
Neuropathy After Surgery: Causes, Recovery, and What to Do
When I had my first surgery years ago, I expected the usual recovery — some soreness, a few weeks of taking it easy, and then back to normal. What I didn't expect was the tingling that started in my hand three days later and didn't stop. It took me weeks to learn that what I was experiencing had a name: post-surgical neuropathy. If you're dealing with nerve pain, numbness, or tingling after a procedure, I want you to know that you're not imagining things — and you're definitely not alone.
Post-surgical neuropathy affects somewhere between ten and fifty percent of surgery patients, depending on the type of procedure. That's a staggering number, and yet many people are caught off guard when it happens to them. In this guide, I'll walk you through what causes nerve damage after surgery, which procedures carry the highest risk, what recovery really looks like, and the treatment options that may actually help.
What Is Post-Surgical Neuropathy?
Post-surgical neuropathy — sometimes called surgically induced neuropathic pain or SNPP — occurs when nerves are damaged, compressed, or irritated during or after a surgical procedure. Your peripheral nerves are like an intricate wiring system that carries signals between your brain and the rest of your body. When those wires get damaged, the signals get scrambled, leading to pain, numbness, tingling, or weakness in the affected area.
According to a review published in the Annals of Medicine and Surgery, chronic neuropathic pain develops in ten to forty percent of patients following surgery. A Mayo Clinic Proceedings review further confirmed that while many cases resolve within weeks to months, some patients develop persistent nerve damage that requires ongoing treatment.
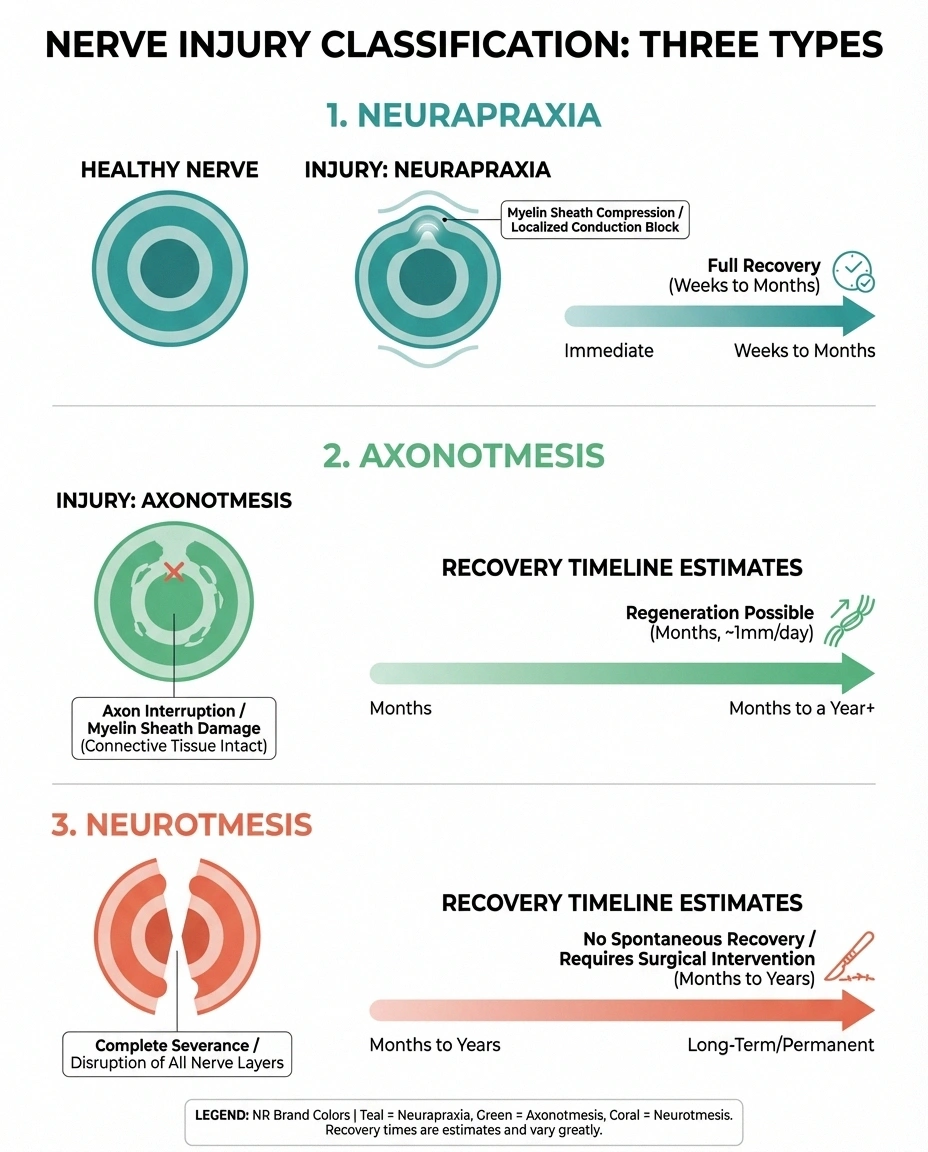
There are three main types of nerve injury that can occur during surgery:
- Neurapraxia — The mildest form, involving damage to the protective myelin sheath around the nerve. Think of it as scuffing the insulation on a wire. Recovery is usually complete within weeks to months.
- Axonotmesis — More significant damage where the nerve fibers themselves are injured, but the surrounding structure remains intact. Recovery is possible but slower, typically at a rate of about one inch per month.
- Neurotmesis — The most severe form, where the nerve is completely severed or torn. This type often requires surgical repair and recovery may be incomplete.
Understanding which type of injury occurred helps your medical team predict your recovery timeline and choose the right treatment approach.
Common Causes of Nerve Damage During Surgery
Nerves can be surprisingly difficult to see during surgery, and their anatomy varies from person to person. Even the most skilled surgeons may inadvertently affect nearby nerves. Here are the most common ways nerve damage happens:
Direct Surgical Trauma
During any procedure that involves cutting, retracting, or manipulating tissue, nerves in the surgical field can be stretched, compressed, or accidentally cut. This is particularly common in surgeries that take place near major nerve pathways, like spinal procedures or joint replacements.
Positioning-Related Nerve Compression
Here's something many people don't realize: nerve damage can occur even in areas far from the surgical site. During lengthy procedures, your body is positioned on the operating table in ways that may compress nerves against hard surfaces. The ulnar nerve at the elbow and the peroneal nerve at the knee are particularly vulnerable. Surgeries lasting longer than three hours carry a significantly higher risk of positioning-related nerve injuries.
Scar Tissue Formation
As your body heals from surgery, scar tissue forms naturally as part of the repair process. But when scar tissue builds up around or near a nerve, it can constrict the nerve — like squeezing a garden hose — reducing the flow of nutrients and chemical signals the nerve needs to function properly. This type of nerve compression can develop weeks or even months after the original procedure.
Inflammation and Immune Response
Research from the University of Oxford published in Brain revealed something surprising: not all post-surgical neuropathies are mechanical. In some cases, the body's immune system appears to attack the nerves in response to the surgical trauma, causing inflammatory neuropathy. These cases may present as pain and weakness that appears days to weeks after surgery, sometimes in locations separate from the surgical site.
Reduced Blood Flow
Nerves require a steady supply of oxygen and nutrients delivered through tiny blood vessels. If surgery disrupts blood flow to an area — through tourniquet use, tissue swelling, or vascular changes — the affected nerves may become ischemic, leading to temporary or permanent dysfunction.
Which Surgeries Carry the Highest Risk?
While any surgery can potentially cause nerve damage, certain procedures are associated with higher rates of post-surgical neuropathy:
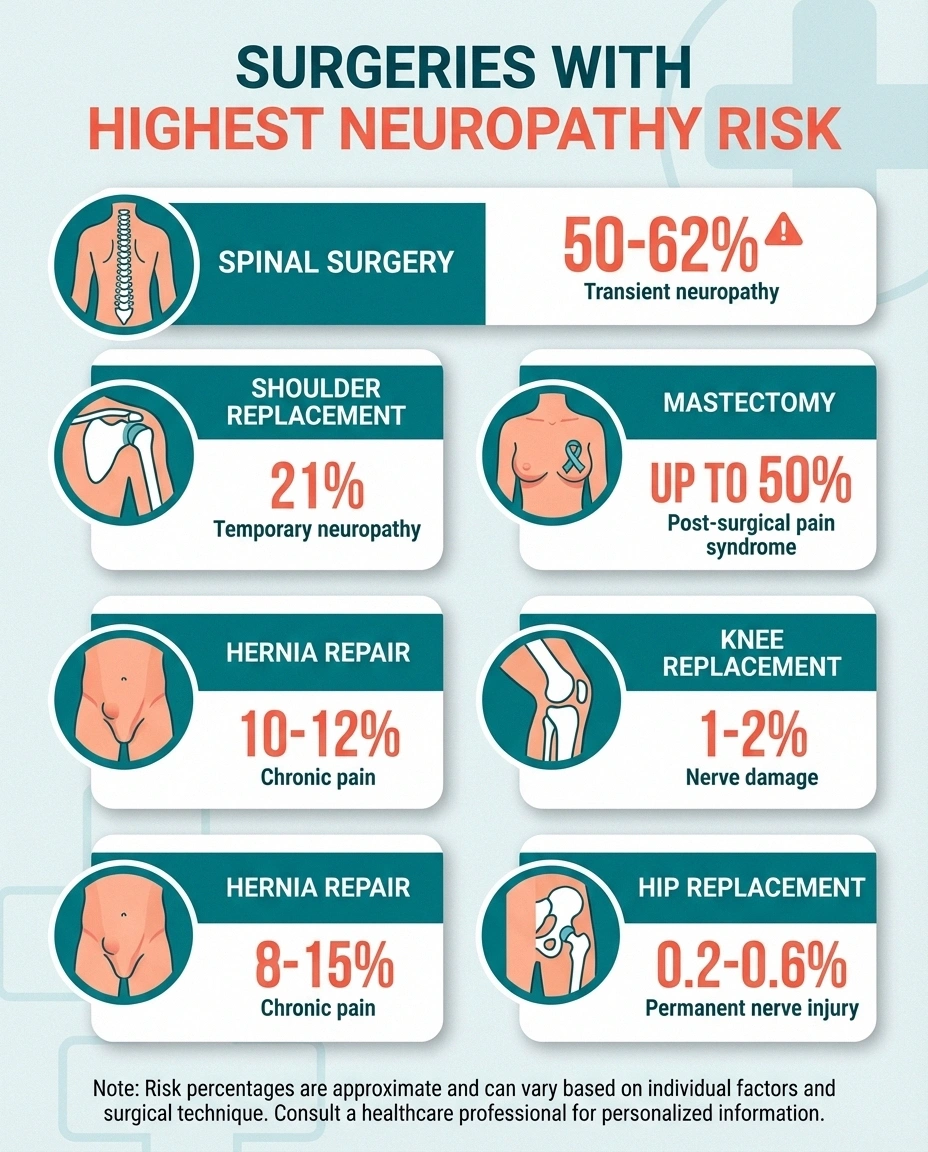
Spinal surgeries — including discectomy, laminectomy, and spinal fusion — carry some of the highest risks. Studies show that transient nerve injury occurs in fifty to sixty-two percent of lumbar fusion patients, though most resolve within three months.
Hip replacement surgery has a reported nerve injury rate of 0.2 to 0.6 percent for permanent damage, with the sciatic and femoral nerves being most vulnerable. The Mayo Clinic review noted that in patients who underwent re-exploration for nerve palsy after hip surgery, only two out of seven achieved complete recovery.
Knee replacement surgery can affect the peroneal nerve, leading to foot drop — difficulty lifting the front part of your foot. This complication occurs in roughly one to two percent of cases.
Shoulder replacement surgery carries a twenty-one percent rate of temporary nerve damage and a two percent rate of permanent damage, often affecting the axillary nerve.
Breast surgery and mastectomy frequently affect the intercostobrachial nerve, leading to numbness, tingling, or chronic pain in the inner arm and chest wall. Some studies report neuropathic pain in up to fifty percent of mastectomy patients.
Hernia repair, particularly inguinal hernia surgery, can damage the ilioinguinal, iliohypogastric, or genitofemoral nerves, causing chronic groin pain in ten to twelve percent of patients.
Other procedures with notable risk include dental and jaw surgery, cardiac surgery (where approximately thirty-eight percent of coronary artery bypass patients experience neuropathy symptoms), cesarean section, and amputation.
Recognizing the Symptoms
Post-surgical neuropathy can manifest differently depending on which nerves are affected and how severely they're injured. Common symptoms include:

- Tingling or “pins and needles” — Often the first sign, this sensation may develop at the surgical site or in seemingly unrelated areas (like your hand after back surgery, which may indicate positioning-related injury).
- Numbness — A loss of sensation that may be partial or complete in the affected area.
- Burning or shooting pain — Sharp, electric-shock-like pain that may come in waves or remain constant.
- Hypersensitivity — Where even light touch or clothing against the skin causes disproportionate pain (allodynia).
- Muscle weakness — Difficulty moving or controlling the muscles served by the damaged nerve.
- Temperature sensitivity — Difficulty sensing hot or cold, or unusual reactions to temperature changes.
It's important to distinguish between normal post-surgical pain — which tends to improve steadily — and neuropathic pain, which may begin after the initial surgical pain subsides, or may persist long after other healing is complete. If your pain changes character (becoming burning, shooting, or electrical) or doesn't improve on the expected timeline, bring it up with your surgeon or talk to your doctor about the possibility of nerve involvement.
Risk Factors: Who Is More Vulnerable?
Certain factors can increase your risk of developing neuropathy after surgery:
- Pre-existing neuropathy — If you already have diabetic neuropathy, small fiber neuropathy, or another nerve condition, your nerves are already compromised and more vulnerable to additional injury.
- Diabetes — Even without existing neuropathy, diabetes impairs nerve healing and increases complication risk.
- Longer surgery duration — Procedures lasting more than three hours significantly increase the risk of positioning-related nerve compression.
- Age — Older adults tend to have slower nerve regeneration and may have undiagnosed subclinical neuropathy.
- Obesity — Excess weight can make nerve visualization more difficult during surgery and may increase positioning pressure on nerves. As we've discussed in our article on neuropathy and weight, obesity independently affects nerve health.
- Autoimmune conditions — Conditions like rheumatoid arthritis or lupus may trigger inflammatory nerve damage after surgical stress.
- Previous surgeries — Prior operations in the same area increase the likelihood of scar tissue affecting nerves.
- Nutritional deficiencies — Low levels of B vitamins, particularly B12, can impair nerve function and recovery.
If you know you have any of these risk factors, discuss them with your surgical team before your procedure. In many cases, extra precautions — like careful positioning, padding, or shorter operative times — can reduce your risk.
How Post-Surgical Neuropathy Is Diagnosed
Getting an accurate diagnosis is the first step toward proper treatment. Your doctor may use several approaches:
Clinical examination — A thorough neurological exam to assess sensation, reflexes, and muscle strength in the affected area. Your doctor will map out exactly where your symptoms occur, which helps identify which nerve is involved.
Electromyography (EMG) and nerve conduction studies — These electrical tests measure how well your nerves are transmitting signals. While highly specific, they have lower sensitivity — meaning they're better at detecting moderate to severe nerve damage than mild cases. If you've had these tests before for other reasons, you can read more in our guide to neuropathy diagnosis.
Ultrasound imaging — High-resolution ultrasound can visualize nerve swelling, constriction, or structural changes. It's less invasive than EMG and works comparably well for many diagnoses.
MR neurography — A specialized MRI technique tuned specifically to visualize nerves. This can reveal inflammation, compression, or structural damage that other imaging may miss.
The timing of diagnostic testing matters. EMG and nerve conduction studies may not show abnormalities until two to three weeks after the nerve injury, so testing too early can produce false-negative results.
Recovery: What to Realistically Expect
I wish I could tell you that every case of post-surgical neuropathy resolves quickly and completely. The reality is more nuanced — but there is genuine reason for hope.
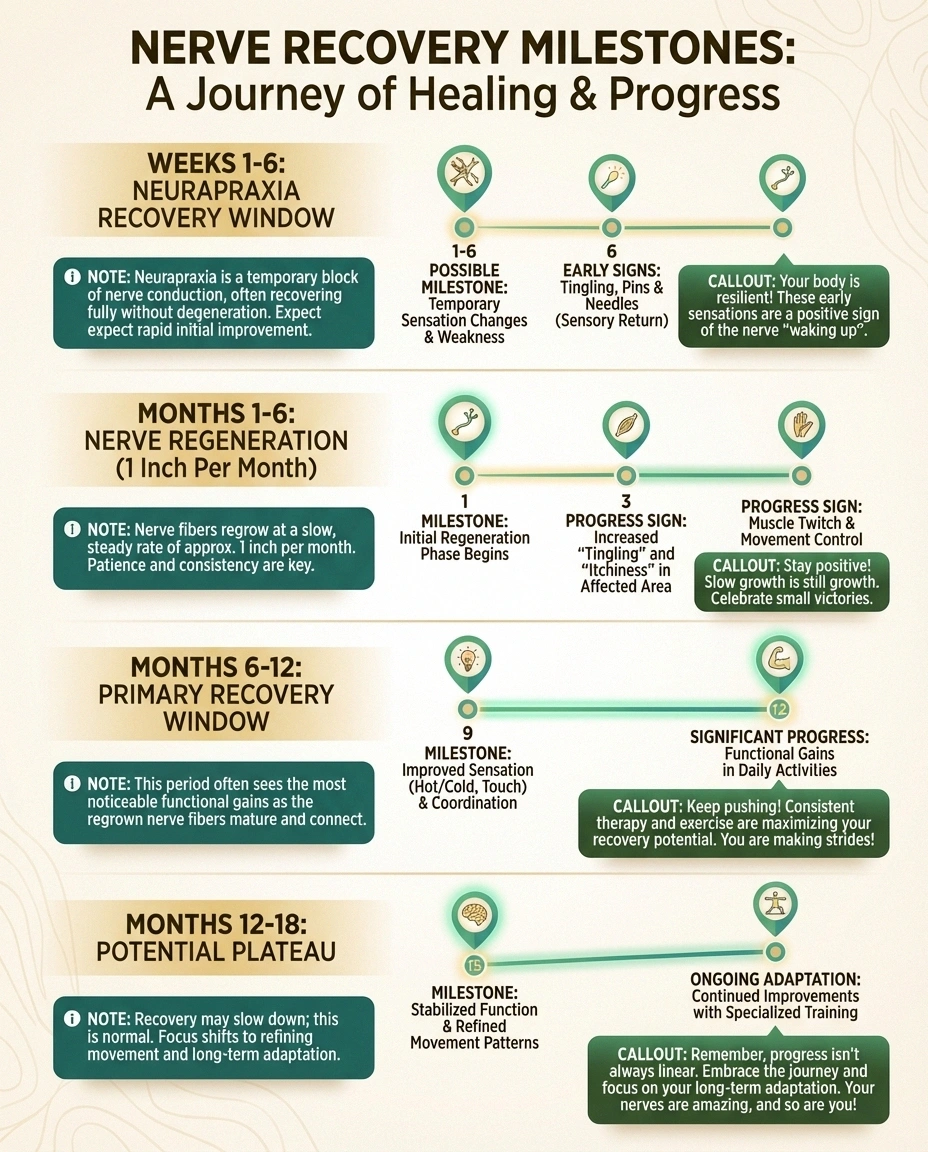
Many cases do resolve on their own. Most episodes of post-surgical nerve damage last a few weeks to a few months. Neurapraxia injuries — where only the myelin sheath is affected — typically recover within six to eight weeks as the nerve's insulation repairs itself.
Nerve regeneration is slow but real. When the nerve fibers themselves are damaged (axonotmesis), nerves regrow at approximately one inch per month. This means a nerve injury in your lower back that needs to regrow to reach your foot could take over a year — sometimes two — before you notice significant improvement. This pace can feel agonizingly slow, but it's important to know that healing may still be occurring even when you can't feel it yet.
Permanent damage is possible but less common. Research suggests that 0.5 to 2 percent of surgery patients develop permanent nerve damage. Neurotmesis injuries, where the nerve is completely severed, carry the poorest prognosis without surgical intervention.
The first six months are critical. Most neurologists consider the first six to twelve months the primary recovery window. If you're showing steady improvement during this period — even if it's gradual — that's a very positive sign. Recovery that plateaus completely after twelve to eighteen months may indicate the limit of natural nerve regeneration.
One thing I've learned from talking with readers is that recovery from nerve damage isn't always linear. You may have good weeks and bad weeks. Some people notice sensation returning in patches rather than evenly. This is normal — nerves don't heal in a straight line.
Treatment Options That May Help
Treatment for post-surgical neuropathy typically involves a combination of approaches, tailored to the severity and type of nerve damage:

Medications for Nerve Pain
Several medication classes may help manage neuropathic pain after surgery:
- Gabapentin (Neurontin) and pregabalin (Lyrica) — These anticonvulsants are considered first-line treatments for neuropathic pain. They work by calming overactive nerve signals.
- Duloxetine (Cymbalta) — This SNRI antidepressant has proven effectiveness for neuropathic pain and may also help with the emotional toll of chronic pain.
- Amitriptyline — A tricyclic antidepressant often used at low doses for nerve pain, particularly when pain disrupts sleep.
- Topical treatments — Capsaicin cream and lidocaine patches can provide targeted relief for localized neuropathic pain without systemic side effects.
- NSAIDs — While less effective for pure neuropathic pain, anti-inflammatories may help when inflammation is contributing to nerve compression.
Your doctor may need to try different medications or combinations before finding what works best for you. Be patient with this process and communicate openly about what's helping and what isn't.
Physical Therapy and Rehabilitation
Physical therapy plays a crucial role in recovery from post-surgical neuropathy. A skilled therapist can design a program that includes gentle nerve gliding exercises to prevent adhesions, progressive strengthening for muscles affected by nerve damage, desensitization techniques for areas with hypersensitivity, and balance training if lower extremity nerves are involved.
Starting physical therapy early — as soon as your surgeon clears you — tends to produce better outcomes than waiting. The goal isn't just pain relief; it's maintaining function and preventing the secondary problems (muscle wasting, joint stiffness, falls) that can develop when nerves aren't working properly.
Nerve Blocks and Injections
Corticosteroid injections near the affected nerve can reduce inflammation and provide temporary pain relief. Nerve blocks — injections of anesthetic directly around the nerve — can help both as treatment and as a diagnostic tool (if a nerve block eliminates your pain, it confirms which nerve is causing the problem).
These aren't permanent solutions, but they can provide meaningful relief while your nerve heals and may allow you to participate more actively in physical therapy.
TENS Units and Neurostimulation
Transcutaneous electrical nerve stimulation (TENS) uses mild electrical currents to interfere with pain signals. For some people with post-surgical neuropathy, TENS provides significant relief — particularly for burning or aching pain. It's non-invasive, has few side effects, and can be used at home.
For severe cases that don't respond to other treatments, peripheral nerve stimulation (an implanted device) may be considered.
Surgical Revision
In cases where a nerve is clearly entrapped by scar tissue or was severed during the original procedure, a second surgery to release the nerve or perform a nerve repair or graft may be warranted. This is typically a last resort, pursued after conservative treatments have been given adequate time and have failed to provide relief.
Complementary Approaches Worth Exploring
Beyond conventional medical treatment, several complementary approaches may support nerve recovery:
Acupuncture has shown promise in several studies for neuropathic pain management. While the evidence is still building, some patients report meaningful improvement in pain and sensation.
Nutritional support is essential for nerve healing. Vitamin B12, ALA for nerve health, and acetyl-L-carnitine have all shown neuroprotective properties in research. While they're not miracle cures, ensuring adequate nutrition gives your nerves the best possible foundation for recovery.
Red light therapy and infrared therapy are emerging treatments that may stimulate cellular repair processes in damaged nerves. Early research is encouraging, though more large-scale studies are needed.
Mind-body techniques — including meditation, cognitive behavioral therapy, and relaxation training — can help manage the emotional impact of chronic nerve pain. The connection between anxiety and pain is well-documented, and breaking that cycle can meaningfully reduce your suffering.
Preparing for Surgery: How to Protect Your Nerves
If you have an upcoming surgery, there are concrete steps you can take to reduce your risk of post-surgical neuropathy:
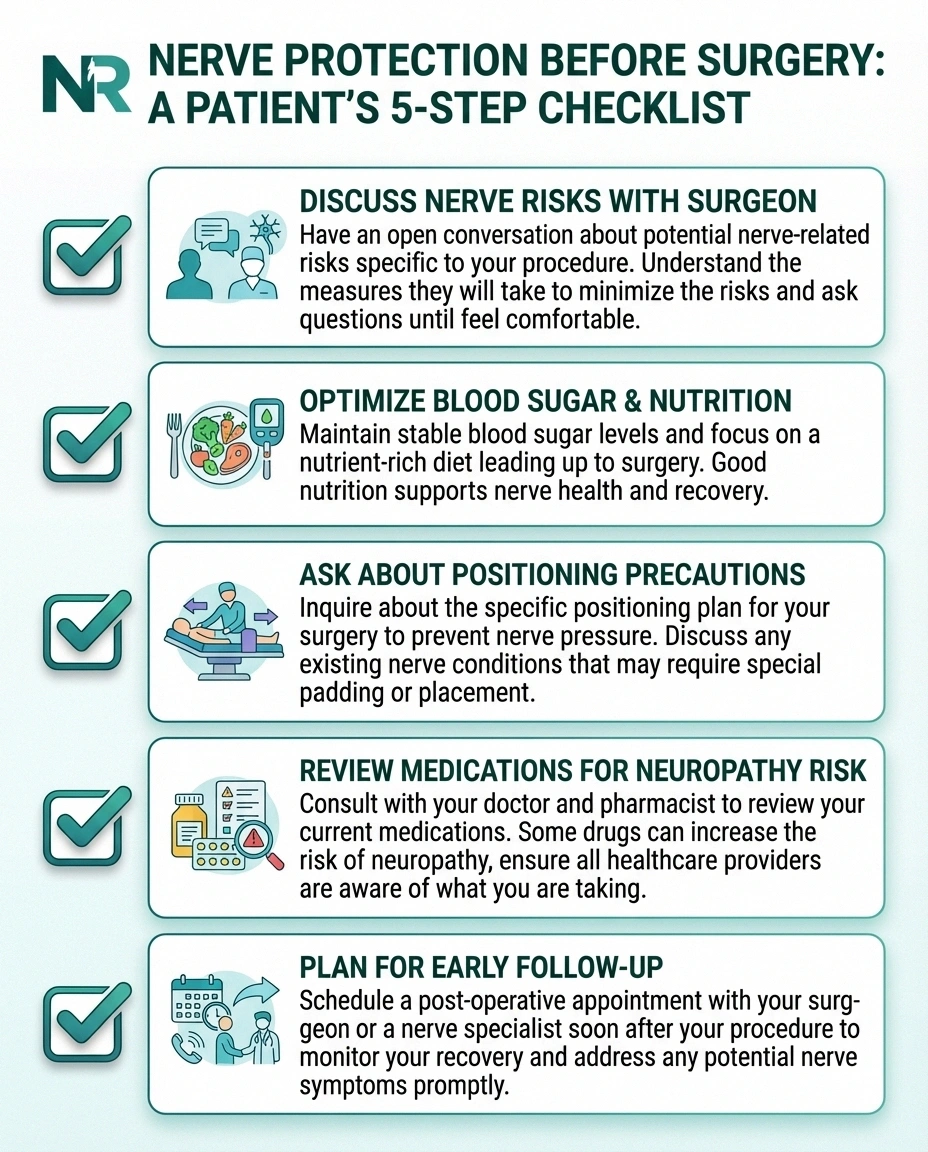
Ask your surgeon specifically about which nerves are at risk during your procedure
Control blood sugar, correct vitamin deficiencies (especially B12), and address nutritional gaps
Discuss padding and positioning precautions with your anesthesiologist, especially for longer procedures
Some medications increase neuropathy risk — review your full list with your doctor
Know the warning signs and have a follow-up appointment scheduled within 2 weeks of surgery
- Talk to your surgical team. Ask specifically about nerve risks associated with your procedure. A surgeon who takes the time to explain these risks is also more likely to take precautions to prevent them.
- Optimize your health beforehand. If you have diabetes, get your blood sugar under the best possible control before surgery. Address any vitamin deficiencies — particularly B12, folate, and vitamin D.
- Discuss positioning. Ask your anesthesiologist about the measures they take to protect nerves during positioning, especially for longer procedures. Proper padding and frequent position checks can prevent compression injuries.
- Consider your medications. Some medications can increase neuropathy risk. Review your full medication list with your doctor before surgery.
- Plan for early intervention. Know the warning signs of nerve damage and have a follow-up plan in place. Early detection and treatment lead to better outcomes.
Living With Post-Surgical Neuropathy: Practical Tips
While you're recovering — and especially if your neuropathy persists — these practical strategies can make daily life more manageable:

Protect numb areas carefully. If you've lost sensation in part of your body, you won't feel injuries, burns, or pressure sores developing. Check these areas visually every day, just as we recommend in our foot care guide.
Address sleep disruption early. Neuropathic pain often worsens at night, creating a vicious cycle where poor sleep increases pain sensitivity. Talk to your doctor about nighttime pain management and practice good sleep hygiene.
Stay as active as safely possible. Gentle movement, walking, and prescribed exercises support nerve recovery and prevent the deconditioning that makes everything harder. Work with your physical therapist to find activities that are safe for your specific situation.
Track your symptoms. Keeping a simple pain journal helps you notice gradual improvements that might otherwise be missed, and provides valuable information for your medical team.
Seek emotional support. Chronic nerve pain can be isolating and demoralizing. Support groups — both in person and online — connect you with people who genuinely understand what you're going through.
When to Seek Urgent Care
While most post-surgical neuropathy develops gradually, certain situations require immediate medical attention:
• Rapidly spreading numbness beyond the surgical area
• Loss of bladder or bowel control (especially after spinal surgery)
• Severe burning pain with skin color/temperature changes (possible CRPS)
• New neurological symptoms combined with signs of infection
- Sudden onset of severe weakness or paralysis in a limb
- Rapid progression of numbness spreading beyond the surgical area
- Loss of bladder or bowel control (which may indicate cauda equina syndrome after spinal surgery)
- Symptoms of complex regional pain syndrome (CRPS) — severe burning pain with skin color changes, temperature changes, and swelling
- Signs of infection at the surgical site combined with new neurological symptoms
These symptoms may indicate complications that need rapid intervention to prevent permanent damage.
Frequently Asked Questions
How long does neuropathy last after surgery?
Most cases of post-surgical neuropathy resolve within a few weeks to a few months. When nerve fibers need to regenerate, recovery occurs at about one inch per month. This means a nerve injury in the hip may take six to twelve months to show significant improvement, while injuries farther from the affected area may take longer. Permanent nerve damage occurs in roughly 0.5 to 2 percent of surgery patients.
Is nerve damage after surgery the surgeon's fault?
Not necessarily. Nerve damage is a recognized risk of many surgical procedures, even when the surgery is performed perfectly. Nerves are small, vary in their exact location from person to person, and may be affected by factors like inflammation and positioning that are difficult to control completely. While surgical error can cause nerve damage, many cases occur despite appropriate surgical technique.
Can post-surgical neuropathy be prevented?
While not all cases can be prevented, risk can be reduced through proper patient positioning during surgery, adequate nerve padding, managing underlying conditions like diabetes before surgery, minimizing surgical duration when possible, and choosing minimally invasive techniques when appropriate. Discussing your risk factors with your surgical team is the most important preventive step.
Should I see a neurologist for nerve pain after surgery?
If your nerve symptoms persist beyond six to eight weeks after surgery, are progressively worsening, or are significantly affecting your daily function, a referral to a neurologist is recommended. Neurologists specialize in diagnosing and treating nerve disorders and can perform targeted diagnostic tests like EMG and nerve conduction studies to assess the extent of damage.
What supplements may help with nerve recovery after surgery?
Several supplements have shown neuroprotective properties in research, including vitamin B12, alpha-lipoic acid, acetyl-L-carnitine, and magnesium. While none are proven cures, they may support the nerve healing process when used alongside conventional treatment. Always discuss supplements with your doctor, especially in the post-surgical period, as some may interact with medications or affect healing.
Does neuropathy after surgery qualify for disability benefits?
If post-surgical neuropathy is severe enough to prevent you from working for twelve months or more, you may qualify for Social Security disability benefits. The key is thorough medical documentation of your nerve damage, functional limitations, and treatment history. Our guide to neuropathy disability benefits provides more detailed information about the application process.
Moving Forward With Hope
Dealing with neuropathy after surgery can feel overwhelming, especially when it wasn't something you anticipated. But here's what I want you to take away from this: most post-surgical neuropathy does improve with time. Nerves are remarkable in their ability to heal and regenerate, even if that process is frustratingly slow.
The most important things you can do are advocate for yourself with your medical team, start treatment early, maintain realistic expectations about the timeline, and take care of your overall health while your nerves heal. Whether your recovery takes weeks or months, every small improvement is a sign that your body is doing its job.
If you're struggling with nerve pain after a procedure, please don't suffer in silence. Talk to your surgeon, ask for a neurology referral, and explore the treatment options available to you. You deserve answers — and relief.


