
Browse all our types and causes of neuropathy guides for more articles like this one.
I'll never forget the first time someone described trigeminal neuralgia to me. She was sitting across from me at a support group meeting, holding her jaw gently, and she said: “It's like someone is holding a live wire to my face.” She paused, then added, “And nobody can see it.” That moment stuck with me — because trigeminal neuralgia is one of those conditions that is invisible to everyone except the person enduring it.
Trigeminal neuralgia (TN) — sometimes called tic douloureux — is widely considered one of the most excruciating pain conditions known in medicine. The pain strikes suddenly, often triggered by everyday actions like brushing your teeth, washing your face, or feeling a breeze. It can last seconds or minutes, but those moments feel like an eternity. And for many people, the fear of the next attack becomes almost as debilitating as the pain itself.
If you or someone you love is dealing with this type of facial nerve pain, I want you to know: you are not alone, and there are real treatment options that may help. Let's walk through what trigeminal neuralgia actually is, what causes it, how it's diagnosed, and the treatments that are making a difference for people right now.
What Is Trigeminal Neuralgia?
Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, also known as the fifth cranial nerve. This nerve is one of the largest in your head and is responsible for carrying sensation from your face to your brain. It has three branches, each covering a different area of the face:
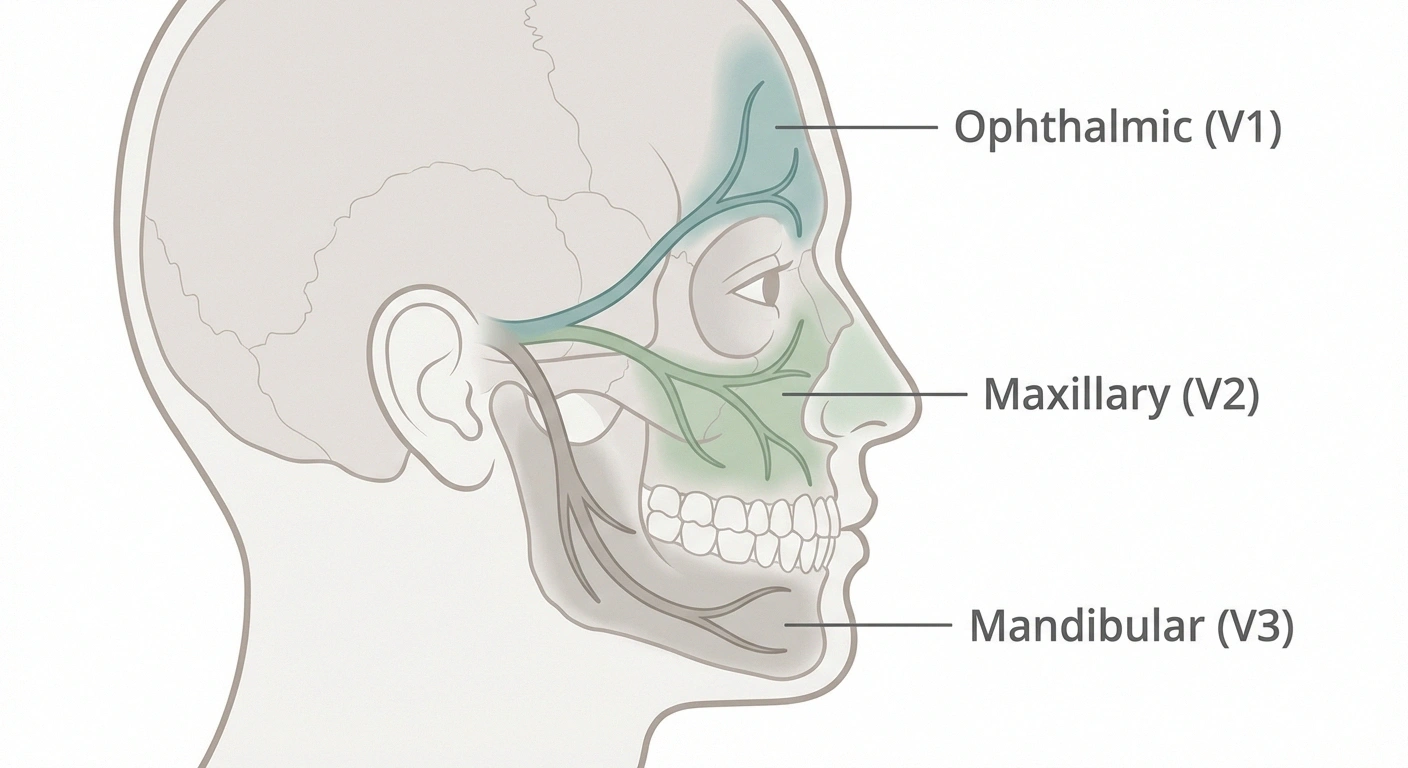
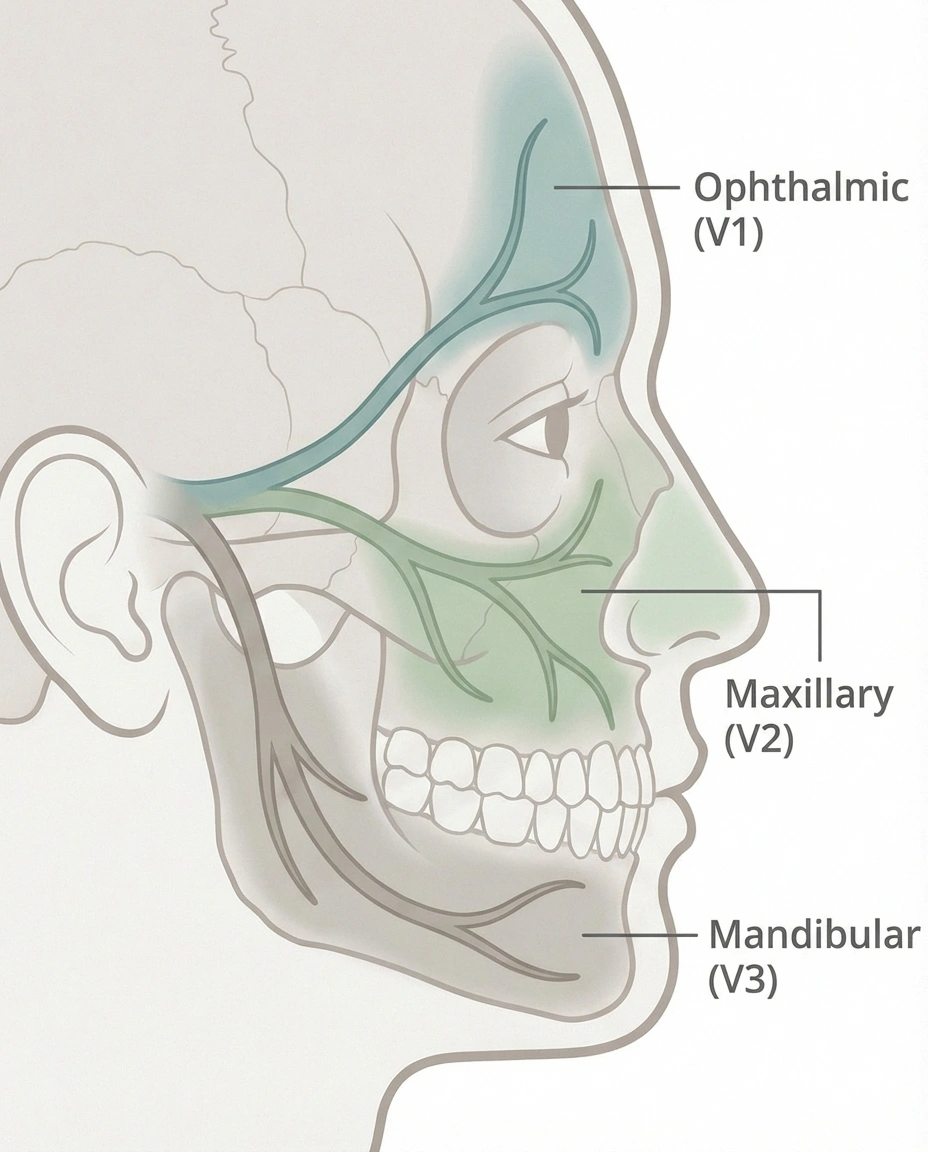
- Ophthalmic branch (V1): Covers the forehead, scalp, and upper eyelid
- Maxillary branch (V2): Covers the cheek, upper lip, upper jaw, teeth, and gums
- Mandibular branch (V3): Covers the lower jaw, lower lip, lower teeth, and gums
The maxillary and mandibular branches are the ones most commonly affected by trigeminal neuralgia, which is why so many people first think they have a dental problem. The pain typically affects one side of the face at a time, though in rare cases — particularly when multiple sclerosis is involved — it can occur on both sides.
According to the National Institute of Neurological Disorders and Stroke (NINDS), trigeminal neuralgia most commonly affects people over age fifty, and it is roughly twice as common in women as in men. An estimated one hundred and fifty thousand people are diagnosed with the condition each year in the United States.
What Does Trigeminal Neuralgia Feel Like?
People who live with trigeminal neuralgia often struggle to describe just how intense the pain is. Here are the most common descriptions:
Do You Recognize These Symptoms?
Sudden, electric shock-like jolts of pain on one side of the face
Pain triggered by brushing teeth, eating, or touching the face
Attacks lasting seconds to minutes, sometimes in rapid clusters
Pain in the cheek, jaw, teeth, gums, or lips
Burning or throbbing sensation between sharp attacks
Previous dental treatments that didn't relieve the pain
people diagnosed with trigeminal neuralgia each year in the U.S.
- Electric shock-like jolts through one side of the face
- Sharp, stabbing, shooting pain that arrives without warning
- Burning or throbbing sensations between attacks (more common in Type 2 TN)
- Pain that stops you mid-sentence or mid-bite
Individual attacks can last from a few seconds to about two minutes. But they often come in rapid-fire clusters — sometimes dozens of episodes per hour during a bad flare. Between flare periods, some people experience weeks or even months of complete remission. Others aren't so fortunate, and the pain becomes more constant and intense over time.
The condition has two recognized subtypes. Type 1 (TN1), sometimes called “classic” trigeminal neuralgia, involves sudden, intense, shock-like episodes of pain with pain-free intervals between attacks. Type 2 (TN2) involves a more constant burning or aching pain with occasional sharp episodes layered on top. Type 2 is often harder to treat and can be more emotionally exhausting because the pain rarely lets up completely.
Common Triggers: When Everyday Actions Become Painful
One of the most challenging aspects of trigeminal neuralgia is that some of the most ordinary parts of daily life can trigger an attack. People with TN often report that the following activities set off their pain:


- Brushing their teeth
- Washing or touching their face
- Shaving
- Applying makeup
- Eating or chewing
- Drinking (especially hot or cold beverages)
- Talking or smiling
- A light breeze blowing across the face
Because so many triggers are connected to basic self-care and social interaction, trigeminal neuralgia can lead to isolation. Some people avoid eating, stop brushing their teeth, or withdraw from conversations — not because they want to, but because the risk of triggering an attack feels too great. If that sounds familiar, please know that you're not being dramatic. This is a real, documented pattern, and your healthcare team should understand it.
What Causes Trigeminal Neuralgia?
In most cases, trigeminal neuralgia is caused by a blood vessel — usually the superior cerebellar artery — pressing against the trigeminal nerve at the base of the brain. This compression irritates the nerve and disrupts its normal function, causing it to “misfire” and send intense pain signals to the face.
There are three recognized categories based on the underlying cause:
- Classic TN: A blood vessel is compressing the trigeminal nerve root. This is the most common type.
- Secondary TN: Another condition is responsible — such as multiple sclerosis, a tumor, or an arteriovenous malformation. About fifteen percent of TN cases are secondary. People with secondary TN tend to be younger and may have pain on both sides of the face.
- Idiopathic TN: No clear cause can be identified even after thorough testing. This is the least common category.
Other potential triggers include facial trauma, stroke, and scalp tingling from nerve damage damage from surgical procedures. A 2021 practical guide published in Practical Neurology emphasized that improved MRI technology has made it easier to identify neurovascular compression, though some cases still defy explanation.
The Dental Misdiagnosis Problem
This is something I hear about far too often, and it deserves its own section. Because trigeminal neuralgia frequently causes pain in the jaw, teeth, and gums, many people are initially misdiagnosed with dental problems. Some undergo root canals, tooth extractions, or other dental procedures before anyone considers that a nerve condition may be responsible.
A retrospective study published in PMC found that a significant number of trigeminal neuralgia patients had teeth extracted due to misdiagnosis, sometimes multiple teeth, before receiving the correct diagnosis. The American Association of Endodontists has also acknowledged that trigeminal neuralgia should be considered in any case of facial or tooth pain that doesn't respond to standard dental treatment.
If you've had dental work that didn't relieve your facial pain, or if your pain has a sudden, electric-shock quality that feels different from a typical toothache, bring up the possibility of trigeminal neuralgia with your doctor or dentist. The right diagnostic approach can save you from unnecessary procedures.
How Is Trigeminal Neuralgia Diagnosed?
There's no single test that confirms trigeminal neuralgia. Diagnosis is typically based on a combination of:
- Detailed pain history: Your doctor will ask about the location, quality, duration, and triggers of your pain. The pattern — sudden, intense, one-sided, triggered by light touch — is highly characteristic of TN.
- Neurological examination: Your doctor will test sensation in different areas of your face to identify which branches of the trigeminal nerve are affected.
- MRI imaging: An MRI of the brain can reveal whether a blood vessel is compressing the trigeminal nerve. It can also rule out other causes like tumors or multiple sclerosis lesions.
In some cases, your doctor may also order nerve conduction studies or refer you to a neurologist or neurosurgeon for further evaluation. The key is to find a healthcare provider who is familiar with trigeminal neuralgia — because misdiagnosis can lead to months or years of unnecessary suffering.
Treatment Options for Trigeminal Neuralgia
The good news is that trigeminal neuralgia is treatable, and most people can find significant relief with the right approach. Treatment typically starts with medication and may progress to surgical options if medications stop working or cause intolerable side effects.
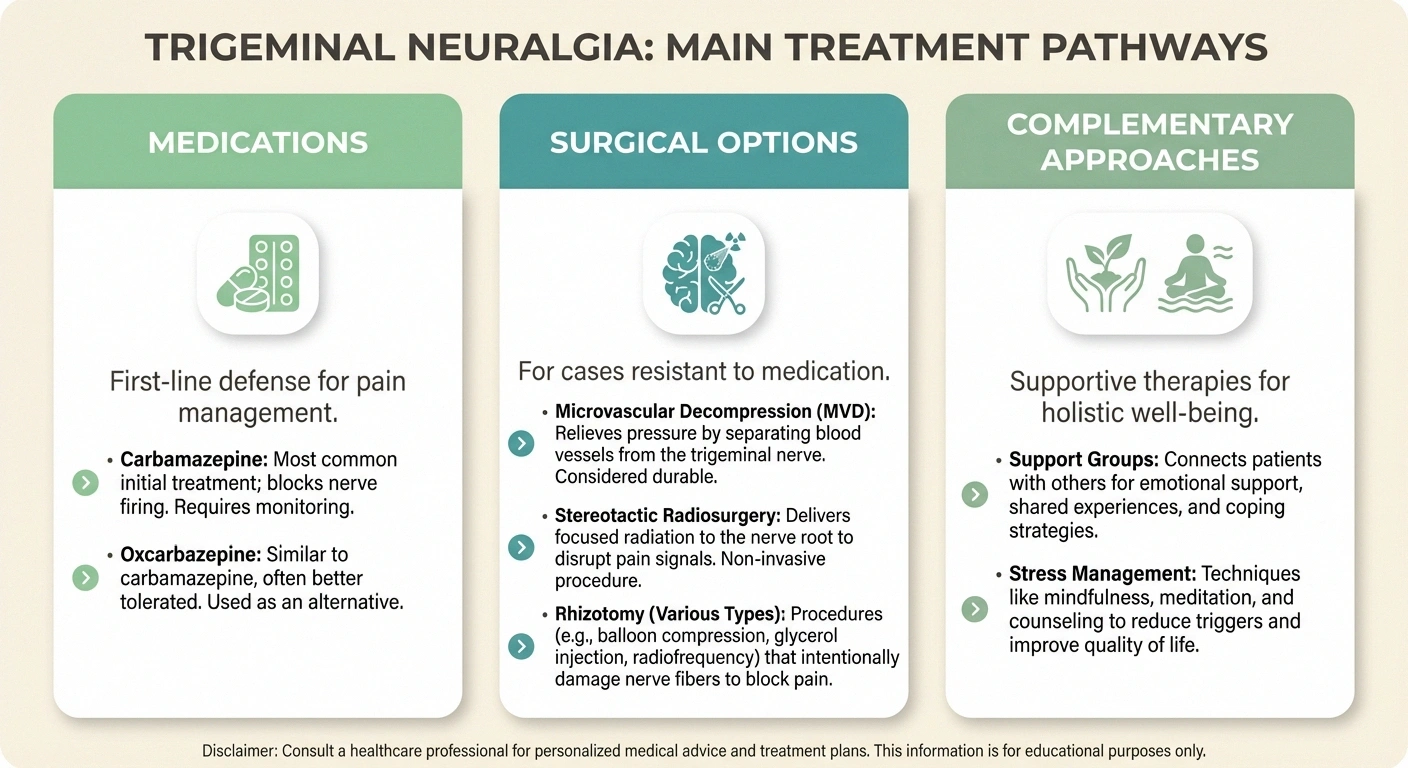
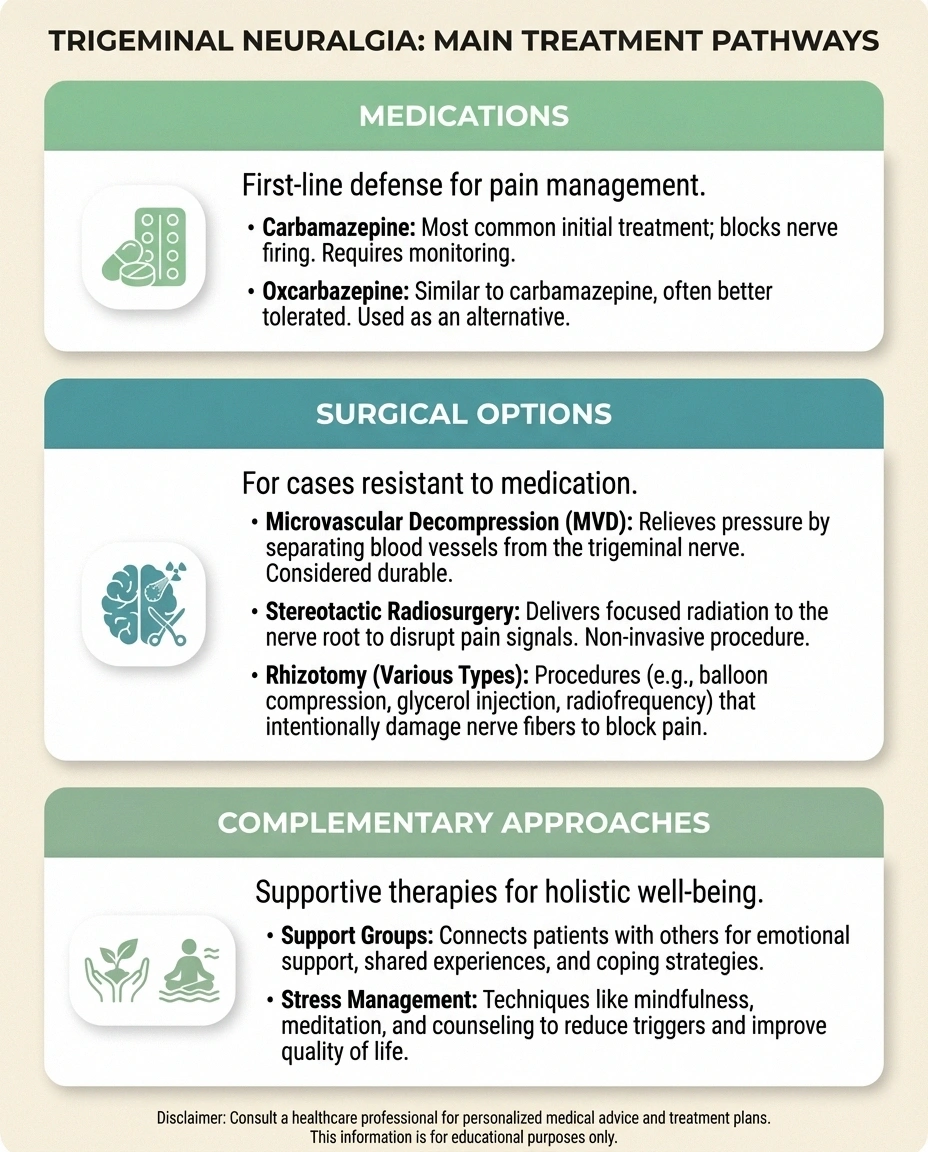
💊 Medications
First-line treatment. Carbamazepine is the gold standard. Effective for most people early on. May lose effectiveness over time.
🏥 MVD Surgery
Most effective long-term option. Relieves nerve compression directly. More invasive but best outcomes for lasting relief.
🎯 Less Invasive Procedures
Gamma Knife, rhizotomy options. Lower surgical risk. May cause some facial numbness. Pain relief may not be permanent.
Talk to Your Doctor
If you've had dental work that didn't relieve your facial pain — especially if the pain feels like an electric shock rather than a dull ache — ask your doctor or dentist about the possibility of trigeminal neuralgia. An MRI can help identify whether nerve compression is the cause.
Medications
Anticonvulsant medications are the first-line treatment for trigeminal neuralgia. These drugs work by calming overactive nerve signals:
- Carbamazepine (Tegretol): This is considered the gold standard for TN. According to the NINDS, carbamazepine is effective for most people, especially in the early stages of the condition. Common side effects include drowsiness, dizziness, and nausea.
- Oxcarbazepine (Trileptal): A close relative of carbamazepine that may cause fewer side effects for some people.
- Gabapentin (Neurontin): Sometimes used when carbamazepine isn't tolerated. Less effective as a standalone treatment for classic TN but may help in combination therapy.
- Pregabalin (Lyrica): Another option that may be tried if first-line medications don't provide sufficient relief.
- Baclofen: A muscle relaxant that may be used alongside anticonvulsants for additional pain control.
- Botulinum toxin A (Botox): Emerging research suggests that Botox injections near the trigeminal nerve may reduce pain episodes for some people.
It's important to know that common over-the-counter pain relievers like ibuprofen and acetaminophen are generally not effective for trigeminal neuralgia pain. Opioid medications are also typically ineffective for this type of nerve pain. If you've been self-treating with these and haven't found relief, that's another reason to talk to your doctor about TN specifically.
Surgical Options
When medications lose effectiveness over time — or cause side effects like cognitive difficulties, memory loss, or fatigue — surgery may be considered. Several procedures are available, and the best choice depends on your overall health, the type of TN you have, and your personal preferences:
- Microvascular decompression (MVD): This is the most invasive but also the most effective long-term surgical option. A surgeon moves or removes the blood vessel that's compressing the trigeminal nerve. According to the NINDS, MVD provides the longest-lasting pain relief and is the only procedure that aims to preserve normal facial sensation.
- Stereotactic radiosurgery (Gamma Knife): A focused beam of radiation targets the trigeminal nerve root. It's less invasive than MVD but pain relief may take weeks to develop and may not be permanent.
- Rhizotomy procedures: These intentionally damage the nerve fibers to block pain signals. Options include balloon compression, glycerol injection, and radiofrequency thermal lesioning. They're less invasive than MVD but typically result in some facial numbness, and pain may eventually return.
Every surgical approach carries risks, including facial numbness, hearing changes, and in rare cases, stroke. A thorough conversation with a neurosurgeon who specializes in trigeminal neuralgia is essential before making a decision.
Living With Trigeminal Neuralgia: Coping Strategies That Help
Beyond medical treatment, learning to manage daily life with trigeminal neuralgia is an ongoing process. Here are practical strategies that many people with TN find helpful:

- Know your triggers and plan around them. Keep a pain diary to identify your personal triggers. Some people find that eating soft foods, using an electric toothbrush on a low setting, or avoiding cold drafts helps reduce flare-ups.
- Protect your face from wind and cold. Many people with TN wear a scarf or face covering outdoors, even in mild weather, to prevent wind-triggered attacks.
- Don't neglect your mental health. Living with severe, unpredictable pain takes a psychological toll. Anxiety, depression, and social isolation are common among people with TN. Counseling, cognitive behavioral therapy, and chronic pain support groups can make a real difference.
- Connect with others who understand. Organizations like the Facial Pain Association offer resources, community forums, and support networks specifically for people with trigeminal neuralgia and related conditions.
- Communicate with your loved ones. Help the people around you understand that your pain is real, even though they can't see it. Simple explanations about triggers and flare patterns can help family and friends support you more effectively.
Trigeminal Neuralgia and Other Neuropathies: What's the Connection?
While trigeminal neuralgia specifically affects a cranial nerve in the face, it shares important features with peripheral neuropathy. Both involve damaged or dysfunctional nerves, both produce pain signals where there shouldn't be any, and both can be progressive if left untreated.

Some conditions that cause peripheral neuropathy — like diabetes and multiple sclerosis — can also contribute to trigeminal neuralgia. If you have diabetes and peripheral neuropathy or another form of nerve damage and begin experiencing facial pain, it's worth mentioning to your doctor. The trigeminal nerve is technically a cranial nerve rather than a peripheral one, but the underlying mechanisms of nerve dysfunction overlap considerably.
Similarly, people who develop post-herpetic neuralgia after shingles can sometimes experience trigeminal nerve involvement, particularly if the shingles outbreak affected the face or forehead.
When to See a Doctor
You should seek medical attention if you experience:
- Sudden, severe facial pain that feels like an electric shock
- Facial pain that keeps returning or gets worse over time
- Pain in your teeth, jaw, or cheek that hasn't responded to dental treatment
- Any facial pain accompanied by facial numbness, weakness, or vision changes
Don't wait for the pain to become unbearable. Early diagnosis and treatment can help prevent the condition from progressing and can significantly improve your quality of life.
Frequently Asked Questions About Trigeminal Neuralgia
Is trigeminal neuralgia the same as peripheral neuropathy?
Not exactly. Trigeminal neuralgia affects a cranial nerve in the face, while peripheral neuropathy involves nerves outside the brain and spinal cord, typically in the hands and feet. However, both conditions involve nerve dysfunction and share some overlapping causes, including diabetes and multiple sclerosis.
Can trigeminal neuralgia go away on its own?
Trigeminal neuralgia sometimes goes through periods of remission where pain disappears for weeks, months, or even years. However, for most people, the condition tends to return and may worsen over time. Treatment is generally recommended to manage the condition and prevent progression.
What is the best medication for trigeminal neuralgia?
Carbamazepine is widely considered the first-line medication for trigeminal neuralgia. It is effective for most people, particularly in the early stages. Oxcarbazepine is an alternative that may cause fewer side effects. Your doctor will work with you to find the medication and dosage that best controls your pain with the fewest side effects.
How is trigeminal neuralgia different from a toothache?
Trigeminal neuralgia pain is typically sudden, intense, and shock-like, lasting seconds to minutes. A toothache is usually more constant and throbbing. Trigeminal neuralgia pain is also triggered by light touch to the face rather than by biting down or temperature sensitivity in a specific tooth. If dental treatment has not resolved your pain, ask your doctor about the possibility of trigeminal neuralgia.
Is surgery for trigeminal neuralgia safe?
All surgical procedures carry some risk, but the procedures used for trigeminal neuralgia are well-established. Microvascular decompression has the best long-term outcomes and aims to preserve normal facial sensation. Less invasive options like radiosurgery and rhizotomy carry lower surgical risk but may result in some facial numbness. A neurosurgeon experienced with trigeminal neuralgia can help you weigh the risks and benefits for your specific situation.
Can stress make trigeminal neuralgia worse?
While stress does not directly cause trigeminal neuralgia, many people report that stress and anxiety can increase the frequency and severity of their pain episodes. Stress may lower your pain threshold and make you more sensitive to triggers. Managing stress through relaxation techniques, therapy, and support networks may help reduce flare-ups alongside medical treatment.
Moving Forward With Hope
Trigeminal neuralgia is one of the most intense pain conditions a person can face — but it is also one of the most treatable forms of facial pain. Whether you find relief through medication, surgery, or a combination of approaches, the most important first step is getting an accurate diagnosis from a healthcare provider who understands the condition.
Key Takeaway
Trigeminal neuralgia is one of the most intense pain conditions known — but it's also highly treatable. If facial pain hasn't responded to dental treatment, ask your doctor about trigeminal neuralgia. Early diagnosis leads to better outcomes.
If you're still searching for answers, if dental treatments haven't helped, or if you've been told the pain is “just stress” — please don't give up. Trigeminal neuralgia is real, it's documented, and there are specialists who focus specifically on treating it. You deserve to eat without fear, to feel a breeze without bracing yourself, and to live your life without the constant threat of that next bolt of pain.
As always, please talk to your doctor before starting or changing any treatment plan. This article is for educational purposes and is not a substitute for professional medical advice.


