
Sciatica vs. Neuropathy: How to Tell the Difference
When shooting pain travels down your leg or a burning sensation won't leave your feet, the first question is always the same: what's causing this? I hear from readers every week who are caught between two possible explanations — sciatica and peripheral neuropathy. Both involve nerve pain, both can make daily life miserable, and both can leave you wondering if you'll ever feel normal again.
Here's what I've learned after years of researching nerve conditions and hearing from thousands of people in our community: the distinction between sciatica and neuropathy matters enormously, because the treatments that help one condition may do nothing — or even worsen — the other. Getting the right answer early can save you months of frustration and unnecessary suffering.
In this guide, I'll walk you through the key differences, help you understand what each condition actually is, and give you practical tools for having a more productive conversation with your doctor.
What Is Sciatica?
Sciatica isn't technically a diagnosis — it's a description of symptoms caused by irritation or compression of the sciatic nerve. The sciatic nerve is the largest nerve in the human body, running from your lower back through your hips and buttocks, then branching down each leg.
When something presses on or irritates this nerve — a herniated disc, bone spur, or narrowing of the spinal canal (spinal stenosis) — the result is pain that radiates along the nerve's path. Most people describe sciatica as a sharp, shooting, or electric-shock sensation that starts in the lower back or buttock and travels down the back of one leg.
Key characteristics of sciatica include:
- One-sided pain — sciatica almost always affects just one leg
- Pain that changes with position — sitting, bending, or coughing may make it worse, while walking or lying down may provide relief
- A clear path of pain — the discomfort follows a predictable route from the lower back down through the hip and leg
- Sudden onset — many people can pinpoint when sciatica started (after lifting something heavy, a fall, or a sudden movement)
- Morning stiffness — symptoms are often worst when first getting out of bed
According to the Penn Medicine database, sciatica is most common in people between the ages of 35 and 55, though it can affect anyone. The good news is that most cases of sciatica resolve on their own within several weeks to months with conservative treatment.
What Is Peripheral Neuropathy?
Peripheral neuropathy is fundamentally different. Rather than a single nerve being compressed, neuropathy involves actual damage to the peripheral nerves themselves — the vast network of nerves that carry signals between your brain and spinal cord and the rest of your body.
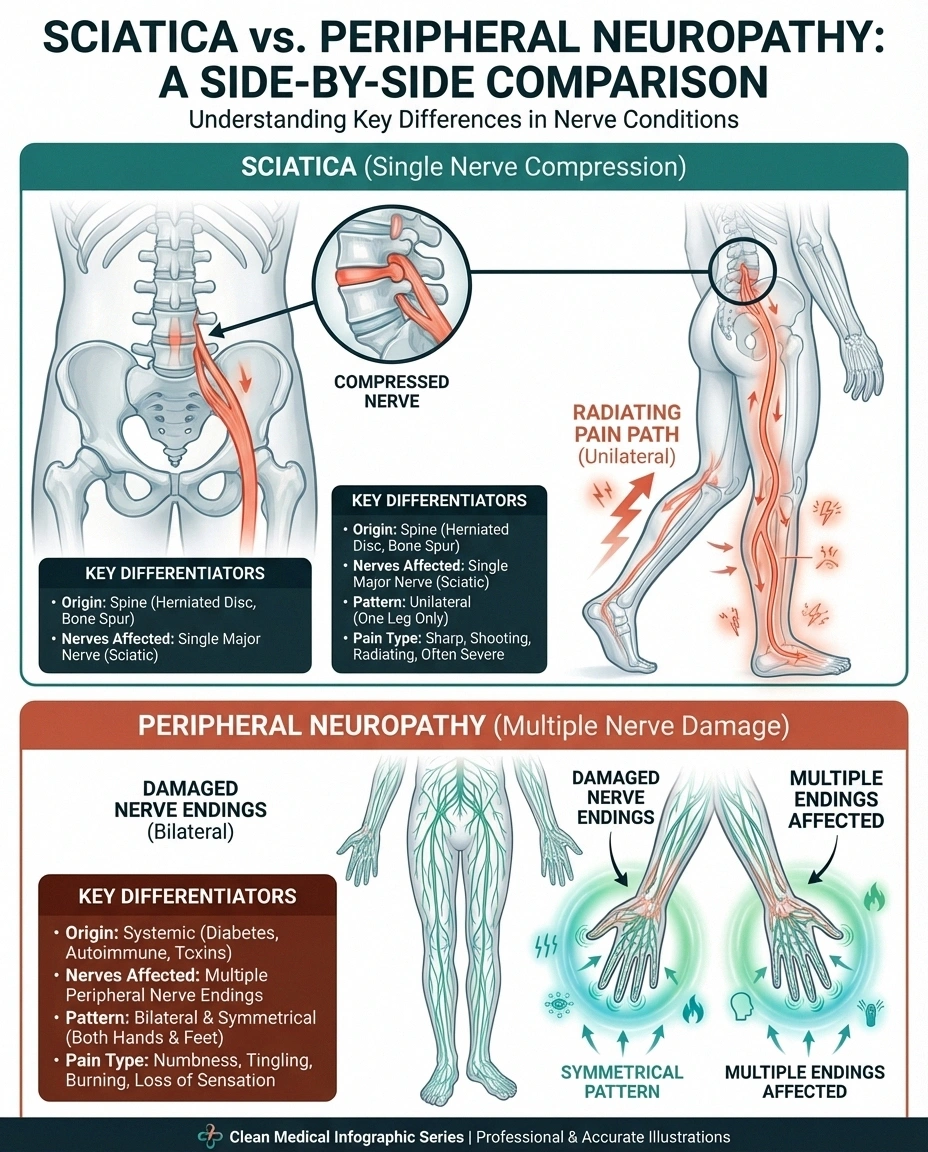
This damage disrupts how nerves send signals, leading to pain, numbness in feet from sciatica versus neuropathyness, tingling, and weakness — most commonly in the hands and feet. Think of it like the difference between a garden hose being kinked (sciatica) versus the hose itself developing cracks and holes (neuropathy).
Key characteristics of peripheral neuropathy include:
- Symmetrical symptoms — neuropathy typically affects both feet or both hands equally, in what doctors call a “stocking-and-glove” pattern
- Constant, steady symptoms — unlike sciatica, the pain and numbness don't significantly change based on position or activity
- Gradual progression — symptoms usually start in the toes and slowly spread upward over months or years
- Temperature sensitivity — many people notice they can't feel hot or cold as well, or that temperature changes make symptoms worse
- Worse at night — neuropathy symptoms frequently intensify in the evening and overnight, disrupting sleep quality
Peripheral neuropathy affects an estimated 20 million Americans, according to the National Institute of Neurological Disorders and Stroke. The most common cause is diabetes, but neuropathy can also result from chemotherapy, vitamin deficiencies, autoimmune conditions, infections, and many other factors.
Side-by-Side Comparison: Sciatica vs. Neuropathy
Understanding the differences at a glance can help you start identifying which condition may be affecting you. Here's how the two compare across the most important characteristics:
✦ Sharp, shooting pain
✦ Changes with position
✦ Usually sudden onset
✦ Lower back pain common
✦ Mechanical cause (compression)
✦ Burning, tingling pain
✦ Constant regardless of position
✦ Gradual onset over months
✦ Back pain is rare
✦ Metabolic cause (nerve damage)
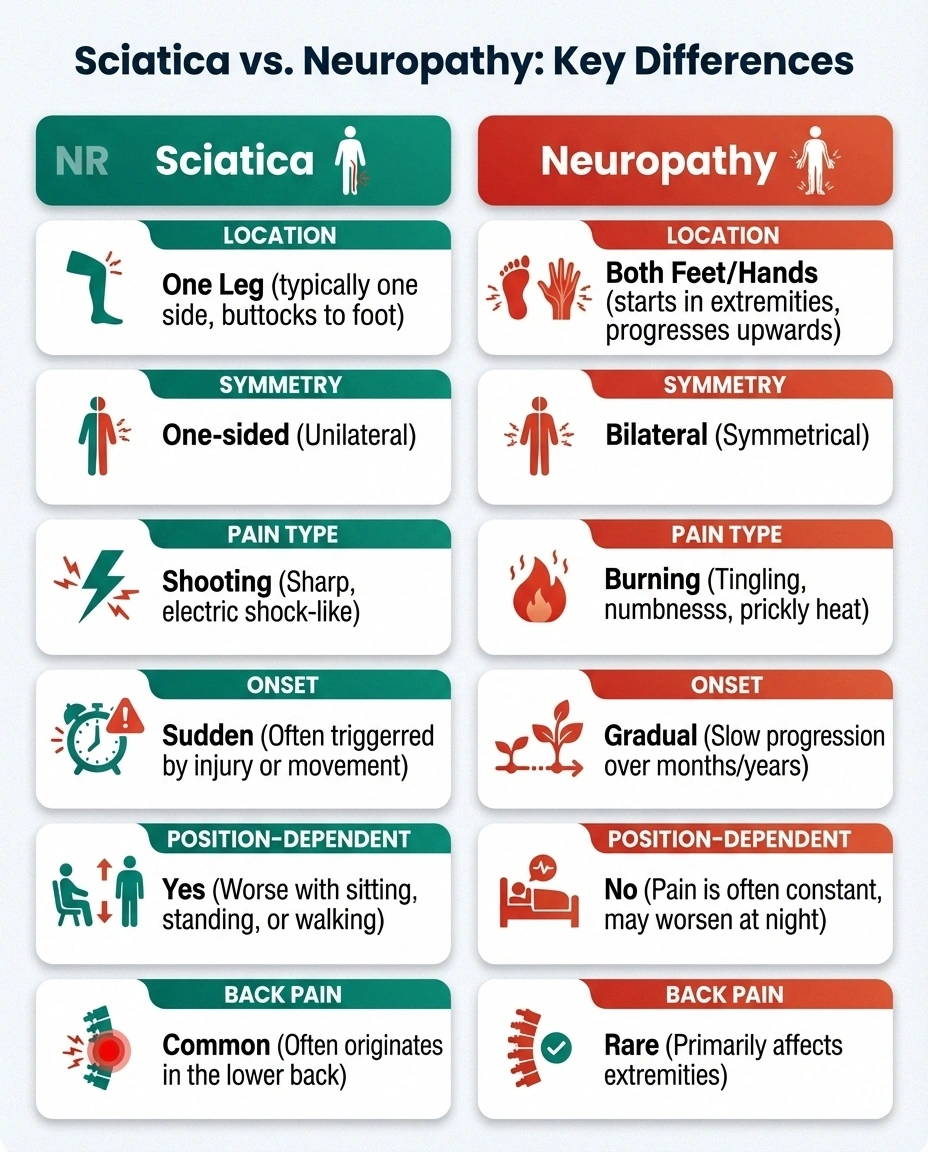
Location of symptoms: Sciatica follows a specific path from the lower back down one leg. Neuropathy typically starts in both feet or both hands and spreads inward over time.
Symmetry: Sciatica is almost always one-sided. Neuropathy usually affects both sides of the body equally.
How symptoms behave: Sciatica pain changes — it may flare when you sit, ease when you walk, and worsen when you cough or sneeze. Neuropathy symptoms are more constant and don't respond as much to position changes.
Type of pain: Sciatica tends to produce sharp, shooting, or electric-shock sensations. Neuropathy more commonly causes burning, tingling, pins-and-needles sensations, or a feeling of wearing invisible socks or gloves.
Onset: Sciatica often has a clear trigger (injury, heavy lifting, sudden movement). Neuropathy develops gradually over months or years without an obvious starting point.
Back pain: Sciatica almost always involves lower back pain. Neuropathy rarely causes back pain unless there's an overlapping condition.
Underlying cause: Sciatica is mechanical — something is physically pressing on the sciatic nerve. Neuropathy is usually metabolic — nerve damage from conditions like diabetes, nutritional deficiencies, or toxic exposures.
Can You Have Both Sciatica and Neuropathy?
Yes — and this is more common than many people realize. Someone with diabetes, for example, may develop peripheral neuropathy from high blood sugar AND develop sciatica from a herniated disc. The two conditions are not mutually exclusive.
When both conditions are present, the symptoms can overlap and make diagnosis more challenging. You might have the constant burning in your feet from neuropathy combined with shooting pain down one leg from sciatica. This is one reason why a proper medical evaluation — not just self-diagnosis — is so important.
Research published in the journal Schmerz has explored the concept of “mixed pain” in sciatica, noting that chronic sciatica can involve both nociceptive (mechanical) and neuropathic pain components. This means that even sciatica itself may sometimes develop neuropathic characteristics if the nerve compression continues long enough to cause actual nerve damage.
Common Causes of Each Condition
Understanding the root causes helps explain why these conditions behave so differently and require different treatment approaches.

What Causes Sciatica
Sciatica is almost always caused by something physically pressing on the sciatic nerve or its roots where they exit the spine:
- Herniated or bulging disc — the most common cause, responsible for roughly 90% of sciatica cases
- Spinal stenosis — narrowing of the spinal canal that puts pressure on nerve roots
- Degenerative disc disease — age-related wear that can lead to disc bulging or bone spurs
- Spondylolisthesis — a vertebra slipping forward over the one below it
- Piriformis syndrome — the piriformis muscle in the buttock spasms and compresses the sciatic nerve
- Pregnancy — the growing uterus can put pressure on the sciatic nerve
What Causes Peripheral Neuropathy
Peripheral neuropathy involves damage to the nerve fibers themselves, and the list of potential causes is much longer:
- Diabetes — the leading cause, affecting up to 50% of people with diabetes over time
- Chemotherapy — certain cancer drugs are toxic to peripheral nerves
- Vitamin deficiencies — particularly B12, B1, B6, and E
- Autoimmune conditions — lupus, rheumatoid arthritis, Guillain-Barré syndrome
- Alcohol abuse — chronic heavy drinking damages nerves directly and causes nutritional deficiencies
- Infections — HIV, Lyme disease, hepatitis C, shingles
- Medications — certain antibiotics, anti-seizure drugs, and HIV medications
- Idiopathic — in up to 30% of cases, no cause is ever identified
How Each Condition Is Diagnosed
Proper diagnosis is crucial because the treatment paths diverge significantly. Here's what to expect when you see your doctor about nerve-related leg or foot symptoms.
Diagnosing Sciatica
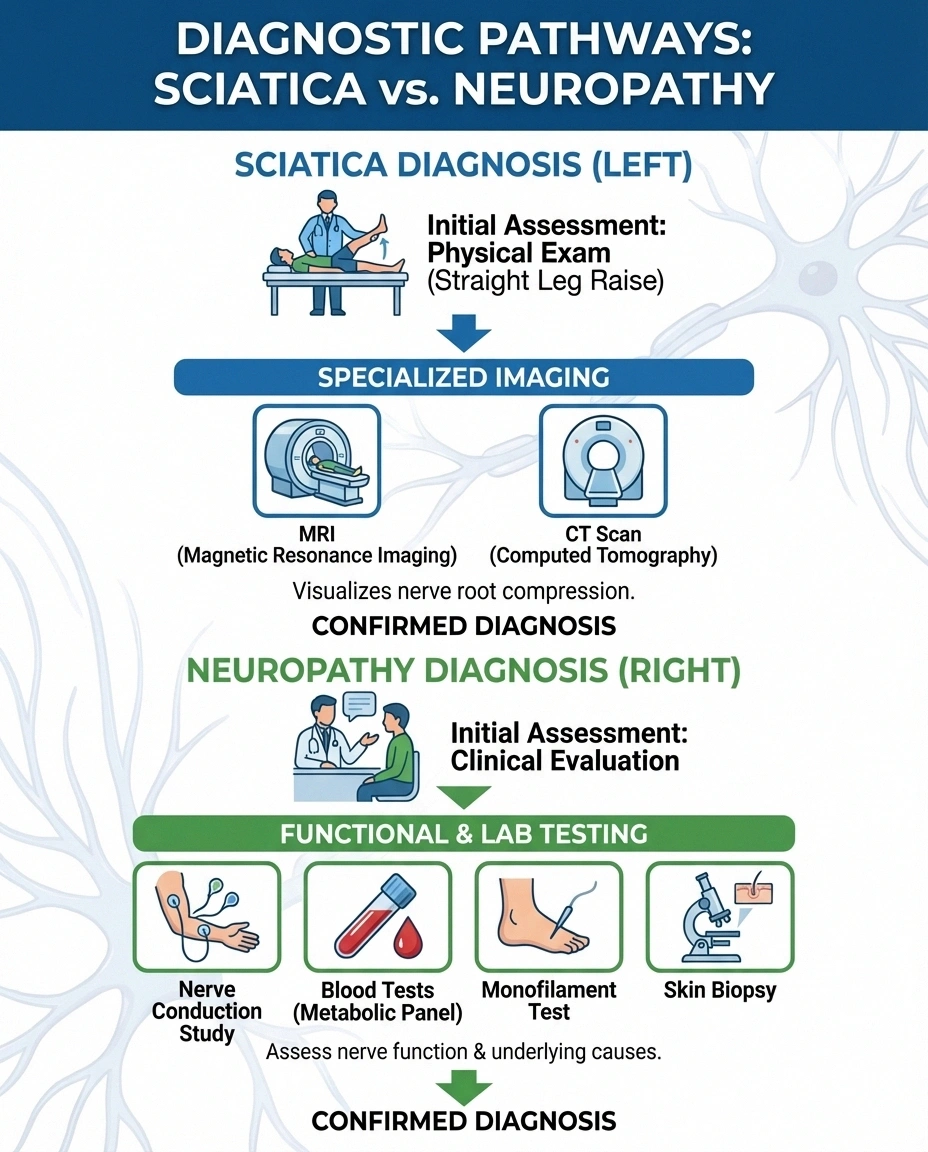
Your doctor will typically start with a physical exam, looking for specific signs that point to sciatic nerve involvement:
- Straight leg raise test — lying on your back while the doctor lifts your affected leg. Pain that shoots down the leg when it's raised between 30 and 70 degrees strongly suggests sciatica.
- Neurological examination — testing reflexes, muscle strength, and sensation in the legs
- MRI scan — the gold standard for visualizing herniated discs, spinal stenosis, and other structural causes
- CT scan — sometimes used if MRI isn't available or is contraindicated
- Electromyography (EMG) — measures electrical activity in muscles to determine whether nerve compression is causing muscle weakness
Diagnosing Peripheral Neuropathy
The diagnostic approach for neuropathy involves both confirming nerve damage and identifying its cause:
- Nerve conduction studies (NCS) — electrodes on the skin measure how fast electrical signals travel through your nerves. Slow conduction indicates nerve damage.
- EMG — combined with NCS, this helps pinpoint which nerves are affected and how severely
- Blood tests — checking blood sugar (for diabetes), vitamin levels (especially B12), thyroid function, liver and kidney function, and inflammatory markers
- Monofilament testing — a thin fiber pressed against the foot to test for loss of protective sensation
- Skin biopsy — a small sample of skin can reveal reduced nerve fiber density, particularly helpful for diagnosing small fiber neuropathy
If you're unsure which specialist to see, start with your primary care doctor. They can perform initial assessments and refer you to a neurologist if needed.
Treatment Approaches: Why the Distinction Matters
This is where the sciatica-versus-neuropathy distinction becomes most practical. The treatments that help one condition may be ineffective or even counterproductive for the other.

Treating Sciatica
Because sciatica is usually caused by mechanical compression, treatment focuses on relieving that pressure:
- Physical therapy — targeted exercises to strengthen core muscles, improve flexibility, and take pressure off the sciatic nerve
- Anti-inflammatory medications — NSAIDs like ibuprofen help reduce inflammation around the compressed nerve
- Ice and heat therapy — ice for acute flare-ups, heat for muscle relaxation
- Epidural steroid injections — corticosteroids injected near the affected nerve root to reduce inflammation
- Chiropractic care — spinal adjustments may help relieve nerve compression in some cases
- Surgery — in severe or persistent cases, procedures like microdiscectomy or laminectomy may be recommended to physically remove the source of compression
The encouraging reality is that most sciatica cases — up to 80-90% — resolve with conservative treatment within 6 to 12 weeks. Surgery is typically reserved for cases where conservative treatment fails or where there are signs of serious nerve damage (like progressive weakness or loss of bladder/bowel control).
Treating Peripheral Neuropathy
Neuropathy treatment focuses on addressing the underlying cause (when possible) and managing symptoms:
- Treating the root cause — managing blood sugar for diabetic neuropathy, supplementing B12 for deficiency-related neuropathy, adjusting medications that cause nerve damage
- Pain medications — gabapentin, pregabalin, duloxetine, and certain tricyclic antidepressants are commonly prescribed for neuropathic pain
- Topical treatments — capsaicin cream and lidocaine patches can provide localized relief
- Physical therapy — balance training, strengthening exercises, and mobility work help manage functional limitations
- Lifestyle modifications — regular exercise, proper nutrition, and avoiding alcohol may help slow progression
- Supplemental support — some people find benefit from alpha-lipoic acid, B vitamins, and other nerve-supporting supplements
Unlike sciatica, peripheral neuropathy is often a chronic condition. While treatment can manage symptoms and sometimes slow progression, complete reversal depends heavily on the underlying cause and how early treatment begins.
A Simple Self-Assessment Guide
While only a medical professional can give you a definitive diagnosis, these questions can help you better understand your symptoms before your appointment:
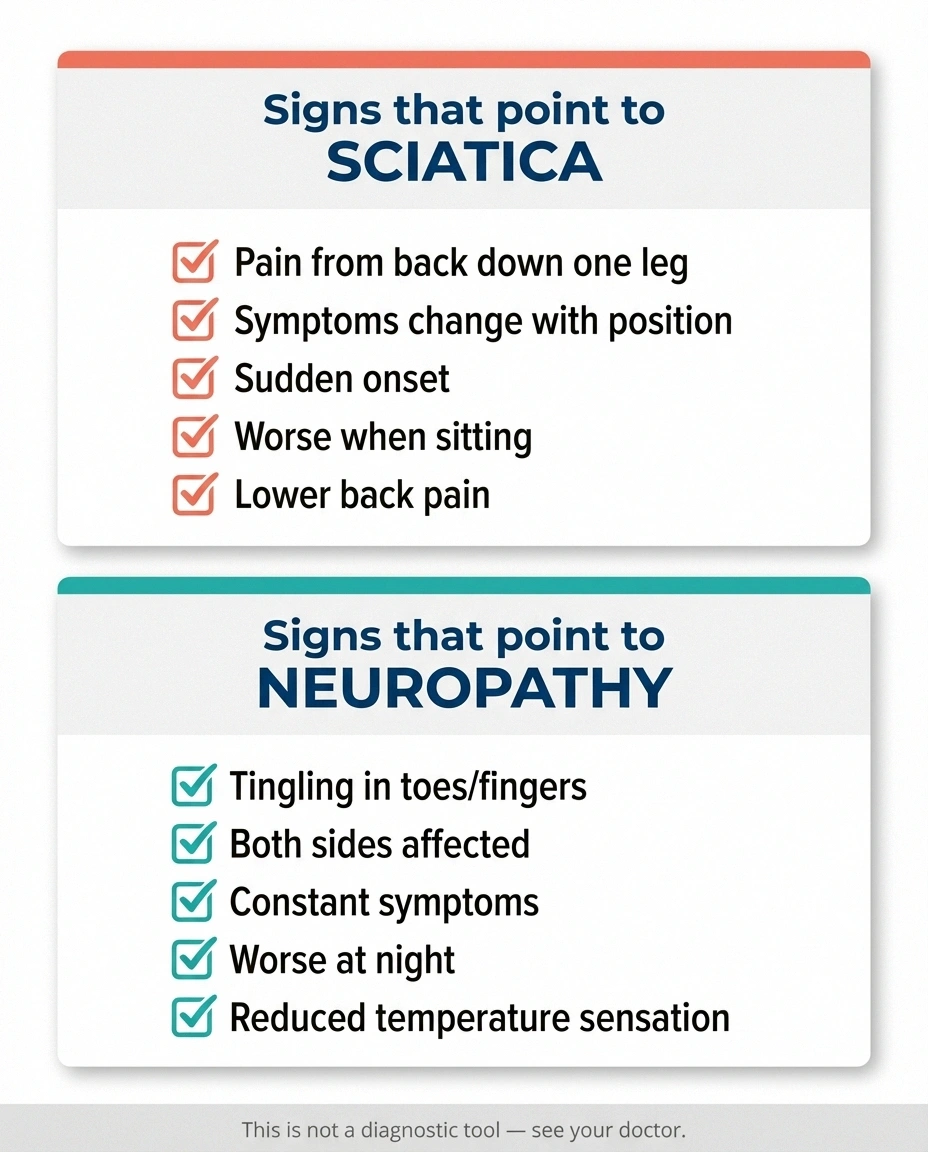
Your symptoms may lean toward sciatica if:
- Pain starts in your lower back or buttock and radiates down one leg
- Symptoms change significantly with different positions (sitting vs. standing vs. walking)
- You can remember when the pain started or what triggered it
- Coughing, sneezing, or straining makes the pain worse
- You have lower back pain along with the leg symptoms
- Only one side of your body is affected
Your symptoms may lean toward neuropathy if:
- Tingling, burning, or numbness started in your toes or fingers and has gradually spread
- Symptoms are roughly equal on both sides of your body
- The discomfort is constant regardless of position or activity
- Symptoms are worse at night, making it hard to sleep
- You notice reduced sensitivity to temperature or touch
- You have a known risk factor like diabetes, vitamin deficiency, or history of chemotherapy
Remember: these are general guidelines, not diagnostic criteria. Some people have atypical presentations, and as we discussed, it's possible to have both conditions simultaneously. The most important step is bringing your specific symptom pattern to a qualified healthcare provider.
When to See a Doctor
Both sciatica and neuropathy warrant medical attention, but certain red flags demand urgent evaluation:
☐ Loss of bladder or bowel control
☐ Rapidly worsening numbness that spreads quickly
☐ Unexplained weight loss combined with nerve pain
☐ Nerve symptoms following a severe injury
- Sudden, severe weakness in one or both legs — this could indicate serious nerve compression requiring emergency treatment
- Loss of bladder or bowel control — a medical emergency that may indicate cauda equina syndrome, requiring immediate surgery
- Rapidly worsening symptoms — especially numbness that spreads quickly
- Unexplained weight loss combined with nerve pain — could signal an underlying systemic condition
- Symptoms following a severe injury — like a car accident or significant fall
Even without these red flags, don't wait too long to seek help. Early diagnosis and treatment — for both sciatica and neuropathy — lead to better outcomes. The longer nerve compression or damage continues without treatment, the harder it may be to reverse.
Living With Nerve Pain: Practical Steps That Help Both Conditions
While sciatica and neuropathy require different medical treatments, some lifestyle strategies may help manage either type of nerve pain:

- Stay active — gentle movement improves circulation and may reduce nerve pain. Walking is often beneficial for both conditions, as movement helps nourish nerves and prevent stiffness.
- Manage your weight — excess weight increases pressure on the spine (worsening sciatica) and is associated with metabolic conditions that contribute to neuropathy.
- Practice good posture — proper alignment reduces stress on the sciatic nerve and supports overall nerve health.
- Prioritize sleep — poor sleep increases pain sensitivity. If nerve pain disrupts your rest, consider strategies like elevating your legs, using supportive pillows, or following a dedicated sleep improvement plan.
- Reduce stress — chronic stress amplifies pain perception. Mindfulness, gentle yoga, and relaxation techniques may help.
- Track your symptoms — keeping a pain journal helps your doctor distinguish between sciatica and neuropathy and track treatment effectiveness.
Frequently Asked Questions
Can sciatica turn into neuropathy?
Sciatica itself is not a form of neuropathy, but prolonged, untreated sciatic nerve compression can cause enough damage to the nerve to produce neuropathic symptoms. This is sometimes called sciatic neuropathy. The key difference is that typical sciatica resolves when the compression is removed, while nerve damage from prolonged compression may persist even after the pressure is relieved.
Does neuropathy show up on an MRI?
Standard MRI scans are not the primary tool for diagnosing peripheral neuropathy. They are more useful for identifying the structural causes of sciatica, like herniated discs. However, specialized MRI techniques called magnetic resonance neurography can visualize nerves and may help identify certain types of neuropathy. Nerve conduction studies and blood tests are the main diagnostic tools for peripheral neuropathy.
Is sciatica worse than neuropathy?
Neither condition is universally worse than the other. Acute sciatica can be intensely painful but usually resolves within weeks to months. Peripheral neuropathy is typically a chronic condition that may progress over years. The severity depends on the individual case, the underlying cause, and how quickly treatment begins.
Can a chiropractor help with neuropathy?
Chiropractic care may help with sciatica because the condition often involves spinal misalignment or disc problems that chiropractic adjustments can address. For peripheral neuropathy, the evidence is more limited. Some people report symptom improvement, but neuropathy is caused by nerve damage rather than compression, so spinal adjustments may not address the root cause. Always discuss any treatment approach with your primary care doctor first.
Why does my nerve pain get worse at night?
Nighttime worsening is more characteristic of peripheral neuropathy than sciatica. Several factors may contribute: fewer distractions allow you to notice pain more, body temperature changes during sleep can affect nerve sensitivity, and lying in one position for extended periods can compress nerves. For sciatica specifically, morning stiffness is more common than nighttime worsening, though some people experience pain at night from certain sleeping positions.
What kind of doctor should I see for nerve pain in my legs?
Start with your primary care physician, who can perform initial evaluations and order basic tests. From there, you may be referred to a neurologist for specialized nerve testing, an orthopedic surgeon or physiatrist if sciatica is suspected, or a pain management specialist for chronic pain. If you have diabetes, your endocrinologist should also be involved in managing any neuropathy-related symptoms.
The Bottom Line
Sciatica and peripheral neuropathy can feel frustratingly similar on the surface, but they are fundamentally different conditions with different causes, different trajectories, and different treatment approaches. Sciatica is typically a mechanical problem — a compressed nerve — that often resolves with the right conservative treatment. Peripheral neuropathy is a condition of nerve damage that requires identifying and addressing the underlying cause.
The most important thing you can do is pay attention to your specific symptom pattern and share those details with your healthcare provider. Whether your pain follows the classic one-sided, position-dependent pattern of sciatica or the gradual, symmetrical progression of neuropathy — or some confusing combination of both — an accurate diagnosis is the foundation for effective treatment.
You don't have to figure this out alone. Talk to your doctor, bring your questions, and don't settle for a vague answer. Understanding exactly what's happening with your nerves is the first step toward feeling better.


