actually Works
This is the simplest, most universal demonstration of the theory. When you stub your toe and grab it, you're not just expressing pain. You're treating it. The pressure and motion of your hand fire the large fibers in the skin of your toe and the surrounding skin. Those large-fiber signals reach the relay station before the slow C-fiber pain signals do. The gate partly closes. The pain dulls.
Melzack and Wall, Science, 1965 — the founding paper:
- Identified the dorsal horn of the spinal cord as a gating mechanism, not a simple relay
- Showed that pain perception depends on the balance of large-fiber vs small-fiber input
- Predicted that electrical stimulation of large fibers would dampen pain — confirmed shortly after with the first TENS units
- Introduced descending modulation from the brain as a real, mechanistic part of pain perception
Still cited in almost every modern pain textbook 60 years later.
The same mechanism is why a massage feels good on a sore back. Why a cold compress helps a bruise. Why you reflexively scratch a mosquito bite. Why a warm hand on a child's stomach can quiet the ache. None of these things repair the underlying problem. They just close the gate temporarily.
For neuropathy patients, this is the foundation of why foot massage, gentle vibration, and even compression socks can take the edge off — they all flood the affected area with large-fiber input.
How TENS Units Use the Same Principle

If you've ever tried a TENS unit for nerve pain, you've used the gate control theory directly — even if no one explained it that way. TENS stands for transcutaneous electrical nerve stimulation. The little patches deliver mild electrical pulses through the skin. Those pulses preferentially stimulate the large A-beta fibers in the skin, because large fibers have lower stimulation thresholds than the small pain fibers.
The result, in theory, is the same as rubbing the spot — a wave of large-fiber input that closes the gate and quiets the pain signals trying to come through. In practice, the results vary. Some neuropathy patients get meaningful relief from TENS. Some feel almost nothing. The difference often comes down to which fibers are still working in their feet or hands. If small-fiber neuropathy has wiped out most of the pain-carrying fibers but spared the large fibers (which is actually common), TENS can work very well. If both fiber types are damaged, the input has less to ride on.
This is one reason it can be worth getting a proper sense of your fiber-type involvement before judging whether TENS, vibration, or massage are working as well as they could. Small fiber neuropathy and large-fiber neuropathy don't behave the same, and the gate control machinery depends on the large fibers being intact.
What Comes Down From the Brain
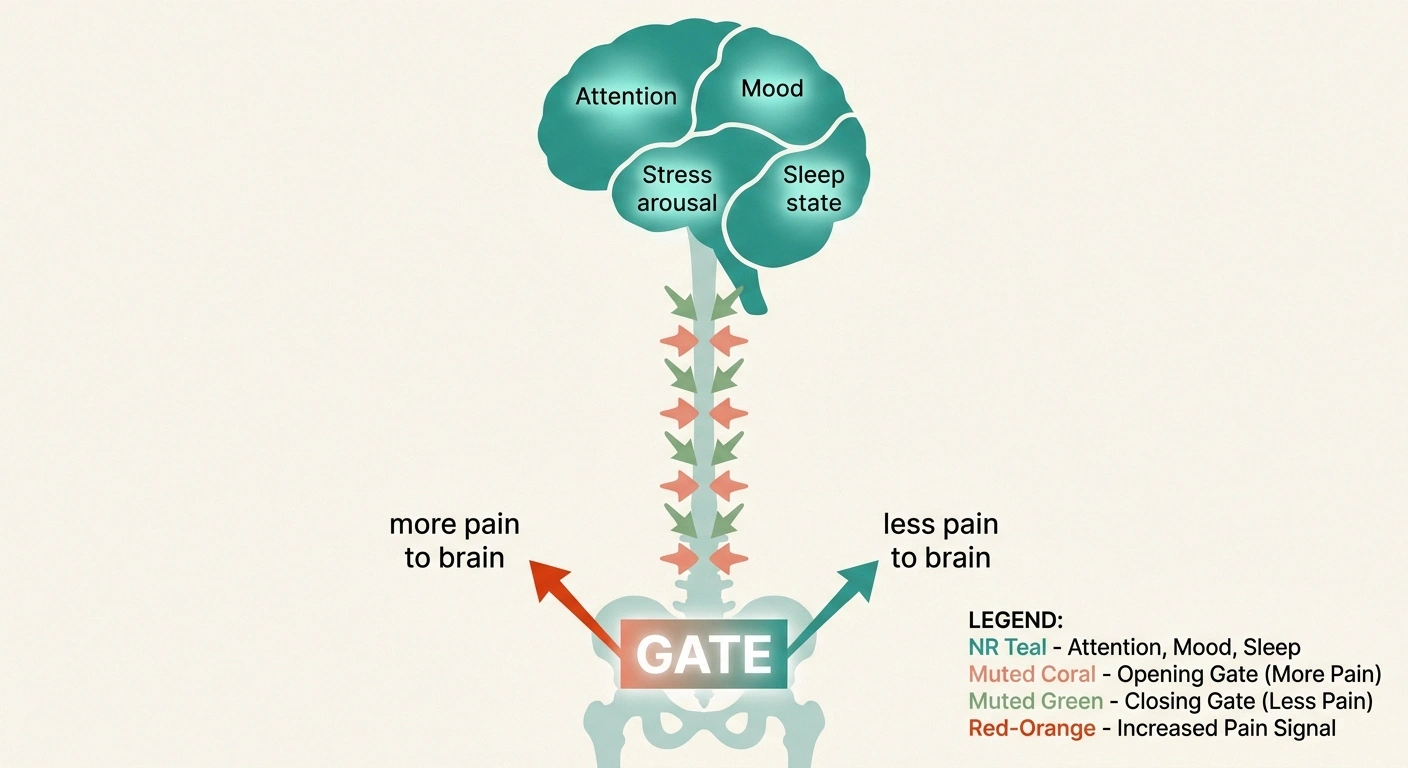
Melzack and Wall's original paper proposed something else that turned out to be just as important. The gate isn't only controlled from below — from the skin and nerves. It's also controlled from above — from the brain itself.
The brain has nerve pathways that descend from areas involved in attention, emotion, and arousal, and those descending fibers can either close the gate or open it. When you're calm, focused, distracted, or experiencing pleasure, descending signals tend to close the gate. When you're anxious, fearful, exhausted, or hyperfocused on the pain, descending signals tend to open it wider.
This is why stress makes neuropathy pain worse. It's why pain feels louder at 3 a.m. than at 3 p.m. It's why you can be absorbed in a movie or a conversation and notice your feet less, and why the pain rushes back the moment you sit alone in silence. It's not “in your head” in the dismissive sense. It's that the literal neural traffic going down from your brain to your spinal cord is opening the gate wider when you're stressed and closing it more when you're calm.
That descending modulation is also why work on sleep, mood, and mental health isn't optional for chronic pain management. They're not “extras” you do once the pills are working. They're load-bearing parts of the gate.
Why Ice, Heat, and Vibration All Have a Place
Every common topical pain therapy you've ever tried — ice, heat, vibration, massage, capsaicin cream, menthol, essential oils — is, at some level, a gate-control intervention. Each of them generates a strong, competing sensory signal from the skin that floods the relay station with non-pain input.
- Cold stimulates A-delta cold fibers (a different small-fiber population from pain fibers), and at the cord level, cold input both competes with C-fiber pain input and triggers descending pain inhibition.
- Heat activates a mix of fibers and also triggers descending modulation by changing the brain's overall arousal state — warmth tends to be calming.
- Vibration is one of the most pure ways to fire A-beta fibers. It's the reason vibration plates, vibrating massagers, and even rumble settings on TENS units can feel surprisingly good on a neuropathic foot.
- Counterirritants like menthol and capsaicin create a strong sensation (cooling or burning) that competes with the underlying pain.
None of these is a cure. None of them repairs nerves. They are tools to close the gate temporarily and give you relief while your nerves heal — or while you work on the underlying causes.
What the Theory Doesn't Explain
It's only fair to say what the gate control theory got wrong, or didn't yet know. By the 1980s, it was clear that the original 1965 model was missing pieces.
Signs of central sensitization — sensory therapies alone won't be enough:
- Light touch becomes painful (allodynia)
- Rubbing the spot makes the pain worse, not better
- Pain spreads beyond the original area
- Pain persists long after the triggering input stops
Talk with your prescriber about gabapentin, pregabalin, or duloxetine in this case — they work on the central nervous system, not the gate.
First, the dorsal horn turned out to be more complex than a single gate. There are multiple layers of cells, multiple neurotransmitters, and a whole inflammatory cascade involving the immune cells in the cord. The “gate” is more like a switchboard with dozens of dials.
Second, in chronic pain conditions — including many forms of neuropathy — the gate can get stuck open. The spinal cord cells become hyperexcitable. The descending inhibition weakens. The brain's pain map itself reorganizes. This is the phenomenon of central sensitization, and it's why some neuropathic pain stops responding to the simple “rub it, ice it, distract from it” approaches that work fine for acute pain.
Third, Melzack himself updated the theory in the 1990s into something called the neuromatrix model. He came to believe that pain is generated by a distributed network of brain regions — not just by signals coming up from the body. The neuromatrix model is what explains phantom limb pain, why amputees can feel agony in a missing leg, and why brain-based therapies like cognitive behavioral therapy and graded motor imagery can actually shift chronic pain.
None of this means the gate control theory is wrong. It's still correct as far as it goes. It just doesn't go all the way to the brain. We've spent the last sixty years filling in what comes after the gate.
What This Means for Living With Neuropathy
If I had to boil the gate control theory down to a single practical insight for someone with neuropathy, it would be this. You have more control over what reaches your brain than you might think.
Every day, you make small choices that either close the gate or open it. The choices that close it tend to be the things we already know are “good” — gentle movement, warmth, calm, social connection, a distracted absorption in something you love. The choices that open it tend to be the things we already know are “bad” — chronic stress, poor sleep, isolation, fear, hyperfocus on the pain itself.
That doesn't mean you can think your way out of neuropathic pain. You can't. The signals are real, the nerve damage is real, and trying to dismiss them as “just” psychological does enormous damage to people who are already exhausted from being dismissed. But it does mean that the gate is partly under your control, and that's worth knowing.
It also means that when you stack multiple gate-closing interventions, you sometimes get more relief than the sum of the parts. A TENS session followed by a warm foot soak followed by a quiet evening with a favorite show is hitting the gate from three angles at once — sensory input, descending mood-based modulation, and reduced sympathetic arousal. Any one of those alone might give modest relief. Together, they often give more.
Why Some Days Feel Worse for No Obvious Reason
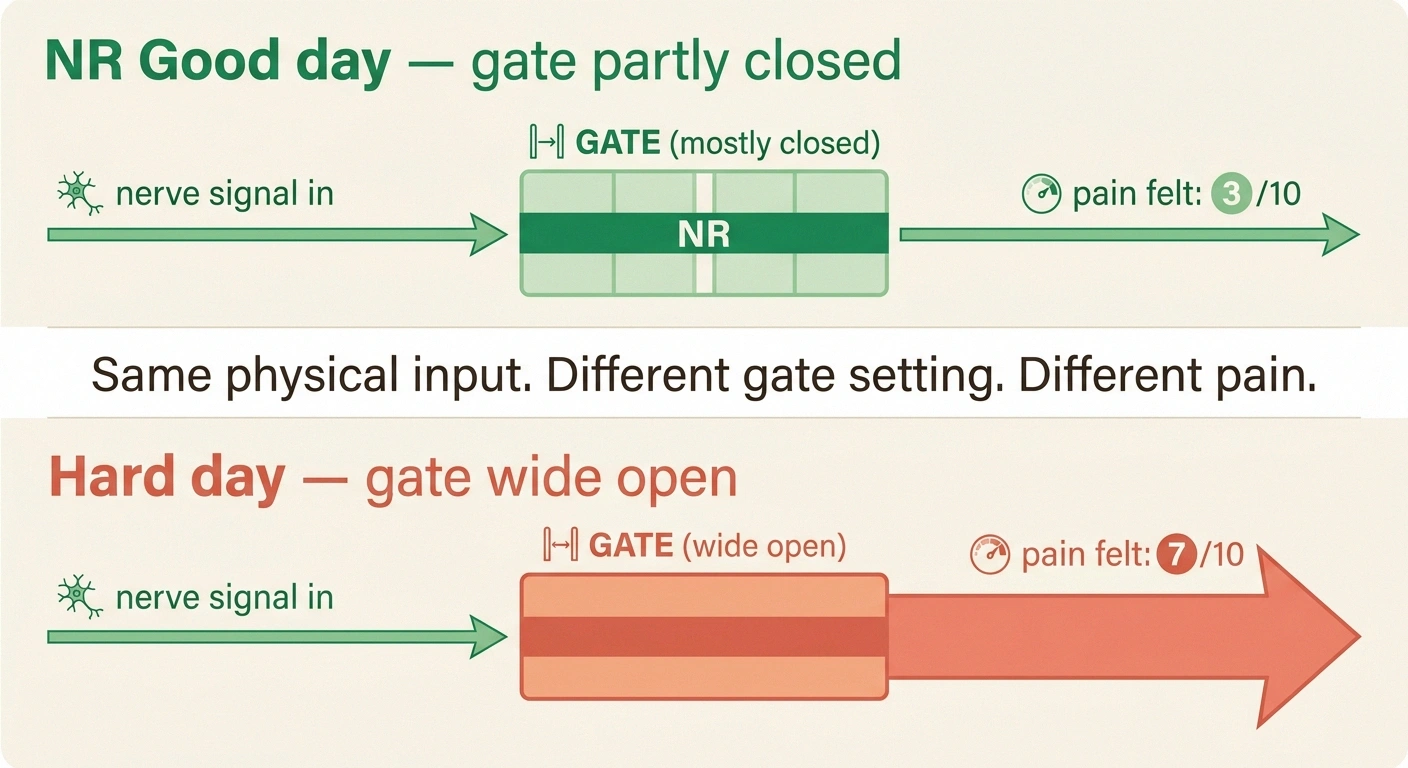
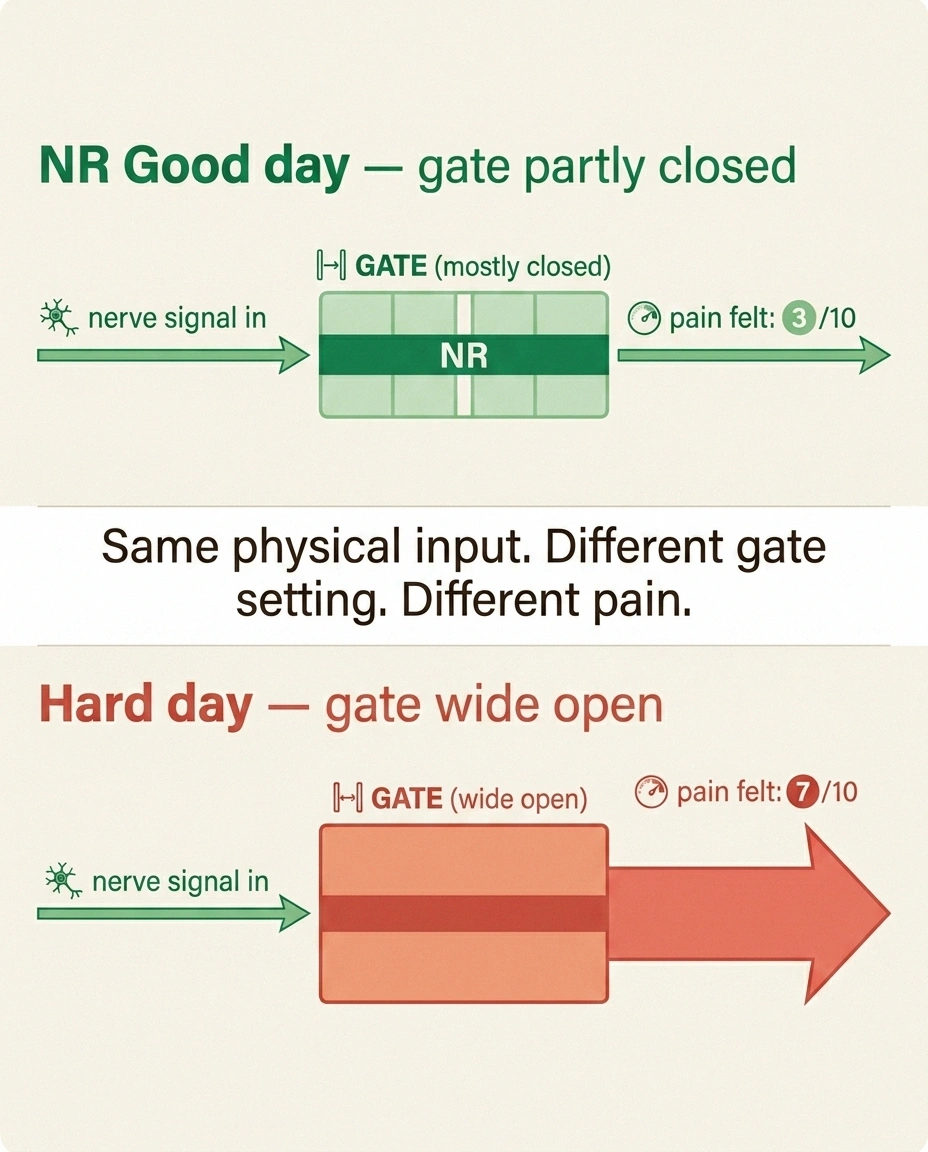
One of the more disorienting parts of living with neuropathy is the day-to-day variability. The damage in your feet doesn't change from Tuesday to Wednesday, but the pain can swing wildly. Gate control gives you a way to think about why.
The literal nerve damage is the input. But what you feel is the input after it's passed through the gate. And the gate is set by sleep quality, stress, weather sensitivity, blood sugar swings, recent activity, mood, and a dozen other things shifting in the background of your day.
This isn't a failure of your discipline. It's the structure of the pain system itself. The same physical damage can produce a 3-out-of-10 day or a 7-out-of-10 day depending on the gate setting. Knowing this can take some of the self-blame out of bad days — and direct your attention toward the things that nudge the gate in the right direction over time.
How to Use the Theory Practically Today

If you wanted to put the gate control theory to work in the next week, here's roughly how I'd think about it.
Layer your sensory input. Pick two or three things from the gate-closing toolkit and use them in sequence rather than alone. A warm soak, then a gentle foot massage, then a TENS session. Or vibration, then compression socks for the rest of the day. The cumulative effect is usually larger than any single tool.
Treat sleep and stress as pain interventions, not lifestyle suggestions. Poor sleep opens the gate. Chronic stress opens the gate. They aren't separate from your nerve pain — they're upstream of it. Anything you do to improve sleep quality or reduce stress is, in a literal sense, closing the gate.
Track which interventions actually work for you. Two people with similar neuropathy can have completely different gate responses. A simple symptom diary — even three rows a day — will tell you in a month which tools are doing real work and which are just busy work.
Don't expect a single intervention to close the gate by itself. The gate is multidimensional. A TENS unit alone might give you 10–20% relief. Combined with good sleep, regular gentle walking, supportive footwear, and stable blood sugar, the same TENS unit might give you 40–50%. The tools work together.
Know when the gate is stuck open. If sensory input no longer dampens your pain at all — if rubbing the sore spot makes it worse, if light touch becomes painful, if pain spreads beyond the original area — that's a signal for central sensitization, and you need a different toolkit. That's the territory of medications like gabapentin, duloxetine, and pregabalin, and it's worth a focused conversation with your prescriber.
The Bigger Picture
What I love about the gate control theory, even sixty years later, is how it shifted the whole moral frame around pain. Before 1965, pain was a doorbell. If it kept ringing, you had a problem to fix or a person who wouldn't stop complaining. After 1965, pain was a conversation — between damage and nerves and mood and attention and meaning — happening in your own body, in real time, all day long.
That's a much more honest picture of chronic pain than the doorbell ever was. And it gives us, as patients, real things to do. Not magical things. Not miracles. But real, evidence-based, gate-closing levers we can pull each day.
I won't pretend I've never had a 9-out-of-10 day where the gate felt jammed wide open and nothing helped. I have. We all have. But on the other days — the average days, the workable days — knowing what's actually happening between my feet and my brain has helped me make better choices about what to do next.
That, in the end, is what good science gives the rest of us. Not a cure. A clearer map.
Frequently Asked Questions
Is the gate control theory still considered accurate? The core of it — that large-fiber input can dampen small-fiber pain at the spinal cord, and that descending signals from the brain modulate the gate — is well-established and still taught in every medical school. What has been updated is the complexity. The dorsal horn is more intricate than a single gate, and chronic pain involves changes throughout the nervous system that the original theory didn't fully capture. Modern pain science builds on gate control rather than replacing it.
Can the gate control theory explain why neuropathy is worse at night? Partly, yes. At night, the distracting sensory input from your environment drops off. There's no movement, no conversation, no visual input. The pain signals have less competition at the gate. At the same time, descending modulation from the brain is often weaker during fatigue, anxiety about sleep, and rumination. Both effects open the gate wider. This isn't the whole story of nighttime neuropathy, but it's a real part of it.
Why does scratching an itch feel so good? The same gate mechanism. Itch is carried by a specific subset of small fibers that travel up the spinal cord alongside pain fibers. When you scratch, you flood the local skin with large-fiber input, which closes the gate on itch signals just as it does on pain signals. The relief is real and immediate. The catch is that scratching also damages skin and can trigger more itch in a longer-term loop.
Does the gate control theory mean I can just distract myself out of pain? Distraction is a real gate-modulating tool, and it works at the level of descending control from the brain. But it's not a substitute for treating the underlying causes. Distraction can take the edge off in a particular moment. It can't fix nerve damage. The honest framing is that distraction is one lever among many — useful, especially for acute spikes, but not the whole answer for chronic neuropathic pain.
If gate control is real, why don't all sensory therapies work for me? Because the gate is multidimensional and your nervous system is specific to you. The fibers carrying the input have to be intact, the descending modulation has to be functioning, and central sensitization has to not be overwhelming the gate from above. If a TENS unit does nothing for you, it doesn't mean the theory is wrong. It means your particular combination of fiber damage, central sensitization, and modulation has the gate set in a way that this specific tool can't reach. Other tools may still work. It's worth trying several.
Are there gate-closing interventions for hand neuropathy specifically? Yes. Vibrating massagers, warm paraffin baths, compression gloves, and small TENS pads designed for the hand all work through the same mechanism as their foot equivalents. The hand actually responds well because the density of large fibers in the palm and fingers is even higher than in the foot. If you have neuropathy in your hands, layered sensory therapy is often quite effective.
Can the gate get permanently stuck open in chronic neuropathy? In a sense, yes — that's what central sensitization is. Repeated pain signaling over months and years can change the spinal cord and brain in ways that keep the gate biased toward open. The good news is that these changes are partly reversible. Consistent gate-closing input over time, combined with appropriate medications and addressing the underlying nerve damage, can shift the system back toward a more normal setting. It's slow work, but it's real work.
Is it safe to use multiple gate-closing therapies at the same time? Generally yes, with sensible caution. Combining TENS with a warm soak, compression, or massage is fine. Combining cold and capsaicin cream is fine. The exceptions are when one therapy might mask a problem you should be tracking — for example, if your nerves are very numb, a heating pad set too high can burn skin without you feeling it, so the gate-closing benefit isn't worth the risk. Use lower-intensity tools layered, not high-intensity tools stacked.