
My friend Margaret called me one afternoon, three days after her doctor finally figured it out. She'd been telling people for almost four years that something was wrong with her feet. The numbness had started slowly — a little tingling at first, the kind you brush off as a bad night's sleep or shoes that don't fit right. Then it crept up her ankles. Then she started losing her balance in the shower. Then she fell going down the back porch steps.
Every doctor she saw shrugged. “You're 64, Margaret. This is what 64 looks like.” One told her to take more vitamin D. Another suggested physical therapy. A third asked, with what she described as a slightly impatient tone, whether she'd considered that maybe she just needed to “move more.” Nobody ran the right blood test. Nobody asked the right question.
It was a new nurse practitioner — fresh out of school, ordering everything because she didn't know what to skip — who finally found it. Margaret's serum B12 was dangerously low. Her methylmalonic acid was sky-high. And tucked at the bottom of the panel: positive for intrinsic factor antibodies. She had pernicious anemia. The strangest part? She didn't have anemia. Her red blood cells looked completely normal on the count. The disease was wrecking her nervous system years before it touched her blood.
If you've been told for years that your burning feet, your numbness, your shaky balance, are “just getting older” — and especially if no one has run a B12 panel — Margaret's story is the reason you should keep reading. Pernicious anemia is one of the most treatable causes of neuropathy in the world, and one of the most commonly missed.
What Is Pernicious Anemia?
Pernicious anemia (PA) is an autoimmune condition in which your own immune system attacks the cells in your stomach that make a protein called intrinsic factor — and sometimes attacks intrinsic factor itself. The result is that you can no longer absorb vitamin B12 from food, no matter how much B12 you eat.
Key Takeaway
Pernicious anemia is an autoimmune condition that destroys your ability to absorb vitamin B12 — and the resulting nerve damage can show up years before any blood abnormality appears. Up to 25% of patients have neurological symptoms first, while their CBC still looks normal.
The name is a leftover from the 1800s, when doctors didn't know what caused it and watched patients slowly waste away from the unexplained anemia and neurological decline. “Pernicious” meant deadly — and before B12 was discovered in the 1940s, it was. Patients died from a disease we can now treat with a $5 vial of medicine.
Two things can go wrong in the autoimmune attack:
- Antibodies against parietal cells — these are the cells in the stomach lining that produce intrinsic factor. When they're damaged or destroyed, intrinsic factor production drops or stops.
- Antibodies against intrinsic factor itself — these come in two types. Type 1 “blocking” antibodies physically prevent B12 from binding to intrinsic factor. Type 2 “binding” antibodies prevent the intrinsic factor and B12 complex from being absorbed once it forms.
Most people with pernicious anemia have one or both types of antibodies. The condition often shows up alongside other autoimmune diseases — Hashimoto's thyroiditis, Type 1 diabetes, vitiligo, and Addison's disease are the most common companions. If you have one autoimmune condition, you're at higher risk for others.
Pernicious anemia is more common in people of Northern European descent, in women than in men, and most often shows up after age 60 — though it can develop at any age, and family history raises your risk significantly.
The B12 Absorption Problem
Here's where it gets a little wonky, but the mechanics matter because they explain why oral B12 from your diet doesn't fix this.
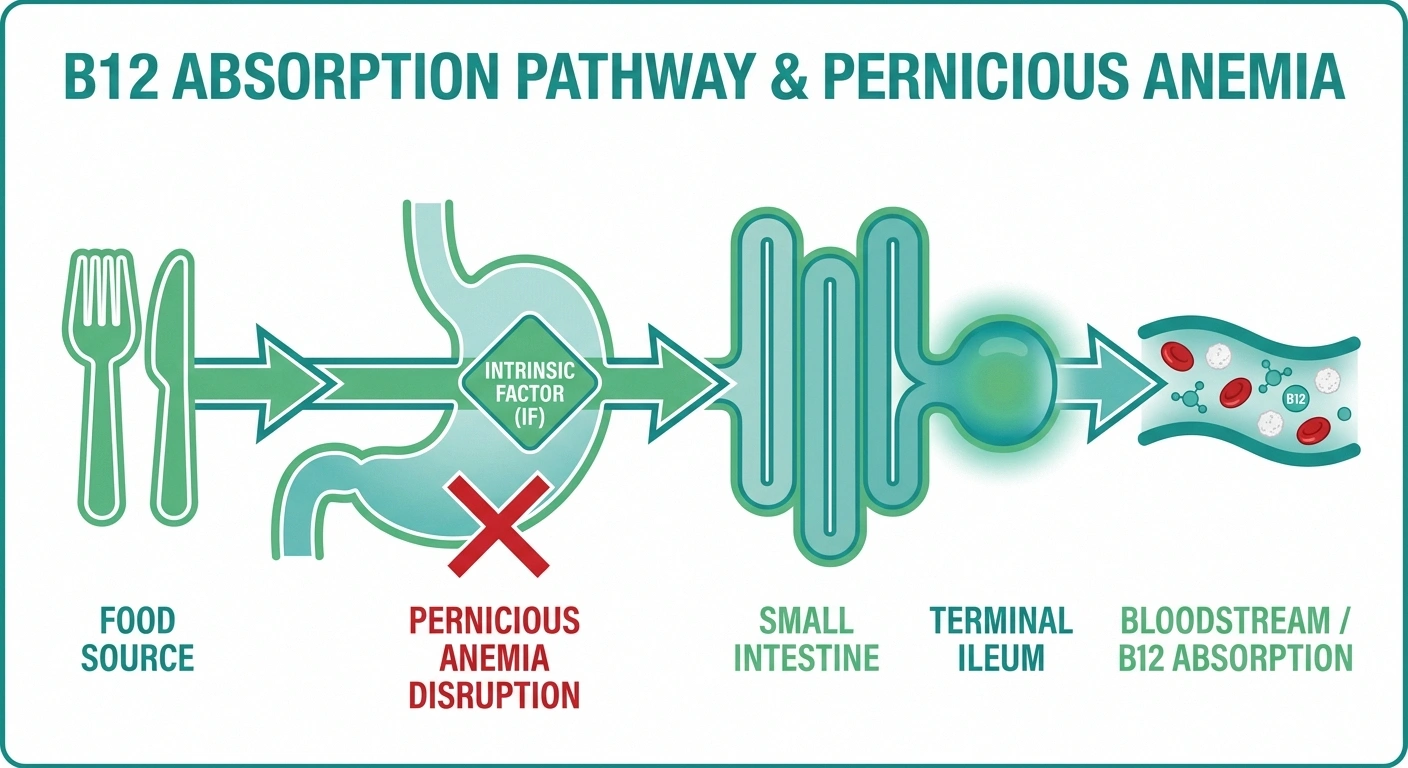
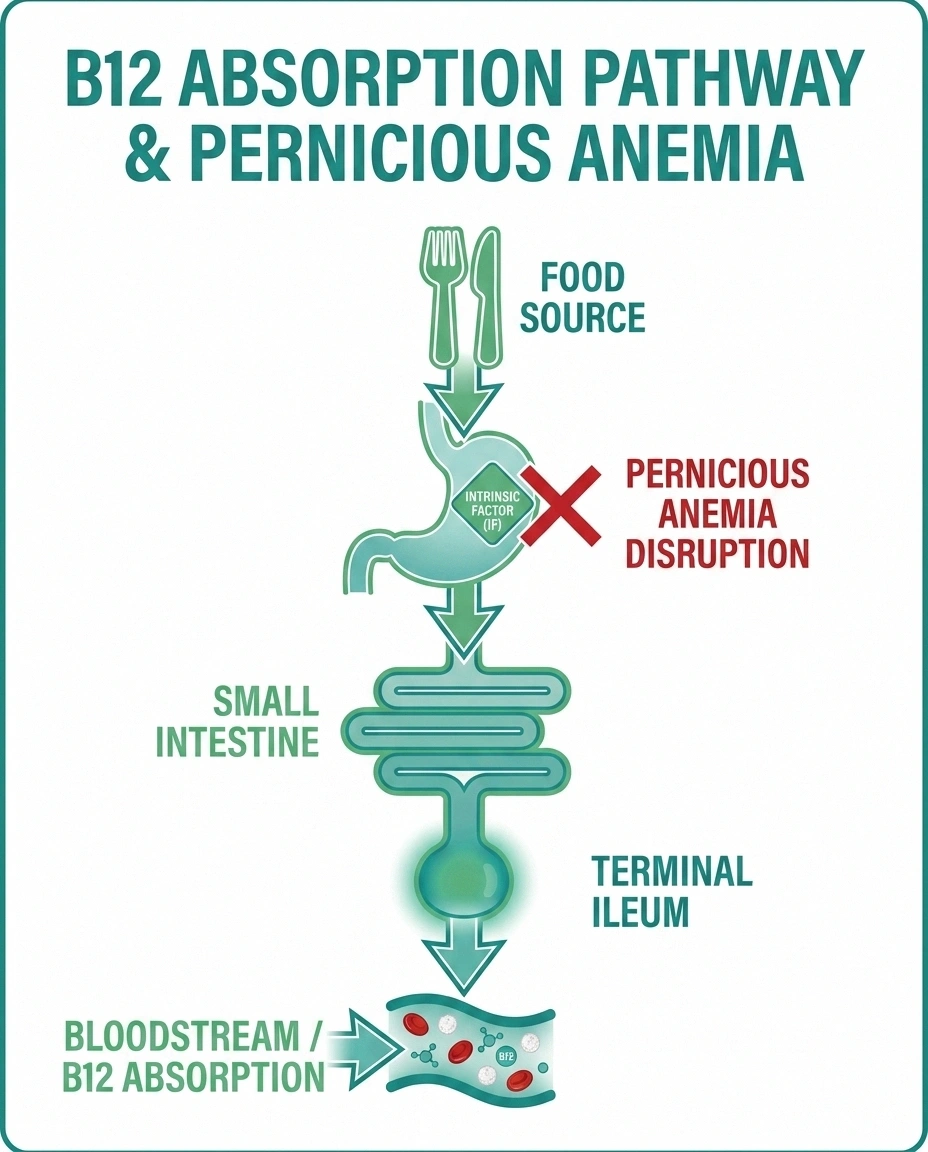
The B12 Absorption Pathway (And Where Pernicious Anemia Breaks It)
1. Food → Stomach
B12 from meat, eggs, fish, dairy, and fortified cereals reaches the stomach, where acid and pepsin release it from food proteins.
2. Stomach → Intrinsic Factor Binding
Parietal cells in the stomach lining produce intrinsic factor, which binds to free B12 and escorts it through the small intestine.
✕ Pernicious Anemia Breaks This Step
Autoimmune antibodies attack parietal cells and/or intrinsic factor. Without intrinsic factor, B12 cannot be escorted forward.
3. Terminal Ileum → Bloodstream
In the last segment of the small intestine, specialized receptors recognize the B12-IF complex and absorb it into the blood.
4. Blood → Tissues (Including Nerves)
B12 travels to the bone marrow, brain, and peripheral nerves — where it's essential for myelin synthesis and DNA production.
Vitamin B12 absorption is a multi-step relay race. When you eat B12-rich food (meat, eggs, fish, dairy, fortified cereals), the B12 first gets bound to a salivary protein called haptocorrin in your mouth. In the stomach, acid and pepsin release the B12 from food and from haptocorrin. Then — and this is the critical step — the freed B12 binds to intrinsic factor, that protein made by your stomach's parietal cells.
The B12-intrinsic factor complex travels all the way through the small intestine until it reaches the very last segment — the terminal ileum. There, specialized receptors recognize the complex and pull it across the gut wall into the bloodstream. From there, B12 gets distributed throughout your body, where it does critical work in red blood cell production, DNA synthesis, and — most important for this article — myelin synthesis.
Knock out intrinsic factor and the whole relay collapses. The B12 in your food just passes through your gut and out the other end. Your liver has stored maybe 3-5 years' worth of B12 from before the autoimmune attack started, so for a while, nothing seems wrong. Then the stores run dry, and the symptoms begin to surface — slowly, insidiously, often in your nerves first.
There's one small workaround your body has: about 1% of any B12 you swallow is absorbed by simple passive diffusion in the small intestine, completely independent of intrinsic factor. That's why very high-dose oral B12 (1,000 to 2,000 mcg per day) can sometimes work for milder cases — 1% of 2,000 mcg is still 20 mcg, well above the daily requirement. But for severe deficiency or active neurological symptoms, most experts still favor injections to bypass the gut entirely.
Why B12 Deficiency Damages Nerves

B12 is essential to two enzyme reactions, and one of them — the conversion of methylmalonyl-CoA to succinyl-CoA — is critical for the production of myelin, the fatty insulation that wraps your nerve fibers and lets them conduct signals quickly and cleanly.
Without enough B12, the building blocks for myelin don't get assembled correctly. Existing myelin starts to break down. New myelin can't be made. The nerve fibers underneath lose their insulation, signals start to misfire, and the symptoms you'd expect from a fraying electrical wire — tingling, numbness, weakness, balance issues — begin to show up.
The damage isn't random. It tends to hit specific tracts in the spinal cord first, especially the dorsal columns (which carry vibration sense and proprioception) and the lateral corticospinal tracts (which carry motor signals). The peripheral nerves in the hands and feet are also affected. This pattern has its own diagnostic name: subacute combined degeneration of the spinal cord.
The same B12-dependent reaction also produces homocysteine when it goes wrong — and elevated homocysteine is itself toxic to the nervous system and is associated with increased cardiovascular risk. So a B12 deficiency creates damage by two mechanisms simultaneously: lack of myelin building blocks, and accumulation of a toxic metabolite.
The Neuropathy Connection: Subacute Combined Degeneration

The classic neurological presentation of B12 deficiency is one of the most distinctive in medicine, even if it isn't always recognized in time.
Early symptoms tend to be sensory. You might notice a glove-and-stocking pattern of tingling or numbness in your hands and feet — symmetric, gradually creeping inward. You might lose vibration sense first (the buzz of a tuning fork on your big toe disappears). You might lose proprioception — the sense of where your limbs are in space without looking — which is what makes balance progressively harder, especially in the dark or with eyes closed.
As the damage spreads, you may develop weakness in the legs, a stiff and unsteady gait, and a positive Romberg sign (you sway or fall when you stand with feet together and eyes closed). Reflexes in the legs may become brisk and overactive (hyperreflexia) because the inhibitory descending pathways are damaged, even while peripheral nerves are also dysfunctional. This odd combination — brisk reflexes plus peripheral numbness — is a classic clue.
If the deficiency progresses untreated, the picture can include cognitive changes ranging from forgetfulness and irritability to frank dementia, mood changes, optic nerve atrophy (blurry or dimmed central vision), and bowel or bladder dysfunction.
None of this is mild. And much of it can be reversed if treatment starts early enough. That's why balance problems and falls in an older adult should always trigger consideration of B12 deficiency as one of the testable causes.
The Diagnostic Catch-22
This is the part that catches doctors off guard and costs patients years of unnecessary nerve damage.
If You're Over 50 With Unexplained Neuropathy
Ask your doctor specifically for a serum B12 AND methylmalonic acid (MMA) test — regardless of what your blood count looks like. If those are abnormal, follow up with intrinsic factor and parietal cell antibodies.
Early diagnosis is reversible damage. Late diagnosis is permanent damage. The test costs almost nothing. Don't leave the office without it.
🔎 Research Says
Up to 25% of pernicious anemia patients present with neurological symptoms before developing anemia or macrocytic red blood cells. Adequate folate intake from fortified foods can mask the blood changes for years while nerve damage progresses silently. A normal CBC does not rule out B12 deficiency.
The medical school version of pernicious anemia goes like this: a patient develops a megaloblastic anemia (low red blood cells, but the cells that are there are abnormally large — macrocytic), the blood smear shows hypersegmented neutrophils, and the doctor checks B12 and finds it low. The diagnosis follows naturally from the blood abnormality.
The reality is that up to 25% of people with pernicious anemia present with neurological symptoms before they ever develop anemia or macrocytic red blood cells. The nerves are damaged first. The blood looks normal on a routine count. And because most clinicians associate B12 deficiency with anemia, a normal CBC reassures them — and the right test never gets ordered.
The reason this happens isn't fully understood, but one factor is folate. If a person eats a lot of fortified breads and cereals (which most Americans do), they get plenty of folate. Folate can mask the red blood cell changes of B12 deficiency for years — but it cannot prevent or reverse the neurological damage. The blood count looks fine. The nerves keep deteriorating. By the time anemia appears, the spinal cord may already be permanently damaged.
So if you take nothing else from this article: a normal CBC does not rule out B12 deficiency or pernicious anemia. If you have unexplained neuropathy and you're over 50 — especially if you have a family history of autoimmune disease, Northern European ancestry, or any other autoimmune condition — ask your doctor to order a serum B12 and a methylmalonic acid (MMA) level, regardless of what your blood count looks like.
Getting the Right Tests

The diagnostic workup for suspected B12 deficiency or pernicious anemia is straightforward when the right tests get ordered. Here's what a thorough evaluation usually includes:
The Pernicious Anemia Diagnostic Panel
| Test | What It Shows | Why It Matters |
|---|---|---|
| Serum B12 | Total B12 in blood | Starting point; misses borderline cases |
| Methylmalonic acid (MMA) | Tissue-level B12 function | More sensitive than serum B12 |
| Homocysteine | B12/folate metabolism | Secondary marker; less specific |
| Intrinsic factor antibodies | Autoimmune attack on IF | ~50% sensitive, ~95-100% specific |
| Parietal cell antibodies | Attack on stomach cells | ~80-90% sensitive, less specific |
| CBC + blood smear | Macrocytic anemia, hypersegmented neutrophils | Can be NORMAL in early PA |
| Folate level | Folate status | Always check alongside B12 |
Serum B12 (cobalamin) level. The starting point. A clearly low level (typically under 200 pg/mL) is diagnostic of deficiency. The grey zone is 200-400 pg/mL — these “borderline” results often turn out to be functional deficiency when MMA is checked, and many experts recommend treating symptomatic patients with low-normal results rather than waiting.
Methylmalonic acid (MMA). When B12 is missing, MMA accumulates because the B12-dependent enzyme that processes it stops working. Elevated MMA is more sensitive than serum B12 itself for detecting tissue-level deficiency, especially in the borderline range. Many neurologists consider MMA the most useful confirmation test.
Homocysteine. Also rises in B12 deficiency, though it's less specific (folate deficiency raises it too). Useful as a secondary marker.
Intrinsic factor antibodies. If positive, this is essentially diagnostic of pernicious anemia. The blood test catches about half of PA cases (sensitivity is around 50%), but it's highly specific (about 95-100%) — meaning a positive result almost certainly means PA, while a negative result doesn't rule it out.
Parietal cell antibodies. More sensitive (around 80-90%) but less specific than intrinsic factor antibodies. Often ordered together as a panel.
Complete blood count and blood smear. Looking for macrocytic anemia (mean corpuscular volume above 100 fL) and hypersegmented neutrophils. Remember — these can be normal even with severe B12 deficiency, especially with adequate folate intake.
Folate level. Always check folate alongside B12. They affect each other and can complicate the diagnostic picture.
The full panel is inexpensive and broadly available. The barrier is rarely the test — it's getting it ordered. The neuropathy lab test guide covers the broader workup if you need to make the case to your doctor for comprehensive testing.
Treatment: Why It's Usually Injections, Not Pills

Once pernicious anemia is diagnosed and neurological symptoms are present, the standard treatment is intramuscular vitamin B12 injections. Here's why and what the typical schedule looks like.
Typical B12 Injection Treatment Timeline
Loading Phase → Weeks 1-2
1,000 mcg intramuscular every other day. Rapidly restores body stores.
Consolidation → Weeks 3-10
1,000 mcg weekly for 4-8 weeks. Begins nerve repair.
Maintenance → For Life
1,000 mcg every 1-3 months. Some neurological cases need monthly.
Recovery window: Most nerve recovery happens in the first 6-12 months.
Treatment is lifelong — the autoimmune attack on parietal cells does not reverse.
The injection bypasses the gut entirely. You're not relying on intrinsic factor to absorb B12 — you're putting B12 directly into your muscle, from where it gets absorbed reliably and predictably. For someone whose autoimmune disease has destroyed their absorption capacity, injection guarantees that the B12 gets where it needs to go.
The two forms typically used are cyanocobalamin (the cheaper and more common form in the US) and hydroxocobalamin (more common in the UK and Europe, with a longer half-life that allows less frequent dosing). Both are effective.
A typical treatment schedule looks something like this:
- Loading phase: 1,000 mcg intramuscular every other day for 1-2 weeks (this rapidly restores body stores).
- Consolidation phase: 1,000 mcg weekly for 4-8 weeks.
- Maintenance phase: 1,000 mcg every 1-3 months for the rest of your life.
For neurological symptoms specifically, some specialists use a more aggressive loading protocol (every other day for several weeks) and recommend more frequent maintenance — every 2 months instead of 3, or even monthly — because nerve repair is slow and seems to benefit from sustained higher levels.
Pills do have a role for some patients. High-dose oral cyanocobalamin (1,000 to 2,000 mcg daily) can work for people who have partial absorption preserved, or for maintenance after the loading phase has restored stores. The 1% passive absorption pathway is enough to maintain levels for many. However, for active neurological symptoms or severe deficiency, most specialists still start with injections to ensure rapid, reliable replenishment. Sublingual and nasal forms also exist and can be options for people who can't tolerate injections.
This is a lifelong treatment. The autoimmune attack on parietal cells doesn't reverse — once you have pernicious anemia, you have it for life, and you need ongoing B12 supplementation in some form to prevent recurrence.
The Window of Reversibility
This is the part Margaret's nurse practitioner explained to her — and the part I want every reader to internalize.
Neurological symptoms from B12 deficiency exist on a spectrum from fully reversible to permanently entrenched, and the determining factor is mostly how long they've been present before treatment starts.
Symptoms present for weeks to a few months tend to reverse substantially with treatment. Symptoms present for 6-12 months may improve significantly but may not fully resolve. Symptoms present for more than a year — and especially symptoms that have progressed to gait instability, weakness, or cognitive changes — often improve only partially. Some never reverse.
The general rule clinicians use is that whatever neurological function is going to come back tends to do so within the first 6-12 months of consistent treatment. Beyond that, the remaining deficits are often permanent. This isn't a reason to delay treatment in late cases — even partial recovery is meaningful, and stopping further damage is essential — but it is the reason that early diagnosis matters so much.
Margaret's neurologist told her to expect about 60-70% recovery of her sensory symptoms over the next 6-12 months, with most of the gain in the first 3-4 months. Her balance, which had been her worst symptom, has already improved enough that she's stopped using a cane around the house. The numbness in her toes is still there, two years in, and probably always will be. But she stopped getting worse.
The question of whether neuropathy can be reversed doesn't have one universal answer — but for B12 deficiency neuropathy caught early, the honest answer is closer to “yes” than for almost any other cause.
Living With Pernicious Anemia Long-Term

Once you're diagnosed and on a treatment schedule, pernicious anemia becomes one of the more manageable chronic conditions to live with. A few practical considerations:
The injections become routine. Many people learn to give them at home (it's a small needle into a large muscle — your thigh or upper outer buttock). Others have a family member trained, or get them at the doctor's office or pharmacy clinic. The shot itself takes seconds.
You'll need ongoing monitoring. Even on treatment, periodic B12 levels (often once a year), thyroid panels, and screening for other autoimmune conditions are smart. Pernicious anemia is associated with a slightly increased risk of stomach cancer, so most guidelines recommend periodic surveillance — discuss the right interval with your doctor.
Be alert for new autoimmune diseases. If you develop unexplained fatigue, weight changes, dry skin, hair loss, or other symptoms that suggest thyroid or adrenal involvement, mention pernicious anemia to whichever doctor you see — it changes the diagnostic considerations.
Tell every new provider. Especially anyone prescribing acid-suppressing medications (PPIs like omeprazole, or H2 blockers like famotidine), because chronic acid suppression further reduces B12 absorption from food. If you're on metformin for diabetes, that's another B12-depleting medication — see metformin and B12 deficiency for the broader picture there. The combination of pernicious anemia and a B12-depleting medication is a recipe for relapse if your injection schedule isn't tight.
Track your symptoms. A simple log of how you feel in the days right before and after each injection helps identify whether the interval is right for you. Some people feel best at every-2-month dosing; others need monthly. Your symptoms are the most useful data.
There's also a broader picture worth keeping in mind: pernicious anemia is just one cause of B12 deficiency. The full landscape of vitamin deficiency neuropathy includes folate, B6, B1, copper, and vitamin E deficiencies, several of which can mimic or coexist with B12 deficiency. A thorough B vitamins guide is worth bookmarking if you're working through this territory with your doctor.
Frequently Asked Questions
Can pernicious anemia cause neuropathy without anemia?
Yes — and this is one of the most important things to understand about the condition. Up to 25% of people with pernicious anemia present with neurological symptoms before any blood abnormality appears. Adequate folate intake from fortified foods can mask the red blood cell changes for years while nerve damage continues to progress. A normal complete blood count does not rule out B12 deficiency. If you have unexplained neuropathy, especially if you're over 50, ask your doctor for a serum B12 and methylmalonic acid level regardless of what your CBC looks like.
What are the early warning signs of B12 deficiency neuropathy?
The earliest signs are usually symmetric tingling or numbness in the feet and hands in a glove-and-stocking pattern, loss of vibration sense, and subtle balance problems that get worse in low light or with eyes closed. Some people notice difficulty buttoning shirts, picking up small objects, or feeling textures with their fingertips. As the condition progresses, weakness, gait instability, and cognitive changes can develop. Because these symptoms are slow and creeping, they're often dismissed as “just aging” — but they shouldn't be.
How is pernicious anemia diagnosed?
The diagnostic workup typically includes serum vitamin B12, methylmalonic acid, homocysteine, intrinsic factor antibodies, parietal cell antibodies, a complete blood count with blood smear, and a folate level. Intrinsic factor antibodies are highly specific for pernicious anemia — if positive, the diagnosis is essentially confirmed — but they have only about 50% sensitivity, meaning a negative result doesn't rule the condition out. Parietal cell antibodies are more sensitive but less specific. Methylmalonic acid is often the most useful confirmation of tissue-level B12 deficiency, especially when B12 levels are borderline.
Why are B12 injections preferred over pills for pernicious anemia?
In pernicious anemia, the autoimmune attack on intrinsic factor or the cells that produce it destroys your ability to absorb B12 from food and most pills through the normal pathway. Injections bypass the gut entirely, putting B12 directly into the muscle for reliable absorption. About 1% of any oral B12 is absorbed by passive diffusion independent of intrinsic factor, which is why high-dose oral B12 (1,000 to 2,000 mcg daily) can work for some patients — especially for maintenance after loading. But for active neurological symptoms or severe deficiency, most specialists still start with injections to ensure rapid restoration of B12 stores and tissue levels.
Can B12 deficiency neuropathy be reversed?
It depends on how long the symptoms have been present. Neurological symptoms caught within weeks to a few months of onset often reverse substantially with B12 replacement. Symptoms present for 6-12 months may improve significantly but may not fully resolve. Symptoms present for more than a year — particularly weakness, gait problems, or cognitive changes — often improve only partially, and some deficits may be permanent. Most of the recovery that's going to happen happens within the first 6-12 months of treatment. This is why early diagnosis matters so much, and why no one with unexplained neuropathy should leave the doctor's office without a B12 panel.
Is pernicious anemia hereditary?
Pernicious anemia is not directly inherited like a single-gene disease, but there is a clear genetic component. Having a first-degree relative with pernicious anemia raises your risk significantly, and the condition clusters in families along with other autoimmune diseases like Hashimoto's thyroiditis, Type 1 diabetes, vitiligo, and Addison's disease. It's also more common in people of Northern European descent. If pernicious anemia or another autoimmune condition runs in your family, mention this when discussing unexplained neurological symptoms with your doctor.
How long does B12 take to work for nerve symptoms?
Energy and cognitive symptoms often improve within days to a few weeks of starting B12 replacement. Sensory symptoms like tingling and numbness usually take longer — most improvement happens over the first 3-6 months of treatment, with some additional gains over 6-12 months. Beyond that, recovery typically plateaus. Balance and proprioception often recover more slowly than tingling. Patience matters, but so does paying attention to whether symptoms are continuing to improve over time. If they aren't, talk with your doctor about increasing the dose frequency or checking for other contributing causes.
Can I just take oral B12 supplements instead of getting tested?
This is well-meaning but risky. High-dose oral B12 will probably correct mild deficiency, and it won't hurt you to take it. But if your symptoms are caused by pernicious anemia or another absorption problem, oral supplements may not be enough — and self-treating without a diagnosis can mask the symptoms long enough for permanent nerve damage to set in. It can also delay diagnosis of the underlying autoimmune condition and the associated risks (other autoimmune diseases, stomach cancer surveillance). Get the testing done first, get the diagnosis if there is one, and then choose a treatment with your doctor that matches the actual problem.


