
If you've been living with the burning, shooting pain of diabetic peripheral neuropathy — and you've already tried the standard medications without much relief — you may have heard whispers about a newer option called Axon Therapy. It's a non-invasive, in-clinic treatment that uses magnetic pulses to calm overactive nerve pain signals. In late 2023 and into 2024, it received a first-of-its-kind FDA clearance specifically for painful diabetic neuropathy (PDN).
I want to walk through what Axon Therapy actually is, what the clinical evidence shows, who it's for, what to realistically expect, how it compares to other options like TENS units or spinal cord stimulators, and the practical questions almost no clinic page is willing to answer plainly — cost, access, sessions required, and whether it could be right for you.
This is not a marketing pitch. I'll tell you what the studies show and where the gaps still are. By the end you should have enough to decide whether it's worth bringing up at your next neurology or pain-management appointment.
What Axon Therapy Is in Plain Language
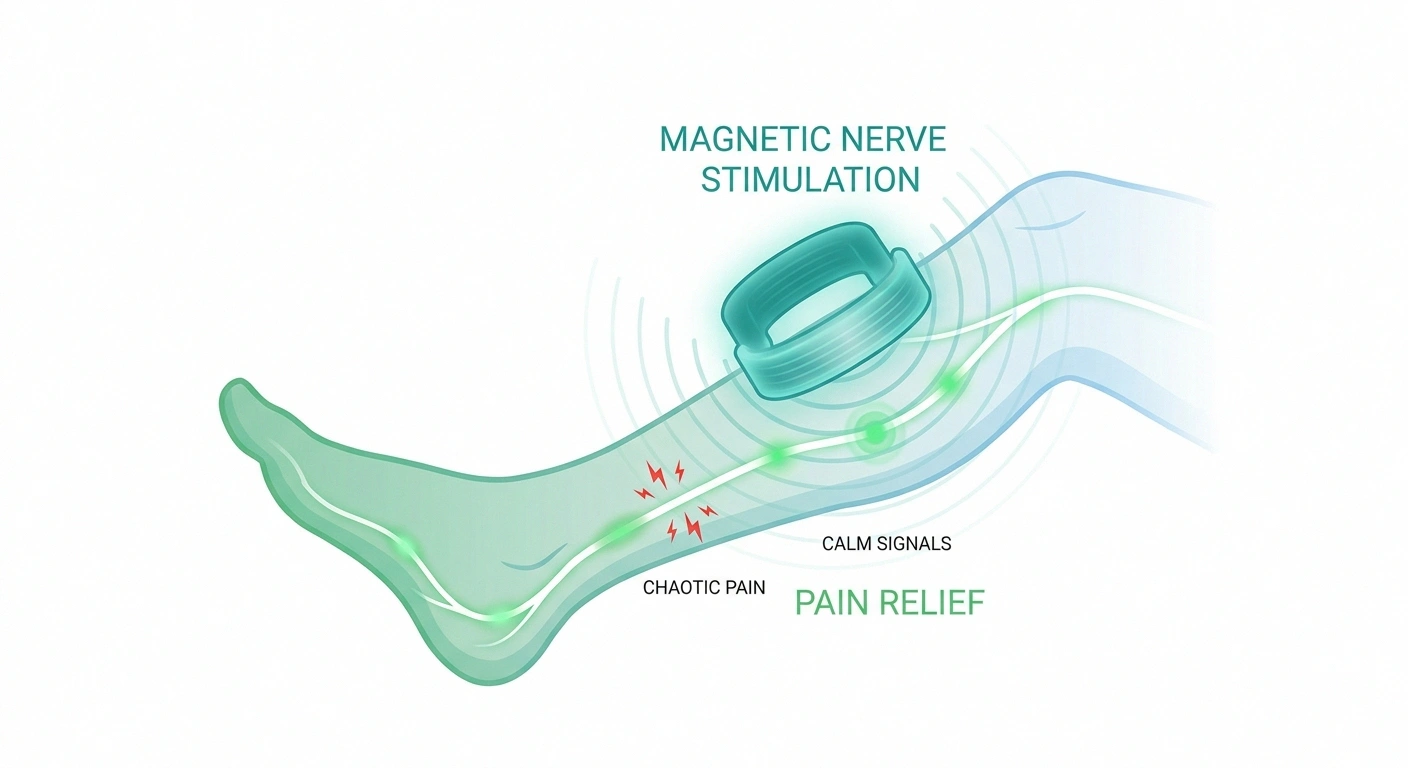
Axon Therapy is an in-clinic, non-invasive treatment made by a company called Neuralace Medical. It uses what's called magnetic peripheral nerve stimulation — abbreviated mPNS. A device that looks a bit like an oversized hair dryer or a handheld paddle is positioned near your foot, ankle, or lower leg, and it delivers focused magnetic pulses to the nerves underneath the skin.
Each session lasts about 13.5 minutes. There are no needles, no implants, no surgery, and most patients describe the sensation as “tapping” or “thumping” rather than painful. You sit in a chair. The technician positions the device. You wait through the session. You go home.
Three things that make this clearance unusual:
- It's the first FDA-cleared non-invasive magnetic peripheral nerve stimulation treatment specifically for painful diabetic neuropathy. Earlier nerve-stimulation devices required implants (spinal cord stimulators) or surface electrodes (TENS). This one delivers stimulation through the skin without contact electrodes or implanted hardware.
- The clearance is supported by a randomized, sham-controlled trial. That matters because many devices reach the market with weaker evidence. This one was tested against a “fake” treatment to rule out the placebo effect.
- It targets a population that's been left behind by current medications. The trial enrolled patients who had already tried — and not gotten enough relief from — the usual neuropathy medications.
The Mechanism — How Magnetic Pulses Calm Pain Signals
To make sense of how Axon Therapy might work, it helps to understand the problem it's targeting.
In painful diabetic neuropathy, peripheral nerves in the feet and lower legs become damaged from chronic high blood sugar. Damaged sensory nerves don't just lose function — they often become hyperexcitable. They fire pain signals on their own, or fire wildly in response to mild touch, temperature, or pressure. That's why ordinary socks can feel like sandpaper, or your sheets at night can feel painful against your toes.
Magnetic pulses delivered to a nerve area do something interesting: they depolarize nerve cells (briefly change their electrical charge) in a way that resets abnormal firing patterns. Over a series of sessions, the theory is that this normalizes the chaotic pain signaling and reduces the overall pain experience. It's the same general family of approach as transcranial magnetic stimulation (TMS) used for depression — using magnetic fields to modulate nerve activity — but Axon Therapy targets peripheral nerves rather than brain regions.
To be clear: this is not “regenerating” damaged nerves or curing the underlying neuropathy. It's reducing the pain that the damaged nerves are generating. That's a meaningful distinction. The diabetes-related nerve damage doesn't go away. What changes is the pain signal volume.
What the Clinical Trial Actually Showed

The pivotal study supporting FDA clearance (sometimes referenced as the AT-PDN study, registered on ClinicalTrials.gov as NCT05620225) is the one to know about. Here are the specifics, told straight:
- Design: Double-blind, multicenter, randomized, sham-controlled trial — the gold standard for evaluating pain treatments.
- Participants: 71 patients with painful diabetic peripheral neuropathy whose pain had not been adequately controlled by their current medications.
- Groups: 50 patients received real Axon Therapy. 21 received a sham (placebo) procedure that mimicked the experience but didn't deliver the active magnetic pulses.
- Endpoint: “Responder” rate — patients reporting at least a 30% reduction in their pain at follow-up. That's the standard threshold used in chronic pain research for a clinically meaningful improvement.
The results:
- Day 30: More than 70% of patients receiving Axon Therapy were responders.
- Day 90: The responder rate rose to over 80%.
- Crossover group: Patients originally given the sham who later crossed over to real Axon Therapy reached close to 89% responder rate at 90 days.
- Safety: No serious adverse events were reported in the trial. Side effects, when they occurred, were mild and transient (skin sensation at the treatment site, mild fatigue).
What does a “responder rate of 80%” really mean? It means roughly 8 out of 10 patients reported their pain had dropped by at least 30%. That's a meaningful number. Pregabalin (Lyrica) trials in painful diabetic neuropathy typically show responder rates around 35–50%. Duloxetine (Cymbalta) similar. So Axon Therapy in this trial substantially outperformed the response rates we typically see with first-line medications — in a population that had already failed those medications.
That said, a few honest caveats are important:
- 71 patients is a small trial. Larger, longer studies are still ongoing. The results need replication.
- Durability isn't fully established. Most data extends to 90 days. Real-world questions about how long the benefit lasts, and whether maintenance sessions are required, are still being answered.
- The crossover responder rate (89%) carries some expectation effect. Patients who had already been through sham and were now getting real treatment knew the difference. Some of that high rate likely reflects positive expectation.
Even with caveats, this is one of the more encouraging pieces of nerve-pain trial data we've seen for a non-medication option in many years.
Who Axon Therapy Is — and Isn't — For
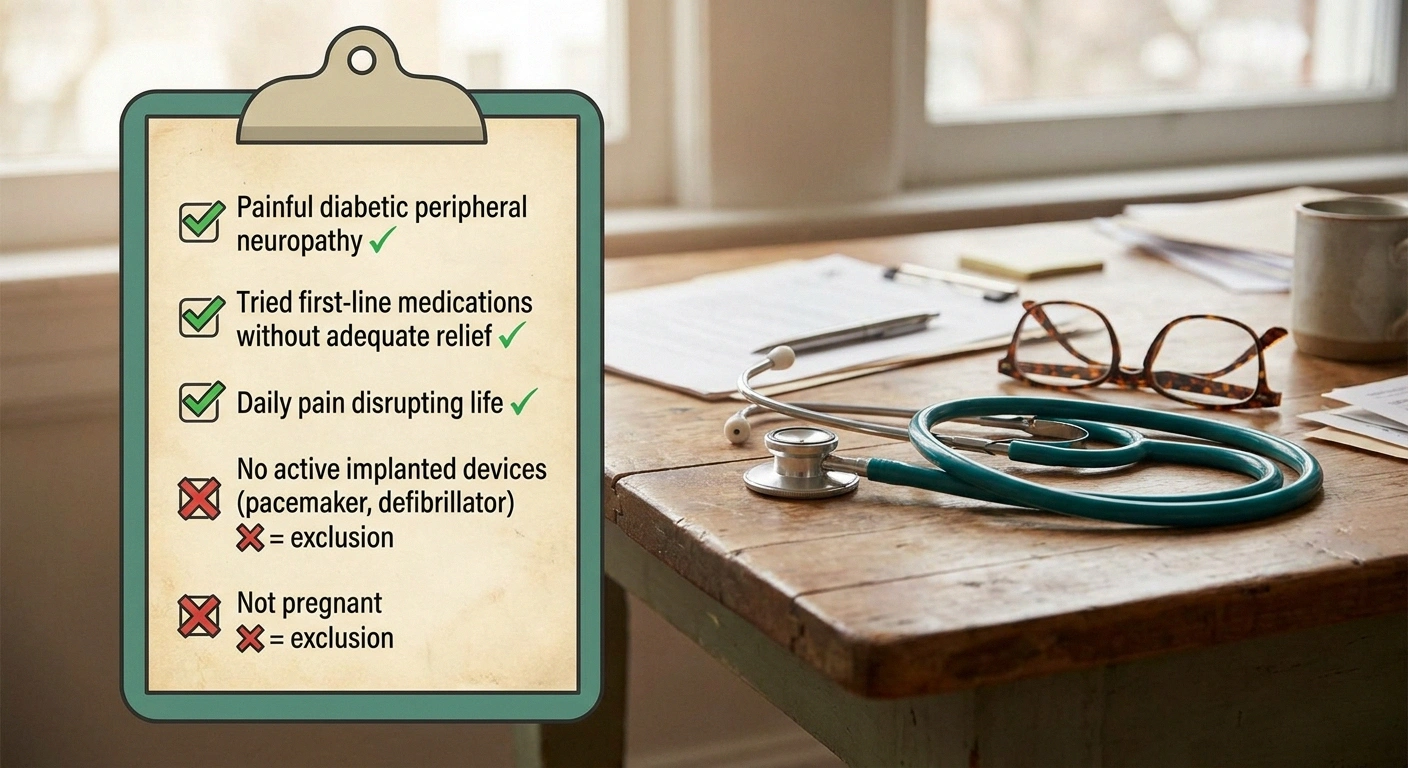
The label is specific: chronic painful diabetic peripheral neuropathy in adults whose pain has been refractory (unresponsive) to conventional medical management. In plain English, that means:
- You have painful diabetic peripheral neuropathy. Not all neuropathy is painful — some causes mostly numbness. The clearance is for the painful variant.
- You've already tried first-line medications (typically pregabalin, gabapentin, duloxetine, amitriptyline, or similar) without sufficient relief, or with side effects you can't tolerate.
- You're not getting enough pain control to live your life. This is for ongoing, daily, life-disrupting pain — not occasional flares.
It is not indicated for:
- Other forms of neuropathy (chemotherapy-induced, idiopathic, hereditary). Studies in those populations are not what the FDA reviewed.
- Mostly-numbness presentations without significant pain.
- Patients with active implants in the treatment area (pacemakers, defibrillators, deep brain stimulators, cochlear implants — magnetic fields can interfere). This is an absolute exclusion.
- Patients with metal implants in the lower legs (orthopedic hardware near the treatment site can be a contraindication — discuss with the prescribing clinic).
- Pregnant patients (lack of safety data, not necessarily a known harm).
How a Course of Treatment Actually Works
The protocol used in trials and now in clinical practice typically looks something like this:
- Initial intensive phase: A series of sessions over several weeks. Common protocols use 6–10 sessions over 2–4 weeks during the intensive phase.
- Each session: About 13.5 minutes of stimulation, with a few minutes of setup and positioning. You're typically in and out within 30 minutes.
- Pain relief onset: Most patients begin reporting reduction in pain after several sessions, not immediately after the first.
- Maintenance: Some patients require periodic maintenance sessions (every few weeks or months) to sustain benefit. Protocols vary by clinic.
The sessions are tolerable for most people. You'll feel pulsing, tapping, or thumping under the device. It's not painful. You can read or chat with the technician.
How Axon Therapy Compares to Other Nerve-Stimulation Options
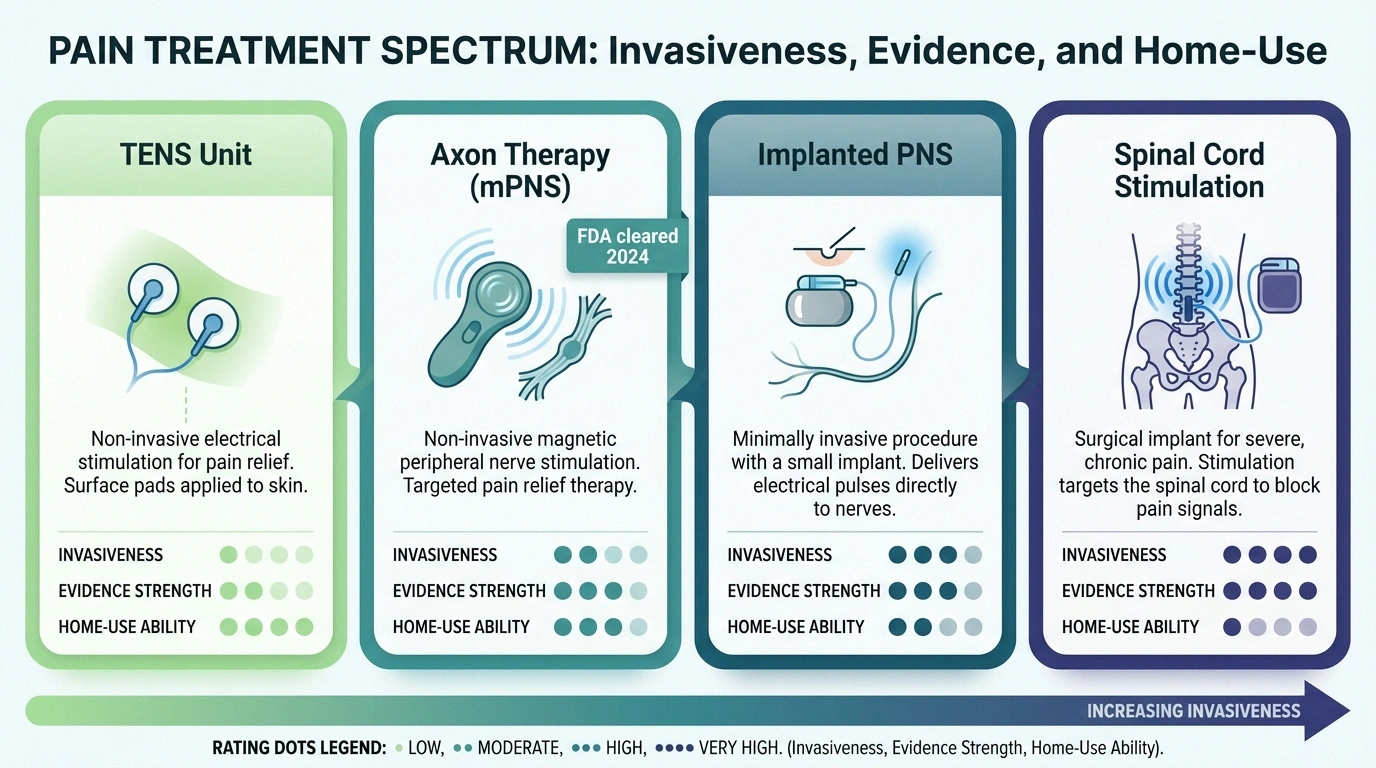
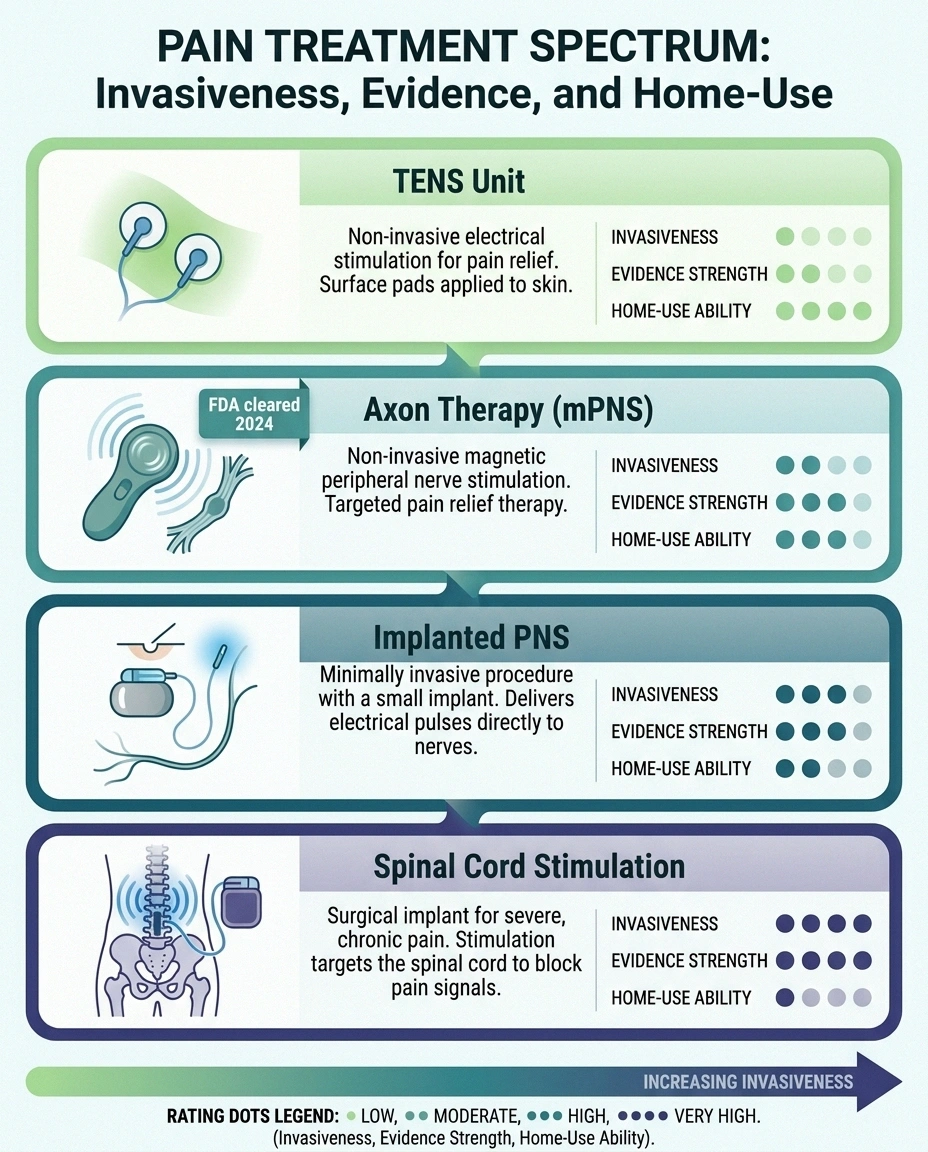
This is where many patients get confused, because “nerve stimulation” is a broad umbrella covering several different things. Here's how to think about the landscape.
TENS units are home-use surface electrical devices. You stick electrode pads to your skin, plug them into a battery-powered controller, and feel a tingling sensation. They deliver electrical current to the skin and shallow nerves. They're inexpensive, available without a prescription, and the evidence for painful diabetic neuropathy is modest. Some patients get meaningful help; many do not. If you've explored options for nerve pain, you may have already tried a TENS unit for neuropathy.
Spinal cord stimulation (SCS) is on the other end of the invasive spectrum. It involves a surgically implanted device with electrodes placed near the spinal cord. SCS has stronger evidence for painful diabetic neuropathy than TENS and can deliver substantial pain relief, but it requires surgery, comes with implant risks (infection, lead migration, hardware failure), and is far more expensive. Learn about spinal cord stimulation for neuropathy for a deeper comparison.
Peripheral nerve stimulation (implanted) sits in the middle — a small implanted device placed near a peripheral nerve. Less invasive than SCS, more invasive than Axon Therapy. More on peripheral nerve stimulation here.
Axon Therapy (magnetic PNS) sits at the non-invasive end of the spectrum — no surgery, no implants, no contact electrodes — but it's also in-clinic only (not a home device) and currently requires a series of visits.
None of these are mutually exclusive. Some patients try TENS at home, fail it, try Axon Therapy in clinic, and never have to consider implants. Other patients eventually need an implanted system. The clinical question is what matches your situation.
Will Insurance Cover It? The Honest Picture

This is where I have to be honest with you: coverage is still developing.
- “Will you verify my insurance benefits and confirm coverage in writing before scheduling?”
- “If insurance doesn't cover it, what is the all-in cash price for a full treatment course?”
- “What's your protocol — how many sessions, over what timeframe, and what happens if I don't respond?”
FDA clearance is not the same as insurance reimbursement. Many private payers and Medicare contractors take 12–36 months after FDA clearance to issue formal coverage policies for newer devices. As of mid-2026, coverage for Axon Therapy is still evolving — some commercial plans cover it in some regions; others classify it as investigational; Medicare coverage varies by jurisdiction. Most clinics offering Axon Therapy will help you with prior-authorization paperwork, but expect some uncertainty.
If insurance won't cover it, out-of-pocket cost for a treatment course can run several thousand dollars depending on the clinic, region, and protocol. That's real money, and it's worth verifying coverage and costs before scheduling.
Practical tip: When you call a clinic, ask three specific questions before agreeing to treatment:
- “Will you verify my insurance benefits and confirm coverage in writing before scheduling?”
- “If insurance doesn't cover it, what is the all-in cash price for a full treatment course?”
- “What's your protocol — how many sessions, over what timeframe, and what happens if I don't respond?”
A good clinic will answer all three without hedging. If you get vague answers, look elsewhere.
How to Find an Axon Therapy Provider
Axon Therapy is delivered in pain-management clinics, podiatry practices, and integrative medicine centers — primarily in areas where Neuralace Medical has built distribution. As of 2026, the largest concentration of providers is in California, Florida, Arizona, Texas, and parts of the Mountain West, with growing presence in the Northeast and Midwest.
The most direct route to finding a provider is through Neuralace's clinic-locator function on their corporate site, or asking your existing neurologist or pain-management physician whether they offer it or know a colleague who does. Increasingly, clinics that previously offered spinal cord stimulation programs are adding Axon Therapy as an earlier-step option in their treatment ladder.
Realistic Expectations — What “Success” Looks Like
I'd be doing you a disservice if I let you walk away thinking Axon Therapy is going to take your nerve pain to zero. Here's the honest expectation-setting:
- Success in the trial meant 30% or more pain reduction — not pain elimination. For someone whose pain is 8/10, that's getting down to around 5–6/10. That's meaningful — it can be the difference between functioning and not functioning — but it's not “cured.”
- Most responders sustained benefit at 90 days. Longer-term durability data is still being collected.
- Some patients respond strongly, some respond modestly, some don't respond. About 1 in 5 didn't reach the 30% threshold in trial. Your individual response can't be predicted in advance.
- Pain reduction may allow medication reduction. Some patients are able to lower their doses of gabapentin, pregabalin, or duloxetine after a successful course — improving side-effect burden and quality of life.
Whether that math is worth it depends on where you're starting from. For someone who's tried everything and is being limited every day by pain, a 50% chance of meaningful reduction is a real option worth considering. For someone whose pain is moderate and well-controlled on medication, the calculation is different.
Questions to Bring to Your Doctor

If you want to explore this option, here's what to ask your neurologist, pain physician, or podiatrist:
- “Based on my history, am I a candidate for Axon Therapy?”
- “Have I tried adequate trials of the standard medications, or are there options I haven't fully explored yet?”
- “Do you refer patients for Axon Therapy, and if so, to which clinic?”
- “How do you typically sequence treatment options for someone in my situation?”
For more on how to prepare for a productive conversation with your provider, take a look at our guide on how to talk to your doctor about neuropathy pain.
Where Axon Therapy Fits in the Bigger Picture
Axon Therapy is part of a broader shift happening right now in diabetic neuropathy treatment — moving away from a medication-only model toward a layered approach that combines targeted therapies, devices, and the foundational work of glycemic control and lifestyle. Several new options are entering trial phases, and the field is changing faster now than it has in decades. Our roundup of new neuropathy treatments in 2026 covers what else is coming.
Whether Axon Therapy specifically is right for you is a clinical decision made with your physician. What I want you to leave with is this: there is now a non-invasive, FDA-cleared option supported by a real randomized trial that targets exactly the population standard medications have failed. That didn't exist a few years ago. For someone living with refractory diabetic neuropathy pain, knowing that option is on the menu — and having the language to ask about it — is part of what advocacy for your own care looks like.
Frequently Asked Questions
How long does Axon Therapy pain relief last?
In the pivotal trial, most patients who responded to Axon Therapy maintained their improvement at the 90-day follow-up. Longer-term durability is still being studied. Some clinics offer maintenance sessions every several weeks or months to sustain benefit, though protocols vary. If pain returns, additional treatment cycles can usually be considered.
Does Axon Therapy hurt?
Most patients describe the sensation as a tapping or thumping pulse rather than pain. The device delivers magnetic pulses without needles, surgery, or contact electrodes pressed firmly into the skin. Many patients can read or chat with the technician during the 13.5-minute session.
How is Axon Therapy different from a TENS unit?
TENS uses surface electrodes that deliver electrical current to the skin and shallow nerves. Axon Therapy uses focused magnetic pulses, which penetrate more deeply without needing direct skin contact through electrodes. Axon Therapy is also in-clinic and requires a prescribed protocol, while TENS units are home-use and available without prescription. The trial evidence for Axon Therapy in painful diabetic neuropathy is stronger than the average TENS study.
Will Medicare cover Axon Therapy?
As of mid-2026, Medicare coverage for Axon Therapy is still developing and varies by Medicare Administrative Contractor jurisdiction. Some regions cover it under specific conditions; others classify it as investigational. Coverage from commercial insurers also varies. Always verify benefits in writing before scheduling treatment.
How many Axon Therapy sessions will I need?
Typical protocols call for an intensive series of 6–10 sessions over several weeks, with each session lasting about 13.5 minutes. Some patients may need maintenance sessions afterward. Your treating clinic will tailor the protocol to your specific situation. Ask up front how many sessions are planned and how response will be assessed.
Can I have Axon Therapy if I have a pacemaker?
No. Active implanted devices like pacemakers, defibrillators, and deep brain stimulators are absolute contraindications because the magnetic field can interfere with the device. Always disclose all implanted devices to the treating clinic before any nerve-stimulation treatment.
Is Axon Therapy a cure for diabetic neuropathy?
No. Axon Therapy reduces pain signals from damaged nerves but does not regenerate or repair the underlying nerve damage caused by diabetes. The diabetic nerve damage itself remains. What changes is the pain experience. Combining Axon Therapy with strong glycemic control, weight management, and other foundational diabetes care is the most evidence-supported approach to slowing future nerve damage.
Can Axon Therapy be used for chemotherapy-induced neuropathy?
The FDA clearance is specifically for painful diabetic peripheral neuropathy. Some clinics offer the technology off-label for other neuropathies, but the trial evidence supporting it is for the diabetic population. If you have chemotherapy-induced neuropathy, discuss with your oncologist or pain physician whether the existing evidence is strong enough to justify the cost in your specific case.


