
Vasculitic Neuropathy: When Blood Vessel Inflammation Damages Nerves
I receive messages from readers dealing with all kinds of neuropathy, but few are as confusing — or as frightening — as those from people diagnosed with vasculitic neuropathy. Unlike the gradual, symmetric tingling of diabetic neuropathy or the predictable pattern of chemotherapy-related nerve damage, vasculitic neuropathy often strikes suddenly and unpredictably. One day your foot drops, or one hand goes numb without warning. Understanding what's happening inside your blood vessels is the key to making sense of this condition.
What Is Vasculitic Neuropathy?
Vasculitic neuropathy is nerve damage caused by inflammation of the blood vessels (vasculitis) that supply your peripheral nerves. When these tiny vessels become inflamed, they narrow or become blocked, cutting off the blood supply that your nerves need to function. Without adequate blood flow, nerve fibers become ischemic — essentially starved of oxygen — and begin to die.
Think of it this way: your peripheral nerves are like electrical cables that need a constant power supply. The blood vessels around them are the power lines. When vasculitis damages those blood vessels, the cables lose power and stop working — sometimes suddenly and in seemingly random patches across your body.
According to a review in Therapeutic Advances in Neurological Disorders, approximately 34% of patients with vasculitis have disease restricted to the peripheral nervous system. This means that for a significant number of people, nerve damage may be the primary or only manifestation of blood vessel inflammation.
How Vasculitis Damages Your Nerves
The mechanism behind vasculitic neuropathy explains its distinctive clinical pattern. Your peripheral nerves are supplied by a network of tiny blood vessels called the vasa nervorum. When the immune system attacks these vessels — which is what vasculitis is — the vessel walls become inflamed, thickened, and sometimes completely blocked.
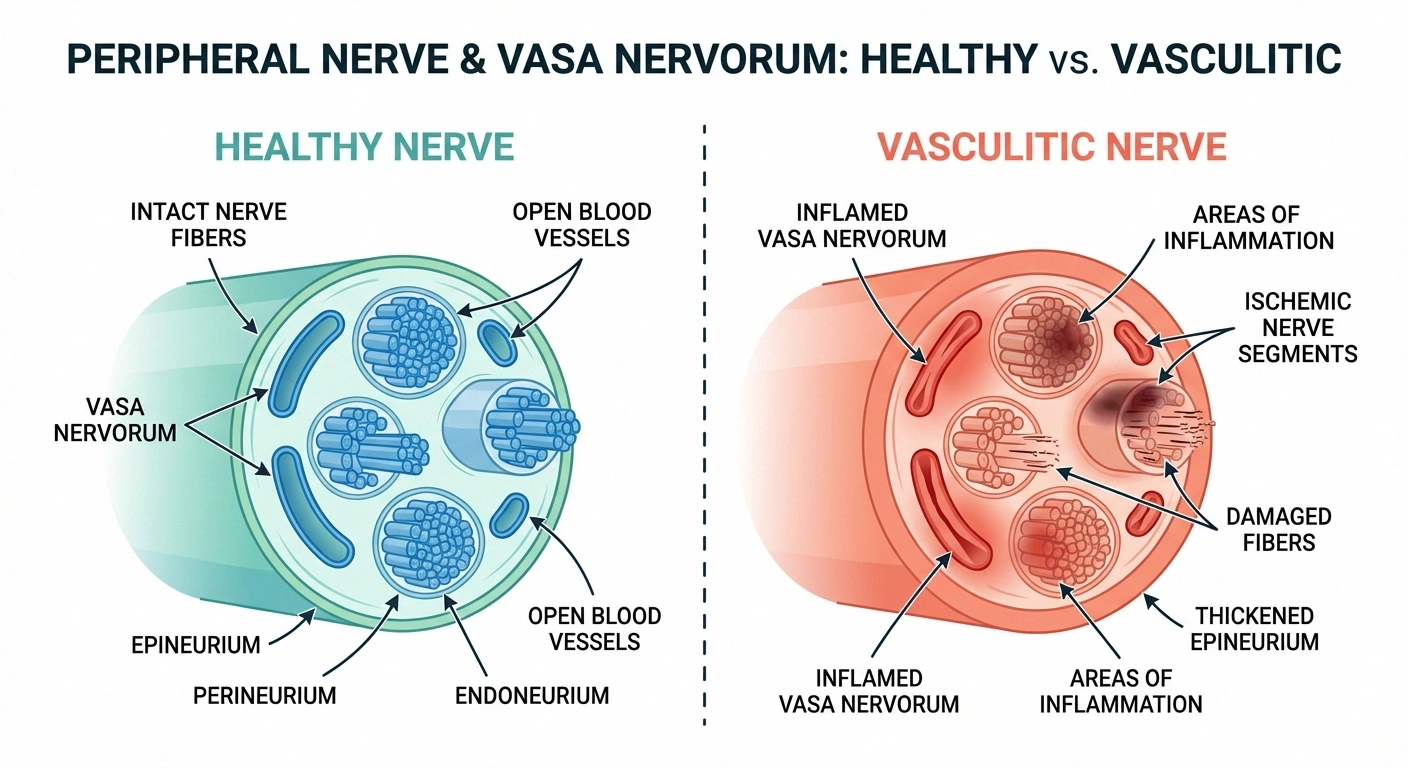
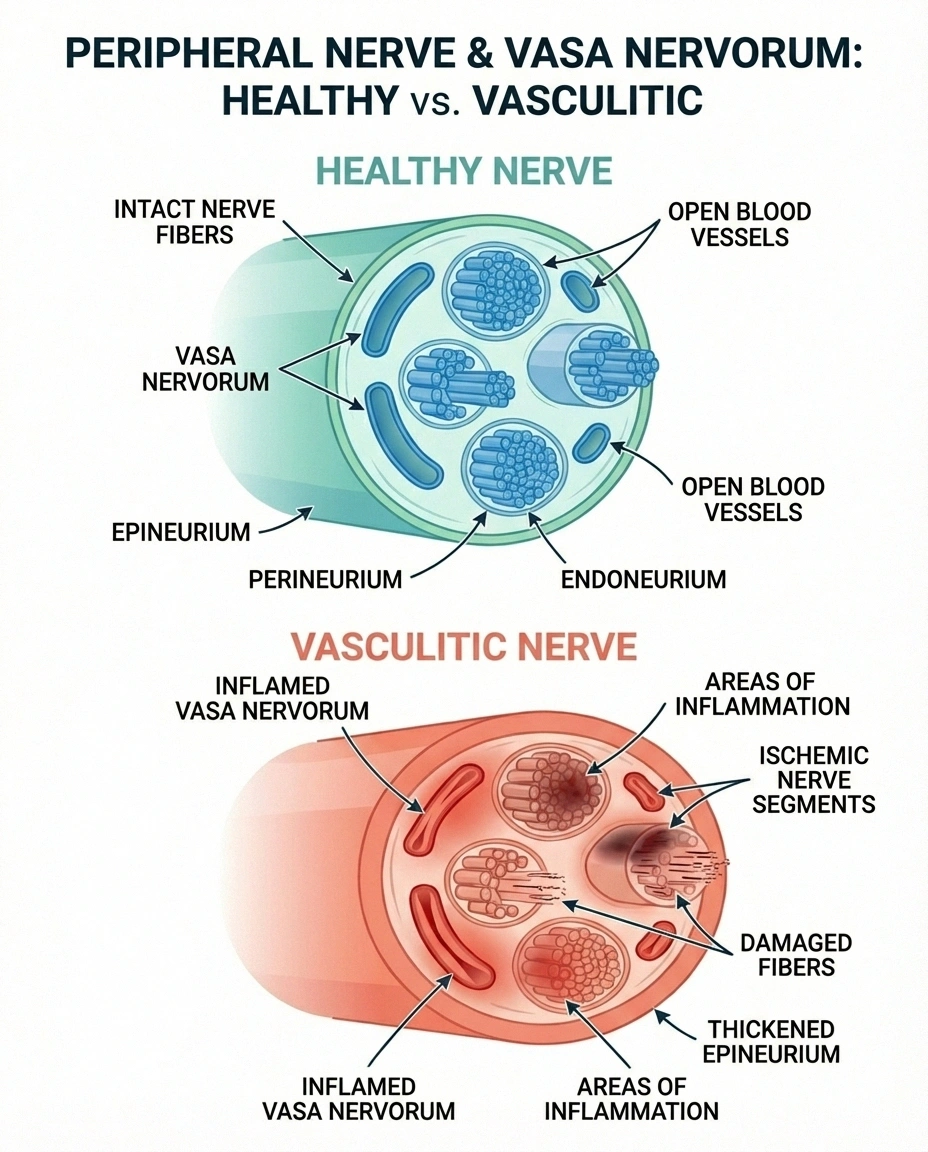
This isn't a diffuse, gradual process like the nerve damage from diabetes. Instead, it tends to affect individual nerves or nerve segments in a patchy pattern, depending on which specific blood vessels are inflamed. The nerve damage occurs through ischemia (oxygen deprivation) and sometimes infarction (complete tissue death) of nerve segments.
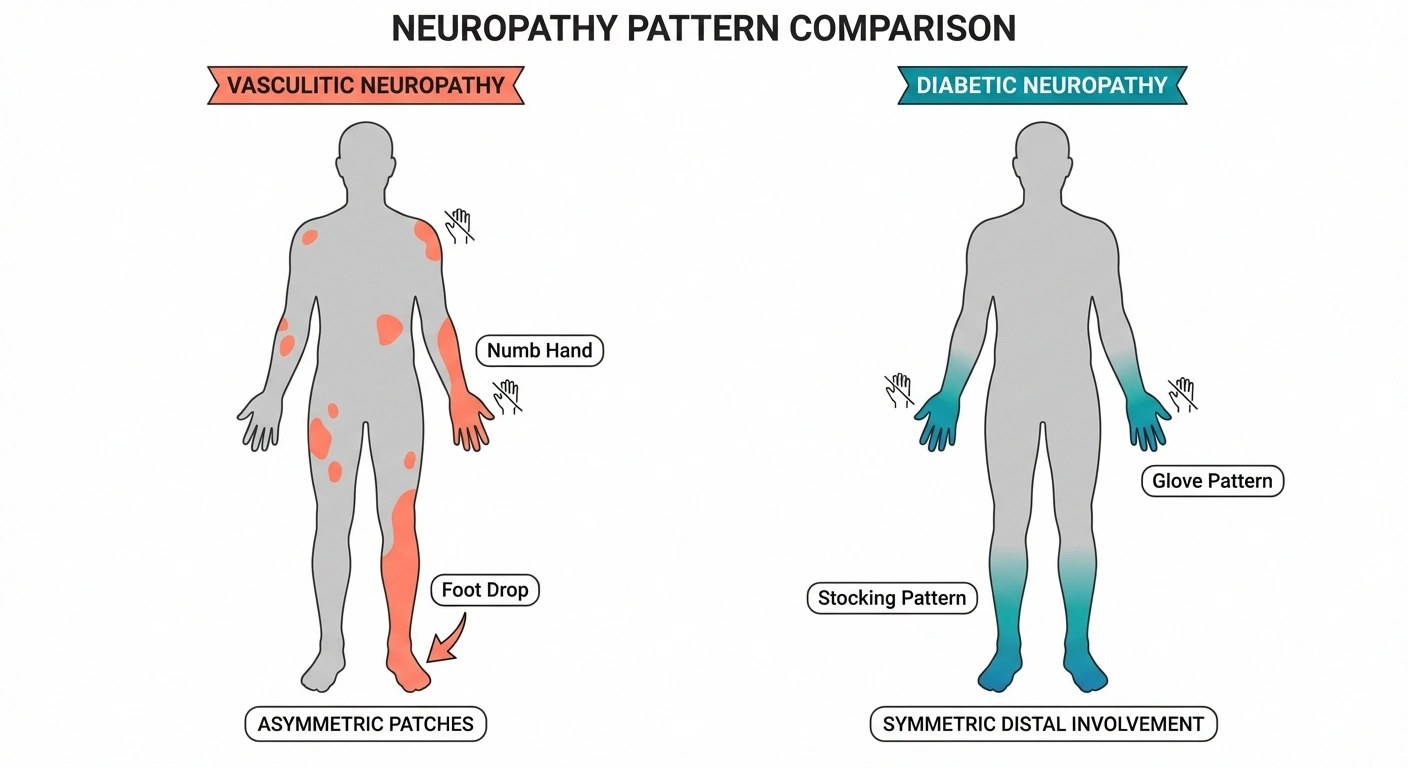
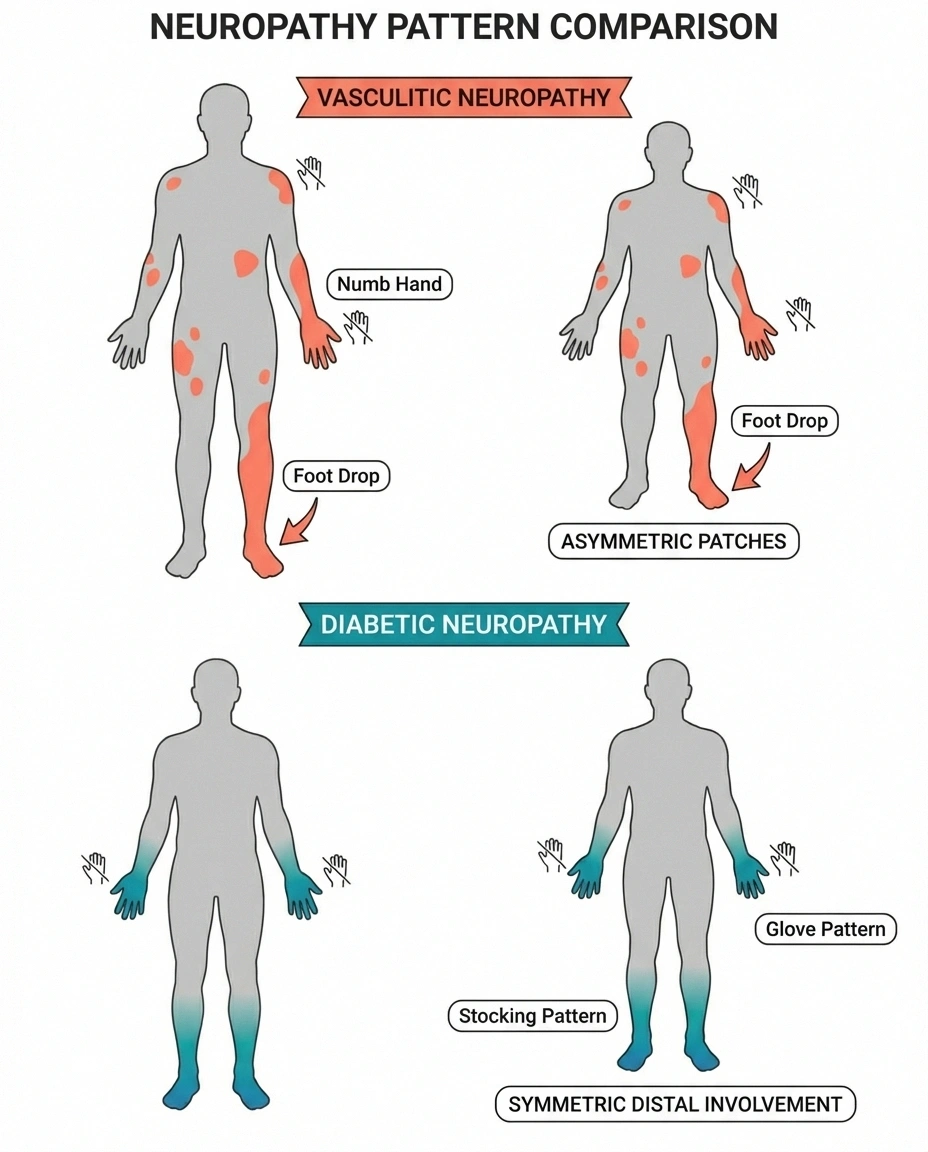
This is why vasculitic neuropathy often presents as mononeuritis multiplex — damage to multiple individual nerves in different parts of the body, rather than the symmetric “stocking-and-glove” pattern typical of diabetic neuropathy or alcohol-related nerve damage.
Types of Vasculitic Neuropathy
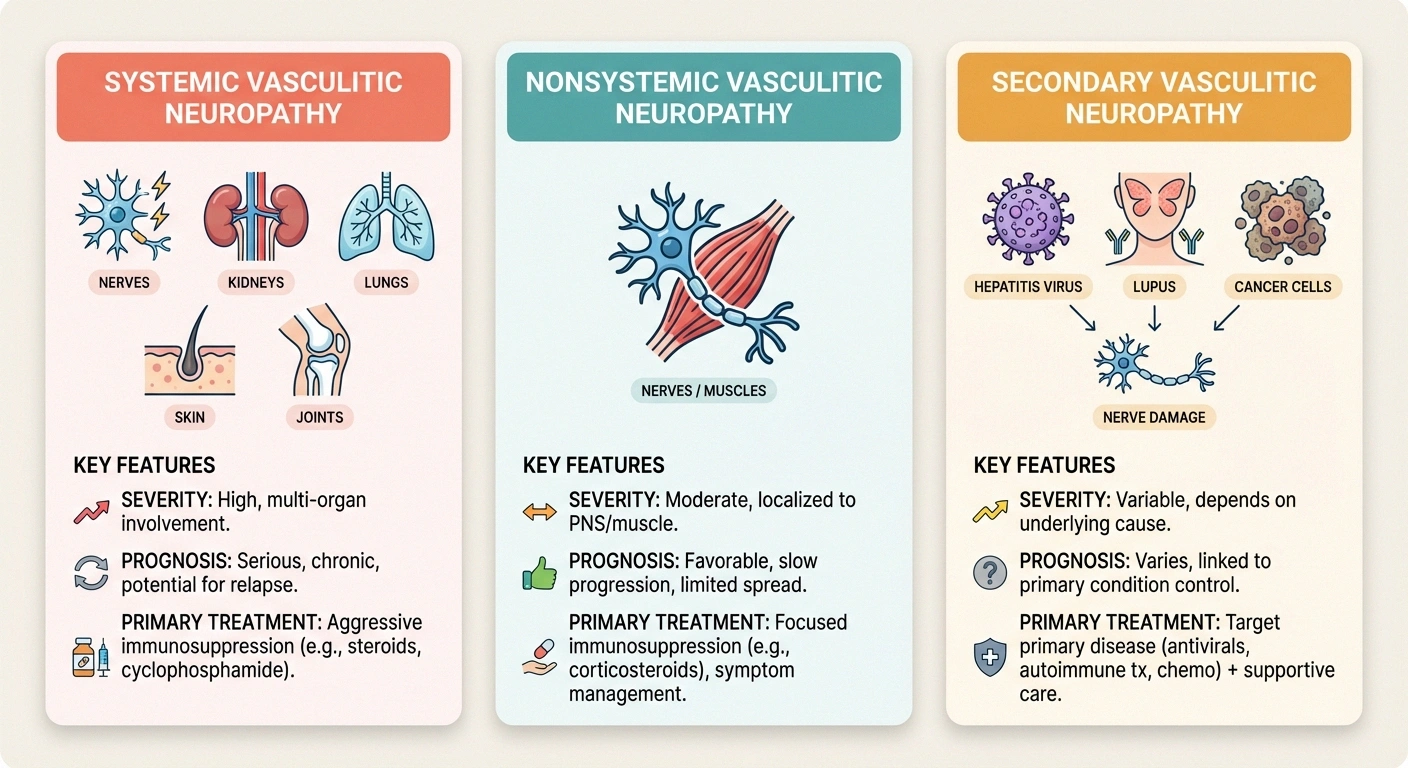
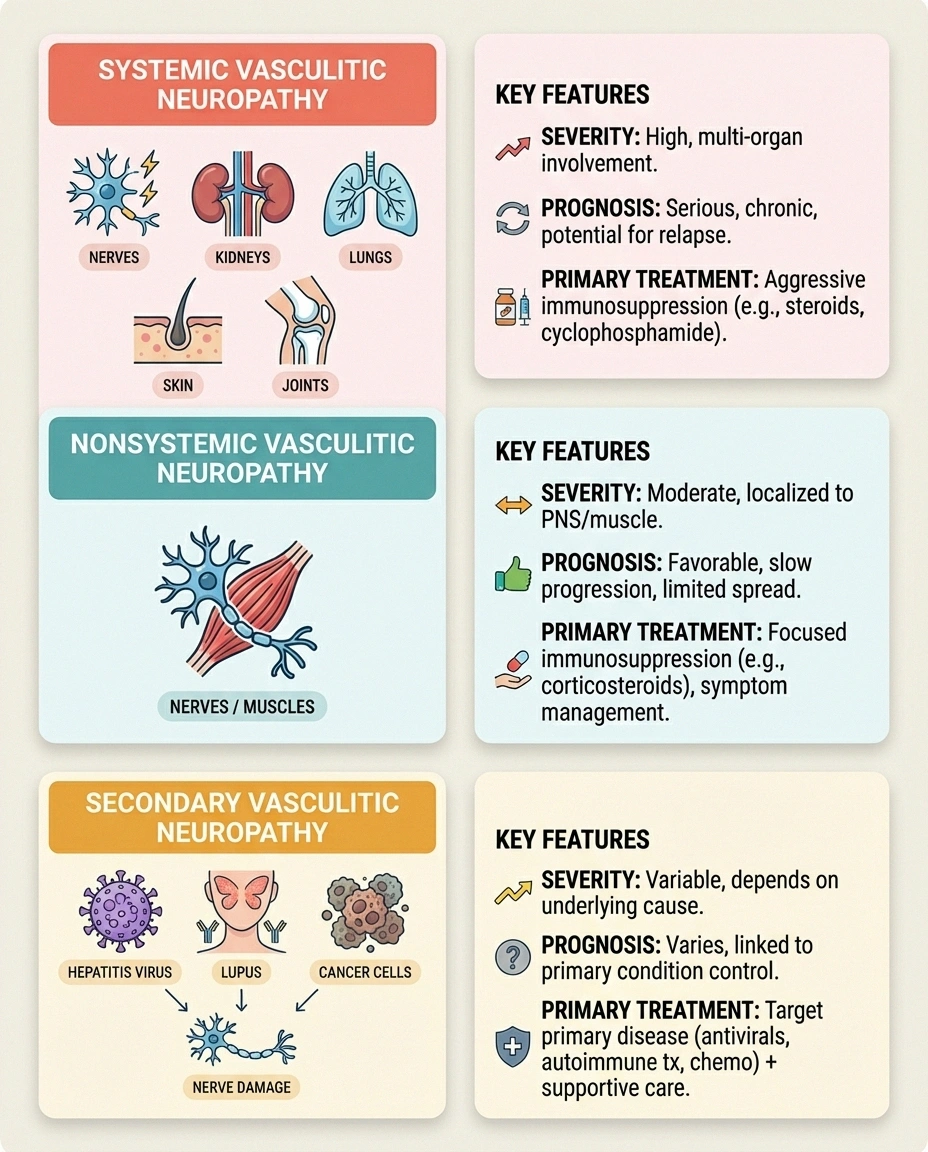
Vasculitic neuropathy falls into three main categories, and knowing which type you have is critical because it determines treatment approach and prognosis.
• More severe, potentially life-threatening
• Requires aggressive immunosuppression
• Higher relapse rates (11-60%)
• Less morbidity, not life-threatening
• May respond to steroids alone
• Rarely progresses to systemic disease
• Treat underlying cause first
• Prognosis depends on primary condition
• Hepatitis B/C are common triggers
Systemic vasculitic neuropathy (SVN) occurs when neuropathy is part of a whole-body vasculitis that also affects other organs — skin, kidneys, lungs, joints, or gut. Conditions that cause SVN include polyarteritis nodosa (PAN), granulomatosis with polyangiitis (formerly Wegener's), eosinophilic granulomatosis with polyangiitis (formerly Churg-Strauss), microscopic polyangiitis, and rheumatoid vasculitis.
Nonsystemic vasculitic neuropathy (NSVN) is confined entirely to the peripheral nerves and sometimes muscles. There's no involvement of other organs. According to Medscape, NSVN typically causes less morbidity than systemic forms and is generally not life-threatening. Importantly, patients with well-defined NSVN who receive treatment almost never go on to develop multi-system vasculitis.
Secondary vasculitic neuropathy develops as a consequence of another condition — most commonly infections (hepatitis B or C, HIV), connective tissue diseases (lupus, Sjögren's syndrome), or certain cancers (lymphoma, leukemia). In these cases, treating the underlying disease is the first priority.
Recognizing the Symptoms
Vasculitic neuropathy has a distinctive presentation that sets it apart from other types of nerve damage. The hallmark feature is its asymmetric pattern — it doesn't affect both sides of your body equally or follow the typical “longest nerves first” pattern of most neuropathies.
Typical symptoms include:
- Sudden onset of weakness or numbness in a specific nerve distribution — such as foot drop (difficulty lifting the front part of your foot), wrist drop, or numbness along one side of a hand
- Burning or sharp pain that may be severe and often precedes or accompanies the weakness
- Stepwise progression — new nerves become affected over days to weeks, with each episode adding to the damage. You might develop foot drop on the left side, then a week later lose sensation in two fingers of the right hand.
- Asymmetric involvement — unlike diabetic neuropathy where both feet are affected similarly, vasculitic neuropathy typically hits one limb harder than the other
If the vasculitis is systemic, you may also experience fever, fatigue, unexplained weight loss, joint pain, skin rashes or ulcers, or kidney problems. These systemic symptoms are important clues that can help your doctor identify the underlying cause.
The Brighton Collaboration notes that vasculitic neuropathies typically manifest with subacute stepwise progression, though some patients experience more insidious chronic progression over many years.
Getting Diagnosed
Diagnosing vasculitic neuropathy requires a combination of clinical evaluation, nerve testing, blood work, and often a tissue biopsy. It can be a complex diagnostic journey, which is why seeing a neurologist experienced with this condition is important.

Electromyography (EMG) and nerve conduction studies are usually the first step. These tests can confirm nerve damage and, importantly, show the pattern of involvement. Vasculitic neuropathy typically shows an asymmetric pattern of axonal damage affecting multiple individual nerves — a pattern called mononeuritis multiplex.
Blood tests help identify the underlying cause of vasculitis and rule out other conditions. These typically include inflammatory markers (ESR, CRP), ANCA antibodies (associated with certain types of vasculitis), cryoglobulins, hepatitis B and C testing, complement levels, and rheumatoid factor and ANA.
Nerve and muscle biopsy is often the definitive diagnostic test. A combined sural nerve and peroneal muscle biopsy can directly show inflammation in the blood vessel walls supplying the nerve, along with evidence of nerve fiber damage from ischemia. Johns Hopkins Peripheral Nerve Center notes that histopathological evaluation through biopsy remains a cornerstone of diagnosis.
Skin biopsy can evaluate cutaneous nerve innervation and is less invasive than nerve biopsy. It may show reduced nerve fiber density and sometimes evidence of small vessel inflammation.
Treatment: Controlling the Inflammation
Unlike many types of neuropathy where treatment focuses mainly on symptom management, vasculitic neuropathy has a treatable cause — the inflammation in your blood vessels. Stopping the immune attack on your blood vessels is the primary goal, and when treatment is started early, nerve function may partially or fully recover.
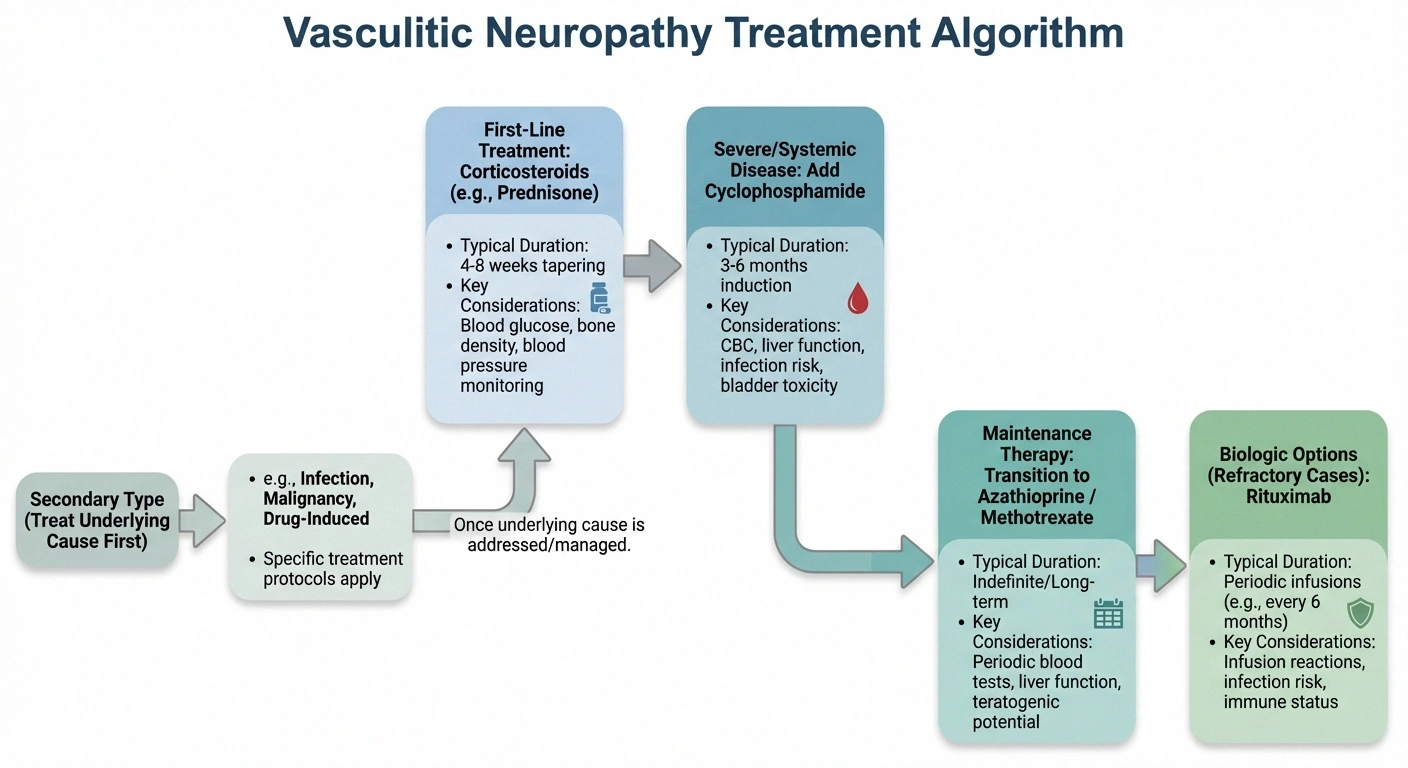
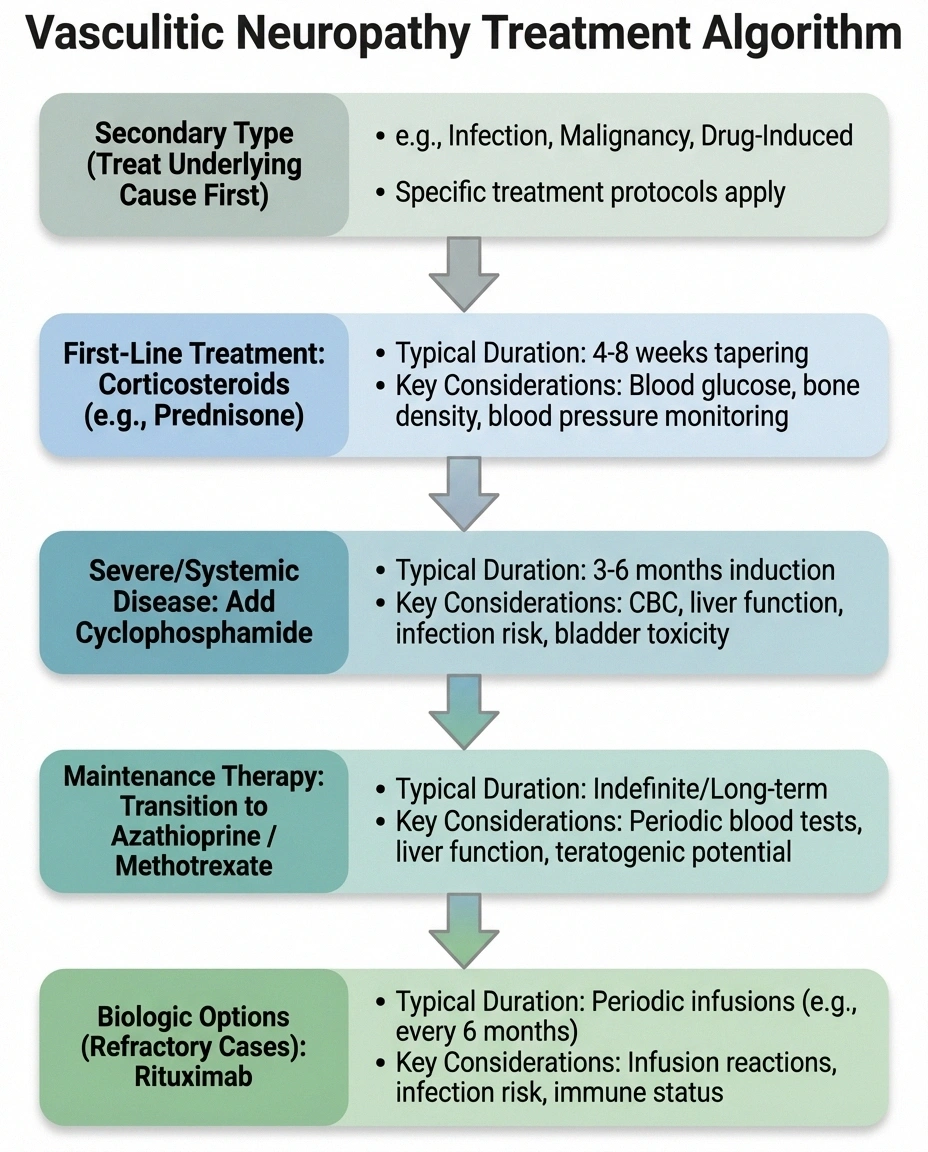
Corticosteroids are the first-line treatment for most forms of vasculitic neuropathy. High-dose prednisone is typically started immediately to rapidly suppress the inflammation. As noted in the Oxford Rheumatology review, treatment generally involves combination therapy (glucocorticoids plus another immunosuppressant), after which motor and sensory recovery are likely to occur — albeit slowly.
Cyclophosphamide is often added for severe or systemic vasculitic neuropathy, particularly when there's evidence of organ involvement beyond the nerves. Research published on Medscape indicates that aggressive early treatment with cyclophosphamide may prevent relapse, while patients treated with prednisone alone show higher relapse rates.
Other immunosuppressive medications used in vasculitic neuropathy include azathioprine (often used as a maintenance therapy after initial treatment with cyclophosphamide), methotrexate, mycophenolate mofetil, and rituximab (a biologic agent increasingly used for ANCA-associated vasculitis).
For nonsystemic vasculitic neuropathy, treatment may be less aggressive. Some patients with NSVN respond well to corticosteroids alone, though many neurologists add a steroid-sparing agent to reduce the long-term side effects of prednisone.
For secondary vasculitic neuropathy, treating the underlying condition is essential. Hepatitis-associated vasculitis may require antiviral therapy. Lupus-related vasculitis needs treatment of the lupus itself. Cancer-associated vasculitis may improve with treatment of the underlying malignancy.
Managing Neuropathy Symptoms
While immunosuppressive treatment addresses the root cause, you'll still need to manage the neuropathy symptoms that the vasculitis has already caused. Nerve recovery is possible but slow — nerves regenerate at approximately 1 millimeter per day, which means recovery can take months to years.
Pain management may include gabapentin or pregabalin for nerve pain, duloxetine for pain and mood support, topical treatments like lidocaine patches, and in some cases, referral to a pain specialist for more comprehensive management.
Physical therapy is critical, especially if you have motor involvement like foot drop or wrist drop. A physical therapist can provide strengthening exercises, gait training, and balance work. Ankle-foot orthoses (AFOs) may be recommended for foot drop while waiting for nerve recovery.
Foot care is essential if sensation is reduced. Daily foot inspections, properly fitted shoes, and careful attention to skin integrity help prevent ulcers and injuries. If you also have diabetes, foot care becomes even more critical.
Recovery and Prognosis
The outlook for vasculitic neuropathy depends largely on the type and how quickly treatment begins. The Oxford Rheumatology review reports that motor and sensory recovery is likely with appropriate treatment, though the patient may be left with chronic neuropathic pain.

Key factors that influence your prognosis include:
- Speed of diagnosis and treatment — The sooner inflammation is controlled, the less nerve damage accumulates. Early treatment is the single most important factor in outcome.
- Type of vasculitis — NSVN generally has a better prognosis than systemic forms. Secondary vasculitis depends on the treatability of the underlying condition.
- Severity of nerve damage at diagnosis — Nerves that are only partially damaged have a better chance of recovery than those that have been completely infarcted.
- Response to treatment — Some patients respond quickly to immunosuppression, while others require multiple medication adjustments.
Relapse is a real concern. The Medscape review notes relapse rates of 11-60% in systemic vasculitides. This means ongoing monitoring is essential even after you've responded to treatment. Most patients require immunosuppressive therapy for at least 18-24 months, and some need long-term maintenance treatment.
Living with Vasculitic Neuropathy
Living with vasculitic neuropathy means managing both a chronic autoimmune condition and the nerve damage it has caused. This dual reality requires an organized approach to your care.
☐ ANCA levels (if ANCA-associated) to monitor disease activity
☐ Kidney function tests — many vasculitides can affect kidneys
☐ Periodic EMG/NCS to track nerve recovery or new damage
☐ Bone density screening if on long-term corticosteroids
☐ Blood pressure and glucose monitoring (steroid side effects)
☐ Infection screening — immunosuppression increases infection risk
☐ Symptom journal tracking new neurological symptoms, pain levels, and energy
- Keep a detailed symptom journal — Track your nerve symptoms along with any systemic symptoms like joint pain, skin changes, or fatigue. This helps your doctor detect relapses early.
- Attend all follow-up appointments — Regular monitoring with blood tests and nerve function assessments is essential to detect relapse and adjust treatment.
- Understand your medications — Immunosuppressive drugs have significant side effects including increased infection risk. Know what to watch for and when to contact your doctor. Ask your doctor about monitoring schedules and warning signs.
- Maintain overall health — Good nutrition, regular exercise (adapted to your abilities), adequate sleep, and stress management all support your immune system and nerve health.
- Seek support — Support groups for vasculitis or neuropathy can connect you with others who understand your experience. Organizations like the Vasculitis Foundation provide patient resources and support networks.
When to Seek Urgent Medical Attention
Vasculitic neuropathy can be a medical emergency in certain situations. Seek immediate medical care if you experience sudden new weakness or numbness (especially foot drop or wrist drop), rapidly worsening symptoms over hours to days, systemic symptoms like high fever, bloody urine, or severe abdominal pain alongside neurological changes, or signs of infection while on immunosuppressive therapy (fever, chills, persistent cough). These may indicate a vasculitis flare, medication side effects, or other serious complications that need prompt evaluation.

Frequently Asked Questions
Is vasculitic neuropathy an autoimmune disease?
Yes, in most cases. Vasculitis is an autoimmune process where the immune system mistakenly attacks blood vessel walls. When this affects the blood vessels supplying peripheral nerves, it causes vasculitic neuropathy. Some forms are triggered by infections or medications rather than a primary autoimmune process, but the inflammatory mechanism is similar.
Can vasculitic neuropathy be cured?
The underlying vasculitis can often be controlled with immunosuppressive treatment, and nerve damage may partially or fully recover once inflammation is stopped. However, “cured” may not be the right word — most patients need ongoing treatment for months to years, and relapse is possible. The goal is sustained remission with manageable treatment side effects.
How is vasculitic neuropathy different from diabetic neuropathy?
Diabetic neuropathy typically causes symmetric symptoms starting in the feet and hands (stocking-and-glove pattern) and progresses gradually. Vasculitic neuropathy affects individual nerves asymmetrically, often with sudden onset. Diabetic neuropathy is caused by metabolic damage from high blood sugar, while vasculitic neuropathy is caused by inflammatory destruction of blood vessels. The treatment approaches are fundamentally different.
What tests diagnose vasculitic neuropathy?
Diagnosis typically requires EMG and nerve conduction studies to confirm nerve damage pattern, blood tests for inflammatory markers and autoantibodies, and often a nerve and muscle biopsy to directly confirm vasculitis. MRI of the nerves and skin biopsy may also contribute to the diagnosis.
How long does recovery take?
Nerve recovery from vasculitic neuropathy is slow. Peripheral nerves regenerate at about 1 millimeter per day, which means recovery can take 6 to 18 months or longer depending on the severity and location of nerve damage. Some patients continue to show improvement for up to 2 years after treatment begins. Motor recovery (strength) tends to be more complete than sensory recovery, and chronic neuropathic pain may persist even with good nerve regeneration.
Will I need to take immunosuppressive drugs forever?
Not necessarily, but many patients need treatment for at least 18 to 24 months. After achieving remission, your doctor will gradually taper your medications while monitoring for relapse. Some patients with nonsystemic vasculitic neuropathy can eventually stop treatment entirely, while those with certain systemic forms may need long-term maintenance therapy. This decision is highly individualized.
Moving Forward with Knowledge
Vasculitic neuropathy is one of the more treatable forms of neuropathy because the underlying cause — inflammation — can be addressed directly. The key is early recognition and aggressive treatment. If you're experiencing sudden, asymmetric nerve symptoms, particularly with any systemic signs of inflammation, don't delay seeking evaluation. The faster the inflammation is controlled, the better the chance for nerve recovery.
Talk to your doctor about your long-term outlook and what monitoring schedule makes sense for your situation. Understanding your condition puts you in the best position to advocate for the care you need.
Browse all our types and causes guides to learn more about different forms of neuropathy.


