
The first time someone offered me laser therapy for my neuropathy, I almost laughed. I pictured science-fiction beams or a tanning-bed sized contraption. What I got instead was a small device that emitted what looked like an ordinary red light, held against the soles of my feet for about fifteen minutes. There was no heat. There was no sensation at all. The clinician told me it was “photobiomodulation,” and that we should expect to need a series of sessions before knowing whether it was helping.
I was skeptical and curious in equal measure. Skeptical because chronic-illness patients hear a lot of “miracle” claims. Curious because the practitioner wasn't promising miracles — she was honest about mixed evidence and reasonable expectations. By the end of the series, I had a real opinion about photobiomodulation. It is not a cure. It is a legitimate, low-risk option that helps some people meaningfully. And it costs enough that you should know what you're getting into.
I'm Janet Ellis, and this is my honest evidence-balanced explainer of photobiomodulation therapy for neuropathy — what it is, what the science actually shows, and what to ask before paying for a series.
What Photobiomodulation Therapy Actually Is

Photobiomodulation therapy, abbreviated PBMT, is the modern name for what most patients still know as low-level laser therapy or LLLT. You may also see it called “cold laser therapy,” because unlike a surgical laser, it doesn't generate heat that damages tissue. The “cold” name is colloquial; “low-level” is the technical version.
Three Names, One Therapy
PBMT, LLLT, and “cold laser” are three names for the same thing — red and near-infrared light (600–1064 nm) applied to skin to stimulate mitochondrial function in stressed nerves. Not a cure. Real, low-risk, evidence-mixed-but-favorable.
The therapy uses red or near-infrared light at specific wavelengths — typically in the 600 to 1064 nanometer range — applied to the skin over a painful or damaged area. The light penetrates the skin and reaches the deeper tissues where nerves, blood vessels, and muscle live. The patient feels nothing or, occasionally, a mild warmth at higher power. Sessions usually run 5 to 30 minutes per area treated, and a typical course is somewhere between 8 and 20 sessions over four to eight weeks.
Three names for the same thing — PBMT, LLLT, cold laser therapy — and a handful of related products you may have seen advertised. Devices marketed as “red light therapy” panels, “infrared therapy” wraps, and clinical “cold laser” units all sit on the same spectrum. They differ mainly in power output, beam coherence, and whether they're intended for clinic or home use.
How It Is Supposed to Work
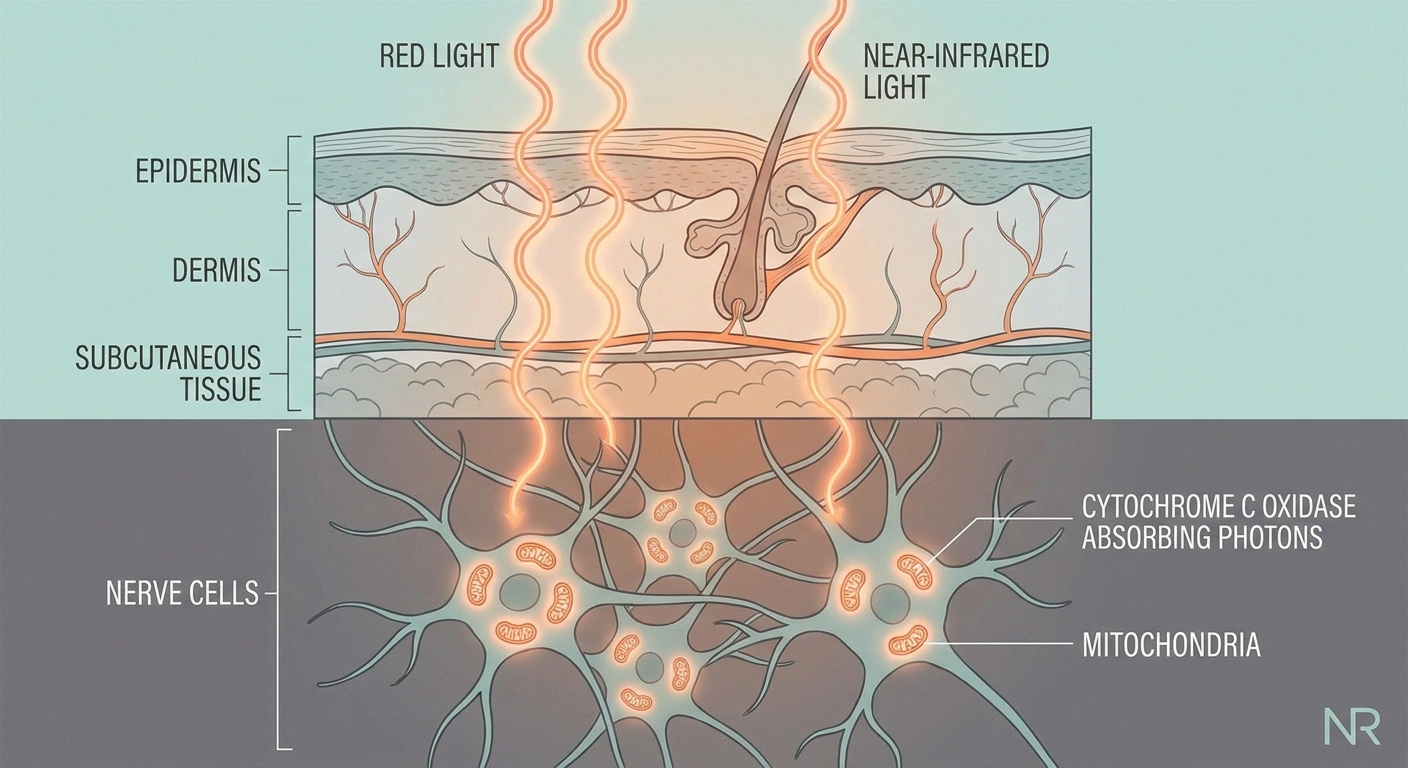
The mechanism, as best researchers understand it, sits at the cellular level. Mitochondria — the energy factories inside every cell — contain a molecule called cytochrome c oxidase that absorbs red and near-infrared light particularly well. When that molecule absorbs the light, it releases nitric oxide and ramps up ATP production, which is the cell's energy currency.
For damaged or stressed nerve cells, this matters because mitochondrial dysfunction is part of the problem. Neuropathy involves reduced energy availability in nerve cells, increased oxidative stress, and inflammation. The proposed mechanism for photobiomodulation: boost cellular energy production, reduce oxidative stress, dampen inflammation, and create conditions where nerves can repair or function better.
The 2025 review in Frontiers in Photonics summarized the proposed mechanisms as enhancing mitochondrial function, reducing oxidative stress, modulating inflammation, and supporting neural repair. That's the theoretical framework. Whether it translates to clinical benefit is the harder question.
What the Evidence Actually Shows
Honest answer: mixed but trending favorable.
The 2025 Frontiers in Photonics review describes photobiomodulation as a “promising non-pharmacological strategy” for neuropathic pain, while flagging protocol heterogeneity as the main barrier to larger conclusions.
Translation: there's real signal, especially in diabetic neuropathy — but no one can yet say “this exact dose works for everyone.”
The picture is messier than supporters make it sound and more promising than skeptics make it sound. Here's the state of play.
A 2017 systematic review found limited evidence for short-term improvement in tactile sensitivity in diabetic peripheral neuropathy patients, but did not find strong evidence for pain reduction. The review concluded that the available studies were small and methodologically inconsistent.
A 2019 review reached a more positive conclusion, finding that photobiomodulation was associated with reductions in neuropathic pain across multiple studies. The studies it pooled were small, and the protocols varied widely.
The 2025 Frontiers in Photonics review described photobiomodulation as a “promising non-pharmacological strategy” for neuropathic pain, while explicitly noting the heterogeneity of protocols and the need for larger trials.
A 2024 systematic review and meta-analysis protocol published in PLOS ONE acknowledged that despite preliminary positive findings, the existing literature lacks substantial evidence regarding safety and effectiveness specifically for diabetes-related peripheral neuropathy.
Several recent randomized controlled trials in diabetic peripheral neuropathy have shown improvements in symptoms, sensation, and quality-of-life scores compared to sham treatment. The samples are typically small (20 to 60 patients), and the duration of follow-up tends to be limited.
The honest takeaway: the evidence base shows real signal, particularly in diabetic peripheral neuropathy, but the studies are too varied in dose, wavelength, and protocol for anyone to say with confidence “this is the dose that works.” Patients respond differently, and the practitioners with the longest experience can usually tell within four to six sessions whether you're a responder.
Who Tends to Respond
Not everyone benefits, and the studies that have looked at predictors of response give some useful clues.
Who Tends to Respond Best
Diabetic peripheral neuropathy patients have the most evidence behind them. The dominant population in the existing research is people with diabetic neuropathy, and that's where the trials show the most consistent benefit.
Earlier-stage neuropathy responds better than late-stage. If you're in the burning-tingling-numbness phase but still have some sensation, photobiomodulation has more to work with than if you're at advanced stages with significant nerve loss. The therapy doesn't regenerate dead nerves — it appears to support stressed-but-living nerves.
People with underlying inflammatory drivers — autoimmune neuropathies, post-surgical nerve pain, chemo-induced symptoms — sometimes respond well because the anti-inflammatory mechanism is part of what photobiomodulation does.
People with significant comorbidities (severe vascular disease, untreated diabetes, end-stage renal disease) often respond less well because the underlying drivers are overwhelming the modest cellular benefit.
None of these are absolute. The honest answer for most patients curious about it is to talk to a practitioner, plan a defined trial of sessions, and reassess.
Clinic Sessions vs. Home Devices


This is the question I get most often. Both paths are legitimate. They serve different needs.
Clinic vs Home Device — Cost & Tradeoffs
Course: 8–20 sessions
Total: ~$300–$2,000
Pro: Higher-power devices, professional protocol
Con: Travel, scheduling, ongoing cost
Use: Daily, indefinitely
Pro: No travel, long-term cost-effective
Con: Lower power, easy to skip, quality varies
Many patients trial in clinic first to confirm response, then buy a home device for maintenance.
Clinic sessions are the traditional path. A trained practitioner — typically a chiropractor, podiatrist, physical therapist, or pain-management specialist — uses a higher-powered, FDA-cleared device on you for a defined session. Sessions run anywhere from $30 to $100 each, depending on region and provider. Most insurance does not cover this for neuropathy. A typical course is 8 to 20 sessions, putting the total cost in the $300 to $2,000 range.
Pros of the clinic path: higher-power devices that may produce stronger effects per session, professional adjustment of dose and protocol, the discipline of going to appointments, no upfront device cost.
Cons: time-consuming, often expensive, transportation each visit, and you stop benefiting the moment you stop going.
Home devices are the alternative. FDA-cleared red light therapy panels and wraps designed specifically for neuropathy run from about $200 (small spot-treatment devices) to $3,000 or more (full-body panels and high-power units). Once owned, daily or near-daily use is possible. Many patients find this is the practical path because compliance becomes easier and the cost amortizes.
Pros of home devices: convenience, daily access, long-term cost-effectiveness if you respond, no scheduling.
Cons: upfront purchase risk if you don't respond, less powerful per session than clinical units, no professional protocol adjustment, the temptation to use too little or too much because no one is metering it.
A middle path some patients take: a short clinic series (4-6 sessions) to assess whether you're a responder, and if you are, transition to a home device for ongoing use. This caps the upfront risk on the home device.
What to Ask Before You Commit
Whether you're considering a clinic or a device, the questions to ask before spending money are similar. I have a list I now run through every time I'm considering a new therapy, and these are the photobiomodulation-specific items.
6 Questions Before You Pay
- What wavelength does your device use? (650 nm and 808 nm are common; the practitioner should know.)
- What's the power output? (Higher class lasers penetrate deeper; ask in milliwatts.)
- How many sessions before we evaluate? (Reasonable answer: 6–8.)
- What does success look like to you? (Listen for honest, modest goals — not “cure.”)
- What's the package cost vs. pay-as-you-go? (Don't prepay 20 sessions on day 1.)
- What happens if I don't respond? (Refund policy, off-ramp, alternative options.)
What wavelength does the device use? 808 to 905 nm and 1064 nm are the most-studied wavelengths for deep-tissue penetration in neuropathy. Devices that only emit visible red (around 630-660 nm) penetrate less deeply and are better suited to skin-level conditions than to nerves.
What is the power output, and how is dose calculated? Therapeutic dose is measured in joules per square centimeter (J/cm²). Studies that show benefit in neuropathy typically deliver between 4 and 60 J/cm² per session. A practitioner who can answer this clearly is one who actually knows what they're doing. Vague answers are a yellow flag.
How many sessions before we'll know if it's working? The honest answer is 6 to 8 sessions for most patients. If a clinic tells you to commit to 20 sessions upfront, with no checkpoint, that's a sales pressure tactic, not a clinical protocol.
What's the FDA clearance status of this device? FDA-cleared (510(k)) is the bare minimum bar — it means the device has been reviewed for safety. Clinical-grade devices and home devices alike should be FDA-cleared. Devices imported from overseas with no FDA clearance are a stay-away.
What does success look like, specifically? A practitioner should articulate measurable goals — pain score reduction, sensation improvement, fewer flare days, longer walking tolerance — not vague “feel better” promises. If the goals aren't specific, it's hard to know whether the money was worth it.
What if I don't respond? Reasonable practitioners offer a checkpoint at session 6 or 8 and will tell you if you're not responding. Reasonable home device companies have return policies in the 60-90 day range so you can test before committing.
Side Effects and Safety

Photobiomodulation is one of the safer modalities in the neuropathy treatment landscape. The reported side effects are minor and infrequent: mild warmth or tingling during treatment, transient redness over the treated area, occasional fatigue after the first few sessions as the body responds.
Never look directly into a therapeutic laser, and always wear the protective goggles a clinic provides. Home devices should come with eye protection — if yours doesn't, buy a pair rated for the wavelength before using it. The eye is the only organ that can be permanently damaged by these devices.
The genuine cautions are short and worth knowing.
Don't shine the light into your eyes. Direct exposure to red and near-infrared light at therapeutic doses can damage the retina. All FDA-cleared devices come with goggles or screening that you should use.
Don't use over active cancer. The mitochondrial-energy-boosting mechanism that helps stressed nerves is the same mechanism that may stimulate cancer cells. Until the research is clearer on cancer safety, photobiomodulation over a known tumor or in an area of active malignancy is not recommended. Chemo-induced neuropathy patients in active cancer treatment should clear photobiomodulation with their oncologist first.
Avoid use over pregnant abdomens. The data on photobiomodulation during pregnancy is sparse, and conservative practice avoids it.
Pacemakers and implanted devices. Generally fine to use over other body areas, but ask your cardiologist before use directly over an implant.
Photosensitizing medications. Some medications (certain antibiotics, retinoids, anti-arrhythmics) increase skin sensitivity to light. If you take any of these, ask your prescriber before starting photobiomodulation.
Outside of those scenarios, the risk profile is genuinely low — substantially lower than most pharmacological interventions for neuropathy.
How to Start a Trial
If you've decided to try photobiomodulation, here's the framework I'd recommend, based on what I see actually work for patients.
A 5-Step Trial Framework
Step 1: Define your baseline. Before the first session, write down where your symptoms are. A pain score (0-10) for an average day. The hours of comfortable walking you have before symptoms ramp up. The number of flare days in a recent week. Sleep quality. Keeping a brief symptom diary makes this easier and gives you a baseline to compare against.
Step 2: Commit to a defined trial. Most clinicians and most home-device protocols suggest 8 to 12 sessions before declaring whether you're a responder. Don't bail at session 3. Don't keep paying past session 12 if there's been no change.
Step 3: Reassess at session 8. Look at your baseline numbers. Are pain scores down by at least 20%? Has walking tolerance improved? Are you sleeping better? If you see meaningful change, continue. If you see no change, the modality probably isn't going to help you, and that's information worth having.
Step 4: If responding, plan for maintenance. Patients who respond often need ongoing maintenance — anywhere from twice a week to twice a month, depending on response durability. This is where home devices often become the practical answer, because daily access at modest cost is cheaper than ongoing clinic visits.
Step 5: Combine with foundational care. Photobiomodulation is one modality among several. It works alongside other natural approaches and any prescribed medications. The patients who do best treat it as one tool in a multi-modal plan, not as a stand-alone solution.
What I Wish Someone Had Told Me
A few practical lessons that took me longer than they should have to learn.
The first response often comes between sessions 4 and 7, not session 1. Patients who expect immediate results sometimes give up before the therapy has had a chance to work. The cellular changes take time to accumulate.
Soreness and tingling shifts are normal. Some patients notice their symptoms briefly intensify or change in quality during the first few sessions before improving. This is uncomfortable but not concerning unless severe.
The placebo effect is real, and it isn't bad. A 30% placebo response is typical in pain studies. If you're getting relief, you're getting relief — the mechanism matters less than the outcome at the daily-living level.
Track honestly. Patients who keep a brief symptom diary are better positioned to make rational continue-or-stop decisions. Patients who go on memory alone often misremember and either over- or under-credit the therapy.
Don't expect it to substitute for blood-sugar control. If diabetic neuropathy is on the table, the foundation is glycemic control. Photobiomodulation supports stressed nerves, but if the underlying glucose damage continues, the therapy is fighting a losing battle.
Frequently Asked Questions
Does cold laser therapy actually work for neuropathy?
The evidence is mixed but increasingly favorable. Multiple studies — particularly in diabetic peripheral neuropathy — have shown reductions in pain, improvements in sensation, and better quality-of-life scores compared to sham treatment. The studies are small, the protocols vary, and not everyone responds. Reasonable estimates suggest somewhere between 40% and 60% of patients see meaningful benefit. That's a real signal but not a cure-all.
How long does it take for laser therapy to work for neuropathy?
Most patients who respond start to see changes between sessions 4 and 7. Full benefit, when it appears, typically emerges over 8 to 12 sessions across four to eight weeks. Patients who notice no change at all by session 8 are probably not going to respond meaningfully and may want to redirect their resources elsewhere.
Is photobiomodulation FDA approved?
“FDA approved” is a higher bar than what these devices have. Most photobiomodulation devices for pain and tissue treatment are FDA-cleared under the 510(k) pathway, which means they have been reviewed for safety and substantial equivalence to existing devices. Specific neuropathy claims are not all approved by the FDA. The devices are legal to sell and prescribe; the specific neuropathy benefit is a clinical use, not a labeled indication for most products.
What are the side effects of laser therapy for neuropathy?
Side effects are uncommon and usually mild: temporary warmth or tingling during sessions, brief redness in the treated area, occasional fatigue after the first sessions. Eye exposure is the main genuine risk and is prevented with the goggles or shielding included with all professional devices. Photobiomodulation should not be used over active cancers, over pregnant abdomens, or by patients on photosensitizing medications without medical clearance.
How much does laser therapy for neuropathy cost?
Clinic sessions typically run $30 to $100 each, with a course of 8 to 20 sessions putting total cost between $300 and $2,000. Most insurance does not cover this for neuropathy. Home FDA-cleared devices range from about $200 for small spot-treatment units to $3,000 or more for full-body panels. Many patients combine a short clinic series to confirm response with a home device for ongoing maintenance.
Can I use red light therapy at home for neuropathy?
Yes. FDA-cleared home red light and near-infrared devices are widely available and many are specifically designed for neuropathy applications. The key parameters to look for are wavelength (808-905 nm or 1064 nm penetrates deepest), power output, FDA clearance, and a reasonable return policy in the 60-90 day range so you can test response before committing fully. Match the device to the body area you need to treat — a hand-sized panel won't cover both feet effectively.
Is photobiomodulation the same as red light therapy?
Photobiomodulation is the umbrella term that includes red light therapy, near-infrared therapy, and low-level laser therapy. They all use light in similar wavelength bands at non-thermal doses to produce the same proposed cellular effects. The differences are mostly in beam coherence (laser vs LED), power, wavelength specifics, and intended use case. For most patient applications, the practical effect is similar; the marketing terms differ.
How is this different from a heating pad?
A heating pad delivers heat, which dilates blood vessels and can temporarily reduce stiffness and pain. The benefit is real but mostly mechanical and short-lived. Photobiomodulation delivers specific wavelengths of light that act at the cellular level — boosting mitochondrial function and modulating inflammation — without heat being the primary mechanism. The two can complement each other but they work through different pathways and are not substitutes for one another.


