
The first time I heard about a child with neuropathy, I was sitting in a support-group meeting, listening to a woman about my age talk about her seven-year-old grandson. She said his teacher had called her daughter to a parent conference because the boy “kept tripping in the hallway and couldn't keep up in P.E.” The pediatrician had brushed it off twice. The third time, an alert school nurse said the words peripheral neuropathy out loud, and the family's life got rearranged.
I had been living with neuropathy myself for nearly a decade by then, and it had honestly never crossed my mind that children could develop nerve damage too. I think a lot of us assume neuropathy is something you earn the slow way — diabetes, age, a chemo regimen, decades of standing behind a counter. The idea that a five-year-old or a ten-year-old could have it felt impossible.
It is not impossible. It is more common than most people know. And the families going through it are doing it largely in private, because pediatric neuropathy is one of those quiet diagnoses that nobody really talks about until it lands in your house.
This article is for the parent who has just heard the words “we'd like to refer your child to a pediatric neurologist” and is trying to take a steady breath. It is for the grandparent quietly worrying. It is for the teacher who suspects something is off. I am not a doctor. I am a patient advocate, a grandmother, and a woman who has spent a long time inside this world. What I want to give you is a map — what pediatric neuropathy looks like, what causes it most often, what the diagnosis path tends to involve, and how to make sure your child has what they need at home and at school. The medical decisions belong to your pediatric neurologist. The orientation belongs here.
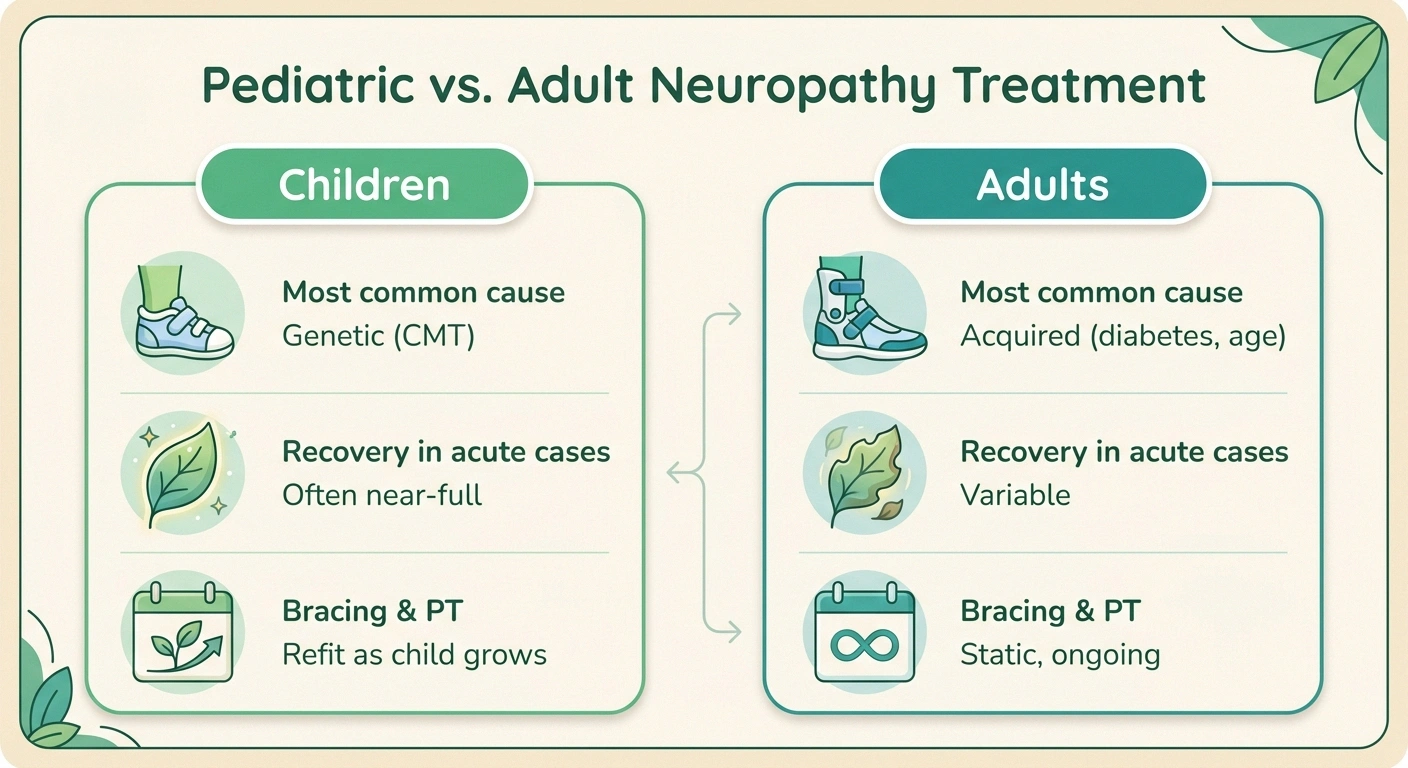
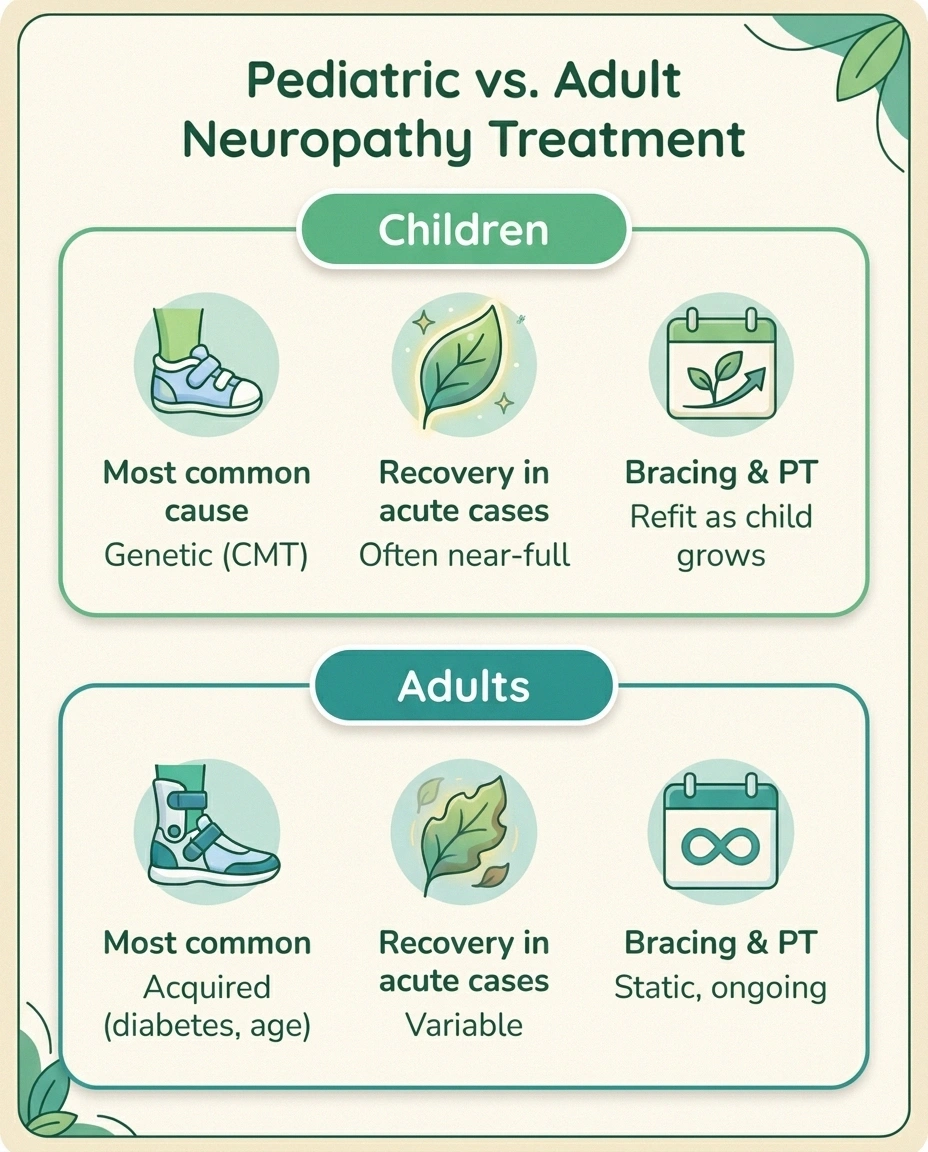
How Pediatric Neuropathy Differs from Adult Neuropathy
When adults develop peripheral neuropathy, the cause is usually something accumulated over decades. Diabetes is the headline example. Chemotherapy, alcohol, autoimmune conditions, B12 deficiency, and idiopathic small-fiber issues round out the list. The nerves are damaged after a long working life.
Children's nerves heal differently than adults' do.
A child's nervous system is still developing, which means three things at once: the most common pediatric cause is genetic (not acquired), motor symptoms often appear before sensory ones, and recovery from acute neuropathies is frequently more complete than in adults. The diagnosis is rarely a sentence — it is the start of a long, manageable conversation.
Children are different. A child's nerves are still developing. The myelin sheath — the fatty coating that lets nerve signals travel quickly — is laying down through early childhood and into adolescence. So when something goes wrong with a child's nerves, the cause and the picture are both shaped by a still-developing nervous system.
A few practical implications follow from this. First, the most common pediatric cause is genetic, not acquired — almost the inverse of the adult landscape. Second, kids often present with motor symptoms (clumsiness, foot deformity, weakness) before sensory ones, partly because young children have a hard time describing tingling or numbness. Third, recovery from acute pediatric neuropathy is often more complete than in adults, because young nervous systems remyelinate and adapt remarkably well. Fourth, a child's diagnosis is rarely a clean one-visit affair — it tends to involve a pediatrician, a pediatric neurologist, often a geneticist, and sometimes a pediatric oncologist or rheumatologist. The team is bigger because the differential diagnosis is wider.
I want parents reading this to know one thing right now: a pediatric neuropathy diagnosis is not a sentence. Children with the most common forms grow up to live full lives. Some need braces. Some need accommodations. Some need a thoughtful pediatric neurologist on speed dial. Almost all of them will have a future their parents could not imagine on the day of the diagnosis.
The Most Common Causes in Children

Here is the practical landscape, in roughly the order pediatric neurologists encounter these conditions.
The five most common pediatric neuropathies
| Condition | Onset Pattern | Hallmark Signs | Treatment Direction |
|---|---|---|---|
| CMT (genetic) | Slow, ages 5-15 | High arches, foot drop, frequent tripping, family history | PT, OT, AFO bracing, supportive |
| Guillain-Barré | Acute, days | Ascending weakness after a recent illness | IVIG, hospital, often near-full recovery |
| CIPN (chemo) | During cancer treatment | Foot pain, refusal to walk, stumbling | Dose adjustment, PT, time |
| Juvenile CIDP | Months, can relapse | Progressive weakness with periods of recovery | IVIG, steroids, plasma exchange |
| Nutritional (B12) | Slow, dietary context | Tingling, fatigue, restrictive diet | Replacement, often reversible |
Charcot-Marie-Tooth Disease (CMT)
CMT is the most common inherited neurological disorder in the world, and it is the single most common cause of pediatric peripheral neuropathy. Roughly one in 2,500 people has some form of it. CMT is genetic — passed down through families — and it primarily affects the nerves that control the feet, lower legs, hands, and forearms. According to the National Institute of Neurological Disorders and Stroke, symptoms most often appear between ages 5 and 15, though some severe forms show up in toddlerhood.
Making CMT the most common inherited neurological disorder in the world — and the most common cause of pediatric peripheral neuropathy. Symptoms typically appear between ages 5 and 15. Source: NINDS.
What parents notice first is almost always physical: high arches (called pes cavus), hammer toes, frequent tripping, an unusually slow run, trouble buttoning a shirt, poor handwriting, dropped pencils, or a child who absolutely refuses to wear certain socks because the seams “feel wrong.” CMT does not affect intelligence or life expectancy. Most kids with CMT walk their whole lives. Many become accomplished professionals, athletes within their range, and parents themselves. We have a deeper article on the genetic story at hereditary neuropathy and CMT for families who want the full picture.
Guillain-Barré Syndrome (GBS)
GBS is acute, dramatic, and frightening — and the recovery rate in children is genuinely encouraging. It is an autoimmune condition where the body's own immune system attacks the myelin coating around peripheral nerves, often after a recent viral illness or stomach bug. The hallmark is ascending weakness: a child who was fine on Monday is dragging her feet on Wednesday and can't climb stairs by Friday.
A four-step parent path
Sudden ascending weakness in a child is a medical emergency.
If a child develops new weakness in the legs that climbs upward over hours or days — especially after a recent viral illness or stomach bug — this can be the pattern of Guillain-Barré syndrome. Other warning signs:
- Difficulty climbing stairs the child handled easily a few days ago
- New trouble swallowing, drooling, or facial droop
- Shortness of breath or shallow breathing
- Inability to stand or walk that is new
Go to a pediatric emergency room immediately. Early IVIG treatment dramatically improves outcomes.
Pediatric GBS is rare — about one in 120,000 children per year — but it is a medical emergency. According to Children's Hospital of Philadelphia, most children require hospitalization, and severe cases need intensive care because the weakness can climb to the breathing muscles. The good news, and it is real news, is that 90 to 95 percent of pediatric GBS cases recover fully or near-fully. Treatments like intravenous immunoglobulin (IVIG) speed recovery dramatically. Our overview at Guillain-Barré syndrome walks parents through what hospital admission tends to look like.
Chemotherapy-Induced Peripheral Neuropathy (CIPN)
Children with cancer — particularly acute lymphoblastic leukemia (ALL), the most common pediatric cancer — frequently develop neuropathy as a side effect of their treatment. Vincristine and other vinca alkaloids are the classic offenders, along with platinum-based agents. Pediatric oncology research suggests that up to 90 percent of children on certain regimens experience some degree of neuropathy during treatment.
What complicates pediatric CIPN is communication. A four-year-old in cancer treatment cannot easily articulate “tingling” or “burning” or “my feet feel asleep.” Parents and oncology nurses watch for behavioral signs instead — a child suddenly refusing to walk, complaining their feet hurt, or stumbling more than usual. Most CIPN improves once chemotherapy ends, though some children carry symptoms forward as survivors. We've written more about treatment-related nerve damage at chemotherapy-induced neuropathy.
Juvenile CIDP (Chronic Inflammatory Demyelinating Polyneuropathy)
CIDP is the chronic cousin of GBS — same general mechanism (immune system attacking myelin), but it develops over months rather than days, and it tends to relapse and remit. Juvenile CIDP is uncommon but treatable, often with IVIG, steroids, or plasma exchange. A child with juvenile CIDP might have weeks of progressive weakness, then partial recovery, then another flare. Diagnosis usually requires nerve conduction studies and sometimes a spinal tap. Our deeper resource at CIDP overview covers the long arc of this condition.
Diabetic Neuropathy in Children
Type 1 diabetes is the most common form in children, and while diabetic neuropathy is more often associated with adults who've had diabetes for many years, children with poorly controlled blood sugar can absolutely develop nerve damage over time. The conversation in pediatric endocrinology has shifted in recent years toward earlier screening, because researchers are finding subtle signs of small-fiber neuropathy in adolescents with diabetes far earlier than once believed.
Nutritional and Vitamin B12 Deficiency
This one matters more than parents often realize. Children on highly restrictive diets — vegan or vegetarian diets without proper supplementation, eating-disorder presentations, certain gastrointestinal conditions, or families who don't have reliable food access — can develop B12 deficiency. B12 is essential for myelin maintenance, and a deficiency in a still-developing nervous system can produce neuropathy that is partially reversible if caught early. Our article at vitamin deficiency neuropathy covers what to look for.
Other and Rarer Causes
Pediatric neuropathy can also stem from sickle cell disease complications, mitochondrial disorders, Lyme disease (post-infectious), heavy metal exposure, and certain inherited metabolic conditions. The list is longer than this article — which is part of why diagnosis is a careful process and not a single test.
What Parents Notice First
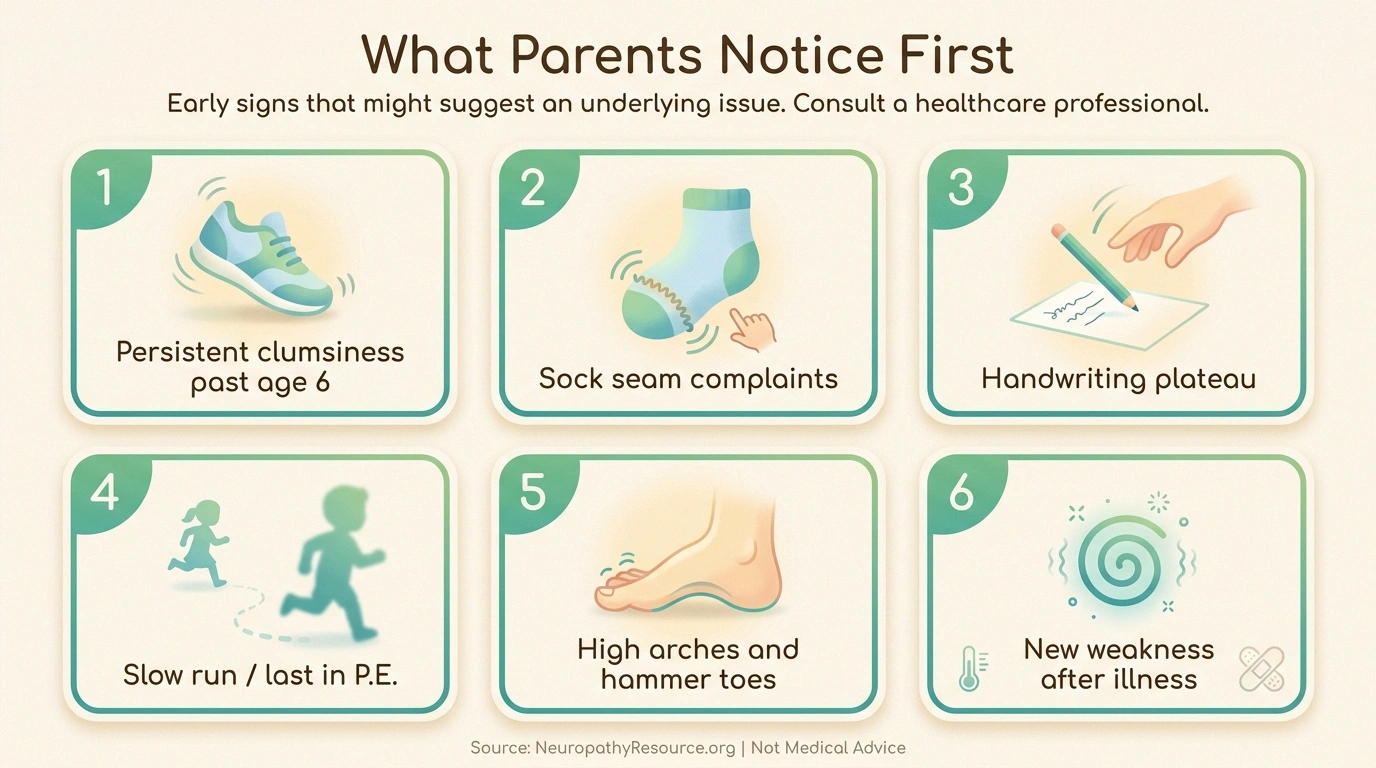

If you ask a pediatric neurologist what brings most parents into the clinic, the answer rarely begins with a child saying “my feet are numb.” It usually begins with a parent's gut.
The patterns I hear about most often:
- The clumsiness that doesn't fade. All toddlers fall. By age six or seven, most children have grown into their feet. A child who is still tripping over thresholds, dragging a toe up stairs, or running in a way that looks “off” past that age often has something going on.
- The sock complaint. Children with sensory nerve issues frequently object to clothing in ways that go beyond ordinary preference — sock seams, tags, shoe linings. It can be misread as sensory processing alone for years.
- The handwriting plateau. A child whose handwriting was developing fine and then simply stops improving — or who avoids buttons, shoelaces, and zippers — may be losing fine motor control in the hands.
- The slow run. Many parents notice their child is always last in tag, always trailing in P.E. relays. This isn't necessarily a fitness issue.
- The high arches. Pes cavus is a hallmark CMT finding. A child with unusually high arches and hammer toes, especially if a parent or grandparent has them too, deserves a neurology consult.
- The post-illness weakness. A child who was sick a couple weeks ago and is now strangely weak in the legs, with new trouble climbing stairs, needs urgent evaluation. This is the GBS pattern.
- The complaint of “my feet hurt” from a child receiving chemotherapy.
Trust the pattern. Pediatricians are trained for the common, and pediatric neuropathy is uncommon enough that it can take more than one visit to be taken seriously. Bring video. Bring a list of moments. Ask for a referral if your gut says something is off and you aren't being heard.
How Pediatric Neuropathy Is Diagnosed

The diagnostic path for a child looks somewhat different from an adult's path, but the core tools are similar. Here is what families typically encounter:
Pediatric neurologist consultation. The first stop after the pediatrician. The neurologist will take a detailed family history (huge in CMT cases), do a clinical exam (reflexes, gait, foot structure, fine motor tasks), and decide what testing makes sense. Our overview at neuropathy diagnosis walks through the broader framework.
EMG and nerve conduction studies (NCS). These tests measure how electrical signals travel along nerves. They are the workhorse diagnostic tool. In children, they are uncomfortable but not dangerous, and skilled pediatric neurology centers have technicians who do them with kids every day. The room is usually warm, parents can stay, and many centers use distraction (tablets, headphones) to make it bearable. Results often suggest whether the issue is demyelinating (myelin coating) or axonal (the nerve fiber itself) — a distinction that points toward likely causes.
Genetic testing. If CMT is suspected, genetic testing has become remarkably sensitive. Most common CMT subtypes can be confirmed from a single blood draw or cheek swab. A confirmed genetic diagnosis spares families a lot of guesswork and helps guide future treatment decisions.
Lumbar puncture (spinal tap). Used selectively, especially when GBS or CIDP is on the table. Cerebrospinal fluid analysis can show characteristic patterns.
Blood work. Vitamin levels (especially B12), thyroid function, blood sugar, autoimmune markers, and infection panels are all common.
Pattern of damage. Some neuropathies follow a “length-dependent” pattern (longest nerves affected first — feet before hands), while others affect small fiber neuropathy structures only. The pattern itself is a clue.
Diagnosis can take weeks or even months. That waiting room is one of the hardest places to live as a parent. I want to validate that and also tell you the wait is not wasted — those weeks are when the team is being thorough so the answer is the right one.
Treatment: What's Different from Adults
Pediatric treatment is shaped by three things adult treatment isn't: ongoing nervous system development, school and life-stage logistics, and a much longer projected lifetime with the condition.
Pediatric Guillain-Barré has a 90-95% full or near-full recovery rate.
Children's nervous systems remyelinate and adapt more completely than adults' do. Studies in pediatric neurology consistently show that children treated promptly with IVIG recover to near-baseline function. The acute phase is frightening; the medium-term picture is genuinely encouraging.
For CMT, there is currently no cure. The standard of care is supportive: physical therapy, occupational therapy, custom ankle-foot orthoses (AFOs) when foot drop or instability appears, careful monitoring for scoliosis and contractures, and surgical correction in selected cases. Many children with CMT thrive with the right shoes, the right braces, and a coach (or family) that understands their range. According to the Charcot-Marie-Tooth Association, research into disease-modifying therapies is genuinely active right now.
For GBS, IVIG is the treatment workhorse in pediatrics. Plasmapheresis is an alternative. Children typically spend time in a hospital, sometimes intensive care, and then move to inpatient rehabilitation. The recovery curve is steep at first and then gradual.
For CIPN, treatment is mostly supportive — dose adjustment of the offending chemotherapy when possible, physical therapy, and time. There are no FDA-approved preventive medications specifically for pediatric CIPN.
For juvenile CIDP, IVIG, corticosteroids, and plasma exchange are the main tools, often used in some combination over a long arc.
For nutritional causes, replacement is the answer — and it tends to work.
Across all causes, three pediatric-specific principles matter. First, physical therapy is more powerful in children because their nervous systems are still adapting. Early, consistent PT pays off. Second, bracing decisions need to be revisited as a child grows — feet change, AFOs need refitting, gait changes. Third, the emotional load is real, both for the child and for the parent. A diagnosis is not just a medical event; it is a family event. Our piece on neuropathy and mental health applies as much to families as to individuals.
School Accommodations and 504 Plans

This is the practical chapter that most clinical articles skip, and it might be the most important section for many families.
A child with a chronic neuropathy almost always qualifies for a 504 Plan under Section 504 of the Rehabilitation Act. According to Nemours KidsHealth, a 504 Plan is a formal agreement between the family and the school that lays out the specific accommodations a child will receive in the regular classroom. It is different from an IEP (Individualized Education Program), which is for children whose disability requires specialized instruction. Most kids with neuropathy need the 504 path, not the IEP path — they don't need different curriculum, they need different conditions.
Common, sensible accommodations for a child with neuropathy include:
- Permission to use the elevator or take stairs slowly with a companion
- Modified P.E. or physical therapy instead of P.E.
- Extra time between classes to accommodate slower walking
- Permission to use a laptop, tablet, or scribe for handwriting-heavy work
- Permission to have a water bottle and take breaks for fatigue
- Seating near the door or near the front for safety and engagement
- Modified or excused recess if outdoor terrain is unsafe
- Allowance for mid-day rest in the nurse's office
- Bracing-friendly dress code adjustments
- Field trip accommodations (golf cart access, accessible buses)
- Test-taking accommodations: extended time, breaks, separate room if fatigue is a factor
- A buddy system in emergencies (fire drills, lockdowns)
The process typically goes: parent requests a 504 evaluation in writing → school 504 team (usually principal, school nurse, counselor, classroom teachers) reviews medical documentation → meeting is scheduled → plan is drafted, agreed to, and implemented. Bring a letter from the pediatric neurologist. Bring specific examples. Be friendly, be firm, and remember the school is required by federal law to participate in good faith.
The Emotional Impact on the Child and Family
I want to talk about this part as a grandmother, not as a researcher. Because you cannot lift a clinical paper off a shelf and find what it feels like when the pediatric neurologist says the words for the first time.
For the child, the experience varies wildly with age. A four-year-old absorbs the diagnosis through their parents' faces. A nine-year-old can feel the shame of being the slowest one in P.E. and not understand it is not their fault. A twelve-year-old can feel suddenly different from their friends. A teenager can be furious that their body is telling them something they didn't ask to hear. Each of these reactions is normal. None of them are forever.
For the parent, the experience is grief and protectiveness colliding. There is grief for the imagined future — the easy childhood you pictured, the sports career, the unblemished body. And there is the protective surge that wants to take this on yourself instead of letting your child carry it. Both are real. Both pass into something more bearable, with time and the right support.
For siblings, the diagnosis can quietly reshape family attention in ways that need conscious balance. Brothers and sisters of children with chronic conditions sometimes feel invisible. Family therapists call this the well-sibling effect, and it is worth talking about openly.
For grandparents, like me — we are often the steady presence. We've been through hard things. We can bring perspective and quiet help. What grandparents should not do is minimize (“I had a sore foot for years and I was fine”) or catastrophize (“I read on the internet…”). What we should do is show up, listen, and ask “what would actually help right now?”
The families I have known who weather this best share a few habits. They build a small, trusted team — pediatric neurologist, primary care doctor, PT, teacher, school nurse, one wise friend — and they trust that team. They learn the names of things and refuse to be afraid of jargon. They let the child know early and in age-appropriate language what is happening, because secrets create more anxiety than truth. They find another family living with the same condition, even if it takes a while. And they take care of themselves, because parenting through a chronic diagnosis is a marathon, not a sprint.
Where to Begin if You're at the Beginning

If you are a parent reading this because you suspect something is wrong, here is what I would do in your shoes:
Questions to bring to the pediatric neurologist
Bring this list to your appointment. Take notes on the answers — you will not remember everything later.
- What conditions are on your differential diagnosis right now?
- Which test results would change the picture, and what are you watching for?
- If this is genetic, what is the inheritance pattern, and should other family members be evaluated?
- What should I watch for between now and the next visit that would warrant calling sooner?
- Are there activities I should restrict, encourage, or modify in the meantime?
- What would you recommend I tell my child about what is happening, given their age?
- Is there a pediatric physical therapist or occupational therapist you'd recommend?
- Which support organizations or family communities have you seen help families like ours?
- How often will we follow up, and how do I reach you between visits?
- Could you write a letter for the school summarizing the diagnosis and recommended accommodations?
Start a journal. Write down what you observe — when she trips, what she says about her hands, when his teacher mentioned slowing down. Take a few short videos. Patterns become clearer on paper than they are in memory.
Ask the pediatrician for a referral to pediatric neurology. Be specific. “I'd like an evaluation by pediatric neurology because I'm seeing a pattern of X, Y, and Z.” If the first pediatrician demurs and the pattern persists, see a different pediatrician. You are allowed to be the squeaky wheel.
Bring family medical history to the first appointment. CMT is genetic, and a quiet uncle with high arches and “weak ankles” is suddenly relevant.
Ask the pediatric neurologist what the differential diagnosis is, what testing they recommend, and what you should watch for between visits. Write the answers down.
If a diagnosis is given, ask for a written summary, ask about a 504 evaluation at school, and ask whether there is a family support organization for that specific condition. There almost always is.
And then breathe. The first weeks are the hardest. The maps fill in over time. The team gets bigger. The child grows, and so do you.
I have known a lot of families who stood in this doorway. I have not yet known one whose child became less of who they were because of a neuropathy diagnosis. Most became more — more thoughtful, more resilient, more aware of what their bodies could and could not do. Their families learned things they would not have learned otherwise. There is no upside to a hard diagnosis, but there is a way through. You will find it.
Frequently Asked Questions
Can children really get peripheral neuropathy?
Yes. While it is much less common in children than in adults, peripheral neuropathy in kids is a real and recognized category. The most frequent cause is genetic — Charcot-Marie-Tooth disease, which affects roughly one in 2,500 people and most often shows up between ages 5 and 15. Other pediatric causes include Guillain-Barré syndrome, chemotherapy-induced neuropathy in children with cancer, juvenile CIDP, vitamin B12 deficiency, and complications from diabetes or autoimmune conditions.
What are the earliest signs of neuropathy in a child?
Parents most often notice clumsiness that doesn't fade with age, frequent tripping, foot deformities like high arches or hammer toes, weakness in running or climbing stairs, complaints about sock seams or shoe linings, plateauing or worsening handwriting, dropped utensils, and difficulty with buttons or shoelaces. After an illness, sudden ascending weakness in the legs is a red-flag pattern that warrants urgent evaluation.
What kind of doctor diagnoses pediatric neuropathy?
A pediatric neurologist is the specialist who diagnoses and manages most cases. The pediatrician is typically the first stop and will refer to pediatric neurology when symptoms suggest a nerve issue. Depending on the cause, the team may also include a geneticist (for CMT), a pediatric oncologist (for chemotherapy-related nerve damage), a rheumatologist (for autoimmune causes), or a physical medicine and rehabilitation specialist.
How is neuropathy tested in a young child?
The main diagnostic tools are nerve conduction studies (NCS) and electromyography (EMG), which measure how electrical signals travel through nerves. These tests are uncomfortable but not dangerous, and pediatric neurology centers have technicians who specialize in working with children. Genetic testing is often used if CMT is suspected. Blood work, vitamin levels, and sometimes a lumbar puncture round out the workup. Diagnosis can take weeks because the differential is wide.
Will my child outgrow it?
It depends entirely on the cause. Acute conditions like Guillain-Barré syndrome have an excellent recovery rate in children — 90 to 95 percent recover fully or near-fully. Nutritional neuropathies often reverse with proper supplementation. Chemotherapy-induced neuropathy usually improves once treatment ends, though some children carry lasting effects. Genetic conditions like CMT do not go away, but they typically progress slowly, and most children grow up to live full lives with appropriate management.
Does CMT affect my child's intelligence?
No. Charcot-Marie-Tooth disease almost never affects the brain, intelligence, or learning. CMT is a peripheral nerve condition — it affects the nerves serving the limbs, not the central nervous system. Children with CMT learn, reason, and develop emotionally on the same trajectory as their peers. They typically need accommodations for physical activities and fine motor tasks, not for academics.
Can my child get a 504 Plan for neuropathy?
Almost always, yes. Section 504 of the Rehabilitation Act covers any child whose disability substantially limits a major life activity, and walking, fine motor skills, and stamina all qualify. A 504 Plan is a formal agreement that lays out specific accommodations — extra time between classes, modified P.E., test-taking accommodations, mobility supports, and others. Parents can request an evaluation in writing through the school. Bring documentation from the pediatric neurologist and a list of specific challenges your child experiences during the school day.
Is pediatric neuropathy painful?
It can be, though not always. CMT is often more about weakness and structural foot changes than pain, especially in younger children. CIPN (chemotherapy-related) and CIDP can include pain. GBS frequently includes pain, especially during the acute phase. Young children often cannot describe pain in adult terms — they might call it “tired feet,” refuse to walk, or become unusually irritable. Tracking these behavioral signs is part of caring for a child with neuropathy.


