Browse all our types and causes of neuropathy guides for more articles like this one.
Guillain-Barré syndrome (GBS) is one of the few nerve conditions where speed matters urgently. Unlike many chronic neuropathies that evolve gradually, GBS can worsen over days. That rapid progression is exactly why this condition deserves clear, plain-language education.
If you or someone you love develops quickly spreading weakness, trouble walking, facial weakness, or breathing symptoms after a recent infection, this is not a “wait and see” situation. GBS is rare—but it is a medical emergency when active.
Emergency signal: rapidly worsening weakness, swallowing trouble, or shortness of breath needs immediate hospital evaluation.
What Guillain-Barré Syndrome Is
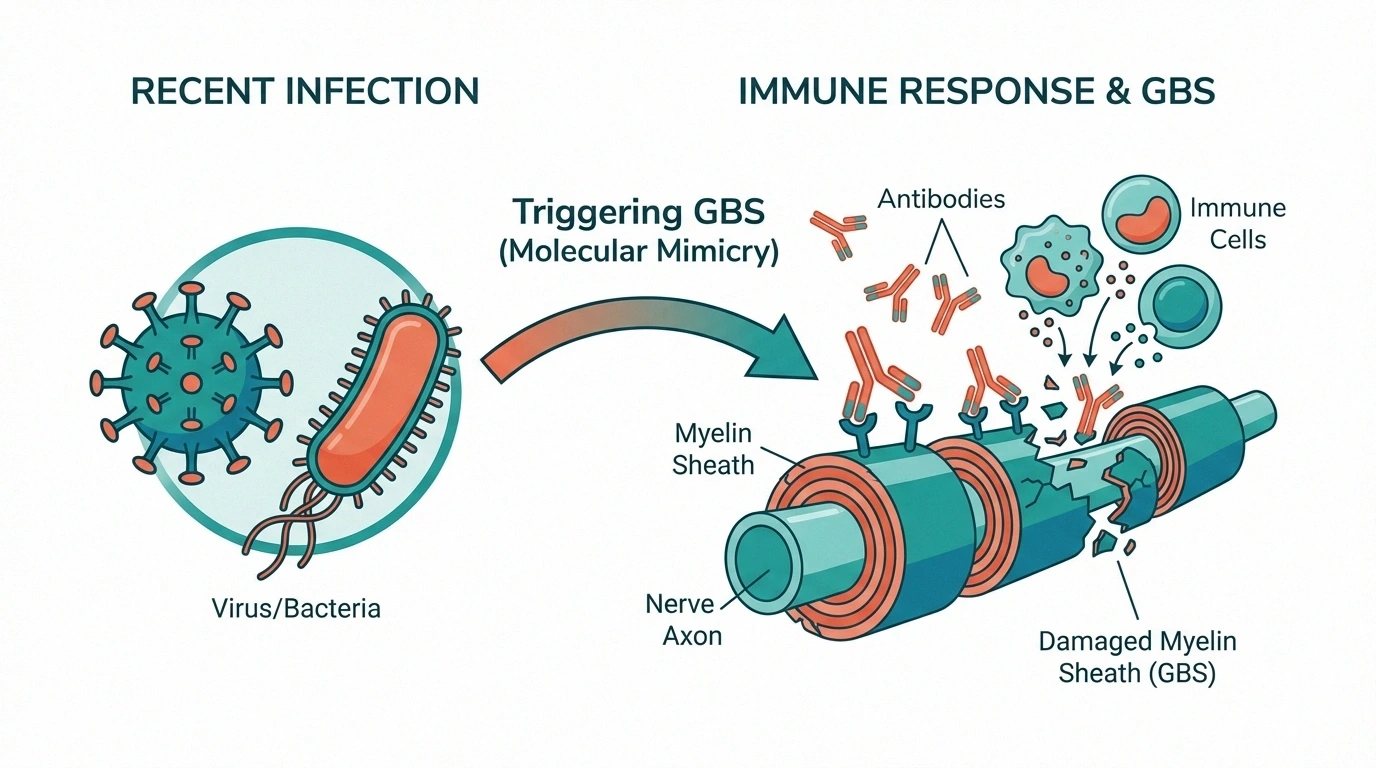
GBS is a rare immune-mediated disorder in which the body mistakenly attacks peripheral nerves. In many cases, symptoms begin after a respiratory or gastrointestinal infection. Mayo Clinic, NINDS, WHO, and NHS all describe this post-infectious pattern and emphasize urgent monitoring in hospital settings.

The exact trigger is not always identifiable in a single person, but known associations include recent viral illness and bacterial gastroenteritis, especially Campylobacter jejuni.
Early Symptoms and How Fast They Can Progress
- Tingling or pins-and-needles in feet/hands
- Weakness that starts in legs and ascends
- Unsteady walking or sudden stair difficulty
- Facial weakness, trouble swallowing, double vision
- Back/leg pain that feels deep, aching, or shooting

Many patients reach peak weakness within about two to three weeks. Some need breathing support. This is why clinicians monitor respiratory function, heart rate, and blood pressure closely in the acute phase.
How GBS Differs From Typical Chronic Neuropathy
People often ask if GBS is “just another neuropathy.” It is not. GBS is usually acute and potentially life-threatening during the active phase. Chronic neuropathies (for example diabetic neuropathy or small fiber neuropathy) often progress more slowly and are managed in outpatient settings.
Hospital Treatment: What Happens and Why
There is no instant cure, but early treatment may shorten or soften the course. The two main immune therapies are:

- IVIG (intravenous immunoglobulin): often first-line in many hospitals
- Plasma exchange (plasmapheresis): removes circulating antibodies
Supportive care is equally critical: breathing support when needed, clot prevention, heart rhythm/blood pressure monitoring, nutrition, pain control, and early rehabilitation planning.
Recovery Timeline: Realistic Expectations
Recovery is often measured in months, not days. Many people improve significantly and may regain independent walking within months, but some continue to experience weakness, fatigue, tingling, or pain for longer. The path is rarely perfectly linear.
- Early rehab helps maintain range of motion and reduce deconditioning
- Physical and occupational therapy support mobility and daily function
- Emotional support matters: abrupt disability can be psychologically intense
- Follow-up is important because a small subset can relapse
Family Caregiver Checklist for the ER
- Bring a current medication list and allergy information
- Note exact time symptoms started and how quickly they spread
- Report any recent infection, diarrhea, flu-like illness, or surgery
- Tell staff immediately if breathing/swallowing worsens
- Ask who the neurology lead is and how respiratory status is being tracked
Related Reading on NeuropathyResource
- Neuropathy Diagnosis: Tests Your Doctor May Order
- Autonomic Neuropathy
- SFN diagnosis and treatment
- Neuropathy and Mental Health
What Triggers GBS After Infection?
Researchers describe GBS as an immune misfire. After an infection, parts of the immune response may mistakenly target components of peripheral nerves. Depending on subtype, damage may involve myelin, axons, or both. That is why symptoms can involve both weakness and sensory changes.
Not everyone who gets a viral illness or stomach bug develops GBS. In fact, GBS remains uncommon. But because progression can be rapid when it occurs, clinicians prioritize early recognition over trying to predict who “should” get it.
Understanding ICU Monitoring Without Panic
Families often feel frightened when they hear “ICU,” but ICU care in GBS is often proactive monitoring, not always catastrophic decline. The team watches breathing strength, oxygenation, heart rhythm, blood pressure variability, swallowing safety, and clot risk. These checks allow fast response if function changes.
- Frequent respiratory checks help decide whether breathing support is needed.
- Cardiac and blood pressure monitoring catches autonomic instability early.
- Swallowing and nutrition assessments reduce aspiration risk.
- Positioning, skin care, and clot prevention reduce secondary complications.
Knowing the purpose of each monitor can reduce fear and help families ask better questions during rounds.
Questions to Ask the Hospital Team
- How is breathing strength being measured today?
- What signs would trigger escalation of respiratory support?
- Which GBS subtype seems most likely right now?
- When did immunotherapy start, and how will response be tracked?
- What is the early rehab plan while still in hospital?
- What discharge criteria should we expect?
Write answers down. In high-stress hospital periods, memory is unreliable, and notes help families stay aligned.
Recovery Phases: What Patients Often Experience
Plateau Phase
Symptoms may stop worsening before clear strength gains appear. This waiting phase can be emotionally difficult.

Early Recovery
Small gains emerge first: improved sitting tolerance, better transfers, stronger breathing, or reduced autonomic swings.
Functional Rebuilding
Rehab shifts toward walking, balance, hand function, and endurance. Fatigue management becomes central.
Long-Tail Recovery
Some symptoms may linger, including neuropathic pain, reduced stamina, or sensory changes. Progress can continue beyond the first year for some people.
Complications to Watch During and After Acute Care
- Breathing compromise
- Autonomic instability (blood pressure or rhythm swings)
- Blood clots from immobility
- Infections related to hospitalization
- Persistent pain and severe fatigue
- Mood symptoms after sudden disability
Most people and families are not prepared for the emotional aftershock of acute neurologic illness. Depression, anxiety, and adjustment stress are common and treatable. Asking for psychological support is part of good neurologic recovery—not a sign of weakness.
Returning Home: A Practical Transition Plan
Discharge planning should include more than a date. Before leaving hospital or rehab, confirm equipment needs, follow-up appointments, medication instructions, and emergency return criteria.

- Clarify home equipment needs (walker, transfer aids, shower support)
- Confirm PT/OT schedule and transportation plan
- Get written red flags for emergency return
- Plan caregiver coverage for the first 1-2 weeks
- Set realistic activity pacing to avoid post-discharge crashes
Recovery tends to improve when transitions are structured. If discharge instructions feel unclear, ask the team to review them in plain language before you leave.
Life After Acute GBS: Building a Recovery Routine
After discharge, many people expect steady daily improvement. Recovery is usually less linear. Good weeks and frustrating weeks can alternate. This is common and does not always mean treatment failed. A structured routine can help you recover function while avoiding overexertion.
- Set baseline first: identify your current safe activity level before increasing anything.
- Progress gradually: small increases in walking or therapy intensity often outperform aggressive jumps.
- Protect sleep: sleep disruption worsens pain, fatigue, and concentration.
- Use energy budgeting: spread demanding tasks through the day with planned recovery breaks.
- Track warning signs: new weakness, breathing change, or autonomic symptoms should prompt rapid reassessment.
Many people also experience fear of relapse. That anxiety is understandable after a sudden severe illness. Discuss clear return precautions with your neurology team so you know exactly what requires urgent care and what can wait for outpatient follow-up. Clarity reduces panic and improves confidence.
If mood symptoms, trauma responses, or sleep anxiety persist, ask for mental health support. Psychological recovery is part of neurologic recovery, not a separate problem. Families often need support too, especially after ICU-level care.
With coordinated care, many patients recover substantial independence. The timeline varies, but progress remains possible long after hospital discharge, especially when rehab and follow-up are consistent.
FAQ
How quickly should I seek emergency care?
Immediately if weakness is spreading, breathing is harder, swallowing is affected, or facial weakness appears.
Can GBS start after a stomach bug or flu?
Yes. Many cases occur after a recent respiratory or gastrointestinal infection.
Is Guillain-Barré syndrome permanent?
Not usually permanent in full, but some people have lasting symptoms such as fatigue, weakness, or pain.
What does recovery usually look like?
Recovery often unfolds over months with rehabilitation, close follow-up, and gradual functional gains.
Can children get GBS?
Yes, although GBS is more common in adults. Any child with rapidly worsening weakness needs urgent evaluation.
Can GBS return after recovery?
A relapse can happen in a minority of patients, which is why continued medical follow-up is important.
Takeaway
Guillain-Barré syndrome is rare, serious, and treatable—but only if recognized quickly. If symptoms are progressing fast, seek emergency care first and sort details later. For ongoing recovery, partner with your clinical team and rehab providers. This article is educational and does not replace personal medical advice from your doctor.