Prediabetes and Neuropathy: How Borderline Blood Sugar Damages Nerves
Here's something that surprises most people: you don't need a diabetes diagnosis to develop neuropathy. If your blood sugar is even slightly elevated — what doctors call prediabetes — your nerves may already be taking damage. And it's not subtle. Research shows that prediabetic neuropathy can be just as severe as neuropathy in people with newly diagnosed type 2 diabetes.
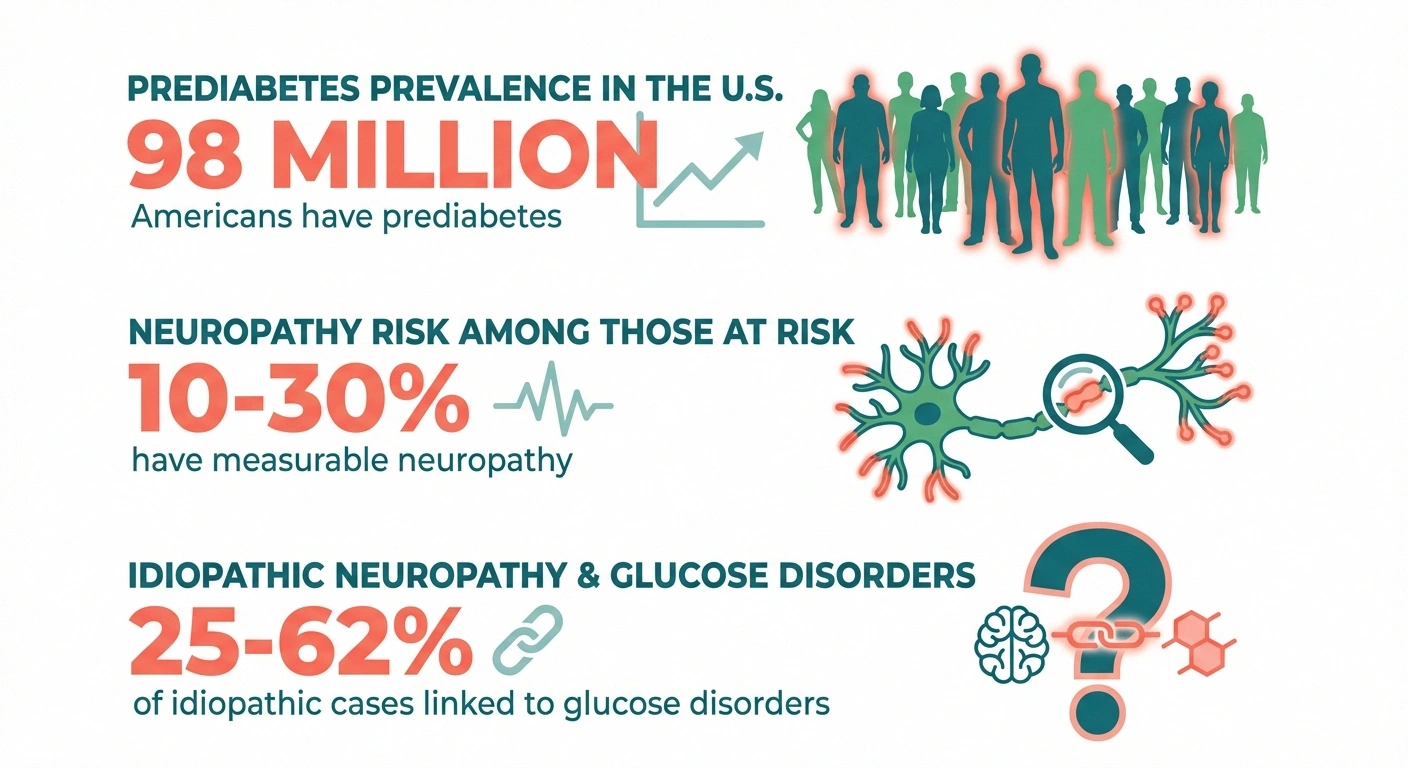
I bring this up because prediabetes affects roughly 98 million American adults — about 1 in 3 — and most of them have no idea their nerves are at risk. If you've been told your blood sugar is “a little high” or “borderline,” or if you have tingling in your feet that no one can explain, this article may connect some important dots.
What Is Prediabetes?
Prediabetes is the stage where your blood sugar is higher than normal but not high enough for a type 2 diabetes diagnosis. The specific numbers:
- Fasting blood glucose: 100-125 mg/dL (normal is below 100; diabetes is 126+)
- HbA1c: 5.7%-6.4% (normal is below 5.7%; diabetes is 6.5%+)
- Oral glucose tolerance test: 140-199 mg/dL at 2 hours (normal is below 140; diabetes is 200+)
The critical thing to understand: prediabetes is not a “pre-disease.” It's an active metabolic condition where damage is already happening — including to your nerves. The name gives people a false sense of security, as if they're in a waiting room before the real problem starts. In reality, the waiting room is the problem.
How Borderline Blood Sugar Damages Nerves
The nerve damage in prediabetes primarily affects small nerve fibers — the tiny, unmyelinated C-fibers and thinly myelinated Aδ fibers that detect pain, temperature, and light touch. This is important because standard nerve conduction studies often miss small fiber damage entirely, which is why many people with prediabetic neuropathy are told their tests are “normal.”
Several mechanisms drive this damage:
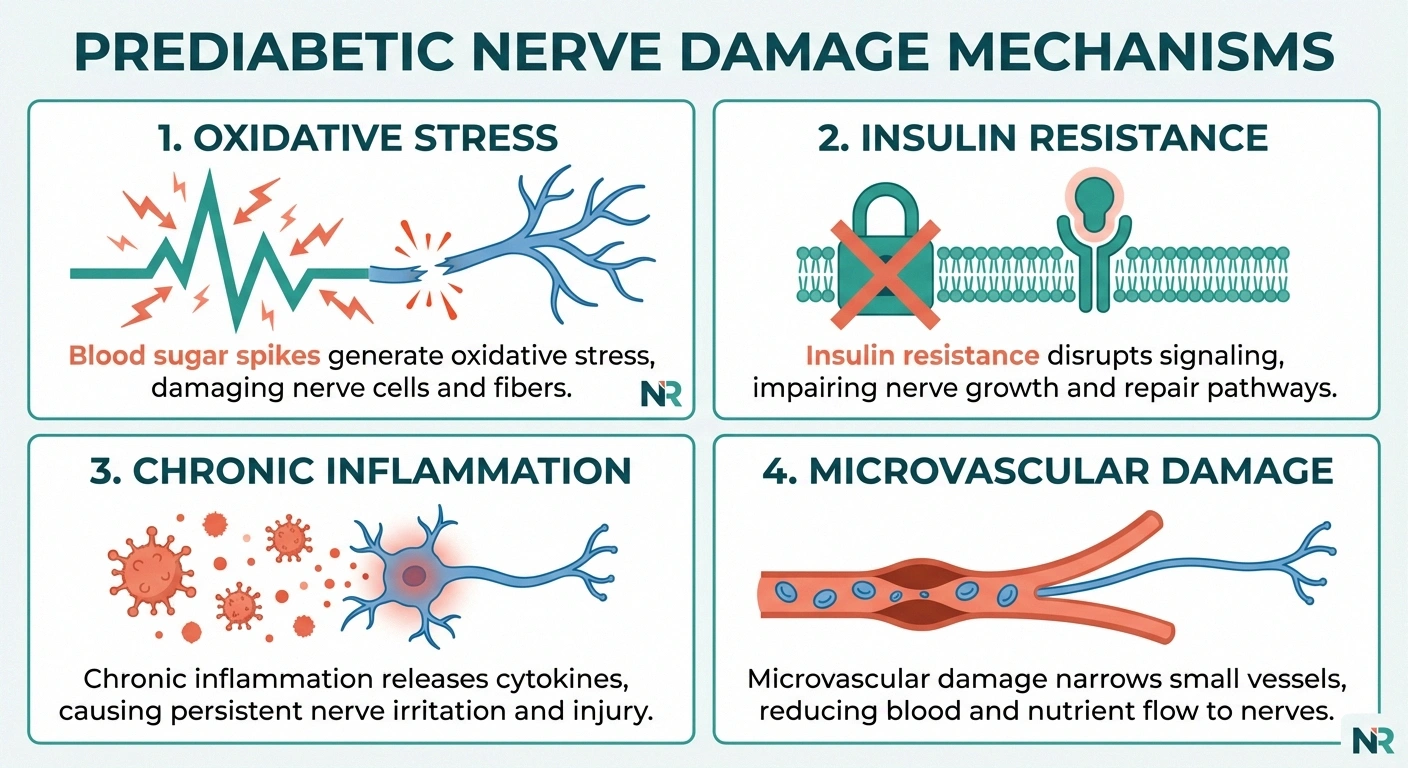
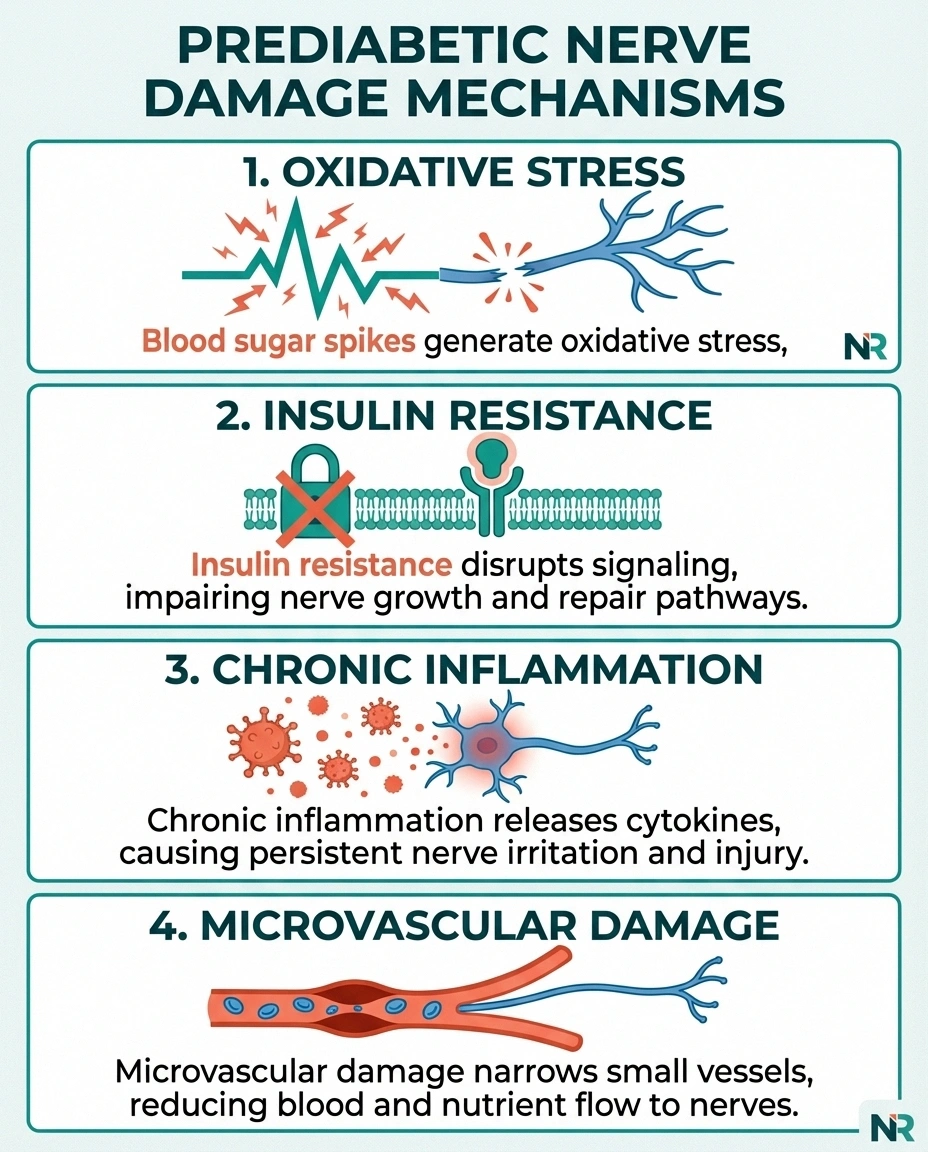
Blood Sugar Spikes and Oxidative Stress
Even in prediabetes, blood sugar levels spike after meals — sometimes dramatically. These post-meal spikes generate reactive oxygen species (free radicals) that directly damage nerve cell membranes, mitochondria, and DNA. Unlike sustained high blood sugar, these intermittent spikes may be particularly harmful because they trigger repeated cycles of oxidative injury followed by incomplete repair.
A landmark review in the Journal of Diabetes Investigation found that the pathophysiology of nerve injury in prediabetes and early type 2 diabetes differs from that in longstanding type 1 diabetes — suggesting that metabolic dysfunction, insulin resistance, and inflammation play proportionally larger roles than hyperglycemia alone.
Insulin Resistance and Nerve Signaling
Nerve cells have insulin receptors and depend on insulin signaling for survival and function. In prediabetes, insulin resistance means these receptors don't respond normally. This disrupts the neurotrophic support that keeps nerve cells alive and functioning. Think of insulin resistance as cutting off a supply line — the nerve cells are still there, but they're not getting the resources they need to maintain themselves.
Chronic Low-Grade Inflammation
Prediabetes and metabolic syndrome are associated with elevated levels of inflammatory markers — TNF-α, IL-6, C-reactive protein. This chronic inflammation doesn't just affect your blood vessels and joints; it attacks the endoneurial microenvironment where your nerve fibers live. Over time, this inflammatory assault degrades the delicate small fibers that are already the most vulnerable.
Microvascular Damage
Your peripheral nerves are supplied by tiny blood vessels called vasa nervorum. Even modestly elevated blood sugar damages these microvessels, reducing blood flow and oxygen delivery to nerve fibers. The smallest fibers — the ones most affected in prediabetes — are the most sensitive to this reduced oxygen supply.
How Common Is Neuropathy in Prediabetes?
More common than most doctors realize. A 2021 systematic review in BMJ Open Diabetes Research & Care found that the prevalence of peripheral neuropathy in people with prediabetes ranges from 10% to 30%, depending on the diagnostic method used. When sensitive tests like skin biopsy or corneal confocal microscopy are used instead of standard nerve conduction studies, the numbers climb to the higher end of that range.
A 2024 study published in Journal of the Peripheral Nervous System reported that prediabetes was associated with similar risks for peripheral neuropathy and similar severity of nerve dysfunction as new-onset diabetes — meaning by the time someone gets a diabetes diagnosis, the nerve damage may have been accumulating for years.
Perhaps most revealing: when researchers take patients with idiopathic neuropathy — neuropathy with no known cause — and test them for glucose metabolism disorders, they find prediabetes or impaired glucose tolerance in 25-62% of cases. Many people diagnosed with “neuropathy of unknown cause” actually have neuropathy from prediabetes that was never properly tested for.
Symptoms of Prediabetic Neuropathy
Because prediabetes primarily damages small nerve fibers, the symptoms differ somewhat from the classic neuropathy symptoms that most people associate with full-blown diabetes:

Burning pain in feet or hands — often the first symptom, frequently worse at night. The pain may be described as hot, stinging, or like standing on hot sand. This is characteristically worse in the evening and can significantly disrupt sleep.
Sharp, stabbing pains — brief, intense jolts that come without warning. These can occur in the feet, legs, or even the trunk.
Temperature sensitivity changes — difficulty distinguishing hot from cold, or an increased sensitivity to temperature extremes. Some people find that warm water feels scalding or that mild cold causes disproportionate pain.
Tingling or “pins and needles” — a constant or intermittent prickling sensation, typically starting in the toes and gradually moving upward.
Autonomic symptoms — because small fibers also control autonomic functions, you may notice changes in sweating (too much or too little in the feet), dry skin, or digestive changes. These are often overlooked as neuropathy symptoms.
Notably, you may experience significant pain without numbness. This is a hallmark of small fiber neuropathy — the pain fibers are damaged and misfiring, but the larger sensory fibers that detect touch and pressure are still intact.
Getting the Right Diagnosis
Diagnosing prediabetic neuropathy requires the right tests — and many standard approaches miss it entirely.
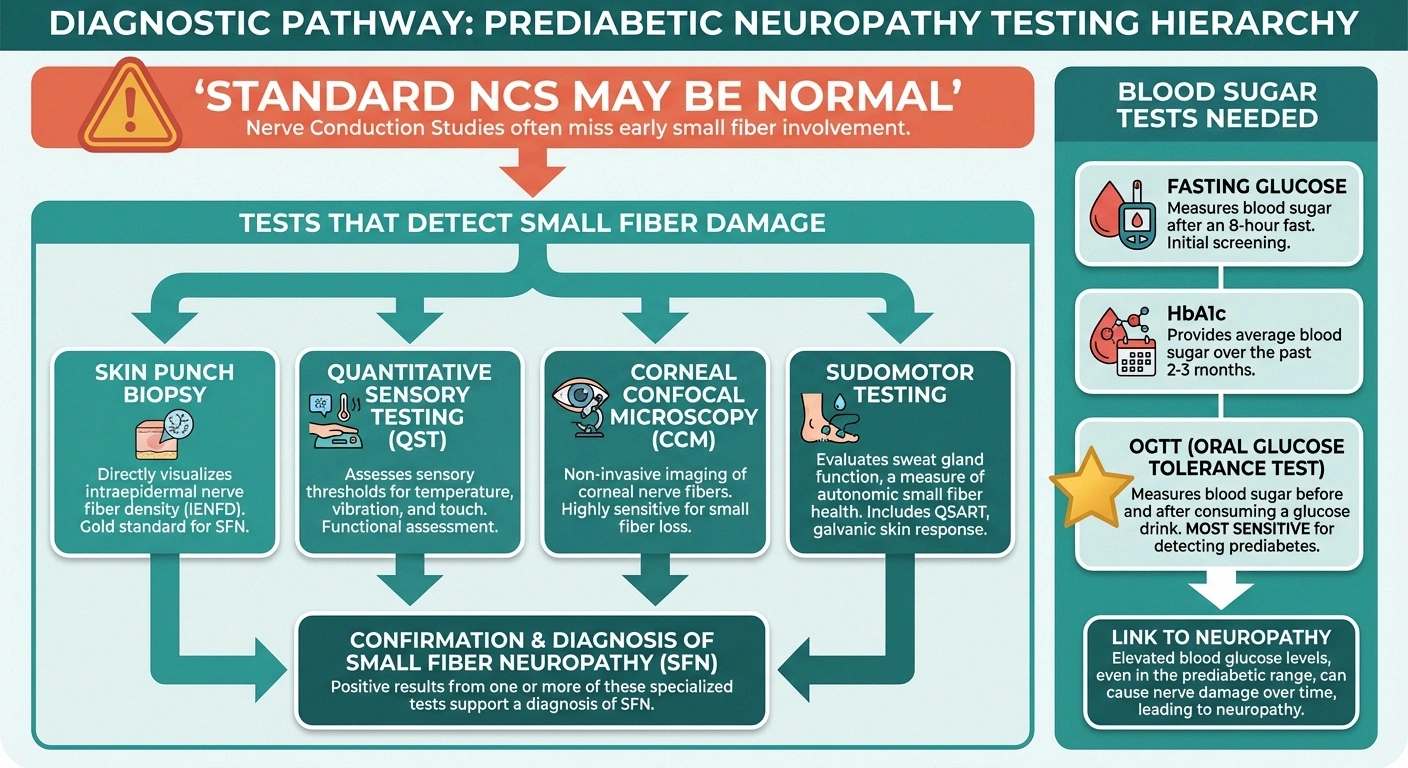
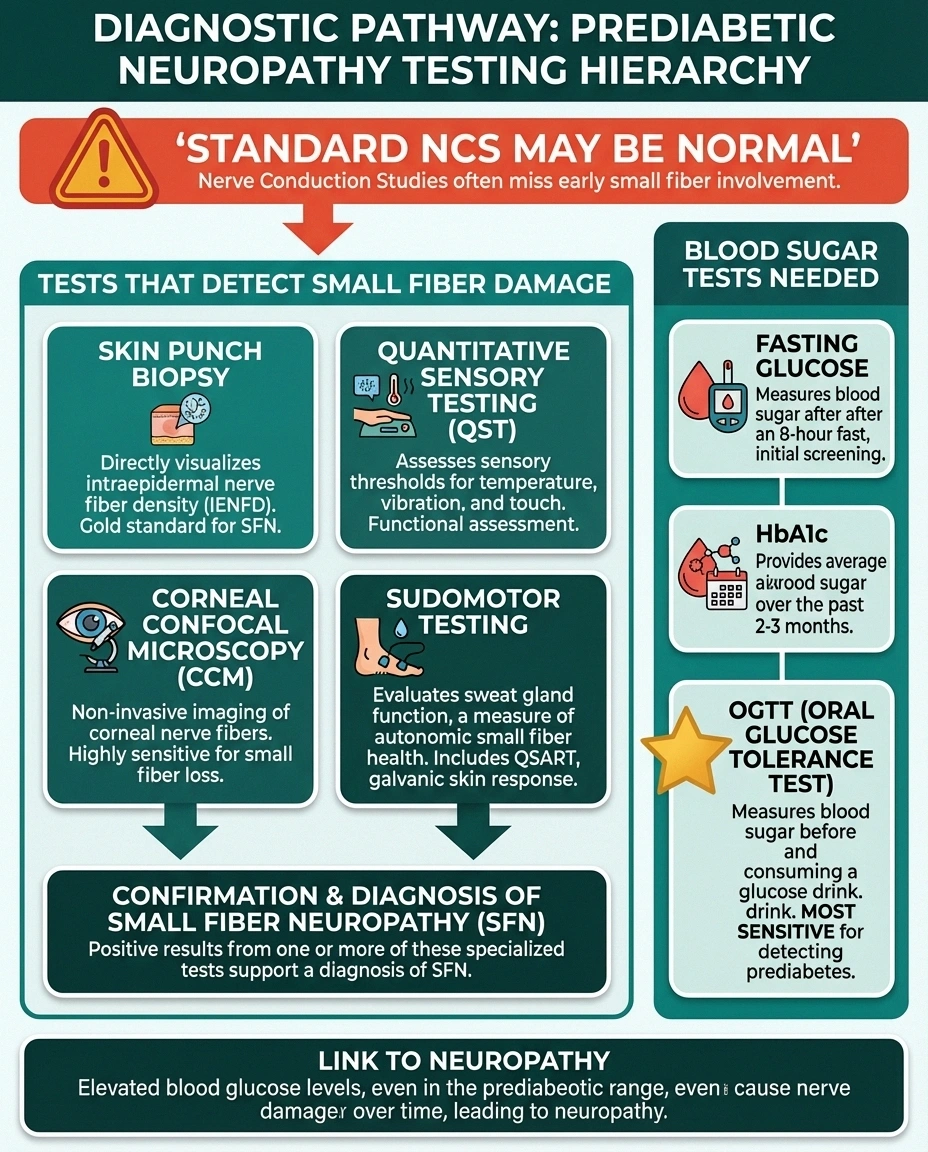
Standard nerve conduction studies (NCS) are often normal. Because prediabetes predominantly damages small fibers, and NCS primarily measures large fiber function, a “normal” NCS does not rule out prediabetic neuropathy. If your doctor tells you your nerve test was normal and therefore you don't have neuropathy, push for additional testing.
Tests that can detect small fiber damage:
- Skin punch biopsy: Measures the density of small nerve fibers (intraepidermal nerve fiber density, or IENFD) — the gold standard for diagnosing small fiber neuropathy
- Quantitative sensory testing (QST): Measures your ability to detect specific sensations like vibration, temperature, and pain thresholds
- Corneal confocal microscopy: A non-invasive imaging technique that visualizes small nerve fibers in the cornea — increasingly used as a rapid screening tool
- Sudomotor function testing: Measures sweat gland function, which depends on small nerve fibers
Blood sugar testing should go beyond fasting glucose. A standard fasting glucose test can miss prediabetes. Request an HbA1c and a 2-hour oral glucose tolerance test (OGTT). The OGTT is particularly important because it catches impaired glucose tolerance — people whose blood sugar spikes dramatically after meals but returns to normal range when fasting. These post-meal spikes may be the primary driver of nerve damage.
Can Prediabetic Neuropathy Be Reversed?
Here's the genuinely good news: prediabetic neuropathy is one of the most treatable forms of neuropathy, particularly when caught early. Unlike advanced diabetic neuropathy where nerve damage becomes permanent, the small fiber damage in prediabetes has a real chance of reversing — if you address the underlying metabolic dysfunction.

Research suggests that returning blood sugar levels to normal ranges can lead to measurable improvements in nerve fiber density and symptom reduction. A 2023 study in Diabetes/Metabolism Research and Reviews found that normalizing HbA1c levels was associated with improvements in nerve conduction measures and neuropathic deficits, suggesting that regression from prediabetes to normal glucose tolerance may actually reverse nerve damage.
The key strategies for reversing prediabetes — and potentially reversing neuropathy with it — are:
Dietary Changes
An anti-inflammatory, blood-sugar-stabilizing diet is the foundation. Focus on reducing refined carbohydrates and added sugars, increasing fiber intake (slows glucose absorption), eating adequate protein with each meal, choosing anti-inflammatory fats (omega-3s, olive oil, nuts), and minimizing processed food. The Mediterranean-style diet pattern has the strongest evidence for both blood sugar management and reducing inflammation.
Exercise
Regular physical activity improves insulin sensitivity more effectively than most medications. Both aerobic exercise and resistance training help, and the combination is most effective. Even walking 30 minutes a day can make a measurable difference. The Diabetes Prevention Program — the largest lifestyle intervention study ever conducted — found that moderate exercise combined with modest weight loss reduced progression to diabetes by 58%.
Weight Management
Losing just 5-7% of body weight can significantly improve insulin sensitivity and reduce the metabolic stress driving nerve damage. Importantly, the rate of weight loss matters — gradual, sustained weight loss is better for your nerves than rapid drops. The goal is metabolic improvement, not a number on the scale.
Targeted Supplementation
Alpha-lipoic acid (600mg/day) has the strongest evidence for neuropathic pain in the context of glucose metabolism disorders. B vitamins should be checked and supplemented if deficient. Magnesium supports both glucose metabolism and nerve function.
When Prediabetes Goes Unrecognized: The Idiopathic Neuropathy Connection
If you've been diagnosed with idiopathic neuropathy — neuropathy with no identified cause — consider whether prediabetes may be the missing piece. The connection is well-established in the research literature but frequently missed in clinical practice.
Standard screening for diabetes in neuropathy patients typically involves only a fasting glucose or HbA1c. But these tests can miss impaired glucose tolerance, which requires a 2-hour OGTT to detect. If your fasting glucose and HbA1c are “normal” but you have unexplained neuropathy, specifically ask your doctor for an oral glucose tolerance test.
This matters because finding a cause changes the treatment strategy. Idiopathic neuropathy is managed primarily with symptom control — pain medications, lifestyle adjustments. But prediabetic neuropathy can be addressed at its root by correcting the metabolic dysfunction, with a real chance of reversing the nerve damage rather than just managing it.
Monitoring Your Progress
If you've been diagnosed with prediabetes and neuropathy (or you're working on reversing prediabetes), tracking your progress is important both for motivation and for catching changes early:
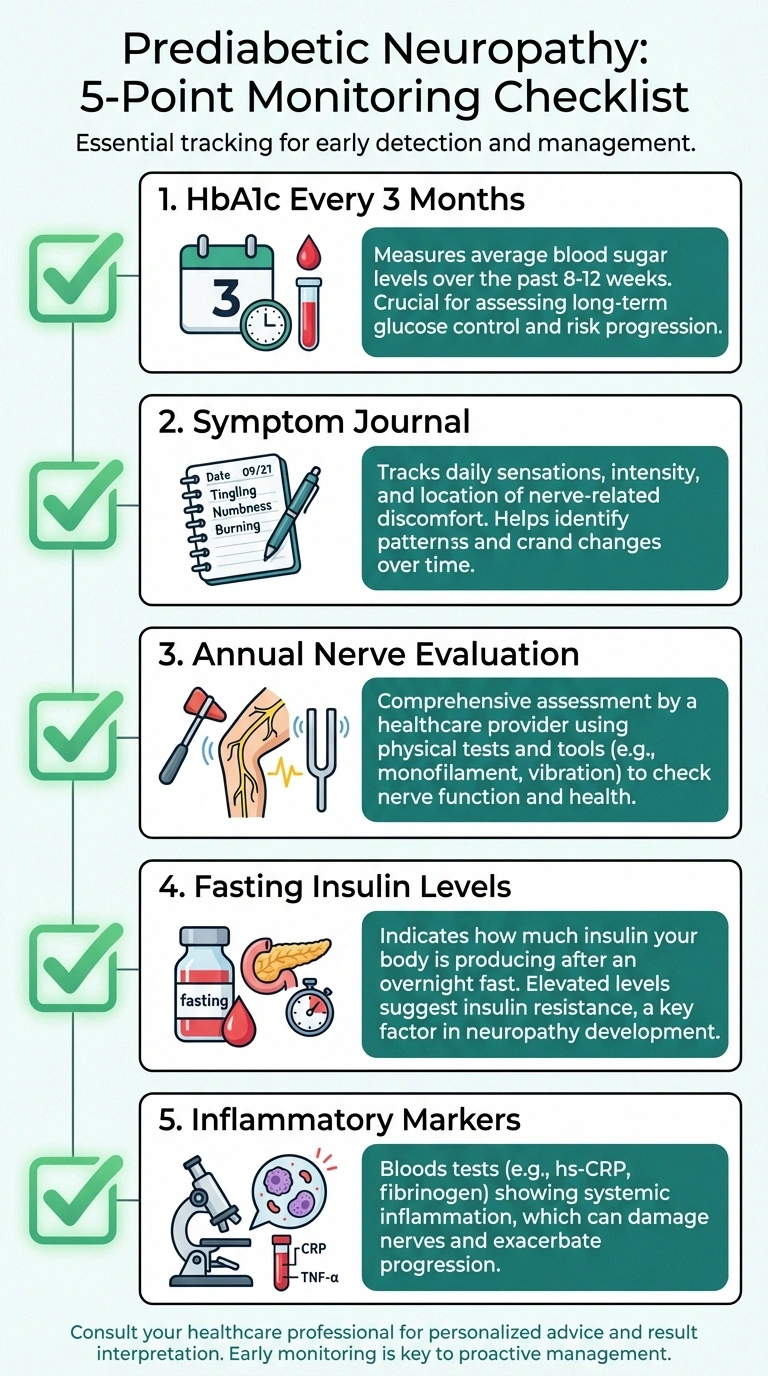
- HbA1c every 3 months — track your glucose control trend
- Symptom journal — track pain levels, location, triggers, and changes over time
- Annual nerve evaluation — repeat QST, skin biopsy, or other small fiber tests to measure objective improvement
- Fasting insulin levels — measures insulin resistance directly, can detect improvement before glucose numbers change
- Inflammatory markers — CRP, ESR — tracking inflammation reduction
Improvements in nerve symptoms may lag behind metabolic improvements by several months. Small nerve fibers regenerate, but they do so slowly — typically 1-2 inches per month. Be patient with the process and focus on sustaining the lifestyle changes rather than expecting immediate symptom relief.
Talk to Your Doctor
If you have prediabetes and any symptoms of neuropathy — or if you have unexplained neuropathy and haven't been thoroughly tested for glucose metabolism disorders — bring this up with your doctor at your next visit. The combination of proper testing, early intervention, and lifestyle changes gives you the best chance of stopping and potentially reversing nerve damage before it becomes permanent.
Prediabetes is a window of opportunity. The nerves are telling you something is wrong before the situation becomes irreversible. Listening to that signal — and acting on it — can change your long-term trajectory.
Frequently Asked Questions
Can prediabetes really cause neuropathy if I don't have diabetes?
Yes. Multiple studies confirm that prediabetes — even blood sugar levels that are only slightly above normal — can cause peripheral neuropathy, primarily affecting small nerve fibers. Research shows 10-30% of people with prediabetes have measurable neuropathy. The nerve damage occurs through blood sugar spikes, insulin resistance, oxidative stress, and chronic inflammation, all of which are active in prediabetes.
Why did my nerve conduction test come back normal if I have symptoms?
Standard nerve conduction studies primarily measure large fiber function. Prediabetes typically damages small fibers first, which these tests cannot detect. A normal nerve conduction study does not rule out small fiber neuropathy. Ask your doctor about a skin punch biopsy, which measures small nerve fiber density and is the gold standard for detecting the type of neuropathy most common in prediabetes.
If I reverse my prediabetes, will my neuropathy go away?
There is good evidence that reversing prediabetes — returning blood sugar and insulin sensitivity to normal — can lead to measurable improvements in nerve function and symptom reduction. Small nerve fibers can regenerate, though the process is slow (about 1-2 inches per month). Early intervention gives the best chance of reversal. Long-standing damage is harder to reverse but may still improve with sustained metabolic correction.
What blood tests should I ask for if I suspect prediabetic neuropathy?
Request a fasting glucose, HbA1c, and a 2-hour oral glucose tolerance test (OGTT). The OGTT is the most important because it catches impaired glucose tolerance that fasting tests miss. Also ask for fasting insulin levels (measures insulin resistance directly), a lipid panel, inflammatory markers (CRP), and a complete metabolic panel. For neuropathy-specific testing, ask about skin biopsy for intraepidermal nerve fiber density.
Is prediabetic neuropathy different from diabetic neuropathy?
Yes, in important ways. Prediabetic neuropathy predominantly affects small nerve fibers and is driven more by insulin resistance, inflammation, and metabolic syndrome components than by sustained hyperglycemia alone. It is also more likely to present as painful neuropathy without significant numbness, and it is more responsive to lifestyle interventions. Diabetic neuropathy in advanced stages affects both large and small fibers and is often more difficult to reverse.
Does metformin help with prediabetic neuropathy?
Metformin is sometimes prescribed for prediabetes to prevent progression to diabetes, and it may help indirectly by improving blood sugar control. However, long-term metformin use can cause B12 deficiency, which itself causes neuropathy. If you take metformin, have your B12 levels monitored regularly and supplement if needed. Lifestyle interventions — diet, exercise, and weight management — have stronger evidence than metformin for both reversing prediabetes and improving neuropathy outcomes.