The first time someone in our support group brought in a small device with an ear clip and asked if it could really fix her neuropathy, I had to be honest: I didn't know yet. That was a year and a half ago. I've spent a lot of evenings since then reading studies, talking to specialists, and watching the research evolve in real time.
Vagus nerve stimulation (VNS) is one of the most genuinely interesting frontiers in neuropathy treatment, and one of the easiest to be misled about. The early data is real. So is the marketing hype. So is the gap between the two. Let me walk you through what we know — and what I'd ask before spending money on it.
What Is the Vagus Nerve, and Why Stimulate It?
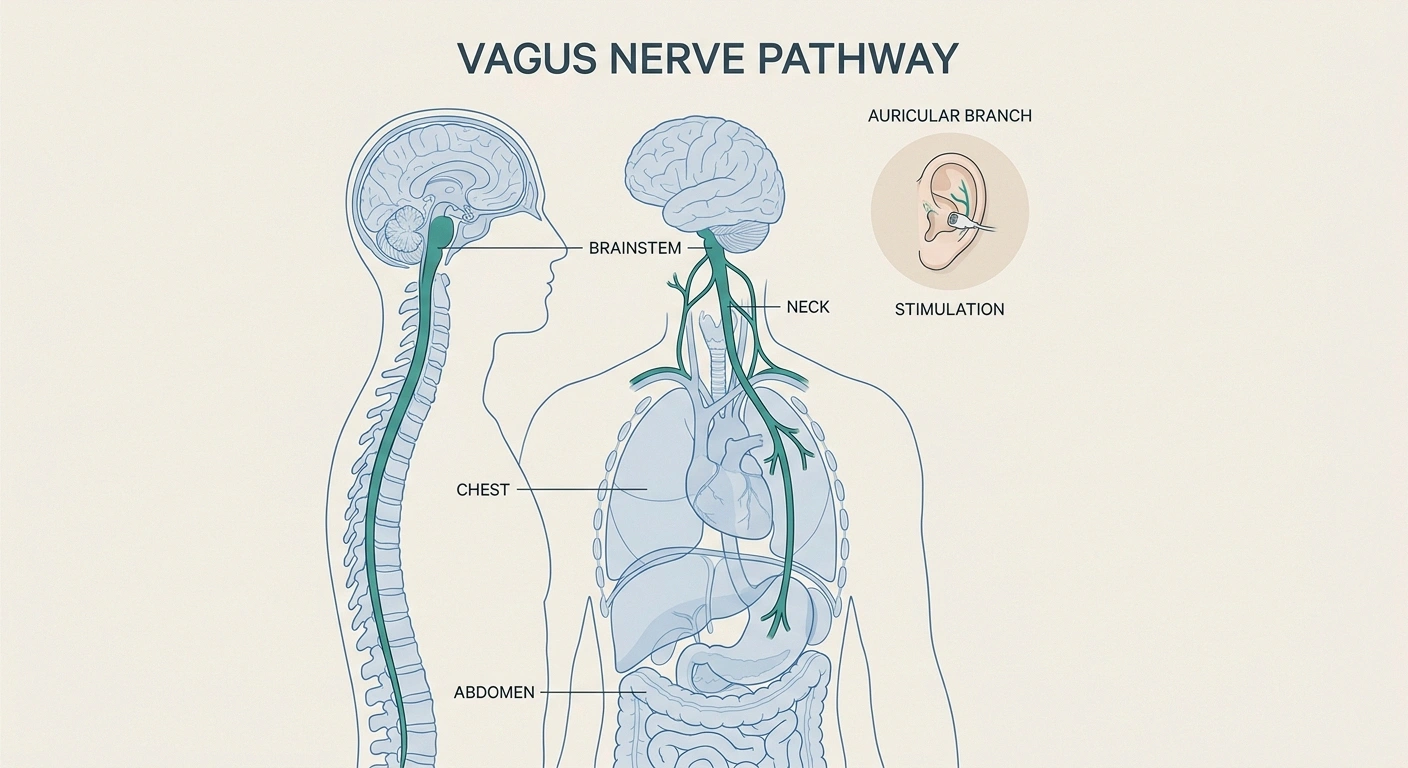
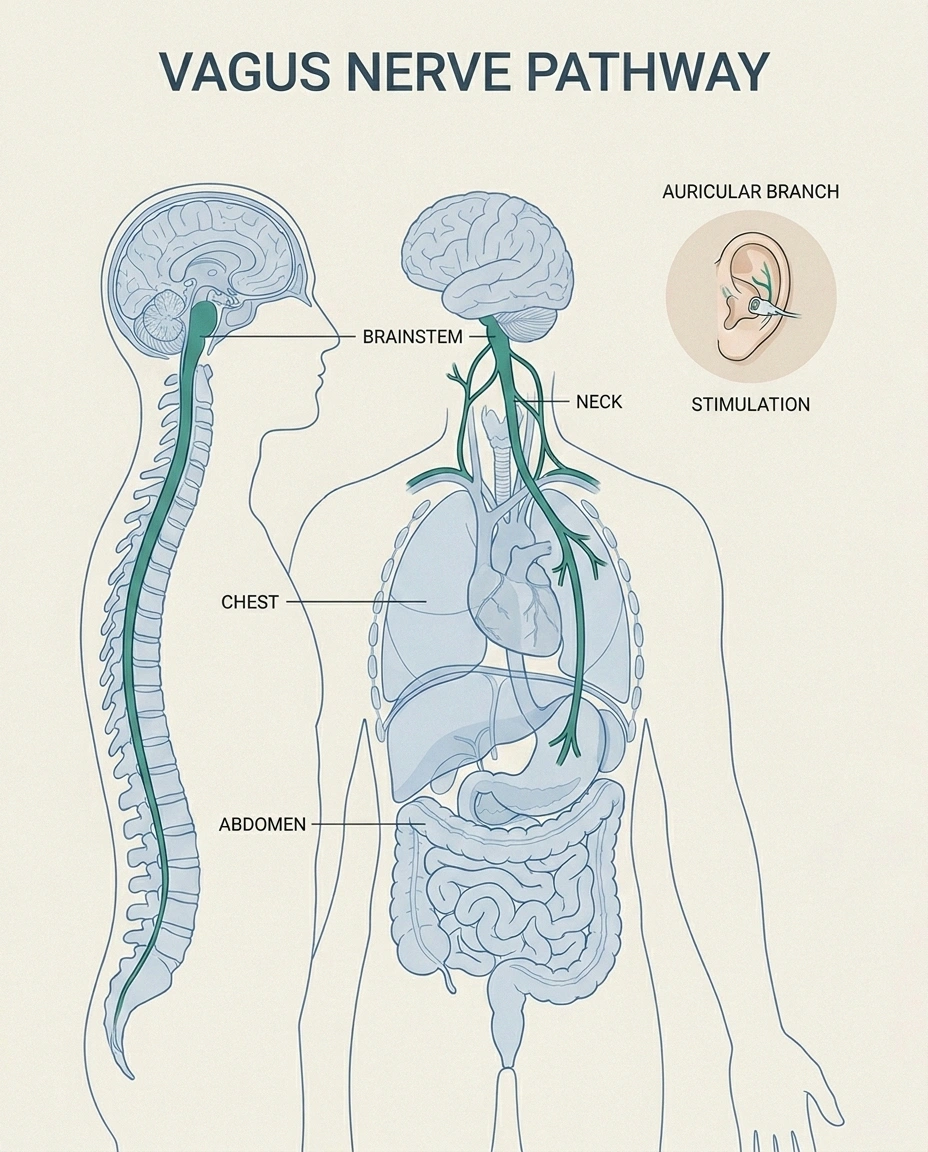
Your vagus nerve is the longest cranial nerve in your body. It runs from your brainstem down through your neck, branches into your chest and abdomen, and connects nearly every internal organ to your central nervous system. It carries roughly 80% of the signals from your body up to your brain — heart rate, breathing, gut activity, immune signals, the works.
Key Takeaway
Transcutaneous auricular vagus nerve stimulation (taVNS) is a non-invasive, ear-clip-sized device that targets the body's anti-inflammatory pathway. Early research is promising for diabetic and chemotherapy-induced neuropathy. It is not yet FDA-approved for neuropathy.
The reason researchers are interested in stimulating it for neuropathy comes down to one specific job the vagus nerve does: it serves as the on-off switch for what scientists call the cholinergic anti-inflammatory pathway. When the vagus nerve is active, it tells the immune system to dial down inflammation throughout the body. When it's underactive — which can happen with chronic stress, poor sleep, autonomic dysfunction, or aging — inflammation tends to run higher.
For people with neuropathy, this matters because much of the day-to-day suffering of nerve damage is driven by inflammation: inflamed small fibers, inflamed nerve roots, central sensitization in the spinal cord, autonomic instability that worsens pain perception. If you could reliably calm that inflammation without immunosuppressive drugs, you'd address the engine driving symptoms — not just the symptoms themselves.
That's the theory. Now to the practice.
Two Very Different Devices
The first thing to understand — because most articles online blur this line — is that “vagus nerve stimulation” refers to two completely different categories of treatment.
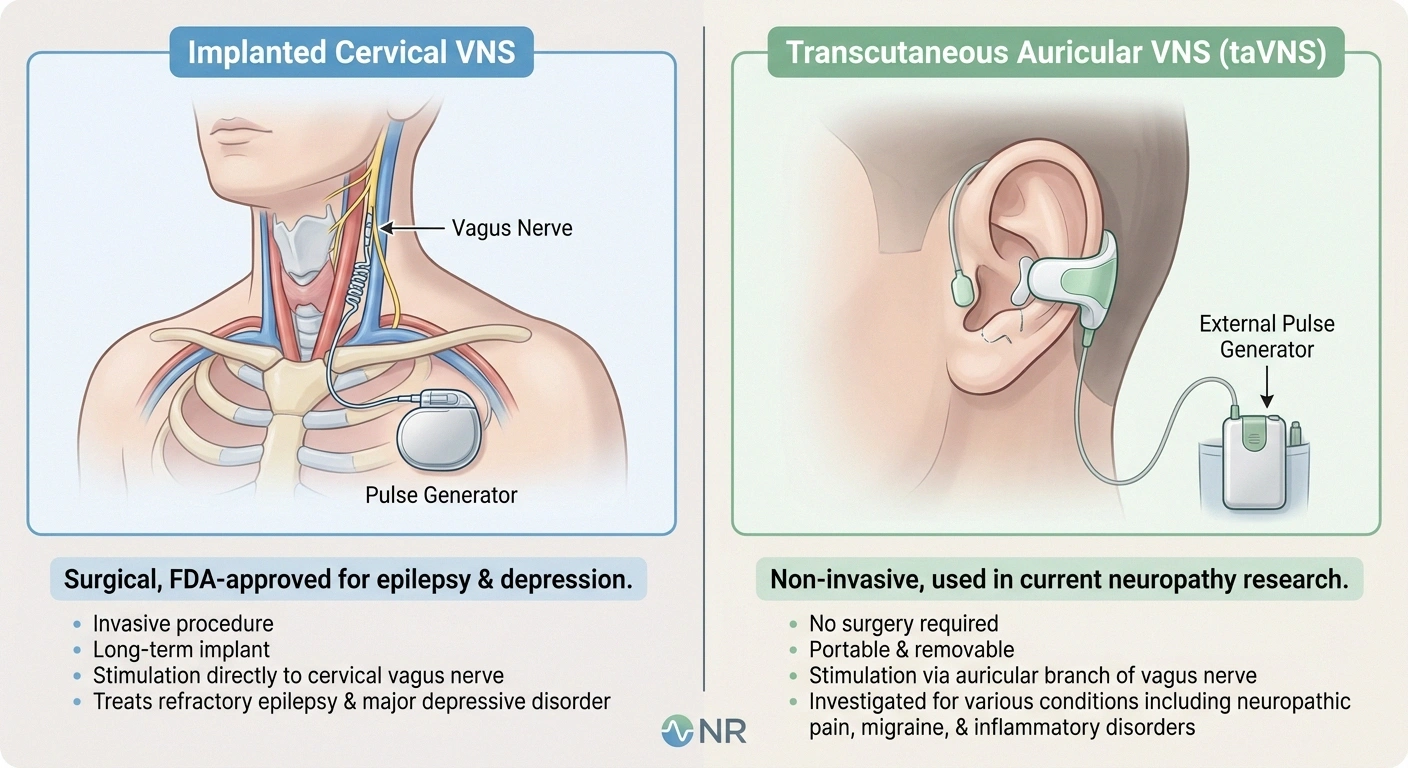
Two Very Different “VNS” Devices
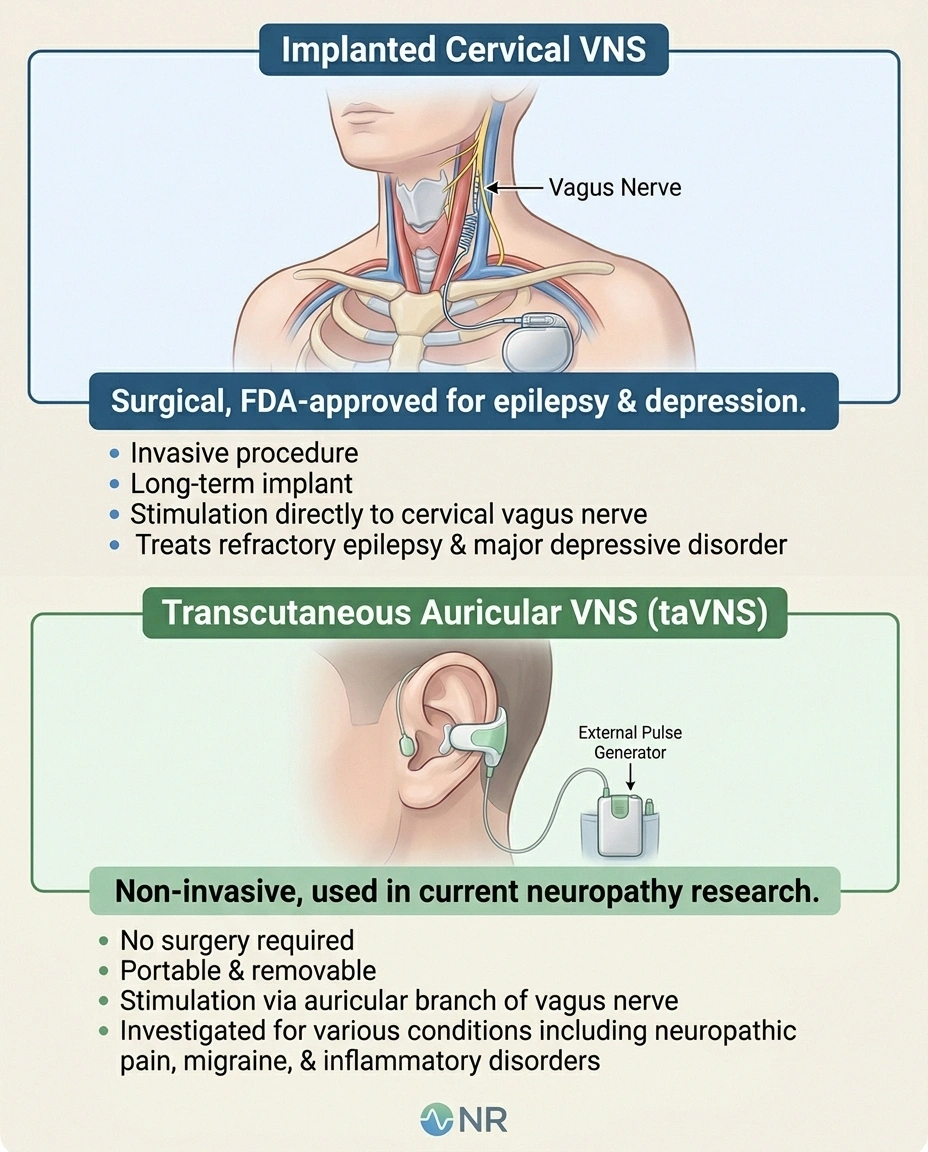
Implanted Cervical VNS
Surgical implant. Pulse generator in chest, electrode wraps around left vagus nerve. FDA-approved for epilepsy and depression. Not used for neuropathy.
Transcutaneous Auricular VNS (taVNS)
Non-invasive ear-clip device targeting the auricular branch of the vagus nerve. 30-min daily sessions. THIS is what current neuropathy research is studying.
1. Implanted Cervical VNS
This is the original VNS technology. A small pulse generator is implanted in the chest wall, similar to a pacemaker. A wire runs from it up through the neck and wraps around the left vagus nerve. The whole thing is controlled by an external programmer.
Implanted VNS is FDA-approved for two conditions: drug-resistant epilepsy and treatment-resistant depression. It is not FDA-approved for peripheral neuropathy. Surgery is required, costs run $20,000–$30,000 in the US, and the procedure carries the typical risks of any device implant — infection, lead displacement, voice changes from proximity to the recurrent laryngeal nerve. For neuropathy alone, this approach is essentially never used.
2. Transcutaneous Auricular VNS (taVNS)
This is the version that's relevant to neuropathy patients today. It's non-invasive, no surgery, no implant. The auricular branch of the vagus nerve travels through the ear, specifically through a small region called the cymba conchae and along the tragus. A small electrode placed against this part of the ear can stimulate the vagus nerve through the skin.
The devices look like an over-ear earpiece or a small clip with attached pads. Sessions typically last 30 minutes once or twice a day. The stimulation feels like a mild tingling or pulsing in the ear — uncomfortable for some people at higher settings, completely tolerable at lower ones.
Almost every modern study on “VNS for neuropathy” uses taVNS, not implanted VNS. Unless you've specifically been referred for an implant for epilepsy or depression, the conversation about VNS for nerve pain is a conversation about taVNS.
What the Research Actually Shows
The taVNS research base for neuropathy is small but growing rapidly. Here's an honest summary of where it stands as of 2026.
🔎 Research Says
A 2024 sham-controlled trial in Frontiers in Pain Research showed taVNS reduced tingling by a median of 2.0 points and pain by 1.5 points in patients with painful peripheral neuropathy. A 2025 Frontiers in Neuroscience study found combined VNS + peripheral nerve stimulation produced prolonged improvement in painful diabetic neuropathy plus reduced hyperglycemia.
Diabetic Peripheral Neuropathy
A 2024 feasibility randomized sham-controlled trial published in Frontiers in Pain Research studied taVNS in Black and Hispanic/Latino patients with painful peripheral neuropathy (mostly diabetic and chemotherapy-induced). Active stimulation reduced tingling by a median of 2.0 points and pain by 1.5 points on standard pain scales. Heart rate variability — a measure of vagal tone — increased during stimulation. The trial was small (a couple of dozen patients), but the directional signal was clean and the effect size was meaningful.
A 2025 paper in Frontiers in Neuroscience went further: combining minimally invasive vagal cranial nerve stimulation with peripheral nerve stimulation produced prolonged improvement in painful diabetic peripheral neuropathy and — interestingly — also reduced hyperglycemia in the participants with type 2 diabetes. The mechanism appears to involve both direct anti-inflammatory effects on nerves and improvements in autonomic regulation of blood sugar.
Several actively recruiting trials (including NCT04539964 and NCT07080749) are looking at taVNS specifically for moderate-to-severe diabetic peripheral neuropathy. Results expected over the next 18–36 months will help define exactly how big the effect is.
Chemotherapy-Induced Peripheral Neuropathy (CIPN)
A 2024 paper in PubMed reported on a randomized exploratory study of transauricular VNS for chemotherapy-induced painful peripheral neuropathy. The findings were positive but cautious: improvements in pain scores and quality of life, with no significant safety issues. Larger phase II/III trials are needed to confirm and quantify the effect.
The treatment options for established chemotherapy-induced neuropathy are limited and disappointing — duloxetine is the only agent with strong supporting evidence, and the symptomatic toolbox is otherwise thin. taVNS is one of the more promising additions to that toolkit being studied — and importantly, it appears safe to combine with cancer treatment.
Inflammatory and Autoimmune Conditions (the Adjacent Evidence)
The strongest large-scale data for VNS so far doesn't come from neuropathy trials at all — it comes from rheumatoid arthritis. A 2025 pivotal randomized controlled trial published in Nature Medicine showed that vagus nerve stimulation produced clinically meaningful reductions in disease activity in rheumatoid arthritis. That's important for our readers because RA, IBD, and other autoimmune conditions often co-occur with autoimmune neuropathies. If VNS calms systemic autoimmunity, it should — in theory — calm immune-driven nerve inflammation by the same mechanism.
The translation from “works for RA” to “works for autoimmune neuropathy” is plausible but not yet proven. Studies are underway.
Where the Evidence Is Quiet
Honest disclosure: there is little to no published data showing meaningful benefit of taVNS for:
- Idiopathic small fiber neuropathy
- Hereditary neuropathies (CMT, etc.)
- Alcoholic neuropathy
- Vitamin-deficiency neuropathies
- Post-herpetic neuralgia (some adjacent data, but not robust)
That doesn't mean taVNS doesn't help these conditions. It means the trials haven't been done. Don't let a marketing pitch confuse “no evidence” with “evidence of no effect.” But also, don't pay for a device on the assumption that an unproven application will work.
How taVNS Actually Works (The Three Mechanisms)
The biology is interesting enough to be worth a paragraph for readers who like to know why.
Three Mechanisms of taVNS
Anti-inflammatory effect
Triggers the cholinergic anti-inflammatory pathway. Reduces TNF-α, IL-6, and other pro-inflammatory cytokines that drive nerve symptoms.
Central pain modulation
Activates descending pain inhibition through the locus coeruleus and periaqueductal gray. Dials up the body's natural pain-suppression circuitry.
Autonomic balance
Improves heart rate variability and shifts the autonomic nervous system toward “rest and digest.” Better sleep, lower anxiety, less pain catastrophizing.
1. Anti-inflammatory effect. Vagal activation triggers the cholinergic anti-inflammatory pathway. The vagus nerve releases acetylcholine, which signals immune cells (specifically macrophages) to reduce production of pro-inflammatory cytokines like TNF-α and interleukin-6. Less systemic inflammation means less small-fiber irritation and less neuroinflammation in the spinal cord.
2. Central pain modulation. Vagal afferents project to brain regions involved in descending pain inhibition, including the locus coeruleus and the periaqueductal gray. Stimulating these pathways can dial up the body's natural pain-suppression circuitry — similar in principle to what mindfulness, antidepressants, and certain pain medications do, but through a different entry point.
3. Autonomic balance. Increased vagal tone improves heart rate variability and shifts the autonomic nervous system toward “rest and digest” rather than “fight or flight.” Better autonomic balance is associated with improved sleep, lower pain catastrophizing, and reduced anxiety — all of which independently improve the experience of chronic pain. (Our article on central sensitization covers some of this overlap.)
What a Course of taVNS Looks Like
Most clinical and research protocols use a similar template:
Realistic Device Costs (2026)
Cheap devices may not deliver effective stimulation; “no benefit” can mean device failure, not VNS failure.
- Schedule: 30 minutes once or twice a day, 5 days a week.
- Duration: At least 4–6 weeks before assessing whether it's helping. Some patients respond earlier; others need a full 8–12 weeks.
- Sensation: Mild to moderate tingling in the ear at the electrode contact point. Adjustable intensity. Should feel noticeable but not painful.
- What you do during a session: Anything quiet. Reading, resting, light meditation. Not driving, not exercising — the device shouldn't interfere with daily life, but you do want to be still enough to track your response.
- What to track: Pain score, tingling, sleep, energy, autonomic symptoms (lightheadedness, digestion). A simple symptom diary is invaluable for telling whether it's actually helping or whether you're hoping it is.
If 6–8 weeks of consistent use produces no measurable change, you have your answer — taVNS isn't your treatment. If it produces meaningful change, the question becomes how to keep it going.
The Devices on the Market
This is where I have to be especially careful about what I say, because the device market is a mess. Three categories exist:
Red Flags for Predatory Devices
- Promises to “cure” neuropathy
- No published pulse parameters (frequency, pulse width, intensity)
- Testimonials but no FDA registration of any kind
- Subscription “treatment plans” or proprietary apps
- Sells through social ads with countdown timers
Research-Grade and Medical Devices
Devices like NEMOS (used widely in European studies) and gammaCore (FDA-cleared for primary headache disorders) deliver carefully calibrated, validated pulses. Costs range from $400 to $3,500 retail, depending on the device and the indication. Some require a prescription; some don't. These are the devices used in published research.
Consumer “Wellness” taVNS Devices
A growing market of $30–$200 ear-clip devices marketed for “stress relief,” “vagal tone,” “anxiety reduction,” and increasingly for pain. The quality and stimulation parameters vary enormously. Some are reasonable approximations of research-grade stimulation; others deliver inconsistent or incorrect dosing.
The honest truth: a cheap consumer device may deliver enough stimulation to produce some benefit, or it may not. Without clinical-grade calibration, you don't really know what you're getting. If you try one and it works, that's wonderful. If it doesn't work, you can't conclude that taVNS itself doesn't work for you — you might just have a device that wasn't delivering effective stimulation.
Avoid
I would steer clear of any device that:
- Promises to “cure” neuropathy
- Has no published parameters (frequency, pulse width, intensity)
- Comes with testimonials but no FDA registration of any kind
- Asks you to subscribe to ongoing payments for software or “treatment plans”
- Sells through social media ads with countdown timers and “limited supply” claims
The legitimate taVNS market is growing, but so is the predatory one.
Side Effects and Safety
For non-invasive taVNS, side effects are generally mild and uncommon:
- Skin irritation at the electrode contact site (most common — usually solves with electrode gel or repositioning)
- Headache (typically mild, often resolves with reduced intensity)
- Lightheadedness or temporary slowing of the heart rate (the vagus nerve does affect cardiac rhythm)
- Cough or hoarseness (rare; suggests electrode is contacting the wrong area of the ear)
- Tinnitus or jaw pain (rare)
People who should be cautious or talk to their doctor before trying taVNS:
- Anyone with a pacemaker, implantable cardioverter-defibrillator, or other implanted electrical device
- People with significant bradycardia (slow heart rate) or known autonomic instability
- People with active ear infections or skin conditions affecting the ear
- People in the first trimester of pregnancy (limited safety data, generally avoided as a precaution)
- Anyone with a history of seizures triggered by sensory stimulation (rare)
Most of these aren't absolute prohibitions — they're reasons to have a real conversation with your physician before starting. Ask your prescriber. If you don't have a prescriber for this, ask your primary care doctor or neurologist.
How taVNS Compares to Other Neuromodulation Options

You're probably already familiar with TENS units for neuropathy pain. TaVNS shares some DNA with TENS — both apply external electrical stimulation through skin electrodes — but the targets and mechanisms are different.
- TENS: Stimulates peripheral sensory nerves at or near the painful site. Acts mostly on local pain gating in the spinal cord. Cheap, well-established, immediate symptomatic relief while it's running.
- taVNS: Stimulates the auricular vagus to influence systemic inflammation, central pain modulation, and autonomic tone. Effects build over weeks. May produce changes that persist after stimulation stops.
- Spinal cord stimulation: Implanted device that stimulates the spinal cord directly. Reserved for severe refractory cases. Significant cost and procedural risk. Stronger evidence base.
- Scrambler therapy: A specialized device that delivers patterned non-pain signals to “scramble” pain signaling. Different mechanism, similar non-invasive premise.
None of these is a replacement for medical treatment of the underlying cause. They're symptom modulators that may or may not work for any given person.
Questions to Ask Before Spending Money

If you're considering trying a taVNS device, here's the script I'd run through:
A Sensible 6–8 Week taVNS Trial
Cause workup first
Make sure underlying cause has been identified. Don't chase neuromodulation while treatable causes go unaddressed.
Choose a quality device
FDA-cleared (any indication) or research-grade with disclosed parameters. Verify return policy covers a 6-week trial.
Use consistently — 30 min daily
Same time of day, same intensity, same ear position. Inconsistency is the most common reason a trial fails.
Track in a symptom diary
Pain, tingling, sleep, energy, autonomic symptoms — daily 0-10 ratings. Numbers cut through hope and bias.
Decide at 6–8 weeks
Real change in any tracked metric? Continue. Nothing measurable? Move on without regret — you've ruled it out cleanly.
- Has your underlying cause of neuropathy been identified and addressed? (If you have undiagnosed B12 deficiency, treating that will do more than any neuromodulation.)
- Have you tried first-line medical treatments for your specific neuropathy type? (Don't skip standard options to chase a less-proven one.)
- Is the device you're considering FDA-cleared for any indication, or registered in another regulated jurisdiction? “Wellness device” claims are not regulated.
- What does the device manufacturer disclose about pulse parameters? (Frequency, pulse width, intensity range — these should be available.)
- What's the return policy? Most legitimate devices have a 30–60 day return window — important since the trial period of 4–6 weeks may overlap.
- Have you discussed this with your neurologist or pain management physician? (Most are familiar with taVNS now and can offer a real opinion.)
- If you're paying out of pocket, what's the total cost — device plus replacement electrodes plus any software subscription?
If those questions all check out and your doctor doesn't have specific concerns, a 6–8 week trial is reasonable. Track your symptoms carefully so you can make a real decision at the end of it.
What I Tell People in Our Group
I'll be honest about my current take. I think taVNS is one of the most promising emerging tools in the neuropathy toolkit. The biology is sound, the early data is consistent, and the safety profile is good. I think there's a real chance that within 5 years it will be a mainstream adjunct for diabetic and chemotherapy-induced neuropathy, possibly more.
I also think the marketing has run miles ahead of the evidence. The cheap consumer devices are a coin flip in quality. The studies that exist are mostly small. Effect sizes are real but modest — taVNS is unlikely to be a transformative single intervention. It's more likely to be a useful tool that, combined with appropriate medical treatment, sleep care, exercise, and stress management, helps a meaningful subset of patients feel meaningfully better.
That's not nothing. Neuropathy is a stubborn condition where every modest gain is precious. But it's worth setting the expectation honestly so you don't feel disappointed if a 30-minute ear-clip session doesn't change your life in a week.
Talk to your neurologist. If they're open to it, a careful 6–8 week trial with a quality device and a real symptom diary will tell you what you need to know. If it works for you, fantastic. If it doesn't, you've ruled out one option and you can move on to the next without that nagging “what if I'd tried it” question.
Frequently Asked Questions
Does vagus nerve stimulation actually work for neuropathy?
Early research suggests it can help, particularly for diabetic peripheral neuropathy and chemotherapy-induced peripheral neuropathy. Effect sizes in published studies have been modest but real — typically 1.5 to 2 points of pain reduction on standard scales. Larger phase III trials are still needed before VNS can be considered standard treatment. For other types of neuropathy (idiopathic, alcoholic, hereditary), there is limited published data.
Is vagus nerve stimulation FDA-approved for neuropathy?
No, not as of 2026. Implanted vagus nerve stimulators are FDA-approved for drug-resistant epilepsy and treatment-resistant depression. Some non-invasive vagus nerve devices are FDA-cleared for migraine and cluster headache. For neuropathy specifically, taVNS is still considered investigational, even though many neurology and pain practices are using it off-label.
What's the difference between TENS and vagus nerve stimulation?
TENS units stimulate sensory nerves at or near the site of pain to interrupt pain signaling locally. Vagus nerve stimulation targets a specific cranial nerve to influence systemic inflammation and central pain processing. TENS provides immediate symptomatic relief while running and has minimal lasting effect after the device is turned off. Vagus nerve stimulation builds effects over weeks and may produce changes that persist between sessions. They can sometimes be used together.
How long does it take to feel a difference from taVNS?
Most clinical protocols recommend at least 4 to 6 weeks of consistent daily use before assessing whether it's helping. Some patients notice changes in 2 to 3 weeks. Others need the full 8 to 12 weeks. If you've used a quality device daily for 8 weeks with no measurable change in symptoms or sleep or autonomic function, it's reasonable to conclude it's not your treatment.
How much does a taVNS device cost?
Research-grade devices like NEMOS and gammaCore range from about $400 to $3,500 in the United States, depending on the model and what indication it's approved for. Consumer wellness devices that claim vagus nerve stimulation range from $30 to $200, but quality and stimulation parameters vary enormously. The higher cost of clinical-grade devices generally reflects rigorous calibration and validation that consumer devices may lack.
Is it safe to use a taVNS device with a pacemaker?
Generally not without explicit cardiology clearance. The vagus nerve directly affects heart rate, and external electrical stimulation in the head and neck region can interfere with implanted cardiac devices. Anyone with a pacemaker, implantable defibrillator, or other implanted electrical device should consult their cardiologist before starting any form of vagus nerve stimulation, including non-invasive auricular versions.
Can I make my own vagus nerve stimulator at home?
Please don't. Several DIY guides exist online using TENS units modified to apply current to the ear. The risks include burns, inappropriate cardiac rhythm changes, and ineffective dosing. The price difference between a DIY rig and a basic commercial taVNS device is small enough that the safety margin isn't worth the savings. If cost is the barrier, ask your neurologist whether any insurance coverage or research participation might be options.
Will my insurance cover vagus nerve stimulation for neuropathy?
In most cases, no — because there's no FDA-approved indication for neuropathy yet. Some insurers cover taVNS for FDA-approved indications like cluster headache or migraine. For neuropathy specifically, expect to pay out of pocket. Check with your insurer before purchasing, and ask whether your neurologist is participating in any research studies that might provide a device for free as part of the trial.


