Lab Tests for Neuropathy: What Blood Work to Request and Why It Matters
When I was first diagnosed with peripheral neuropathy, my doctor ordered a basic metabolic panel and told me everything looked fine. It wasn't until I saw a neurologist six months later that the real testing began — and we found a B12 deficiency that had been silently damaging my nerves the entire time.
That experience taught me something I've since confirmed with thousands of people in our neuropathy support community: the right B12 testing for metformin users tests can mean the difference between treatable neuropathy and “idiopathic” neuropathy — the frustrating diagnosis that really just means “we don't know why.” According to a 2020 review in the Journal of Neuromuscular Diseases, a systematic lab workup can identify the cause of neuropathy in up to 75% of cases.
This guide walks you through every lab test your doctor should consider, explains what each one reveals, and gives you the confidence to ask for the right tests at your next appointment.
Why Lab Tests Matter for Neuropathy
Peripheral neuropathy has over 100 known causes. Many of them are detectable — and treatable — through blood work. The problem is that many primary care doctors order only the most basic tests, missing causes that a more thorough workup would catch.
Research Says
A systematic lab workup can identify the cause of neuropathy in up to 75% of cases — turning “idiopathic” into treatable.
The American Academy of Neurology (AAN) guidelines recommend that everyone with suspected peripheral neuropathy should receive, at minimum, tests for blood glucose, vitamin B12 levels, and serum protein levels. But many neurologists go further — and you should know what additional tests are available.
Finding the cause matters because treatment changes dramatically based on the result. Vitamin deficiency neuropathy can improve with supplementation. Inflammatory neuropathy can respond to immunotherapy. Diabetic neuropathy can be slowed or stabilized with blood sugar control. But none of these treatments help if you never find the underlying cause.
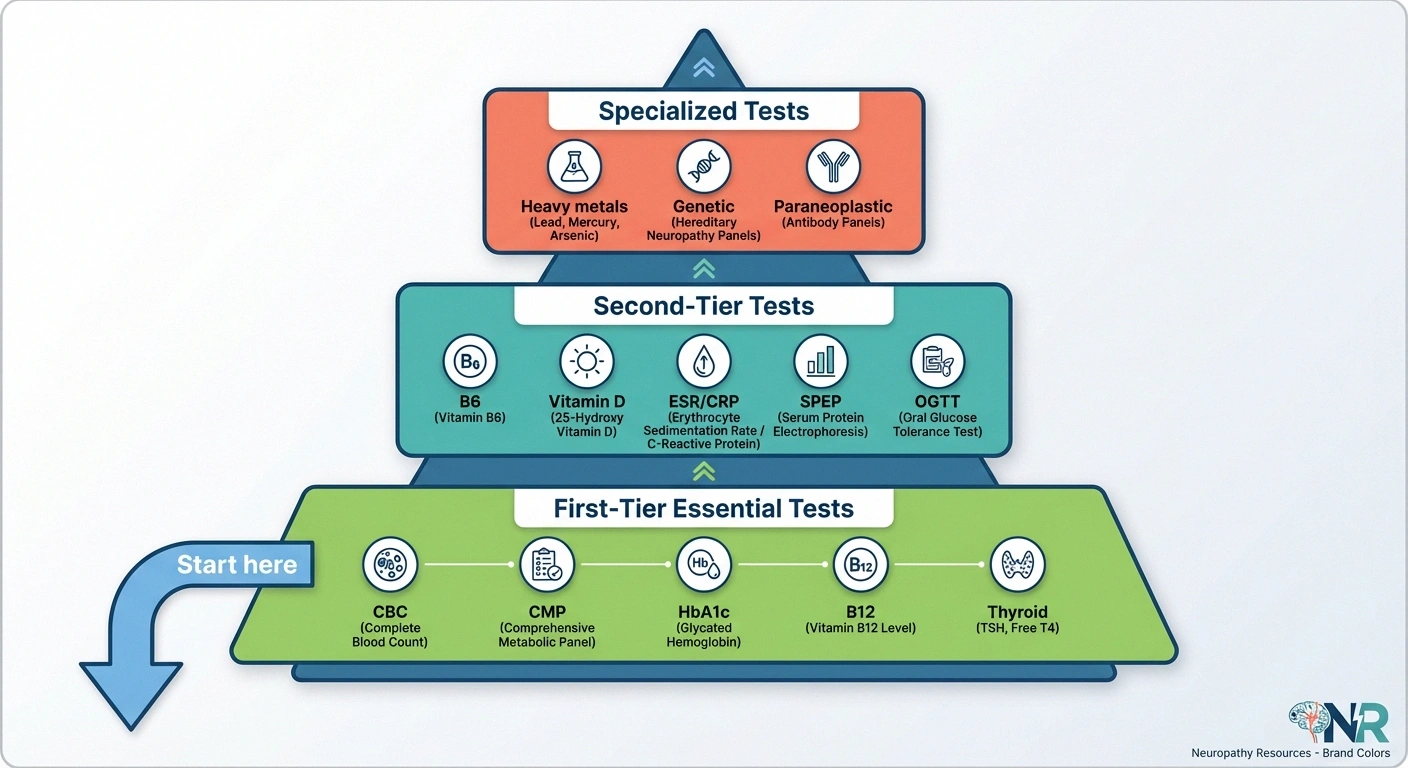
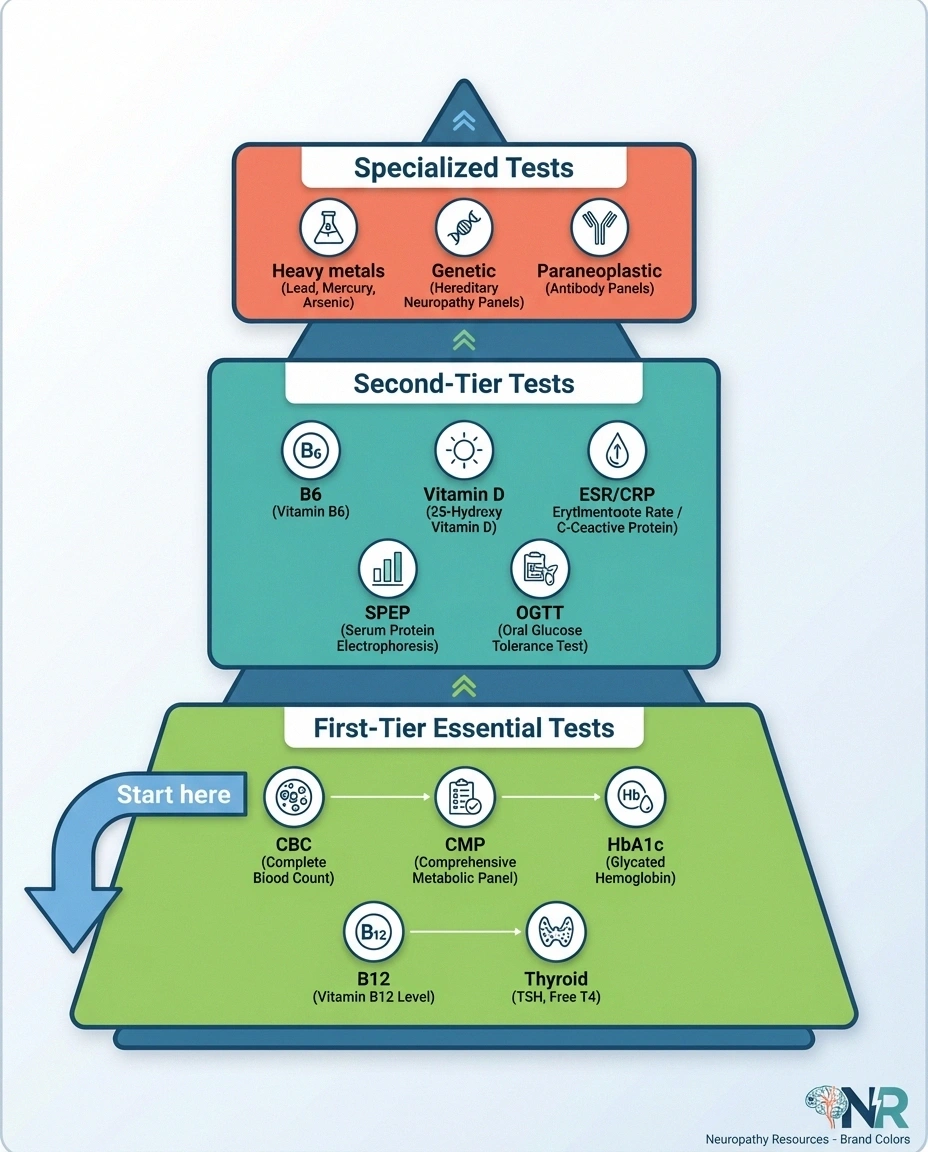
The Essential First-Tier Tests
These are the tests that every neuropathy workup should include, regardless of your symptoms or suspected cause. Think of them as the foundation — the tests most likely to reveal common, treatable causes. Based on NeuropathyCommons.org recommendations and the AAN guidelines, here's what to ask for.
Essential First-Tier Tests
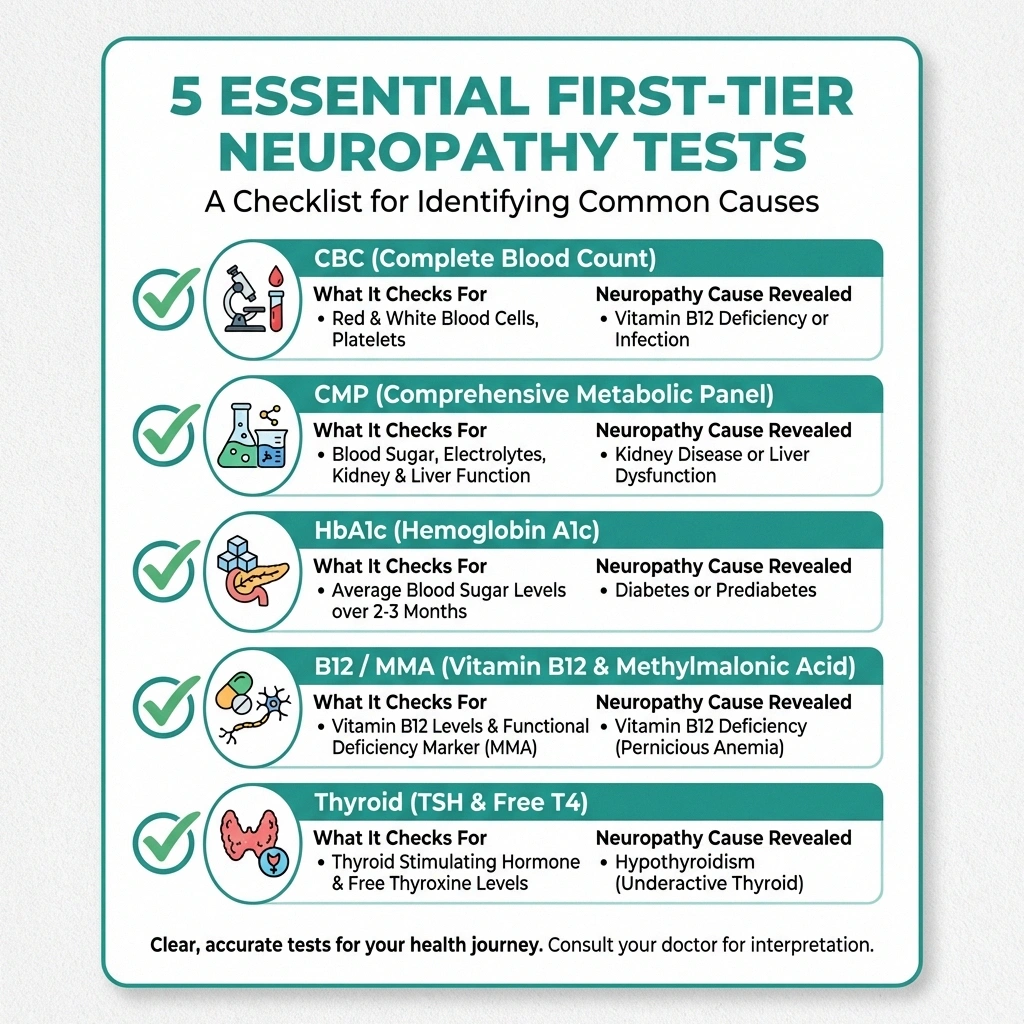
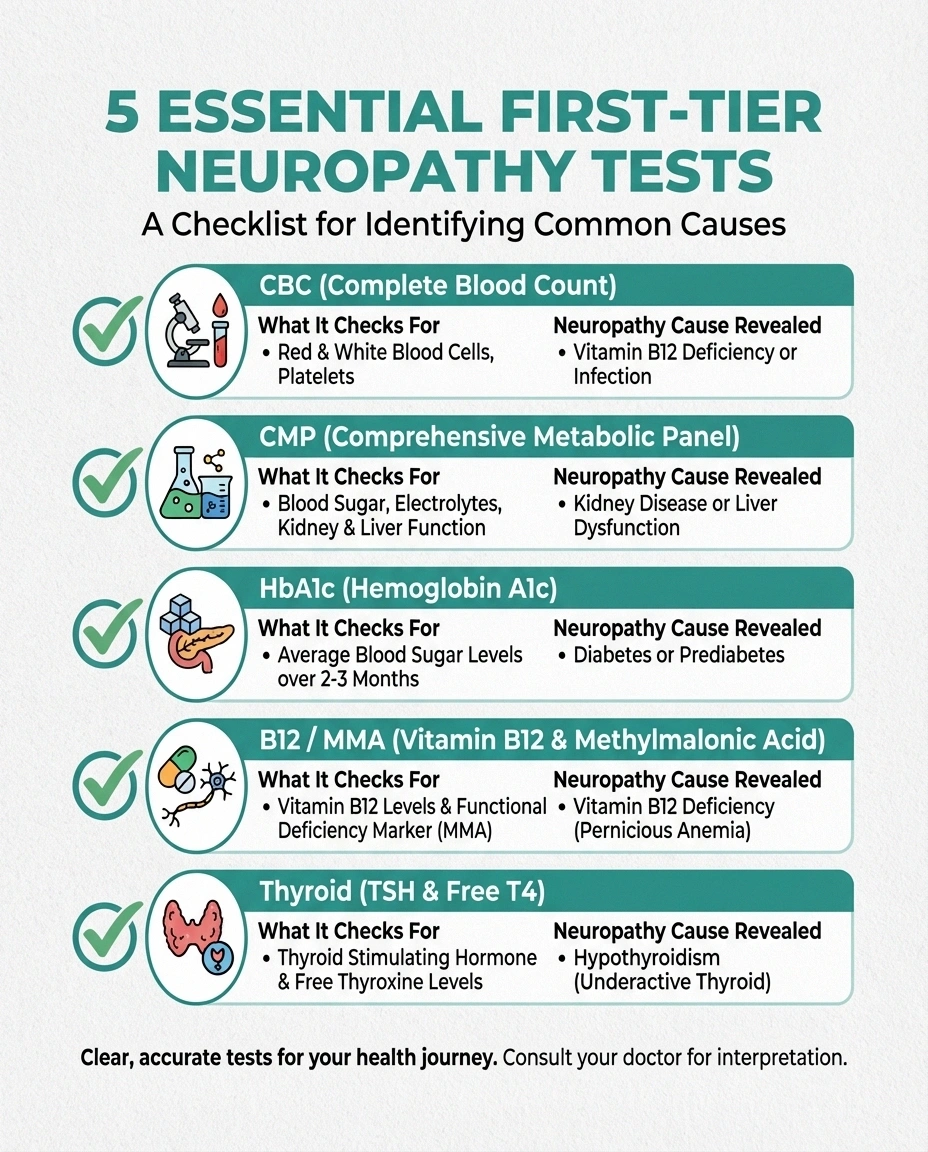
CBC
Blood cell counts → B12 deficiency, blood cancers
CMP
Blood sugar, kidney, liver → diabetes, uremia
HbA1c
3-month blood sugar average → diabetes, prediabetes
B12 + MMA
Functional B12 level → deficiency neuropathy
TSH + Free T4
Thyroid function → hypo/hyperthyroidism
Complete Blood Count (CBC)
A CBC measures the number and types of blood cells circulating in your body. It's a broad screening test that can point toward several neuropathy causes. Abnormal red blood cell size (macrocytosis) can suggest B12 or folate deficiency. Low white blood cell counts may point toward autoimmune conditions or blood cancers. Anemia, regardless of cause, can worsen existing neuropathy symptoms.
Comprehensive Metabolic Panel (CMP)
This panel checks your blood sugar, kidney function, liver function, and electrolytes — all directly relevant to neuropathy. Elevated fasting glucose or HbA1c points to diabetes or prediabetes, the single most common cause of neuropathy in developed countries. Elevated creatinine or BUN indicates kidney dysfunction, which can cause uremic neuropathy. Liver enzymes may reveal hepatitis or other liver conditions associated with nerve damage.
Hemoglobin A1c (HbA1c)
This is the three-month average of your blood sugar, and it's arguably the single most important test in any neuropathy workup. A normal fasting glucose can miss prediabetes and early diabetes — conditions that damage nerves before they cause any other symptoms. An HbA1c above 5.7% indicates prediabetes. Above 6.5% indicates diabetes. Even prediabetes (5.7-6.4%) can cause small fiber neuropathy.
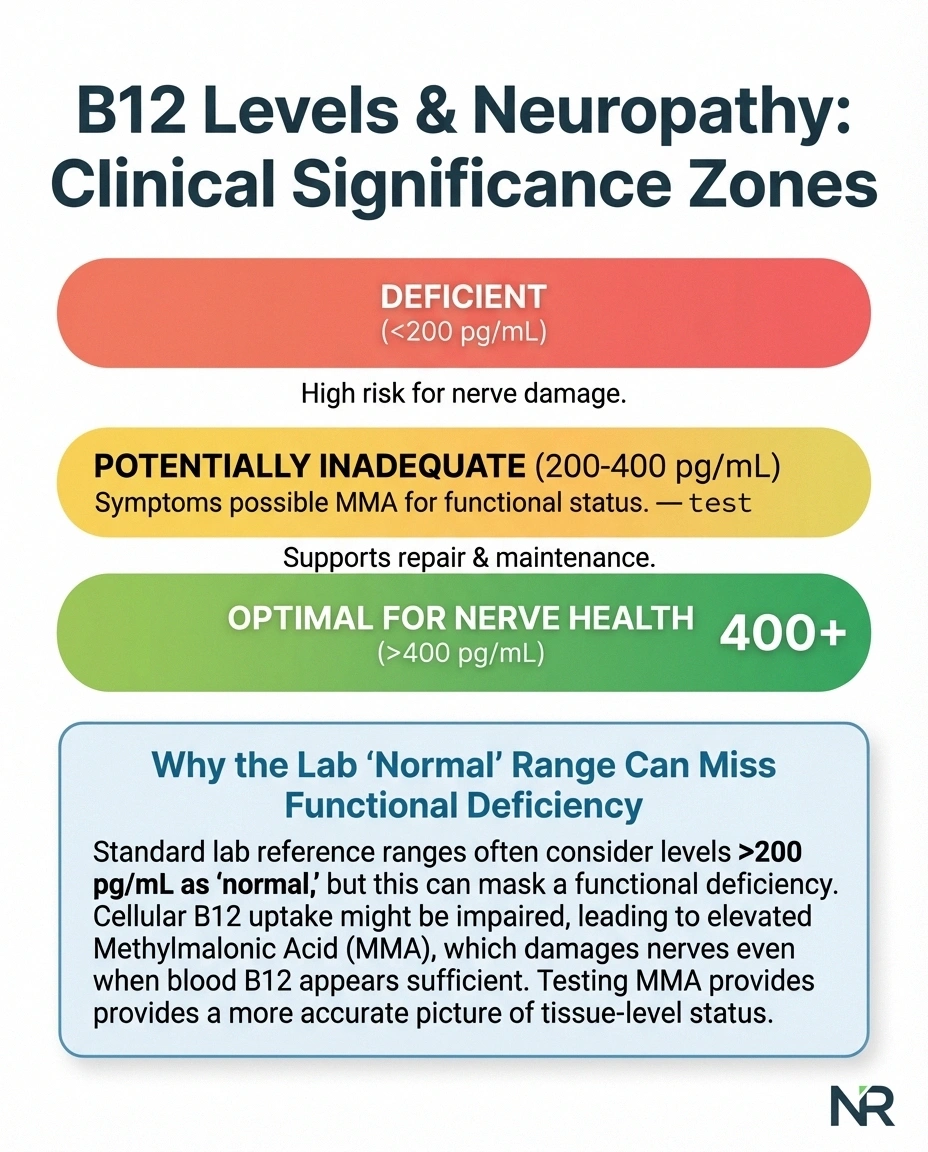
Vitamin B12 and Methylmalonic Acid
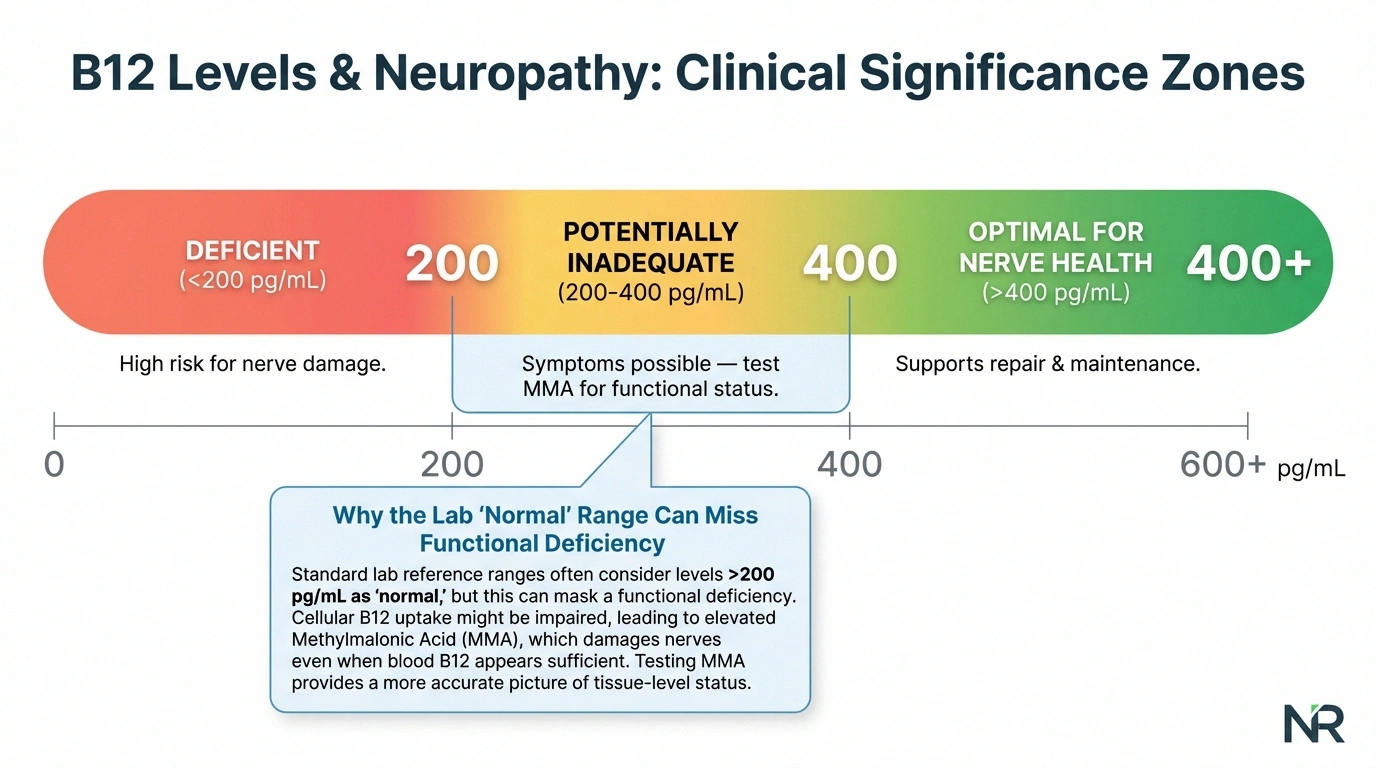
B12 deficiency is one of the most common treatable causes of neuropathy — and one of the most frequently missed. A standard B12 level can appear “normal” even when functional deficiency is present. That's why neurologists also order methylmalonic acid (MMA), which rises when B12 is functionally low even if the serum B12 level looks acceptable. If your B12 is below 400 pg/mL and your MMA is elevated, you may benefit from B12 supplementation or injections.
Thyroid Function (TSH, Free T4)
Both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid) can cause neuropathy. Thyroid-related neuropathy is particularly important to identify because it's treatable — thyroid hormone replacement or regulation often improves nerve symptoms. A simple TSH test is the standard screening tool. If abnormal, free T4 provides additional detail.
Second-Tier Tests: Digging Deeper
If the first-tier tests don't reveal a cause — or if your symptoms suggest something beyond the basics — your neurologist may order these additional tests. These target less common but still treatable causes.
Vitamin B6 Level
Here's a tricky one: both too little and too much B6 can cause neuropathy. B6 toxicity from over-supplementation is actually more common than deficiency as a neuropathy cause. If you take a multivitamin, a B-complex supplement, or a standalone B6 supplement, get your level checked. Levels above 200 nmol/L may indicate toxicity. Many people unknowingly take B6 from multiple sources, accumulating toxic levels over months. Read our complete B vitamins guide for detailed dosing information.
B6 Warning
Too much vitamin B6 can cause neuropathy — not just too little. If you take a multivitamin, B-complex, and standalone B6, you may be accumulating toxic levels. Get your B6 checked, especially if your neuropathy appeared after starting supplements.
Vitamin D and Vitamin E
Vitamin D deficiency is associated with increased neuropathy pain and may contribute to nerve damage. While not a primary cause of neuropathy in most cases, correcting a deficiency may help manage symptoms. Vitamin E deficiency, though rare, can cause a specific form of sensory neuropathy — it's worth checking if your diet is severely restricted or you have fat malabsorption.
Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP)
These are general inflammation markers. They don't tell you what's inflamed, but elevated levels signal that your immune system is active — which may point toward autoimmune or inflammatory neuropathy. If these are elevated, your doctor will likely order more specific autoimmune tests.
Serum Protein Electrophoresis (SPEP) and Immunofixation
These tests look for abnormal proteins in your blood, which can indicate conditions like MGUS (monoclonal gammopathy of undetermined significance), multiple myeloma, or amyloidosis — all of which can cause neuropathy. The AAN guidelines specifically recommend serum protein testing for neuropathy patients. MGUS-related neuropathy, in particular, is underdiagnosed and has specific treatment options.
Glucose Tolerance Test (OGTT)
If your fasting glucose and HbA1c are borderline but not diagnostic, a two-hour oral glucose tolerance test can unmask impaired glucose tolerance — a condition that damages small nerve fibers even before it progresses to full diabetes. This test is especially important if you have symptoms of small fiber neuropathy but no clear cause.
Tests for Autoimmune and Inflammatory Causes
Autoimmune diseases are a significant and often underdiagnosed cause of neuropathy. If you have symptoms suggesting systemic inflammation — joint pain, skin rashes, dry eyes, dry mouth — or if your basic workup was negative, these tests may reveal the cause.

Antinuclear Antibodies (ANA)
ANA is a screening test for systemic autoimmune conditions, including lupus (SLE), Sjögren's syndrome, and rheumatoid arthritis — all of which can cause neuropathy. A positive ANA doesn't confirm a specific diagnosis but tells your doctor to investigate further. About 15% of healthy people have a weakly positive ANA, so this test must be interpreted in context.
Anti-Ro (SS-A) and Anti-La (SS-B)
These antibodies are associated with Sjögren's syndrome, an autoimmune condition that causes dry eyes, dry mouth, and — importantly — neuropathy. Sjögren's is one of the most common autoimmune causes of small fiber neuropathy and is frequently missed because its symptoms overlap with other conditions. Some patients have neuropathy as their first Sjögren's symptom, before the dryness develops.
Anti-Tissue Transglutaminase (IgA-TTG)
This test screens for celiac disease — an autoimmune reaction to gluten that damages the small intestine. Celiac disease causes neuropathy in up to 10% of patients, sometimes before any digestive symptoms appear. If positive, a gluten-free diet can halt and sometimes reverse the nerve damage. Read more about the relationship between diet and neuropathy.
Ganglioside Antibodies (Anti-GM1, Anti-MAG)
These specialized antibodies target components of nerve cell membranes. Anti-GM1 antibodies are associated with multifocal motor neuropathy. Anti-MAG antibodies are linked to a specific type of demyelinating neuropathy. These tests are typically ordered when the EMG pattern suggests a demyelinating rather than axonal neuropathy, or when the clinical picture doesn't fit common diagnoses.
Tests for Infectious Causes
Several infections can cause neuropathy, and they're all detectable through simple blood tests. Your doctor should consider these based on your risk factors and medical history.
HIV Testing
The CDC recommends HIV screening for all adults regardless of symptoms, and HIV is a well-established cause of peripheral neuropathy. HIV neuropathy affects up to 30% of people living with HIV. Early detection and treatment with antiretroviral therapy can prevent or improve nerve damage. Note that some antiretroviral medications can themselves cause neuropathy.
Hepatitis B and C
Hepatitis C in particular is associated with neuropathy, often through cryoglobulinemia — a condition where abnormal antibodies accumulate in blood vessels. Hepatitis B can cause neuropathy through direct nerve inflammation. Both are treatable, making testing important.
Lyme Disease Antibodies
If you live in or have traveled to areas where Lyme disease is common (northeastern and upper midwestern United States), Lyme testing should be part of your neuropathy workup. Lyme disease can cause cranial neuropathies, radiculopathy, and peripheral neuropathy. Early antibiotic treatment can resolve the infection and halt nerve damage.
Specialized Tests for Difficult Cases
When standard testing doesn't reveal a cause, your neurologist may order these more specialized tests. These are typically reserved for cases where the clinical picture is unusual or the neuropathy is progressing despite treatment.
Heavy Metal Testing
Lead, mercury, arsenic, and thallium can all cause neuropathy through direct nerve toxicity. Testing is done through blood and/or urine samples. Your doctor should consider heavy metal testing if you have occupational exposure (mining, manufacturing, art restoration), use herbal remedies from unregulated sources, or have other symptoms of toxicity like hair loss, gastrointestinal problems, or cognitive changes. Read more about toxic neuropathy causes.
Genetic Testing
If your family history suggests inherited neuropathy, or if your neuropathy pattern is unusual (very early onset, specific distribution, foot deformities), genetic testing for Charcot-Marie-Tooth disease and other hereditary neuropathies may be appropriate. This is typically a blood test analyzing specific genes associated with inherited nerve conditions.
Paraneoplastic Antibody Panel
In rare cases, neuropathy can be a paraneoplastic syndrome — your immune system attacking your nerves in response to a hidden cancer. Tests for antibodies like anti-Hu, anti-CV2, and anti-amphiphysin are ordered when neuropathy develops rapidly, is severely painful, or doesn't fit any other pattern. A positive result triggers an urgent search for an underlying malignancy.
How to Talk to Your Doctor About Testing
Requesting specific lab tests from your doctor can feel intimidating, but it's your right as a patient. Here's how to approach it productively.
Practical Tip
Bring this article or a printed test list to your appointment. Frame it as: “I've been researching my condition, and I'd like to discuss whether these tests would be appropriate for me.” Most doctors appreciate informed, prepared patients.
Bring this article — or at least a list of the tests you'd like to discuss. Most doctors appreciate informed patients. Frame it as: “I've been researching my condition, and I'd like to discuss whether these tests would be appropriate for me.”
Start with gaps in your current testing. Review your previous lab results and identify what hasn't been checked yet. If you've never had an HbA1c, methylmalonic acid, or serum protein electrophoresis, those are reasonable requests.
Know your insurance coverage. Most first-tier tests are routinely covered. Second-tier and specialized tests may require pre-authorization. Your doctor's office can often check coverage before ordering.
Consider a neurologist referral. Primary care physicians may not be familiar with the full neuropathy workup. A neurologist — especially one who specializes in neuromuscular disease — will know exactly which tests to order based on your specific symptoms and diagnostic findings.
Keep copies of everything. Request copies of all lab results for your own records. This is especially important if you see multiple doctors or change providers. A complete testing history prevents unnecessary duplicate testing.
Understanding Your Results: What the Numbers Mean
Lab results can be confusing, with ranges that vary between labs and values that fall in gray zones. Here are some practical guidelines for the most important neuropathy-related tests.

Key Numbers to Know
HbA1c: Above 5.7% = prediabetes risk. B12: Below 400 pg/mL may be inadequate for nerves — request MMA test. TSH: Optimal 1.0-2.5 mIU/L. Always discuss results with your doctor — context matters.
HbA1c: Below 5.7% is normal. 5.7-6.4% is prediabetes (and can cause neuropathy). Above 6.5% is diabetes. If yours is above 5.7%, discuss blood sugar management with your doctor.
Vitamin B12: Lab “normal” range is often 200-900 pg/mL, but neurologists consider levels below 400 pg/mL potentially inadequate for nerve health. If your B12 is between 200-400 and you have neuropathy symptoms, request a methylmalonic acid test to check for functional deficiency.
TSH: Normal is typically 0.4-4.0 mIU/L, though many endocrinologists prefer to see it between 1.0-2.5. Values outside this range warrant further thyroid investigation.
ESR and CRP: Elevated values indicate inflammation somewhere in your body. They're not specific to neuropathy, but elevated levels in a neuropathy patient should prompt autoimmune testing.
Always discuss your results with your doctor rather than interpreting them in isolation. Context matters — your symptoms, medical history, and other test results all factor into what your numbers mean for you.
Frequently Asked Questions
What blood tests should I ask for if I suspect neuropathy?
Start with the essential first-tier tests: complete blood count, comprehensive metabolic panel, HbA1c, vitamin B12 with methylmalonic acid, and thyroid function. These cover the most common treatable causes. If results are normal but symptoms persist, discuss second-tier tests including serum protein electrophoresis, vitamin B6, inflammation markers, and autoimmune panels with your neurologist.
Can blood tests definitively diagnose neuropathy?
Blood tests identify the cause of neuropathy, not the neuropathy itself. The diagnosis of peripheral neuropathy typically comes from your symptoms, neurological examination, and nerve conduction studies or EMG. Blood tests then answer the critical question of why the neuropathy is happening, which directly determines treatment.
How often should neuropathy blood work be repeated?
This depends on your diagnosis. Diabetic patients should have HbA1c checked every three to six months. Vitamin levels should be rechecked three to six months after starting supplementation to verify correction. Autoimmune markers may need annual monitoring. Your neurologist will recommend a testing schedule based on your specific situation.
My blood work came back normal but I still have neuropathy symptoms. What now?
Normal first-tier blood work doesn't mean there's no cause — it means the most common causes have been ruled out. Ask your doctor about second-tier tests, glucose tolerance testing, and autoimmune panels. If extensive blood work is negative, further investigation may include nerve biopsy, skin biopsy for small fiber density, or genetic testing. About 25% of neuropathy cases remain idiopathic even after comprehensive testing.
Do I need to fast before neuropathy blood tests?
Fasting for 8-12 hours is recommended for accurate glucose and lipid results included in the comprehensive metabolic panel. Most other neuropathy tests, including B12, thyroid, and autoimmune panels, do not require fasting. Your doctor's office will tell you which specific tests on your order require fasting when they schedule the blood draw.
Can I order neuropathy blood tests myself without a doctor?
Some direct-to-consumer lab services allow you to order blood tests without a doctor's order. However, interpreting results without medical training can lead to unnecessary anxiety or missed findings. It's always better to work with a healthcare provider who can order the right tests, interpret results in context, and connect findings to a treatment plan.
Taking Control of Your Diagnosis
The right lab tests can transform a confusing, frustrating neuropathy diagnosis into a clear treatment path. Don't accept “idiopathic neuropathy” until a thorough workup has been completed. Too many people spend years managing symptoms when the underlying cause — and a targeted treatment — was discoverable with a simple blood draw.
Print this guide or bookmark it for your next appointment. Review your existing test results against the lists above. Identify what hasn't been checked. And have a conversation with your doctor or neurologist about completing your workup. Browse all our resources for understanding neuropathy to continue your learning.
You deserve to know why your nerves are damaged. And in most cases, the answer is waiting in a tube of blood.