
When your doctor suggests an antidepressant for your nerve pain, the reaction is almost always the same: “But I'm not depressed.” I've heard this from dozens of people in my support groups, and I'll admit I had the same thought when my own doctor first mentioned amitriptyline years ago. It felt like my pain wasn't being taken seriously.
But here's what I've learned since: amitriptyline is one of the most widely prescribed medications for neuropathic pain worldwide, and it works through completely different mechanisms than when it's used for depression. At the low doses used for nerve pain — typically 10 to 75 milligrams versus 150 to 300 milligrams for depression — amitriptyline targets the chemical pathways that carry pain signals, quieting overactive nerves and helping many people get their first decent night's sleep in months.
It's not a perfect medication. It doesn't work for everyone, it comes with side effects that can be bothersome, and the evidence behind it isn't as strong as many doctors assume. But for a subset of people with neuropathy, amitriptyline has been genuinely life-changing — and at just a few cents per pill, it remains one of the most accessible options available.
What Is Amitriptyline and How Does It Work for Nerve Pain?
Amitriptyline belongs to a class of medications called tricyclic antidepressants (TCAs), developed in the 1960s. While newer antidepressants have largely replaced tricyclics for treating depression, amitriptyline found a second life as a pain medication — particularly for neuropathic conditions.
Key Takeaway
Amitriptyline works for nerve pain through completely different mechanisms than when it's used for depression. At the low doses prescribed for neuropathy (10-75 mg vs. 150-300 mg for depression), it targets pain signal pathways — not mood pathways.
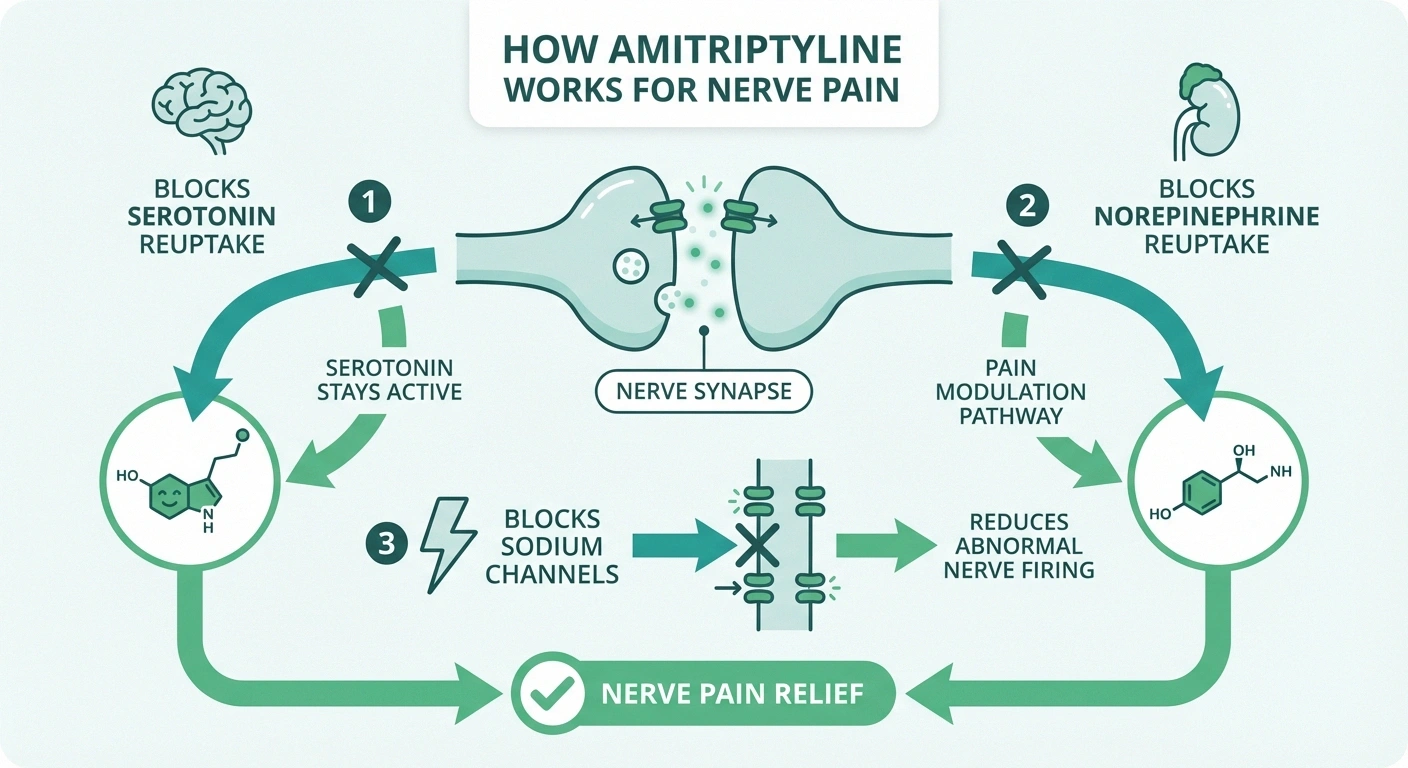
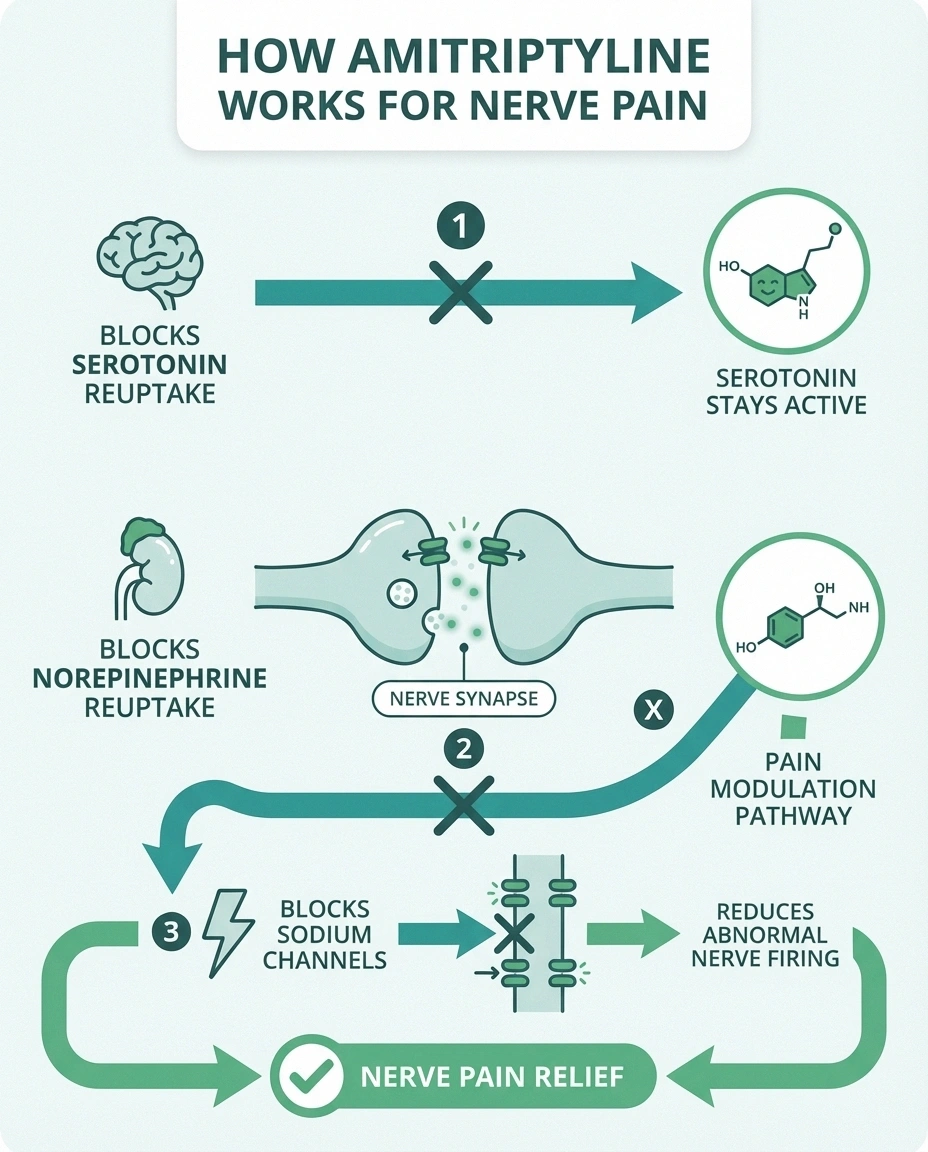
When used for nerve pain, amitriptyline works primarily by blocking the reuptake of two neurotransmitters: norepinephrine and serotonin. These chemicals play crucial roles in how your brain and spinal cord process pain signals. By keeping more of them available in the nervous system, amitriptyline helps turn down the volume on pain transmission — the signals still get sent from damaged nerves, but your brain doesn't amplify them as aggressively.
Amitriptyline also blocks sodium channels in nerves, which may help reduce the abnormal firing patterns that cause burning, shooting, and electric-shock sensations. Additionally, it has mild antihistamine effects, which contribute to the drowsiness that — while sometimes considered a side effect — is actually a benefit for the many neuropathy patients whose pain keeps them awake at night.
It's important to understand that the doses used for pain are much lower than those used for depression. Most people take between 10 and 75 milligrams for neuropathy, compared to 150 to 300 milligrams for depression. At these lower doses, you're unlikely to experience the antidepressant effects — which is exactly the point. You're targeting the pain pathways, not the mood pathways.
What the Evidence Actually Shows
Here's where honesty matters: the evidence for amitriptyline in neuropathic pain is more complicated than most articles acknowledge. A Cochrane systematic review — considered the gold standard of medical evidence analysis — found no first-tier or second-tier evidence supporting amitriptyline for any neuropathic pain condition. All available evidence was classified as third-tier, meaning small studies at significant risk of bias.
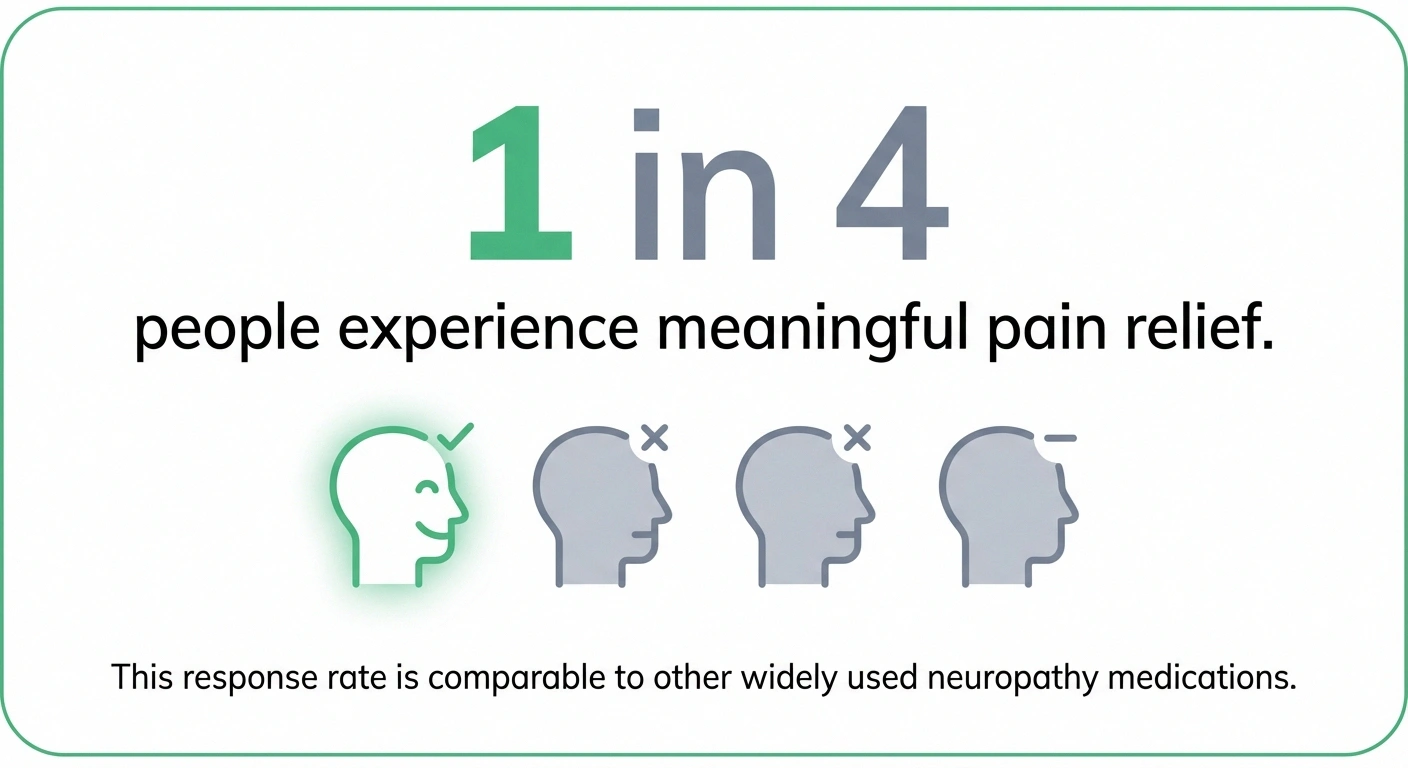
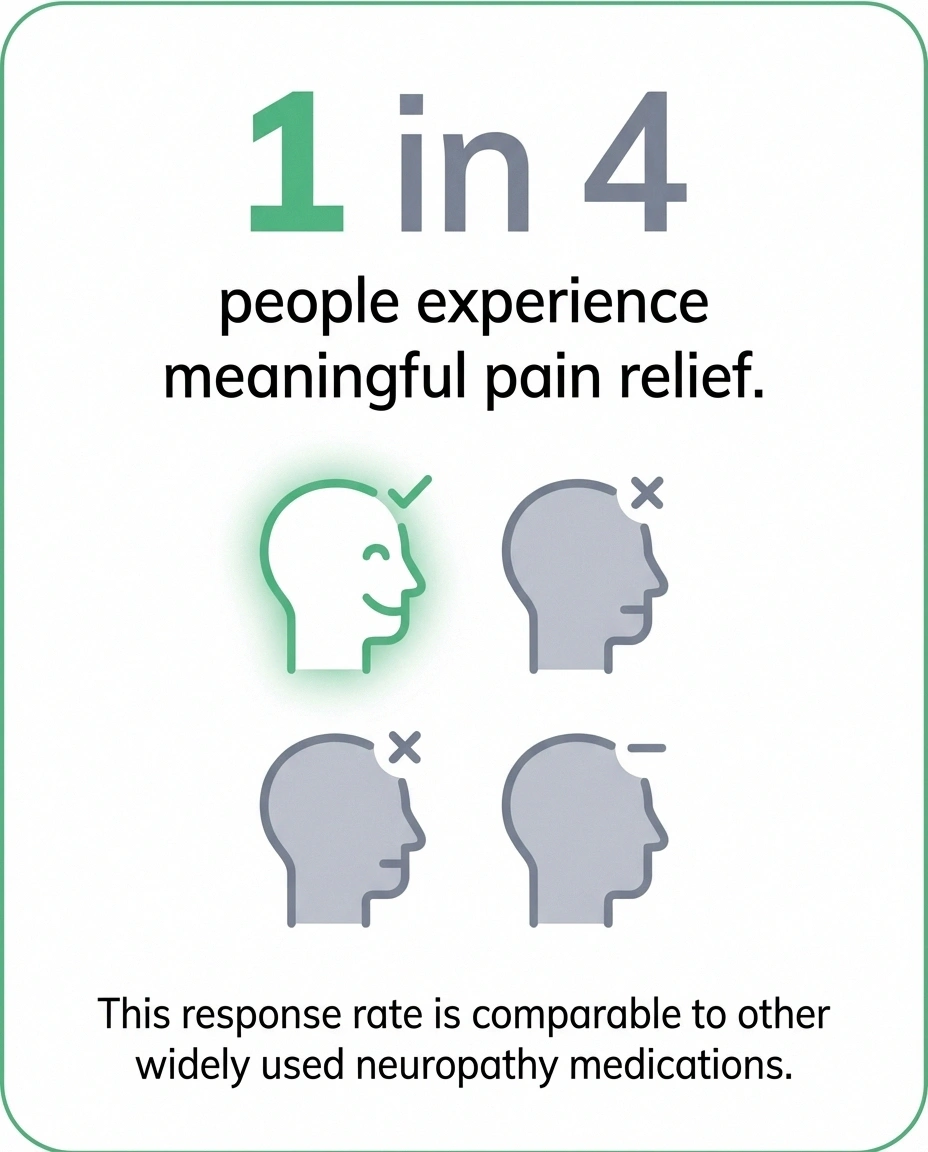
people experience meaningful pain relief with amitriptyline — comparable to gabapentin, pregabalin, and duloxetine
That sounds damning, but the Cochrane authors were careful to add important context: “There is no good evidence of a lack of effect; rather our concern should be of overestimation of treatment effect.” In other words, amitriptyline probably does work for some people — we just can't be as certain about how well it works as decades of clinical use might suggest.
The review's best estimate is that amitriptyline provides meaningful pain relief in roughly one in four people who try it — which is actually comparable to most other neuropathy medications. Gabapentin, pregabalin, and duloxetine all have similar response rates. No single medication works for everyone, which is why neuropathy treatment often involves trying several options.
One landmark study from Neurology specifically examined amitriptyline for diabetic nerve pain and found that its pain-relieving effects were independent of any mood changes — confirming that the mechanism really is about pain pathways, not depression.
Who May Benefit Most from Amitriptyline
While amitriptyline can be tried for most types of neuropathic pain, certain people tend to respond particularly well:
People with pain that disrupts sleep. Because amitriptyline causes drowsiness, it's often prescribed specifically when nighttime pain is a major complaint. Taking it a couple of hours before bed can help you fall asleep more easily while simultaneously dampening pain signals. For many people, this is the most immediate and noticeable benefit.
People with burning or continuous pain. Amitriptyline tends to work best for constant background pain — the steady burning, aching, or throbbing that characterizes many neuropathy cases. It may be less effective for sharp, intermittent shooting pains, though some people find it reduces those as well.
People who haven't responded to gabapentin or pregabalin. Because amitriptyline works through different mechanisms, it may help people who didn't find relief with the first-line anticonvulsant medications. The Cochrane review noted that “failure with one antidepressant does not mean failure with all” — and the same logic applies across drug classes.
People with post-herpetic neuralgia. Amitriptyline has the longest track record in this condition, and it's specifically recommended in most treatment guidelines for nerve pain following shingles.
People looking for an affordable option. Generic amitriptyline costs just a few dollars per month — a fraction of what brand-name topical lidocaine patchess cost. For people without insurance or with high copays, this can be a significant factor.
Amitriptyline does appear to be less effective for some specific conditions. The Cochrane review found it probably does not work well for neuropathic pain associated with HIV or cancer treatments like chemotherapy-induced neuropathy.
How to Take Amitriptyline: The Start Low, Go Slow Approach
The standard approach to amitriptyline for neuropathy follows a “start low, go slow” philosophy that helps minimize side effects while finding your effective dose:
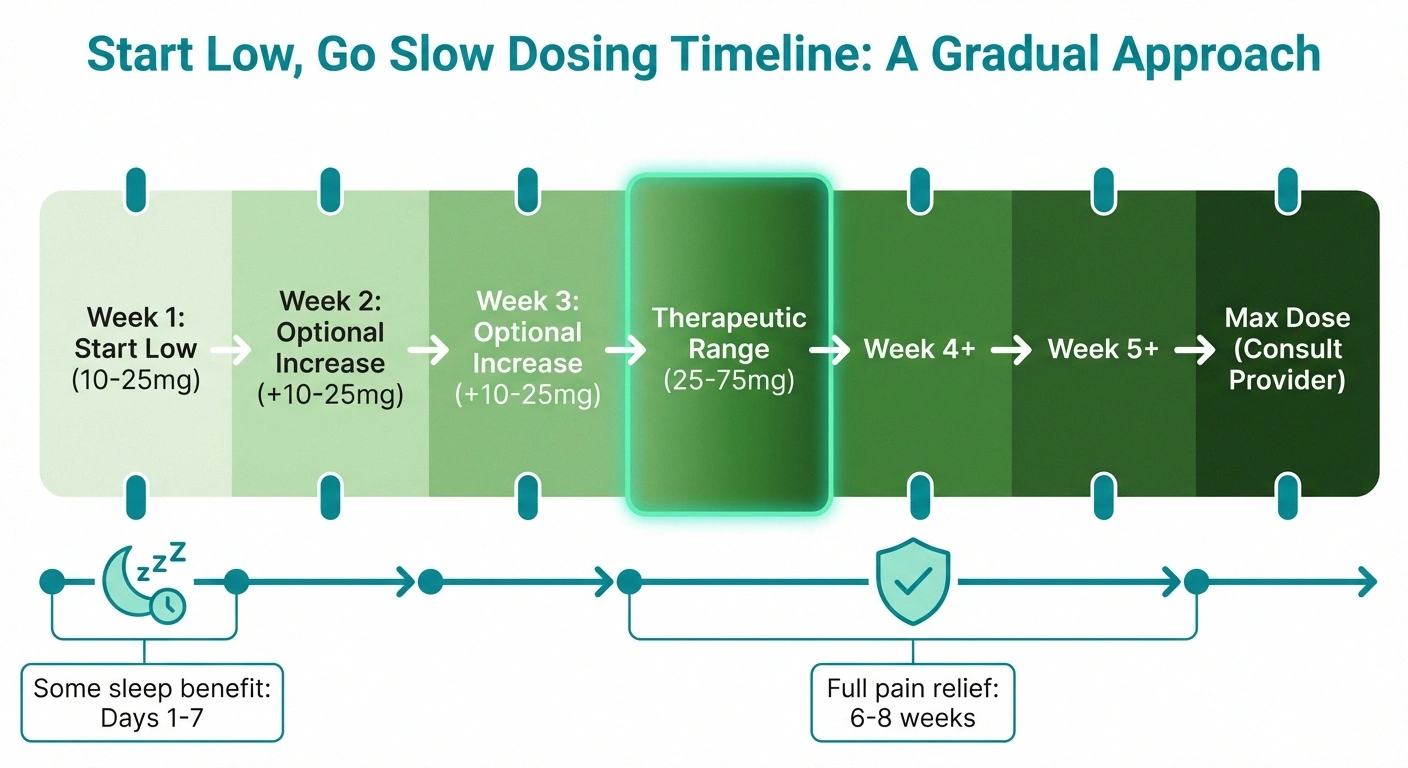
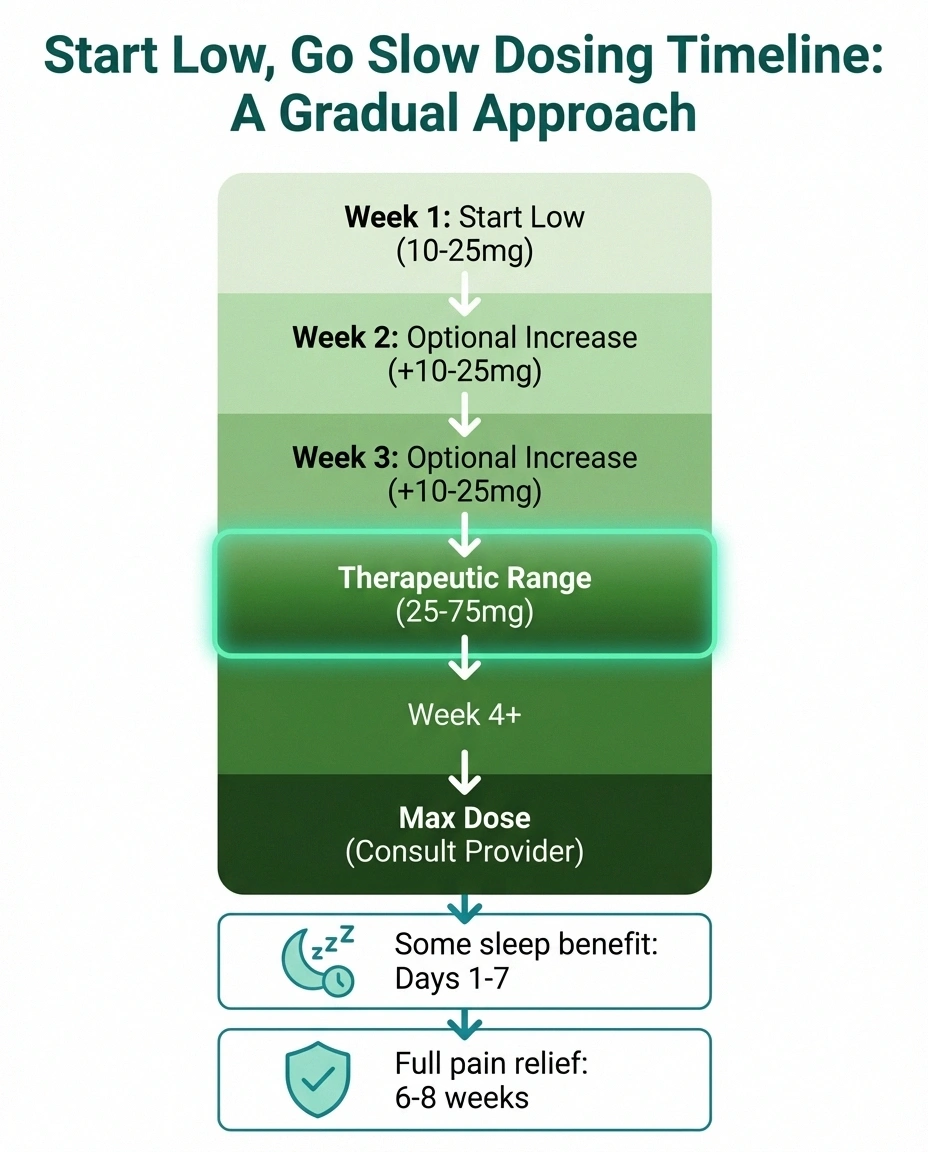
Start Low, Go Slow: Your Amitriptyline Timeline
Start: 10–25 mg at bedtime
Take 1-2 hours before sleep. Sleep improvement may begin within days.
Adjust: Increase 10–25 mg weekly
Only if needed. Wait at least 7 days between increases. Target: lowest effective dose.
Therapeutic range: 25–75 mg
Most people find their effective dose in this range. Pain relief builds gradually.
Full trial: Wait 6–8 weeks
Give amitriptyline adequate time before judging effectiveness. Don't give up after 1-2 weeks.
Starting dose: Most doctors begin with 10 to 25 milligrams, taken as a single dose in the evening — ideally one to two hours before bedtime. This timing takes advantage of the sedating effect rather than fighting against it.
Gradual increases: If the starting dose isn't providing enough relief after one to two weeks, your doctor may increase by 10 to 25 milligrams at a time, waiting at least a week between increases. The goal is to find the lowest dose that provides meaningful pain relief.
Therapeutic range: For neuropathic pain, most people find their effective dose somewhere between 25 and 75 milligrams. Some people respond to as little as 10 milligrams, particularly for sleep improvement. It's unusual to go above 75 milligrams specifically for pain.
Timeline for results: This is where patience becomes important. Some people notice improved sleep within the first few nights, but pain relief typically takes longer — often two to four weeks for noticeable improvement, and up to six to eight weeks for the full effect. Don't give up after a week if the pain hasn't changed yet.
Never stop suddenly. If you and your doctor decide amitriptyline isn't working or you want to switch medications, taper gradually. Stopping abruptly can cause withdrawal symptoms including nausea, headache, and irritability. Your doctor will guide the tapering schedule.
Side Effects: What to Expect and What to Watch For
Amitriptyline's side effects are the main reason some people can't tolerate it — and they should be understood honestly before starting the medication.
Common side effects (these affect a majority of users, though often improve with time):
- Drowsiness — The most reported side effect. It can be a benefit at bedtime but problematic during the day, especially when first starting. Most people adjust within one to two weeks.
- Dry mouth — Very common and often persistent. Sipping water, using sugar-free gum, and saliva substitutes can help manage it.
- Constipation — Amitriptyline slows the digestive tract. Increased fiber, fluids, and staying active can help. For some, this side effect requires treatment with a stool softener.
- Weight gain — Can occur with long-term use, partly due to increased appetite. Not everyone experiences this, but it's worth monitoring.
- Blurred vision — Usually mild and tends to improve over the first few weeks.
- Dizziness when standing — Amitriptyline can lower blood pressure slightly, especially when you stand up quickly. Rise slowly from sitting or lying positions.
- Urinary retention — Difficulty starting urination, particularly relevant for men with prostate issues. Report this to your doctor.
The Cochrane review found that about 55 percent of people taking amitriptyline experienced at least one side effect, compared to 36 percent on placebo. The number needed to harm — meaning how many people need to take the drug before one additional person has a side effect — was about five. However, serious side effects were rare, and people didn't stop taking amitriptyline significantly more often than they stopped taking placebo.
Serious side effects (rare but important to know about):
- Heart rhythm changes — Amitriptyline can affect heart conduction, which is why your doctor may order an ECG before starting it, particularly if you're over 65 or have a history of heart disease.
- Seizure threshold lowering — If you have epilepsy or a history of seizures, amitriptyline may increase risk.
- Serotonin syndrome — Rare but potentially dangerous interaction when combining amitriptyline with other serotonin-affecting drugs (SSRIs, SNRIs, tramadol). Always tell your doctor about all medications and supplements you take.
Amitriptyline Compared to Other Neuropathy Medications
How does amitriptyline stack up against the other commonly prescribed neuropathy medications? Here's an honest comparison based on the available evidence:
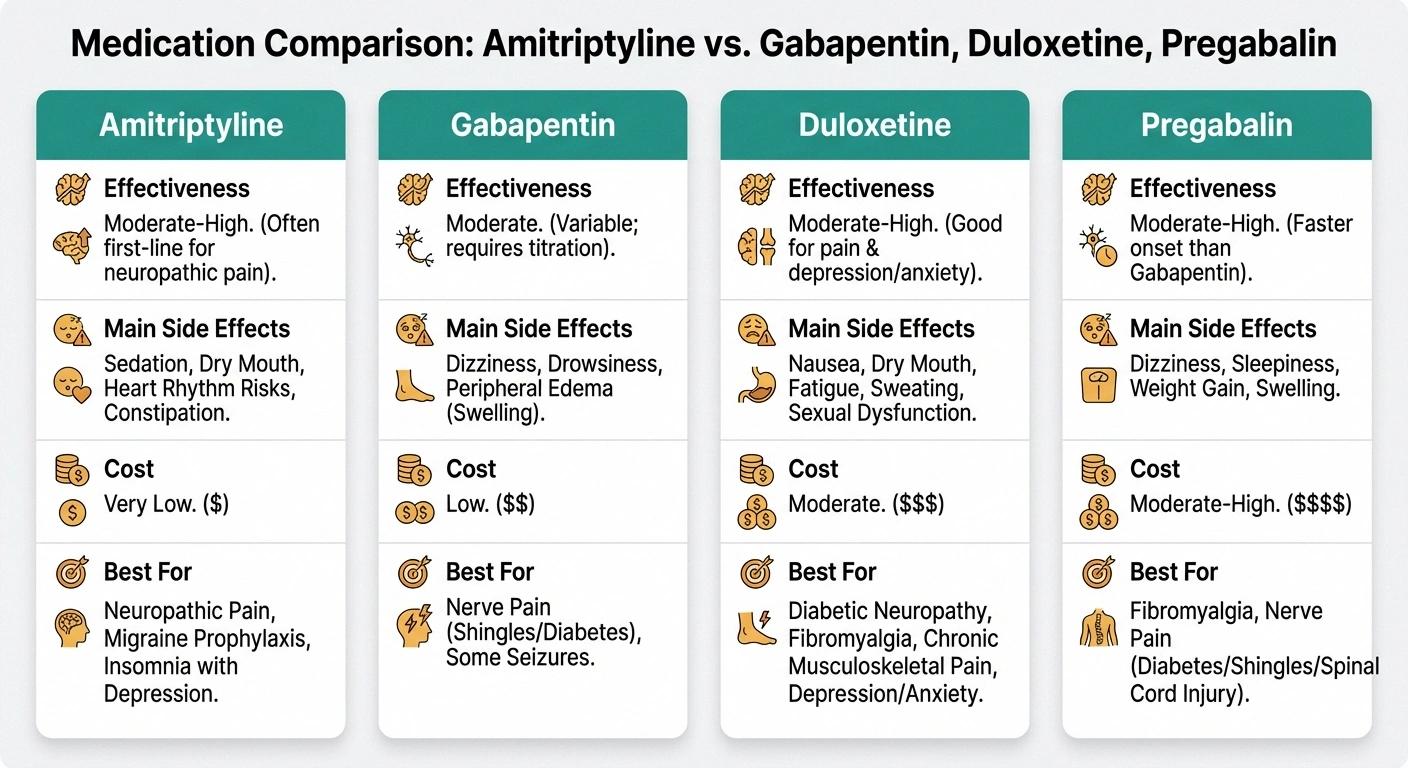
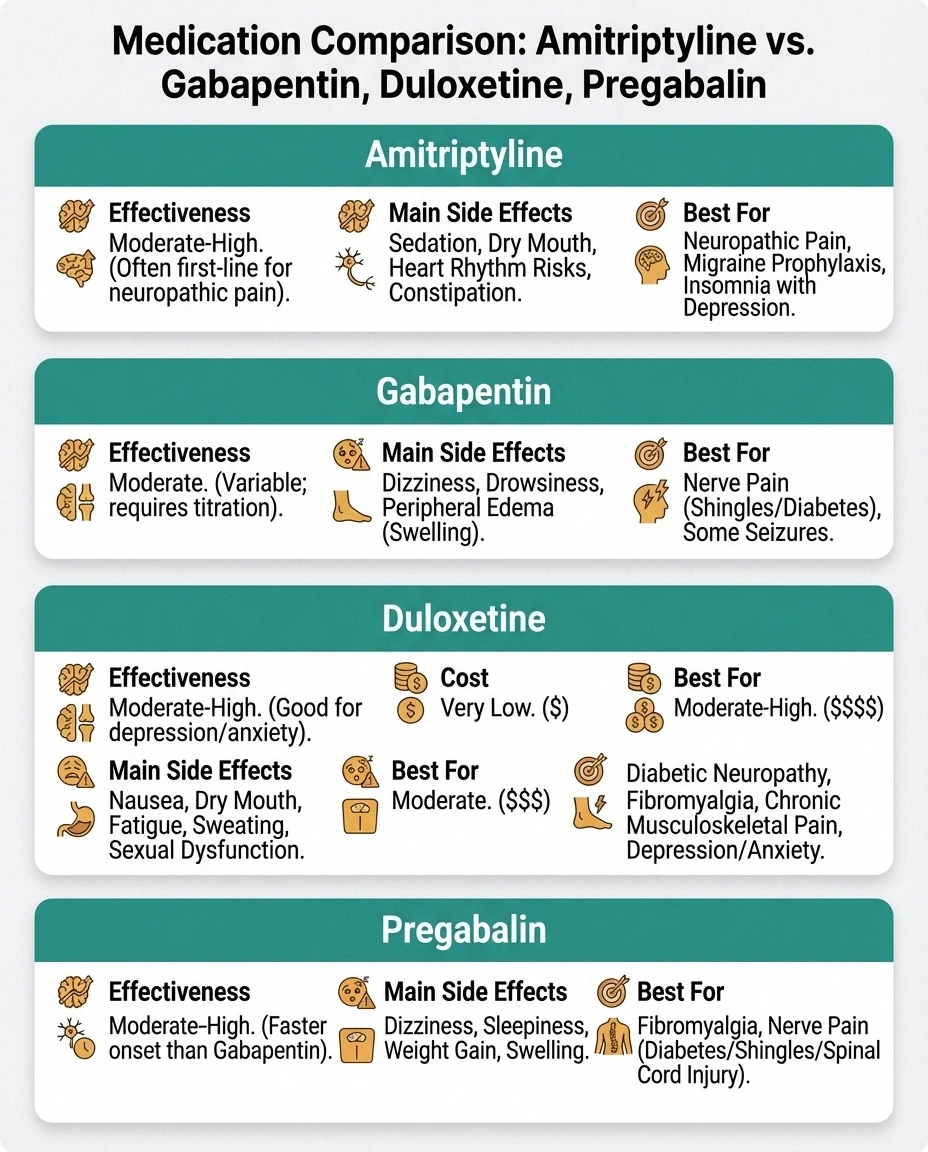
Amitriptyline
Best for: Sleep issues, burning pain
Side effects: Drowsiness, dry mouth
Cost: 💲 Very low
Gabapentin
Best for: Shooting pain, general use
Side effects: Dizziness, balance
Cost: 💲 Low
Duloxetine
Best for: Diabetic neuropathy, mood
Side effects: Nausea, fatigue
Cost: 💲💲 Moderate
Pregabalin
Best for: Pain + anxiety, evidence base
Side effects: Weight gain, drowsiness
Cost: 💲💲💲 Higher
Amitriptyline vs. Gabapentin: A head-to-head study in neuropathy in diabetics found comparable pain relief between the two, with different side effect profiles. Gabapentin tends to cause more dizziness and balance issues; amitriptyline causes more dry mouth and drowsiness. The choice often comes down to which amitriptyline and memory impairment are more acceptable for each individual.
Amitriptyline vs. Duloxetine: Duloxetine is an SNRI that's FDA-approved for diabetic neuropathy — amitriptyline never received a specific FDA indication for neuropathic pain, though it's recommended in every major guideline. Duloxetine may be better tolerated overall and has fewer cardiac concerns, but it's more expensive and may cause nausea.
Amitriptyline vs. Pregabalin (Lyrica): Pregabalin has stronger evidence from larger, better-designed trials, but amitriptyline costs a fraction of the price. Both work for roughly the same proportion of patients. Pregabalin may be preferred when anxiety is also a concern; amitriptyline may be preferred when sleep disturbance is the main issue.
Amitriptyline vs. Nortriptyline: Nortriptyline is actually a metabolite of amitriptyline — your body converts amitriptyline into nortriptyline. Some doctors prescribe nortriptyline directly because it may cause less drowsiness and fewer side effects while retaining most of the pain-relieving properties. If you can't tolerate amitriptyline's side effects, nortriptyline is worth discussing with your doctor.
Important Precautions and Drug Interactions
Amitriptyline is generally safe at the low doses used for pain, but there are important precautions to be aware of:
Talk to Your Doctor
Never stop amitriptyline suddenly — tapering is essential to avoid withdrawal symptoms. Always tell your doctor about ALL medications and supplements you take, especially other antidepressants (SSRIs, SNRIs) and tramadol, due to serotonin syndrome risk.
Age considerations: Amitriptyline is used cautiously in older adults (over 65) because of increased sensitivity to side effects — particularly drowsiness, dizziness, and falls. The American Geriatric Society's Beers Criteria lists amitriptyline as potentially inappropriate for older adults, though many geriatricians still prescribe low doses when the benefits outweigh the risks. If you're over 65, your doctor may start at a very low dose (10 milligrams) and monitor more carefully.
Heart conditions: Because amitriptyline can affect heart rhythm, it should not be taken if you've had a recent heart attack. Your doctor may request an electrocardiogram (ECG) before starting treatment if you have any heart concerns.
Glaucoma: Amitriptyline can increase eye pressure and should be used with caution (or avoided) in people with narrow-angle glaucoma.
Prostate enlargement: The urinary retention side effect can be particularly problematic for men with enlarged prostates.
Drug interactions to know about:
- SSRI antidepressants (fluoxetine, sertraline, paroxetine) — can increase amitriptyline levels and raise serotonin syndrome risk
- SNRI antidepressants (duloxetine, venlafaxine) — similar serotonin concerns
- Tramadol — increased serotonin syndrome risk and lowered seizure threshold
- MAO inhibitors — dangerous combination; should not be taken together
- Alcohol — significantly increases drowsiness and impairment
- Anticholinergic medications — additive effects on dry mouth, constipation, urinary retention
Always provide your doctor with a complete list of your medications, including over-the-counter drugs and supplements. Drug interactions with amitriptyline are manageable when your healthcare team knows the full picture.
Practical Tips for Living with Amitriptyline
Based on years of conversations with people who take amitriptyline for neuropathy, here are practical tips that go beyond what the medication guide tells you:

Time your dose carefully. Most doctors say “take at bedtime,” but many people find that taking it one to two hours before they want to fall asleep works better. This way, the drowsiness peaks right when you're trying to sleep rather than after you've already been lying awake.
Keep water and sugar-free gum handy. Dry mouth is almost universal with amitriptyline. Keeping a water bottle nearby and chewing sugar-free gum throughout the day makes a real difference. Some people also find that biotene mouthwash helps.
Stand up slowly. Orthostatic hypotension (dizziness when standing) is common, especially in the first few weeks. Make it a habit to sit on the edge of the bed for a moment before standing up in the morning.
Monitor your weight. Not everyone gains weight, but keeping an eye on it from the start — and maintaining your usual diet and activity level — can help prevent gradual creep.
Give it a real trial. The biggest mistake I see people make is giving up after a week or two because the pain hasn't improved. Pain relief can take six to eight weeks. If the side effects are manageable, stick with it for the full trial period before making a judgment.
Don't adjust doses on your own. It's tempting to take an extra pill on a bad pain day, but amitriptyline doesn't work as a rescue medication — it builds up in your system over time. Taking extra doses increases side effect risk without providing additional immediate pain relief.
Track your symptoms. Keep a simple daily log of your pain level (1-10), sleep quality, and any side effects. This data is invaluable when discussing dose adjustments with your doctor. It's much more useful than trying to remember how you felt three weeks ago.
Frequently Asked Questions
Does amitriptyline actually heal nerve damage, or does it just mask the pain?
Amitriptyline does not repair damaged nerves. It works by changing how your brain and spinal cord process pain signals from those damaged nerves. Think of it as adjusting the volume rather than fixing the speaker. While it doesn't heal the underlying nerve damage, reducing pain can improve sleep, activity levels, and quality of life — all of which support your body's own nerve repair processes.
Can I take amitriptyline with gabapentin or pregabalin?
Yes, combining amitriptyline with gabapentin or pregabalin is actually a common strategy when a single medication isn't providing enough relief. These drugs work through different mechanisms, so they can complement each other. Your doctor will typically start one medication first, then add the second at a low dose if needed. The main concern is additive drowsiness.
Will amitriptyline make me feel depressed or emotional?
At the low doses used for pain (10-75 milligrams), amitriptyline is unlikely to cause significant mood changes. Some people actually report feeling slightly calmer due to better sleep and reduced pain. However, all medications that affect brain chemistry can occasionally cause unexpected emotional effects — report any mood changes to your doctor.
How long can I stay on amitriptyline?
Many people take amitriptyline for years without problems. Your doctor may periodically suggest a trial reduction to see if you still need it — neuropathic pain can sometimes improve over time, and you may not need the same dose indefinitely. Never reduce or stop without medical guidance.
Is amitriptyline addictive?
No, amitriptyline is not addictive in the way that opioids or benzodiazepines can be. However, your body does adjust to it, which is why stopping suddenly can cause withdrawal symptoms like nausea, headache, and irritability. This is physical dependence, not addiction — an important distinction. Tapering off gradually avoids these issues.
My doctor wants to prescribe an antidepressant for my pain. Should I be concerned?
Not at all. Tricyclic antidepressants like amitriptyline are recommended as first-line treatments for neuropathic pain by every major medical guideline, including the American Academy of Neurology and NICE guidelines. Using them for pain is not off-label guesswork — it's standard evidence-informed practice. The pain-relieving mechanism works independently of the antidepressant effect.
The Bottom Line on Amitriptyline
Amitriptyline is a medication with a track record spanning decades — older than most of the alternatives, cheaper than all of them, and still recommended as a first-line option in every major neuropathic pain guideline. The evidence supporting it isn't as robust as we'd like, but the clinical experience of millions of patients and their doctors tells a story that matters too.

Is it the right choice for you? That depends on your specific type of neuropathy, your other health conditions, the medications you're already taking, and which side effects you're willing to tolerate. The best thing you can do is have an honest conversation with your doctor about the pros and cons — and if they suggest trying it, give it a fair trial of at least six to eight weeks before deciding.
If amitriptyline doesn't work, that's valuable information — not a failure. It means your doctor can move on to other options. And if it does work, you may find yourself sleeping better, hurting less, and getting back to activities that pain had taken from you. Either outcome moves you closer to finding what works for your neuropathy.
Interested in learning about other medication options? Read our guides on gabapentin for neuropathy, duloxetine for neuropathy, and pregabalin for neuropathy. For a broader view of pain management approaches, visit our natural remedies guide.


