
Here's an irony that frustrates me: metformin is one of the best medications for managing type 2 diabetes — and managing diabetes is one of the most important things you can do to prevent neuropathy. But metformin itself can cause the very nerve damage it's supposed to help prevent, through a sneaky back door called vitamin B12 depletion.
If you take metformin and you're experiencing numbness, tingling, or burning in your feet, don't assume it's “just diabetic neuropathy.” It might be. But it might also be a fixable B12 deficiency caused by your medication — and telling the difference matters, because one is progressive and the other is treatable.
How Metformin Depletes Vitamin B12
Metformin doesn't attack B12 directly. Instead, it interferes with how your body absorbs it. Vitamin B12 absorption is a multi-step process that depends on a protein called intrinsic factor binding to the vitamin in your gut, and that complex then attaching to receptors in the terminal ileum (the end of your small intestine) through a calcium-dependent process.
Metformin disrupts this calcium-dependent binding step. Research published in Diabetes, Obesity and Metabolism describes how metformin interferes with the calcium-dependent binding of the intrinsic factor-B12 complex to the cubam receptor — essentially preventing the final step of B12 absorption.
The result: even if you're eating plenty of B12-rich foods, your body can't fully absorb them. Over months and years, your B12 stores gradually deplete. A large-scale study using the NIH's All of Us research database found that the risk of B12 deficiency increases approximately 3% per year after starting metformin.
How Common Is This Problem?
More common than most patients — and some doctors — realize. The numbers vary by study, but the picture is consistent:
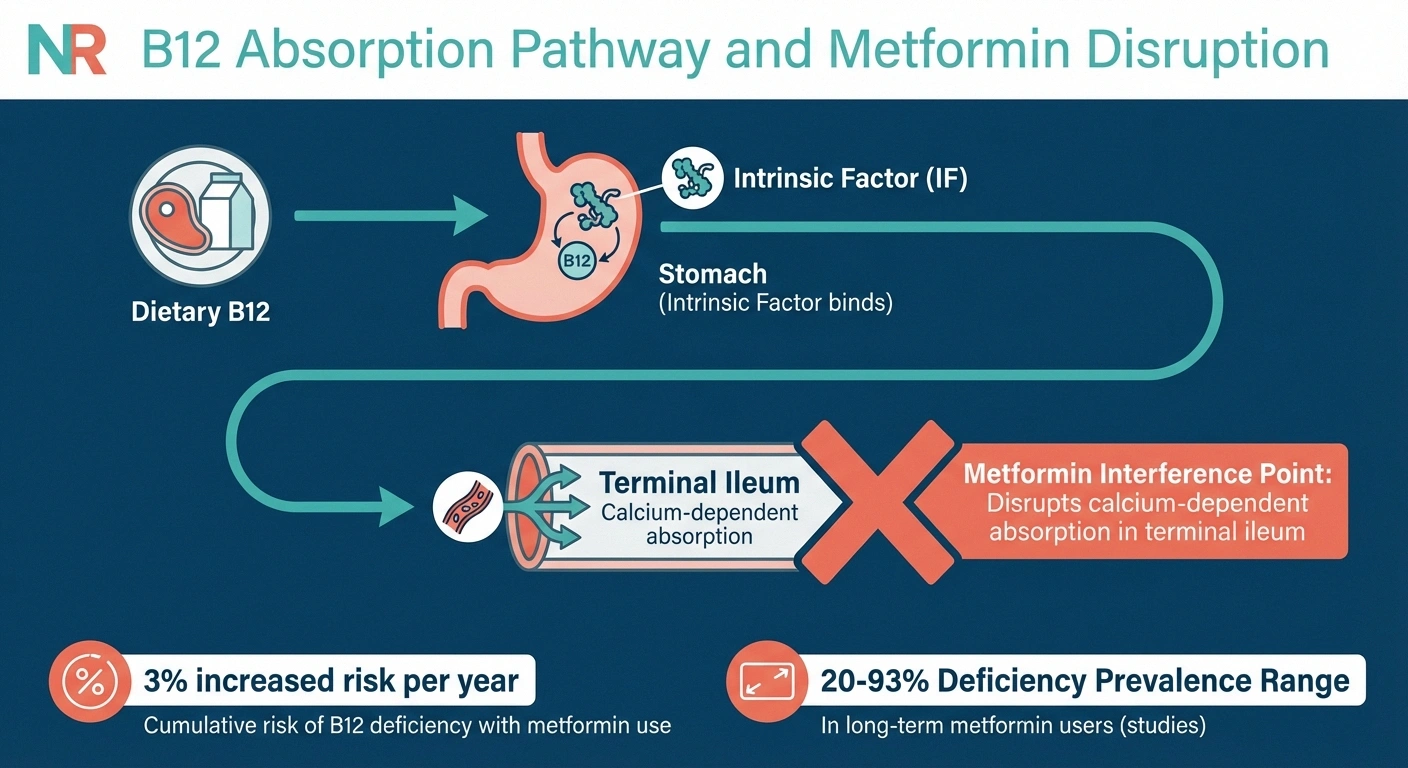
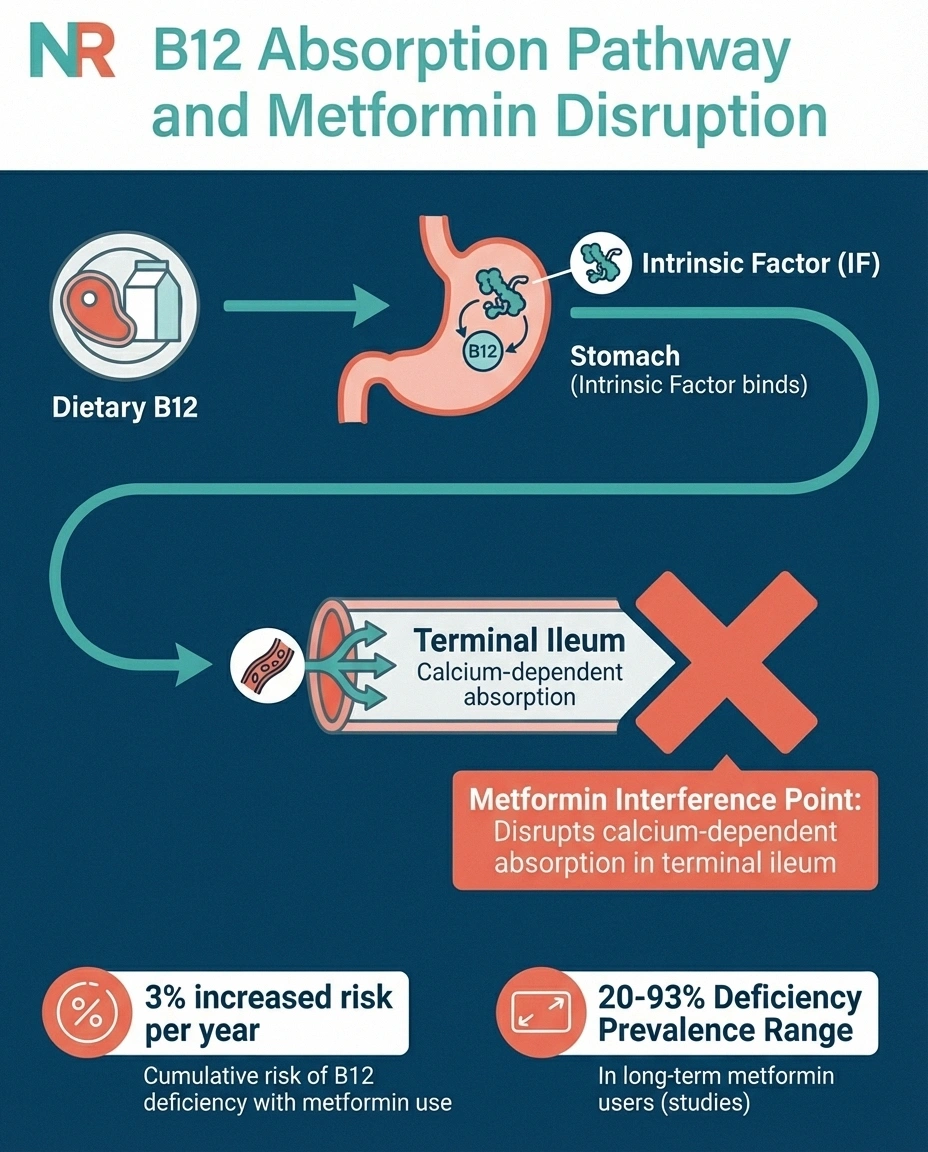
A 2024 narrative review in the Irish Journal of Medical Science reported that B12 deficiency prevalence in diabetic patients on metformin has been documented as high as 93% in some studies. While that upper range comes from a specific population, even conservative estimates place the rate at 20-30% — meaning at least one in five long-term metformin users develops clinically meaningful B12 depletion.
The UK's Medicines and Healthcare products Regulatory Agency (MHRA) issued updated guidance in 2022 explicitly warning that decreased B12 levels are a “known consequence of long-term treatment with metformin” and recommending monitoring to avoid permanent symptoms.
Yet despite these warnings, routine B12 monitoring isn't universally practiced. Many patients take metformin for years without ever having their B12 levels checked.
Metformin-Induced B12 Neuropathy vs. Diabetic Neuropathy
This is where things get clinically tricky. Both metformin-related B12 deficiency and diabetic neuropathy can cause numbness, tingling, and burning in the feet. The symptoms overlap significantly, which means one can mask the other — or worse, a treatable B12 deficiency gets mislabeled as irreversible diabetic neuropathy.
☑️ Daily dose of 2,000 mg or higher
☑️ Age 65 or older
☑️ Also taking a proton pump inhibitor (omeprazole, etc.)
☑️ Vegetarian or vegan diet
☑️ Previous stomach or intestinal surgery
A case report in Southern Medical Journal highlighted this exact problem: “Vitamin B12 deficiency, which may present without anemia and as a peripheral neuropathy, is often misdiagnosed as diabetic neuropathy, although the clinical findings are usually different.”
There are some differences to watch for, though they're not always clear-cut:
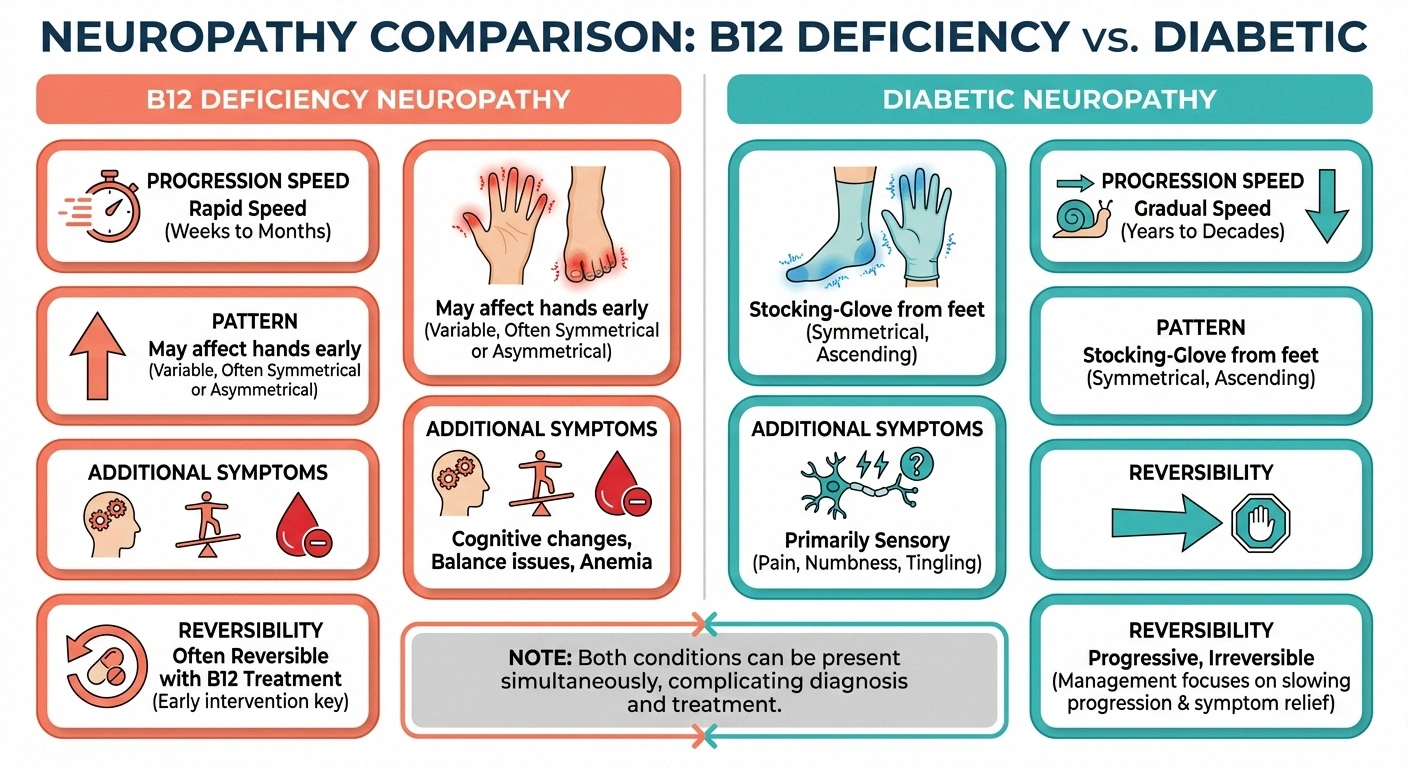
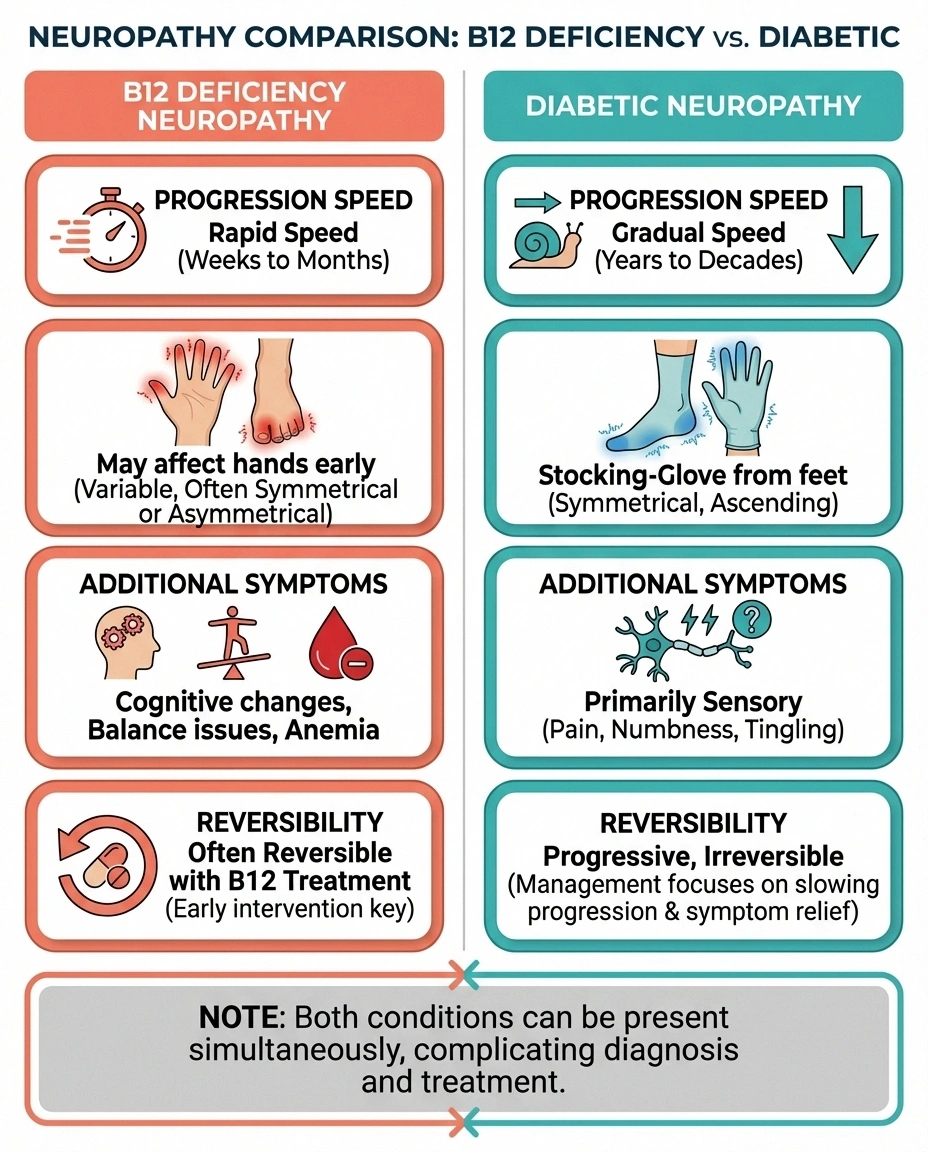
B12 deficiency neuropathy tends to progress more rapidly than typical diabetic neuropathy. It may affect the hands earlier than diabetic neuropathy typically does. It can also cause symptoms beyond nerve pain — including cognitive changes, balance problems, and a specific type of anemia (though anemia doesn't always accompany the neurological symptoms).
Diabetic neuropathy typically follows a “stocking-glove” pattern starting in the feet and progressing upward gradually over years. It correlates with duration and severity of diabetes and poor blood sugar control.
The uncomfortable truth: both can be present simultaneously. A person with diabetes on metformin can have diabetic neuropathy and B12-related neuropathy at the same time, each worsening the other.
Risk Factors for Metformin-Related B12 Deficiency
While any metformin user can develop B12 depletion, certain factors increase the risk:

- Duration of use: Risk increases with years on metformin. The All of Us study found a cumulative 3% annual increase in deficiency risk.
- Higher doses: Patients on higher daily doses of metformin (2,000+ mg) appear to be at greater risk than those on lower doses.
- Age: Older adults already have reduced B12 absorption capacity, and adding metformin compounds the problem.
- Proton pump inhibitor (PPI) use: Acid-reducing medications like omeprazole further impair B12 absorption. Taking PPIs and metformin together substantially increases risk.
- Vegetarian or vegan diet: Lower dietary B12 intake means less reserve to draw from when absorption is impaired.
- Previous gastric surgery: Any surgery that alters the stomach or small intestine can reduce B12 absorption further.
Getting Tested: What to Ask Your Doctor
If you take metformin — especially if you've been on it for more than two years — ask your doctor to check your B12 levels. This is a simple blood test, and it should be part of routine monitoring for anyone on long-term metformin therapy.
200-400 pg/mL: Borderline — request MMA and homocysteine tests
Above 400 pg/mL: Likely adequate — retest annually
Key insight: Serum B12 can appear “normal” while cellular levels are already inadequate. MMA is the more sensitive test for functional deficiency.
The basic test: Serum B12 level. Normal range is typically 200-900 pg/mL, though “normal” ranges vary by lab. Levels below 200 pg/mL indicate deficiency, and levels between 200-400 pg/mL are considered borderline — a range where neurological symptoms can already be developing.
More sensitive tests: If your serum B12 is borderline, two additional markers provide a clearer picture:
- Methylmalonic acid (MMA): Elevated MMA is a more sensitive indicator of functional B12 deficiency than serum B12 alone.
- Homocysteine: Also elevated in B12 deficiency, though less specific than MMA.
These additional tests are particularly important for metformin users because serum B12 can appear “normal-ish” while cellular B12 levels are already inadequate. For more on what blood work to request, see our comprehensive guide to lab tests for neuropathy.
Treatment: Fixing the Deficiency
The good news: if your neuropathy symptoms are caused by or worsened by metformin-related B12 deficiency, treating the deficiency can improve — and sometimes reverse — the nerve damage. But timing matters. The longer B12 deficiency goes undetected, the more likely the nerve damage becomes permanent.
Supplementation options:
Oral B12 supplements: High-dose oral B12 (1,000-2,000 mcg daily) can overcome the absorption barrier in many patients. Since metformin impairs the intrinsic factor pathway, about 1% of a high oral dose is absorbed passively — which is enough to replete stores when the dose is high enough.
B12 injections: Intramuscular B12 injections bypass the gut entirely, making them more reliable when absorption is severely impaired. A typical repletion schedule is weekly injections for 4-8 weeks, then monthly maintenance. For a detailed comparison, see our guide to B12 injections vs. oral supplements for neuropathy.
Sublingual B12: Dissolving B12 under the tongue allows some absorption through the oral mucosa, bypassing the gut. Evidence for this route is less robust than for injections, but some patients prefer it.
Calcium supplementation: Because metformin specifically impairs calcium-dependent B12 absorption, some research suggests that taking calcium supplements alongside metformin may help restore B12 absorption. This is an area of active investigation.
Important: Do not stop metformin without talking to your doctor. The blood sugar management benefits of metformin generally outweigh the B12 issue, and the deficiency can be managed through supplementation while continuing the medication.
Can the Nerve Damage Be Reversed?
This depends on how long the deficiency has been present and how severe the nerve damage is.
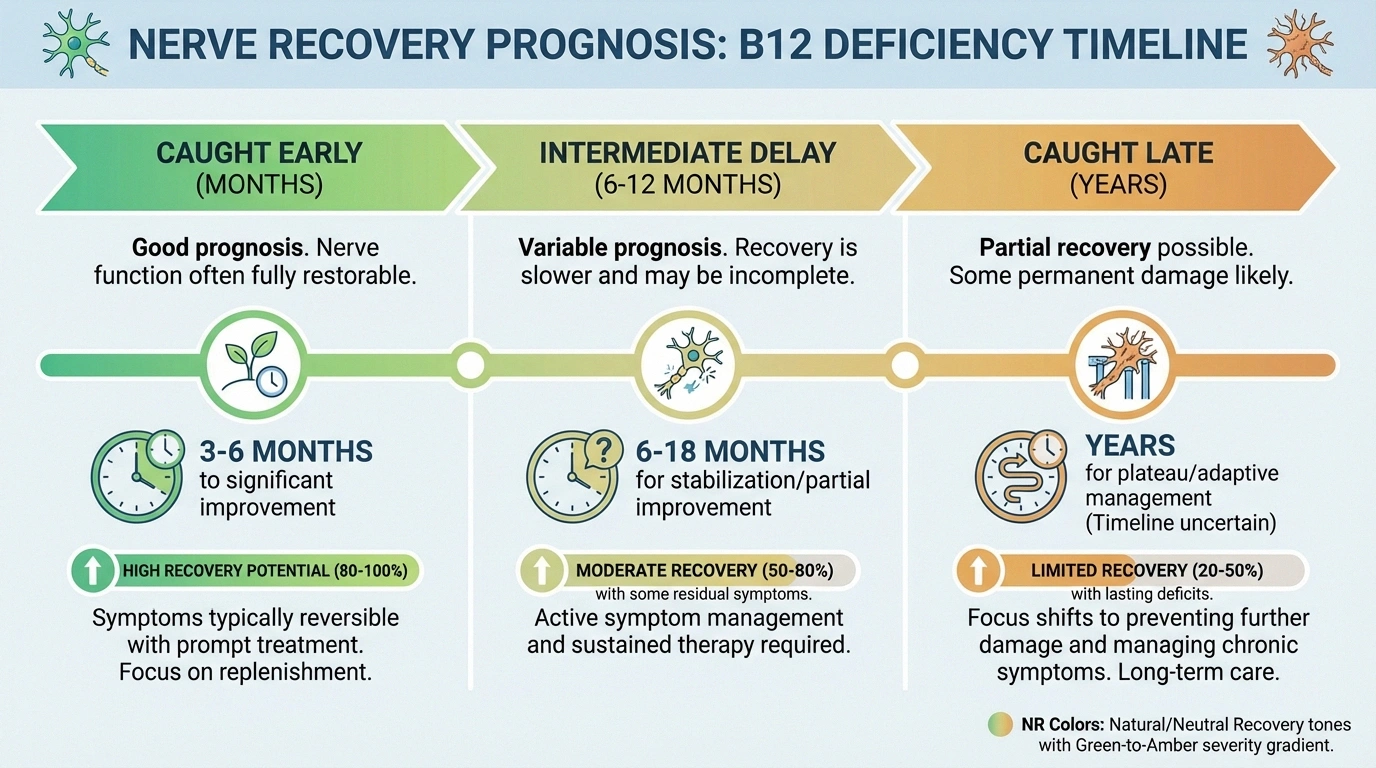
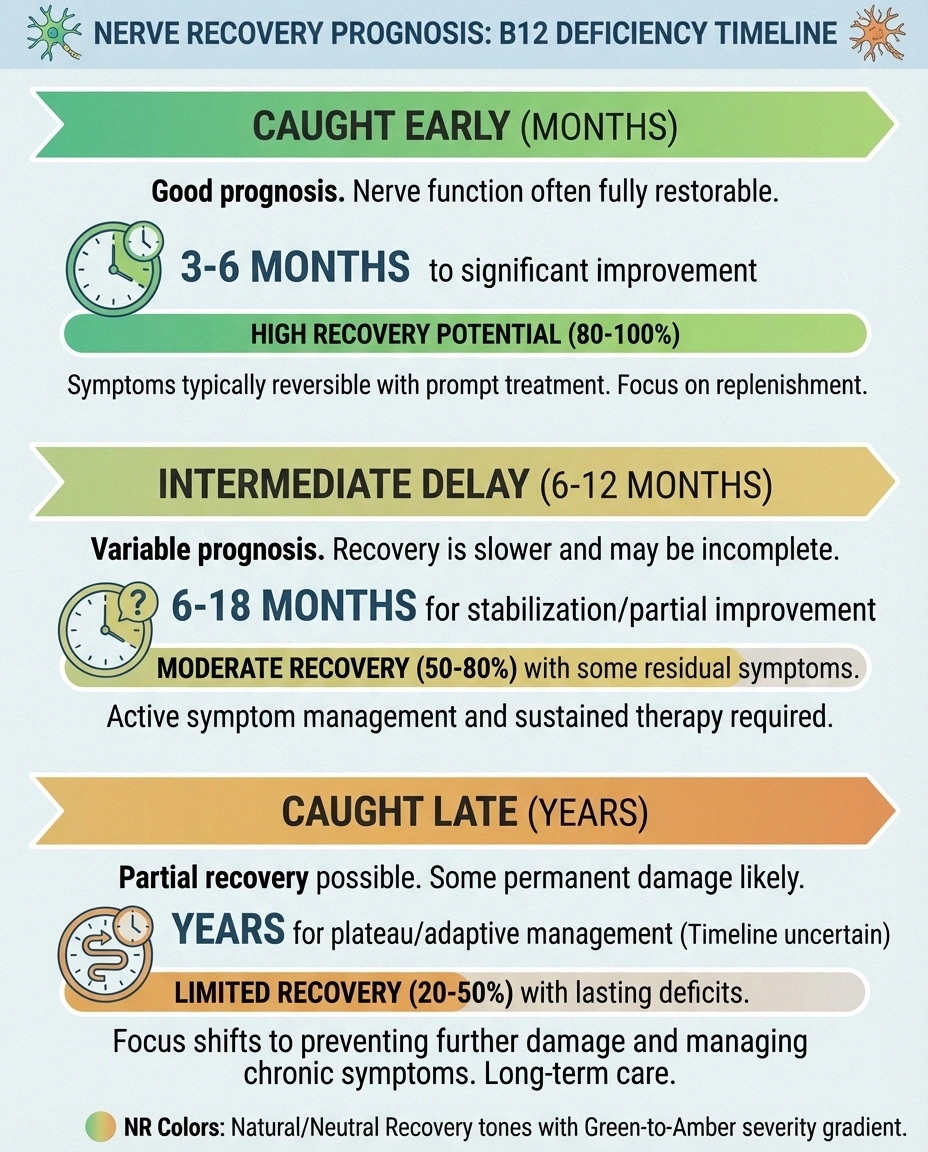
Caught early (within months): Nerve symptoms frequently improve significantly or resolve completely with B12 repletion. The nerves may need 3-6 months of adequate B12 levels to show meaningful recovery, but the prognosis is good.
Caught late (years of deficiency): Some nerve damage may be permanent. The myelin sheath — the protective coating around nerves that B12 helps maintain — can sustain irreversible damage after prolonged deficiency. Even in these cases, treatment usually prevents further progression and may provide partial improvement.
This is why early detection matters so much. The MHRA's emphasis on monitoring patients “at risk” of B12 deficiency is specifically aimed at catching the problem before permanent damage occurs. For more on whether nerve damage can heal, see our article on reversing neuropathy.
Prevention: Protecting Your Nerves While Taking Metformin
The best approach is prevention — maintaining adequate B12 levels from the start of metformin therapy, rather than waiting for symptoms to appear.
Recommended monitoring schedule:
- Baseline B12 level before starting metformin (or as soon as possible if already taking it)
- Annual B12 testing for all metformin users
- More frequent testing (every 6 months) for patients with additional risk factors
- Immediate testing if neuropathy symptoms develop or worsen
Preventive supplementation: Some experts now recommend prophylactic B12 supplementation for all patients on metformin — 1,000 mcg oral B12 daily — without waiting for deficiency to develop. This approach is inexpensive, safe, and eliminates the risk entirely. Discuss this with your doctor.
Dietary sources: While diet alone may not overcome metformin-induced malabsorption, ensuring adequate dietary B12 supports overall levels. Good sources include meat, fish, eggs, and dairy. For plant-based eaters, fortified foods (cereals, nutritional yeast, plant milks) provide B12. For more on nerve-protective nutrition, see our neuropathy diet guide.
What to Discuss with Your Doctor
If you're on metformin and experiencing neuropathy symptoms — or if you simply want to be proactive — here are the key points to raise at your next appointment:

- “I'd like to check my B12 levels, including methylmalonic acid if B12 is borderline.”
- “Should I start a B12 supplement as a preventive measure?”
- “Could my neuropathy symptoms be related to B12 depletion rather than (or in addition to) diabetes?”
- “How often should we recheck my B12 levels?”
- “Are any of my other medications (PPIs, H2 blockers) also affecting B12 absorption?”
These aren't confrontational questions — they demonstrate that you're an informed patient who understands the medication's known effects. For more on productive doctor conversations, see our guide to talking to your doctor about neuropathy. Browse all our supplement and nutrition guides for related information.
Frequently Asked Questions
Should I stop taking metformin if I have neuropathy?
No — do not stop metformin without your doctor's guidance. The blood sugar management benefits of metformin are significant and protect against diabetic neuropathy. The B12 issue can almost always be managed with supplementation while continuing metformin. Stopping metformin could worsen your blood sugar control, which would accelerate diabetic nerve damage.
How long does it take for metformin to cause B12 deficiency?
B12 stores in the body are substantial, so deficiency typically develops gradually over 2 to 5 years of metformin use. However, individuals who start with lower B12 levels, take higher metformin doses, or have additional absorption impairments may develop deficiency sooner. The risk increases by approximately 3% per year.
Can B12 supplements completely prevent metformin-related neuropathy?
In most cases, yes. Adequate B12 supplementation from the start of metformin therapy should prevent B12-related neuropathy. This doesn't prevent diabetic neuropathy from other causes (poor blood sugar control, vascular damage), but it eliminates the B12 pathway. A daily 1,000 mcg oral B12 supplement is typically sufficient.
My B12 level came back “normal” — could I still have a problem?
Yes. Serum B12 in the 200-400 pg/mL range is technically “normal” by many lab standards but may be functionally inadequate. Methylmalonic acid and homocysteine levels provide a more sensitive picture of cellular B12 status. If your B12 is in the low-normal range and you have neuropathy symptoms, ask for these additional tests.
Are B12 injections better than pills for metformin users?
Both can work. Injections bypass the gut entirely, making them more reliable when absorption is severely impaired. However, high-dose oral B12 at 1,000-2,000 mcg daily has been shown to be effective for most patients because enough is absorbed passively even when the intrinsic factor pathway is disrupted. Injections are typically recommended for severe deficiency or when oral supplements don't raise levels adequately.
Does this mean metformin is a bad medication?
Not at all. Metformin remains one of the most effective and safest medications for type 2 diabetes, with benefits that extend beyond blood sugar control including potential cardiovascular protection. The B12 issue is a manageable side effect, not a reason to avoid the medication. The key is awareness and monitoring — knowing about the risk and proactively supplementing eliminates most of the danger.


