
Numbness in Feet: Neuropathy vs. PAD vs. Sciatica vs. Diabetes — A Complete Differential Guide
You know that moment when you stand up and realize you can't quite feel the floor beneath your feet? Or when you're walking and it's like stepping on cotton balls? I've been there — and so have millions of others. Foot numbness is one of the most common symptoms that brings people to a neurologist's office, and for good reason: it can signal several very different underlying problems.
The challenge is that numbness in the feet is a shared symptom across conditions that have completely different causes and treatments. Peripheral neuropathy, peripheral artery disease (PAD), sciatica, and diabetic complications can all make your feet go numb — but what's happening inside your body is fundamentally different in each case. Getting the wrong diagnosis doesn't just delay treatment — it can mean treating the wrong thing entirely.
This guide breaks down each condition, explains how and why it causes foot numbness, and gives you the specific patterns that help distinguish one from another. Think of it as the diagnostic conversation your doctor wishes you'd already had before walking in the door.
The Anatomy of Foot Numbness
Your feet have one of the densest concentrations of nerve endings anywhere in your body. Those nerves serve a critical function — they tell your brain where the ground is, whether something is hot or cold, sharp or smooth, and where your body is in space. When that communication system breaks down, numbness is the result.
Americans with peripheral neuropathy
of people with diabetes develop neuropathy
Americans over 40 affected by PAD
But the breakdown can happen at different points along the pathway. The nerves themselves can be damaged (neuropathy). The blood supply feeding those nerves can be reduced (PAD). A nerve root in the spine can be compressed (sciatica). Or chronically elevated blood sugar can silently poison the nerve fibers over years (diabetic neuropathy). Each mechanism produces numbness, but the specific pattern, progression, and accompanying symptoms are different — and those differences are your diagnostic roadmap.
Peripheral Neuropathy: The Most Common Cause of Foot Numbness
Peripheral neuropathy is far and away the most frequent reason for chronic foot numbness. According to the National Institute of Neurological Disorders and Stroke, over 20 million Americans have some form of peripheral neuropathy — and the feet are almost always the first place symptoms appear.
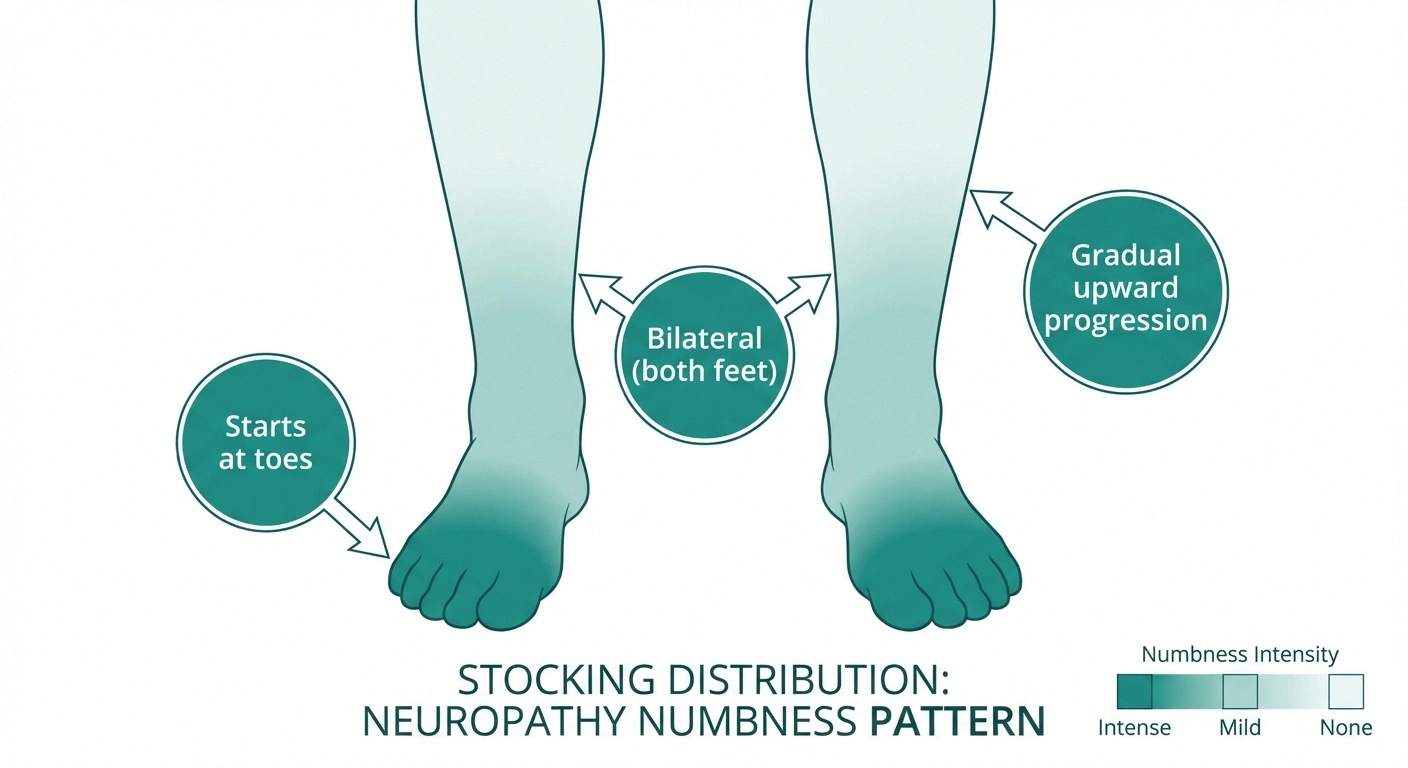
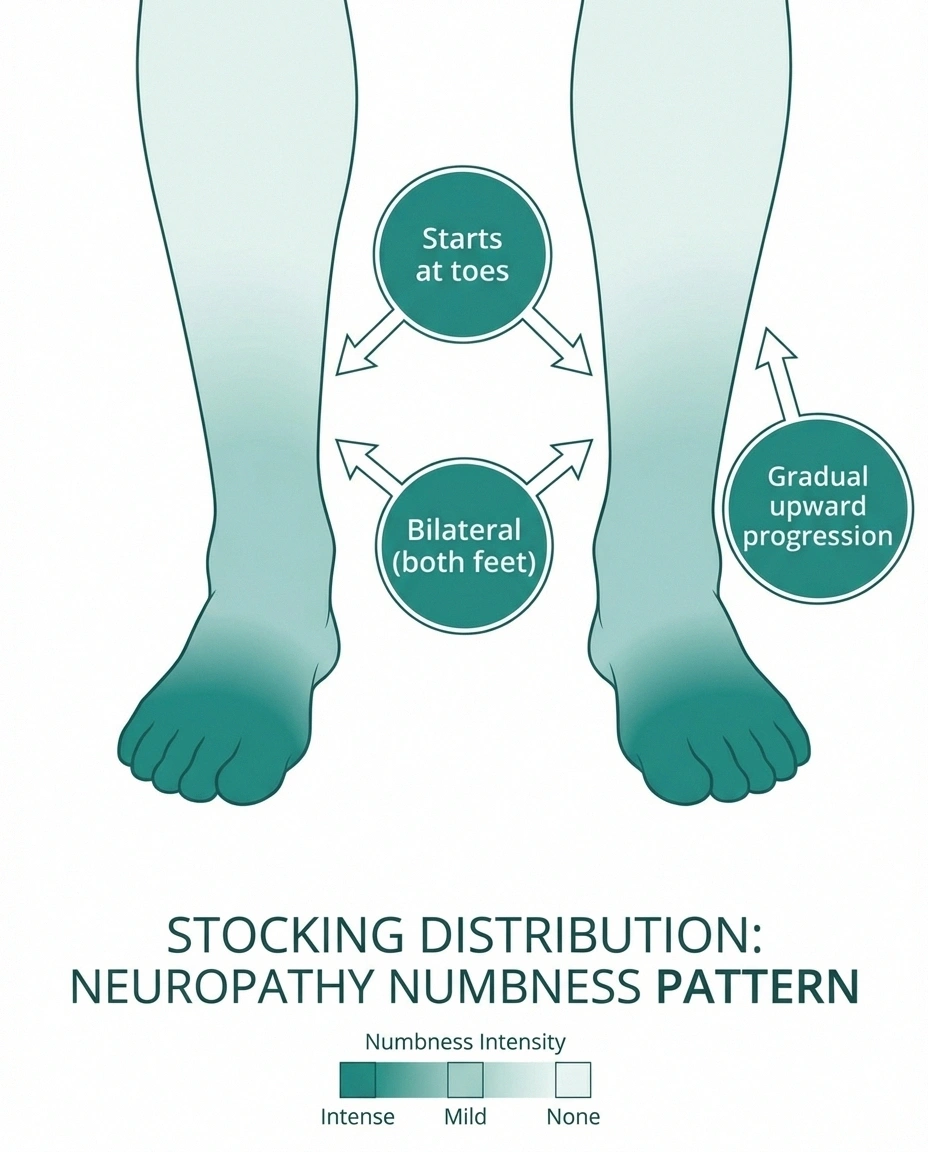
The numbness from neuropathy follows a very specific pattern that neurologists call “stocking distribution.” Picture pulling on an invisible pair of socks — the numbness starts at the tips of your toes and gradually extends upward over the foot, ankle, and potentially into the lower leg. This pattern occurs because the longest nerve fibers in your body (the ones reaching to your toes) are the most vulnerable to damage.
Crucially, neuropathy numbness is almost always bilateral — it affects both feet at roughly the same time and severity. If numbness is in one foot only, neuropathy is less likely (though not impossible with conditions like small fiber neuropathy).
What Neuropathy Numbness Feels Like
People describe neuropathy numbness in remarkably consistent ways: “walking on cotton,” “feet wrapped in thick socks,” “like my feet fell asleep and won't wake up.” Unlike the temporary numbness from sitting on your foot wrong, neuropathy numbness doesn't resolve by shaking your foot or walking around. It's persistent, often worse at night, and tends to progress slowly upward over months to years.
Neuropathy Signature
The combination of numbness AND pain (burning, tingling, pins and needles) is the fingerprint of neuropathy. Other causes of foot numbness typically don't produce this “painful numbness” combination.
The numbness is frequently accompanied by other sensory disturbances: burning sensations, tingling (pins and needles), shooting pains, or extreme sensitivity to touch where even bed sheets feel uncomfortable. This combination of numbness AND pain (called painful neuropathy) is a distinctive feature that other conditions don't typically produce.
Neuropathy has dozens of potential causes, but the most common include diabetes (which we'll address separately below), vitamin B12 deficiency, chronic alcohol use, chemotherapy, autoimmune conditions, and idiopathic cases where the cause isn't identified.
Peripheral Artery Disease: When Blood Can't Reach Your Feet
PAD causes foot numbness through vascular compromise rather than nerve damage. Atherosclerosis — the buildup of fatty deposits in artery walls — reduces blood flow to the legs and feet. When your peripheral nerves don't receive adequate oxygen-rich blood, they begin to malfunction, and numbness can result.
The PAD Test
PAD numbness is activity-dependent — it appears with walking and resolves within minutes of rest. If your foot numbness is constant regardless of activity, PAD alone is unlikely to be the cause.
However, PAD numbness has a very different character than neuropathy numbness. The key distinction is that PAD symptoms are typically activity-dependent. Your feet may feel normal at rest but become numb, crampy, or achy during walking — a pattern called intermittent claudication. The numbness resolves within a few minutes of stopping, because rest reduces the oxygen demand on your muscles and nerves.
The American Heart Association estimates PAD affects approximately 8.5 million Americans over age 40, with prevalence increasing significantly after age 65. Risk factors closely mirror heart disease: smoking (the strongest risk factor), diabetes, high blood pressure, high cholesterol, and family history of cardiovascular disease.
Physical Signs That Point to PAD
Unlike neuropathy, PAD often leaves visible physical clues. Check for skin that appears pale, shiny, or bluish on the affected foot. Feel the top of your foot and behind your ankle — weak or absent pulses suggest reduced blood flow. Hair loss on the legs and feet, thickened toenails, and wounds that heal slowly are all vascular red flags. One practical test: elevate your legs for 30-60 seconds, then let them hang down. If PAD is present, the foot may turn pale when elevated and then flush deep red as gravity assists blood flow back.

Temperature differences are another clue — a foot with reduced blood flow often feels noticeably cooler than the other foot. While neuropathy can also cause temperature sensation changes, the actual skin temperature with PAD is objectively different (measurable, not just perceived).
Sciatica: When a Pinched Nerve Mimics Foot Numbness
Sciatica isn't a disease — it's a symptom caused by compression or irritation of the sciatic nerve or the nerve roots that form it in the lower spine. When the L5 or S1 nerve root is compressed (usually by a herniated disc or spinal stenosis), the pain and numbness can radiate all the way down through the buttock, thigh, and calf into the foot.
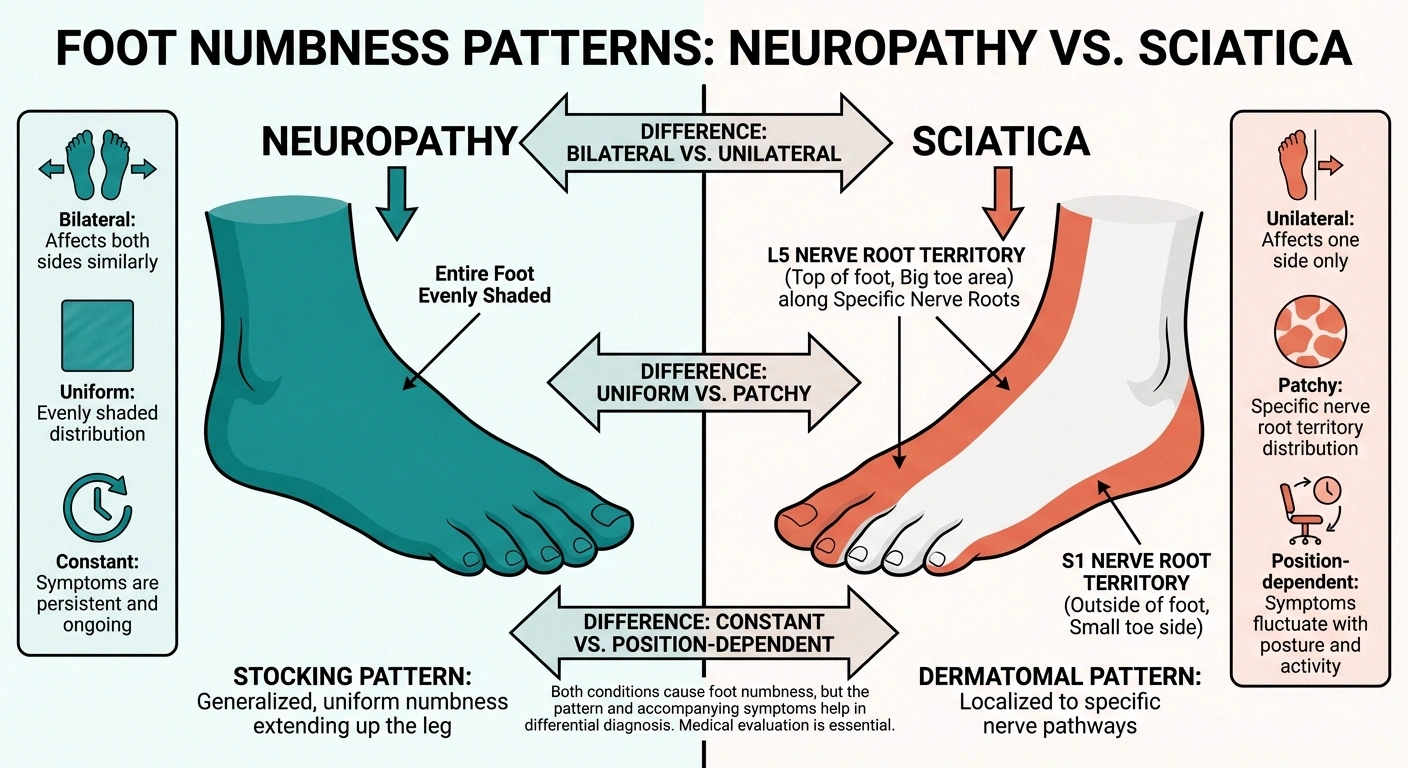
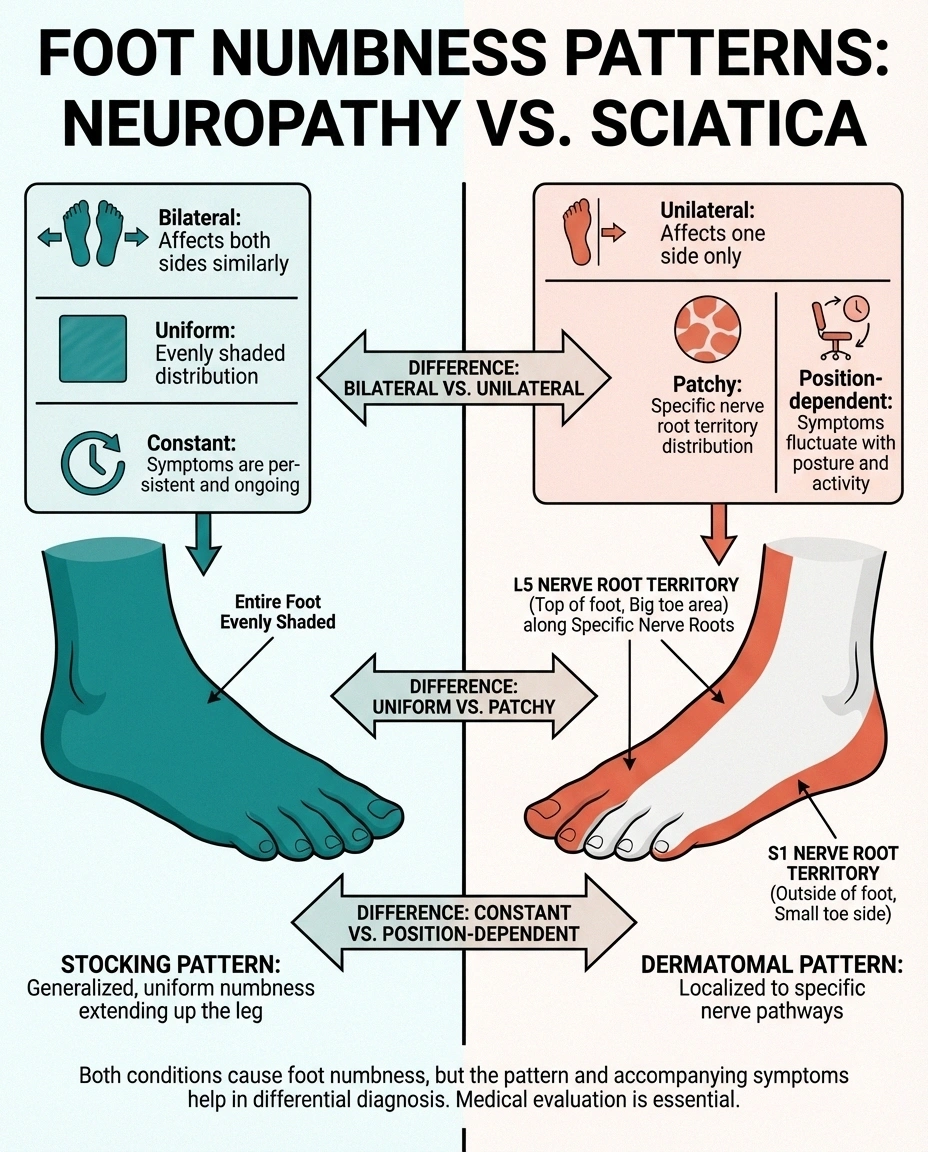
What distinguishes sciatica from neuropathy is the distribution pattern. Sciatica follows a specific nerve root territory — typically running down the back or side of the leg in a narrow band (called a dermatome). The numbness in the foot affects a specific region: L5 compression tends to numb the top of the foot and big toe, while S1 compression typically affects the outside of the foot and little toe.
The Sciatica Fingerprint
Sciatica has several characteristic features that separate it from the other conditions. The numbness is almost always unilateral — it affects one foot, not both. It frequently comes with back pain or buttock pain, though not always. And crucially, the numbness changes with body position and activity: sitting, bending, coughing, or sneezing can trigger or worsen it, while lying down with knees bent often provides relief.
The onset of sciatica can be sudden (after lifting something heavy or a specific injury) or gradual (from progressive disc degeneration). This matters for diagnosis because neuropathy and PAD almost never start suddenly — they develop slowly over weeks to months.
One key differentiator: sciatica numbness doesn't follow the stocking pattern. It's patchy — numb in specific spots along the nerve path rather than a uniform loss of sensation across the entire foot. And unlike neuropathy, sciatica doesn't typically cause the burning, tingling, pins-and-needles sensation that neuropathy patients describe.
Diabetic Neuropathy: The Special Case
Diabetes deserves its own section because it causes foot numbness through multiple mechanisms simultaneously — making it both the most common cause of neuropathy AND a condition that can coexist with PAD and spinal problems. Approximately 50% of people with diabetes will eventually develop diabetic neuropathy, according to the American Diabetes Association.

Chronically elevated blood sugar directly damages peripheral nerves through several pathways: it creates toxic metabolic byproducts, damages the small blood vessels that feed the nerves (vasa nervorum), triggers inflammation, and impairs the nerves' ability to repair themselves. The result is a progressive sensory neuropathy that typically begins in the feet.
What makes diabetic foot numbness particularly tricky is that diabetes also increases the risk of PAD (by 2-4 times compared to non-diabetics). So a person with diabetes and numb feet may have neuropathy, PAD, or both — and the treatment approach differs significantly depending on which is the primary driver.
Warning Signs Unique to Diabetic Foot Numbness
Diabetic neuropathy often progresses silently. Many people don't notice the numbness until it's advanced because the loss of sensation is so gradual. The dangerous consequence: numb feet can't feel injuries, blisters, or pressure sores. Unnoticed wounds combined with diabetes-related poor wound healing can lead to serious infections and, in severe cases, amputation. This is why daily foot checks are non-negotiable for anyone with diabetes.
The numbness pattern in diabetic neuropathy is identical to other peripheral neuropathies — bilateral, stocking distribution, starting at the toes. The distinguishing factor isn't the numbness pattern itself; it's the context. If you have diabetes (or prediabetes with A1C above 5.7%) and develop foot numbness, diabetic neuropathy is the presumptive diagnosis until proven otherwise.
Side-by-Side: How to Tell Them Apart
When you're lying in bed at 2 AM wondering why your feet are numb, a structured comparison can cut through the confusion. Here are the features that matter most for distinguishing these four conditions.
Pattern of Numbness
Neuropathy: Both feet equally, stocking distribution from toes upward. Constant, doesn't change with activity or rest. Progresses slowly upward over months.
PAD: May affect one or both feet. Activity-triggered — comes on with walking, resolves within minutes of rest. Often accompanied by cramping in calves.
Sciatica: One foot only, following a specific nerve root territory. Changes with position — worse with sitting, bending, or coughing. Often comes with back or buttock pain.
Diabetic Neuropathy: Both feet equally, stocking distribution — identical pattern to other neuropathies. The context of diabetes or prediabetes is the distinguishing factor, not the numbness pattern itself.
Associated Symptoms
Neuropathy: Burning, tingling, pins and needles. Worse at night. Sensitivity to touch. Balance problems.
🧦 Neuropathy
Both feet, stocking pattern. Burning + tingling. Worse at night. Balance issues. Constant — doesn't change with activity.
❤️ PAD
Activity-triggered numbness + cramping. Cool skin, weak pulses. Resolves with rest. Pale/bluish skin color changes.
⚡ Sciatica
One foot only. Follows nerve root path. Changes with position. Back/buttock pain. Sharp, shooting quality.
🩸 Diabetic
Same stocking pattern as neuropathy. Plus: poor wound healing, infection risk. May coexist with PAD. Foot checks critical.
PAD: Leg cramping with exertion (claudication). Cool skin. Weak foot pulses. Slow wound healing. Pale or bluish skin.
Sciatica: Radiating pain from low back through buttock and leg. Worse with sitting or bending. May have muscle weakness in the foot (foot drop). Sharp or shooting pain quality.
Diabetic Neuropathy: All neuropathy symptoms plus diabetes-specific risks — poor wound healing, increased infection risk, potential Charcot foot deformity. Often coexists with autonomic symptoms (digestive issues, blood pressure changes).
Risk Factor Profile
Neuropathy: Diabetes, vitamin B12 deficiency, alcohol overuse, chemotherapy, autoimmune conditions, family history of neuropathy.
PAD: Smoking (strongest risk factor), diabetes, high blood pressure, high cholesterol, age over 50, family history of cardiovascular disease.
Sciatica: Heavy lifting, prolonged sitting, obesity, age 30-50, physically demanding occupations. Often triggered by a specific incident.
Diabetic Neuropathy: Duration of diabetes (longer = higher risk), poor blood sugar control (A1C above 7%), smoking, high blood pressure, kidney disease.
Diagnostic Tests for Foot Numbness
Your doctor has specific tools to determine which condition is causing your foot numbness. Understanding these tests can help you prepare for appointments and interpret results.
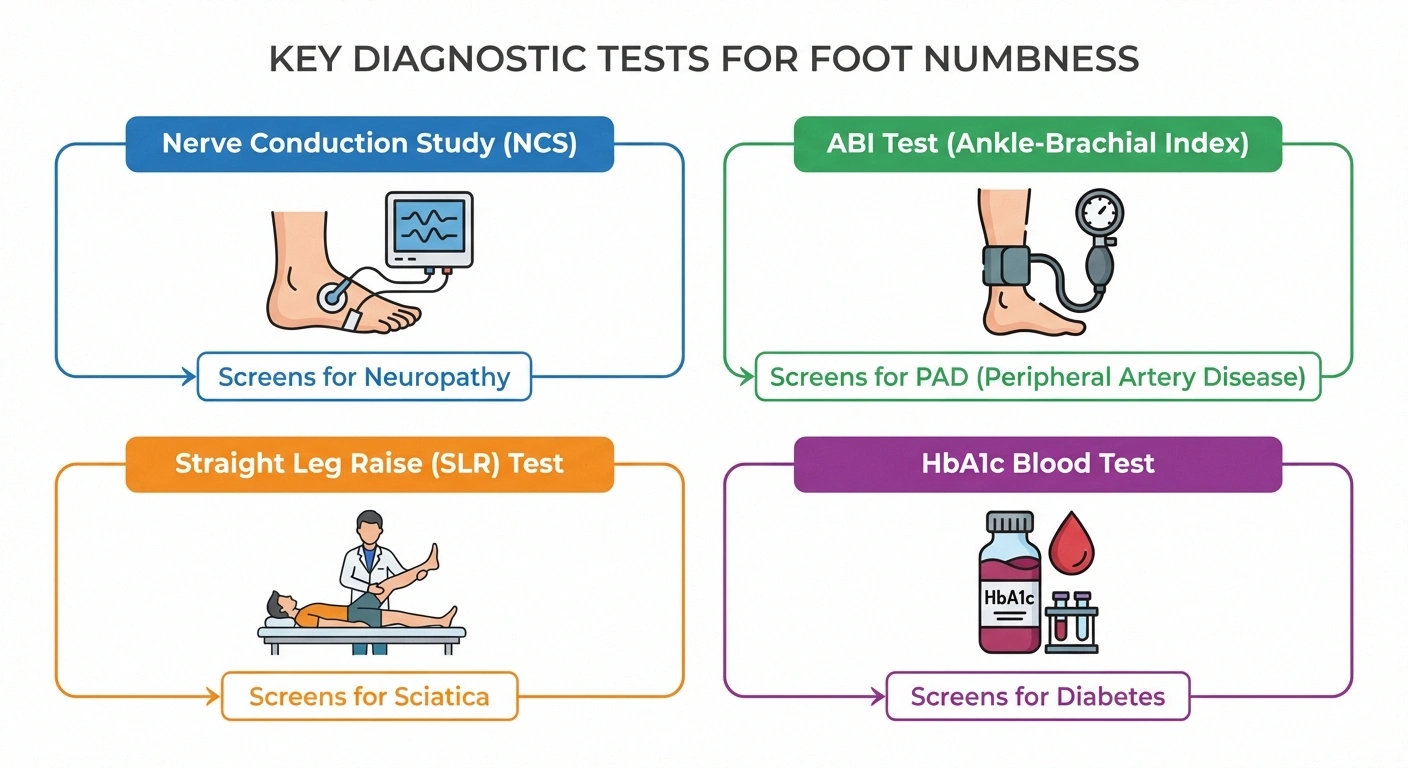
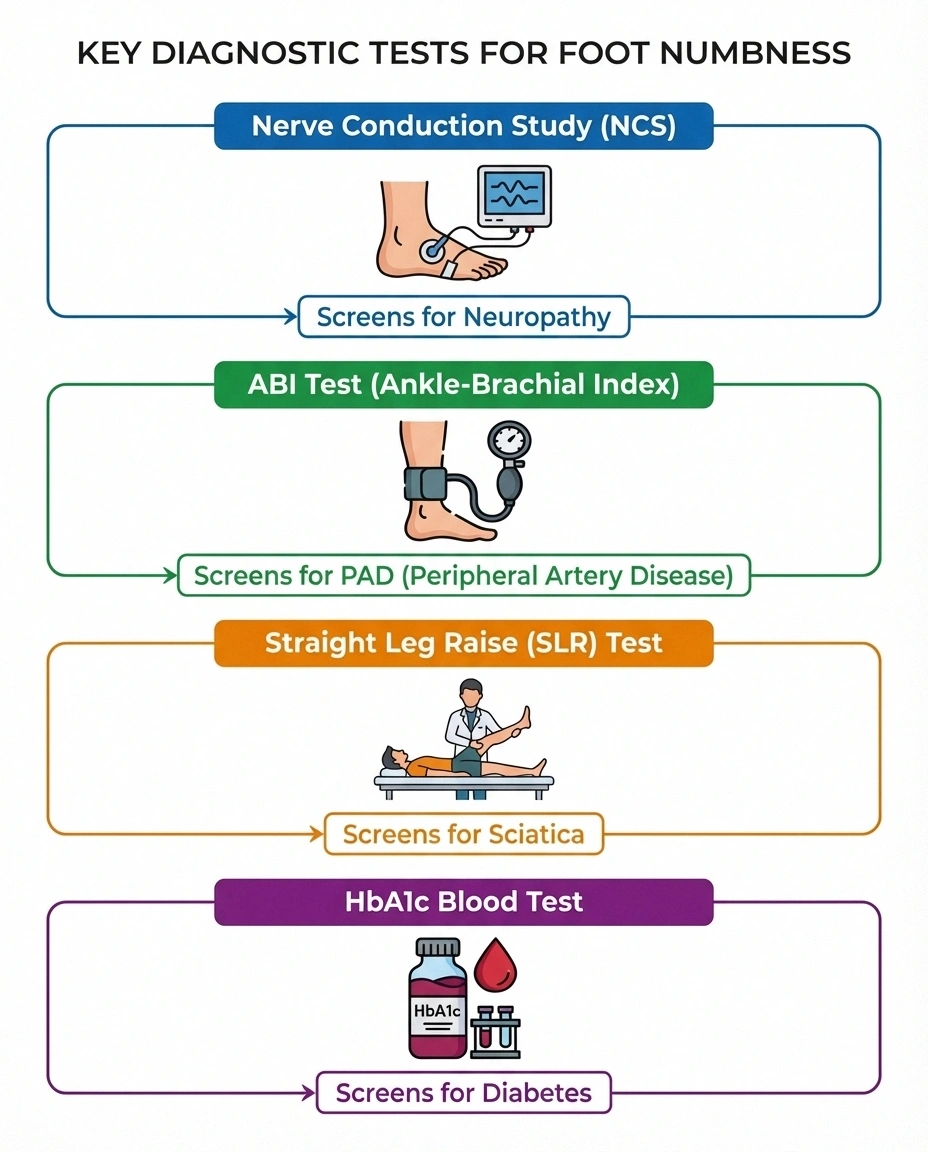
For Neuropathy
Nerve conduction studies (NCS) and electromyography (EMG) are the primary diagnostic tools. NCS measures the speed and strength of electrical signals traveling through your nerves — slowed conduction indicates nerve damage. EMG assesses whether your muscles respond normally to nerve signals. Blood work to identify the cause includes glucose, B12, folate, thyroid function, kidney function, and inflammatory markers. For suspected small fiber neuropathy (which NCS may miss), a skin biopsy can count the small nerve fibers in a tiny punch sample.
For PAD
The ankle-brachial index (ABI) is the first-line screening test — it compares blood pressure at the ankle to blood pressure in the arm. An ABI below 0.9 indicates PAD. Doppler ultrasound provides a non-invasive view of blood flow through the leg arteries. CT angiography or MR angiography offers detailed images of arterial blockages when intervention is being considered.
For Sciatica
MRI of the lumbar spine is the gold standard — it shows disc herniations, spinal stenosis, and other structural causes of nerve compression. Physical examination tests like the straight leg raise (Lasègue's test) can provoke sciatic symptoms and support the diagnosis. EMG may be helpful in distinguishing which nerve root is affected.
For Diabetic Neuropathy
In addition to the NCS/EMG tests above, your doctor will check hemoglobin A1C (reflecting 3-month blood sugar averages), fasting glucose, and potentially an oral glucose tolerance test. A 10-gram monofilament test (pressing a thin nylon fiber against the sole of your foot to test sensation) is a simple, reliable screening tool that your primary care doctor can do in the office. Annual diabetic foot exams are recommended for all people with diabetes.
When Foot Numbness Is an Emergency
Most foot numbness develops gradually and allows time for outpatient evaluation. But certain scenarios demand immediate medical attention. Seek emergency care if you experience sudden-onset numbness in both feet that develops over hours (possible spinal cord compression or stroke), numbness accompanied by severe leg pain that turns the foot pale, blue, or cold (possible acute arterial occlusion — a medical emergency), foot numbness combined with loss of bladder or bowel control (cauda equina syndrome), or rapidly worsening numbness that ascends from feet upward over days (possible Guillain-Barré syndrome).
Emergency Signs — Call 911
Sudden numbness in both feet over hours • Foot turns pale, blue, or cold with severe pain • Loss of bladder or bowel control • Numbness rapidly spreading upward from feet over days. These are neurological or vascular emergencies requiring immediate care.
What Your Feet Are Telling You: The Diagnostic Decision Tree
Here's a practical way to think through your symptoms before your appointment.
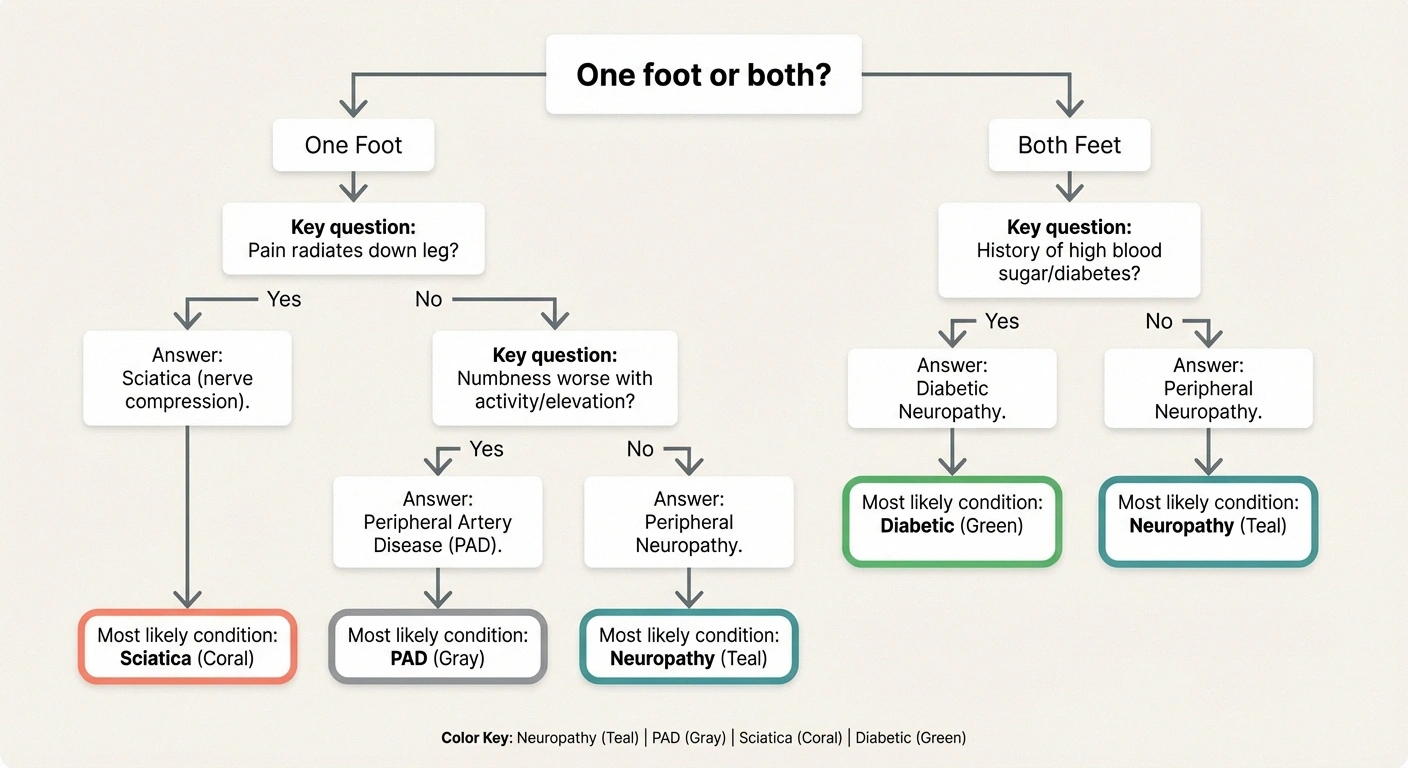
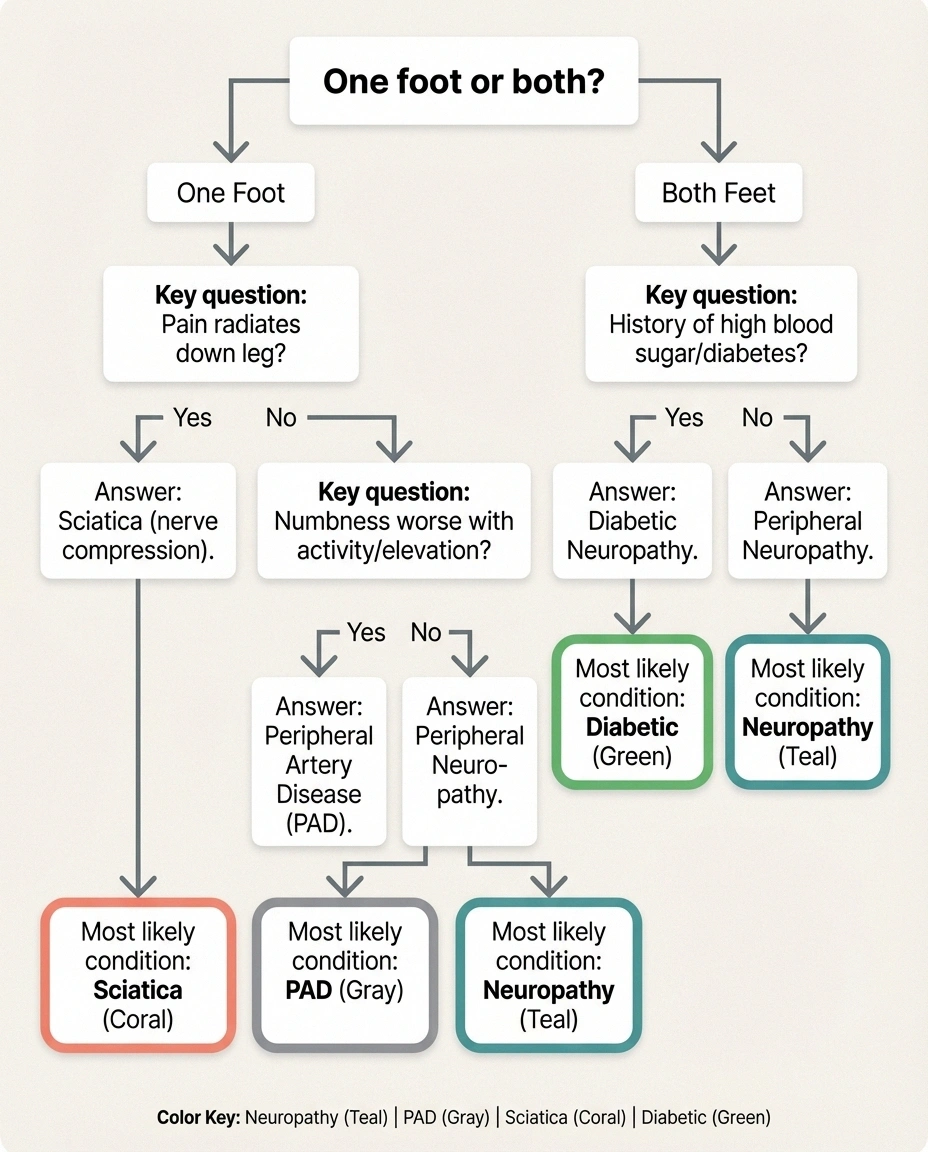
Start by asking: is the numbness in one foot or both? If one foot, sciatica or localized nerve entrapment is more likely. If both feet, neuropathy (including diabetic) or PAD moves to the top.
Next: does the numbness change with activity? If it worsens with walking and improves with rest, PAD is the primary suspect. If it's constant regardless of activity, neuropathy is more likely. If it changes with body position (worse sitting, better lying down), sciatica is the likely culprit.
Then: what accompanies the numbness? Burning, tingling, and night pain suggest neuropathy. Leg cramping and cool skin suggest PAD. Back pain and radiating leg pain suggest sciatica. Diabetes or prediabetes with any of these patterns suggests diabetic neuropathy as the underlying driver.
This isn't a substitute for professional diagnostic testing, but it can help you and your doctor get to the answer faster.
Managing Numb Feet: Protecting Yourself Regardless of the Cause
While you're pursuing a diagnosis, there are universal safety practices that apply regardless of what's causing your foot numbness.

✅ Daily Foot Safety Checklist
Inspect all surfaces of both feet (use a mirror for soles)
Check shoes for pebbles or objects before wearing
Test bath/shower water temperature with your elbow
Never walk barefoot — even at home
Moisturize dry skin (avoid between toes)
Keep nighttime path to bathroom well-lit
Daily foot inspections are essential. When you can't fully feel your feet, you can't rely on pain to alert you to injuries. Check for cuts, blisters, redness, swelling, or any changes daily — use a mirror or ask someone to help check the soles. This is critical for preventing serious complications.
Wear properly fitting shoes with adequate protection. Never walk barefoot, even inside your home. Check your shoes for foreign objects before putting them on — a small pebble you can't feel can cause a wound that doesn't heal. Keep your toenails trimmed carefully and moisturize dry skin to prevent cracking.
Temperature awareness matters. Test bath water with your elbow or a thermometer before putting your feet in — numb feet can't tell if water is dangerously hot. Avoid heating pads directly on numb feet. Keep feet warm with appropriate socks rather than direct heat sources.
Fall prevention should be a priority. Numb feet significantly impair your proprioception (sense of where your body is in space), which affects balance. Remove tripping hazards, install adequate lighting (especially for nighttime bathroom trips), and consider grab bars in the bathroom.
Frequently Asked Questions
Can foot numbness from neuropathy be reversed?
It depends on the cause and how early treatment begins. Numbness caused by vitamin B12 deficiency may partially or fully reverse with supplementation. Diabetic neuropathy numbness may stabilize or slow with tight blood sugar control but rarely fully reverses once established. Chemotherapy-induced numbness sometimes improves after treatment ends, though recovery can take months to years. The earlier you identify and address the underlying cause, the better your chances of recovery.

Why are my feet numb only at night?
Nighttime numbness has several potential explanations. For neuropathy, symptoms often feel worse at night because daytime distractions are removed and you become more aware of the sensations. For PAD, lying flat can reduce blood pressure at the extremities, worsening numbness. For sciatica, sleeping positions may compress the affected nerve root. If you notice numbness predominantly at night, mention this specific pattern to your doctor as it helps narrow the diagnosis.
Can numb feet cause falls?
Yes. Foot numbness significantly increases fall risk because your brain relies on sensory feedback from your feet to maintain balance. Studies show that people with peripheral neuropathy have a 15 to 25 times greater risk of falling compared to those with normal foot sensation. Fall prevention strategies including home modifications, balance exercises, and appropriate footwear are essential for anyone with persistent foot numbness.
How do I know if foot numbness is serious?
All persistent foot numbness deserves medical evaluation. Red flags that increase urgency include sudden onset (over hours rather than weeks), numbness spreading rapidly upward, accompanying weakness that causes tripping or foot drop, loss of bladder or bowel control, and visible skin changes like color changes or non-healing wounds. Even gradual numbness should be evaluated because early treatment of the underlying cause produces the best outcomes.
Is it possible to have neuropathy and PAD at the same time?
Yes, and this combination is especially common in people with diabetes. Diabetes damages both peripheral nerves (causing neuropathy) and blood vessels (contributing to PAD). When both conditions are present, foot numbness may be more severe and harder to distinguish because the vascular component adds to the nerve damage. A thorough workup including both nerve conduction studies and ankle-brachial index testing can identify whether one or both conditions are present.
Do I need to see a specialist for numb feet, or can my primary care doctor handle it?
Your primary care doctor is an excellent starting point. They can perform initial screening (monofilament test, ABI, basic blood work, physical exam) and often identify the most likely cause. Referrals to a neurologist make sense when the cause is unclear, when nerve conduction studies are needed, or when symptoms are progressing despite treatment. A vascular specialist is appropriate when PAD is suspected. Many people with straightforward diabetic neuropathy are managed effectively by their primary care doctor or endocrinologist.
The Bottom Line
Foot numbness is your body's signal that something in the nervous or vascular system needs attention. Whether it's neuropathy quietly damaging your peripheral nerves, PAD reducing blood flow, sciatica compressing a nerve root, or diabetes attacking through multiple pathways simultaneously — the cause matters because the treatment is different for each one.

Don't ignore persistent foot numbness or dismiss it as “just getting older.” While age-related changes are real, numb feet always have an identifiable cause — and most of those causes are treatable or at least manageable when caught early. Track your symptoms, note the patterns, and bring that information to your doctor. Your feet are worth the conversation.
Browse all our symptom guides for more help understanding your neuropathy symptoms and getting the right answers.


