
The first time I heard the word “MTHFR,” I thought my friend Ellen was swearing. We were on the porch with iced tea, and she said her doctor had told her she had an MTHFR variant and that's why the regular folic acid in her multivitamin wasn't doing her much good. I asked her to spell it. Then I went home and spent two hours reading.
What I learned changed how I think about B vitamins for neuropathy. There's a form of folate called L-methylfolate (the active form your body actually uses) that bypasses a metabolic step many people can't complete properly. For folks with diabetic neuropathy in particular, the combination of L-methylfolate, methylcobalamin, and pyridoxal-5′-phosphate has real research behind it — including a randomized clinical trial. It's not a miracle cure. It's also not snake oil. It sits in the small but useful category of “supplement-class interventions with actual evidence.”
Here's what I want you to know about L-methylfolate, who it might help, what it costs, and how to talk about it with your doctor.
What Folate Actually Does for Your Nerves
Folate (vitamin B9) is essential for keeping nerves healthy in several specific ways:
Key Takeaway
L-methylfolate is the active form of folate that bypasses the MTHFR conversion step (which 30-40% of people perform poorly). For diabetic peripheral neuropathy, the prescription combination Metanx (L-methylfolate + methylcobalamin + P-5-P) showed modest but real symptom improvement in a 24-week randomized trial. Best benefit: people with MTHFR variants, on metformin, with elevated homocysteine, or documented diabetic neuropathy.
- Myelin sheath maintenance. The protective coating around nerve fibers needs steady folate availability to stay intact. When myelin breaks down, signals don't travel cleanly — you get the burning, tingling, slowed conduction that defines neuropathy.
- Homocysteine clearance. Folate helps the body convert homocysteine (a toxic byproduct of normal metabolism) into methionine. When folate runs short, homocysteine builds up. Elevated homocysteine independently damages blood vessels and nerve tissue and has been linked to peripheral neuropathy progression.
- Nitric oxide production. Healthy nitric oxide signaling keeps the small blood vessels feeding your nerves dilated and delivering oxygen. Folate is part of that pathway.
- DNA synthesis and repair in fast-dividing tissues — including the cells that support nerve regeneration.
If your folate is low — really low, or just functionally inadequate — your nerves don't get the maintenance support they need. This is part of why low folate has been on the differential for unexplained neuropathy for decades.
The Folic Acid Problem
Here's where things get interesting, and where most multivitamins fall short.
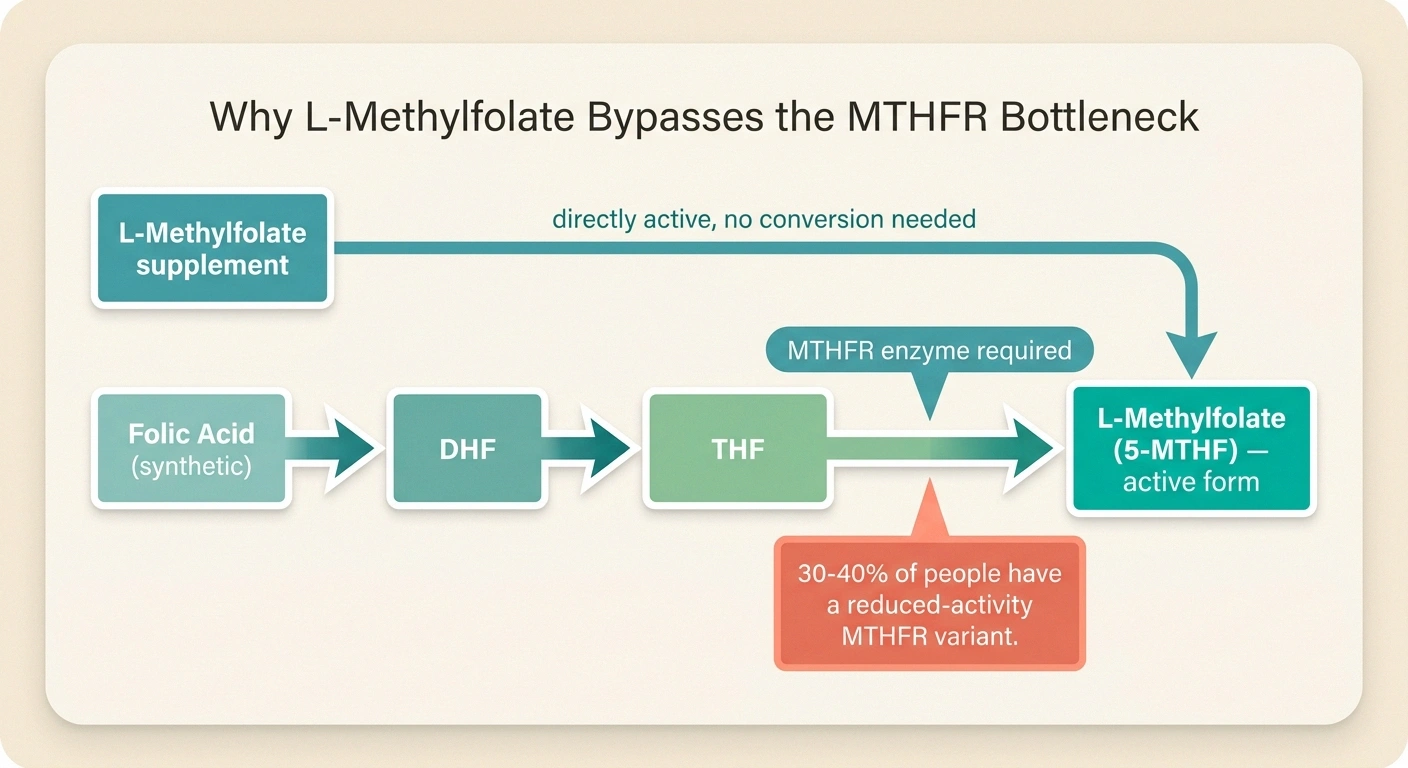
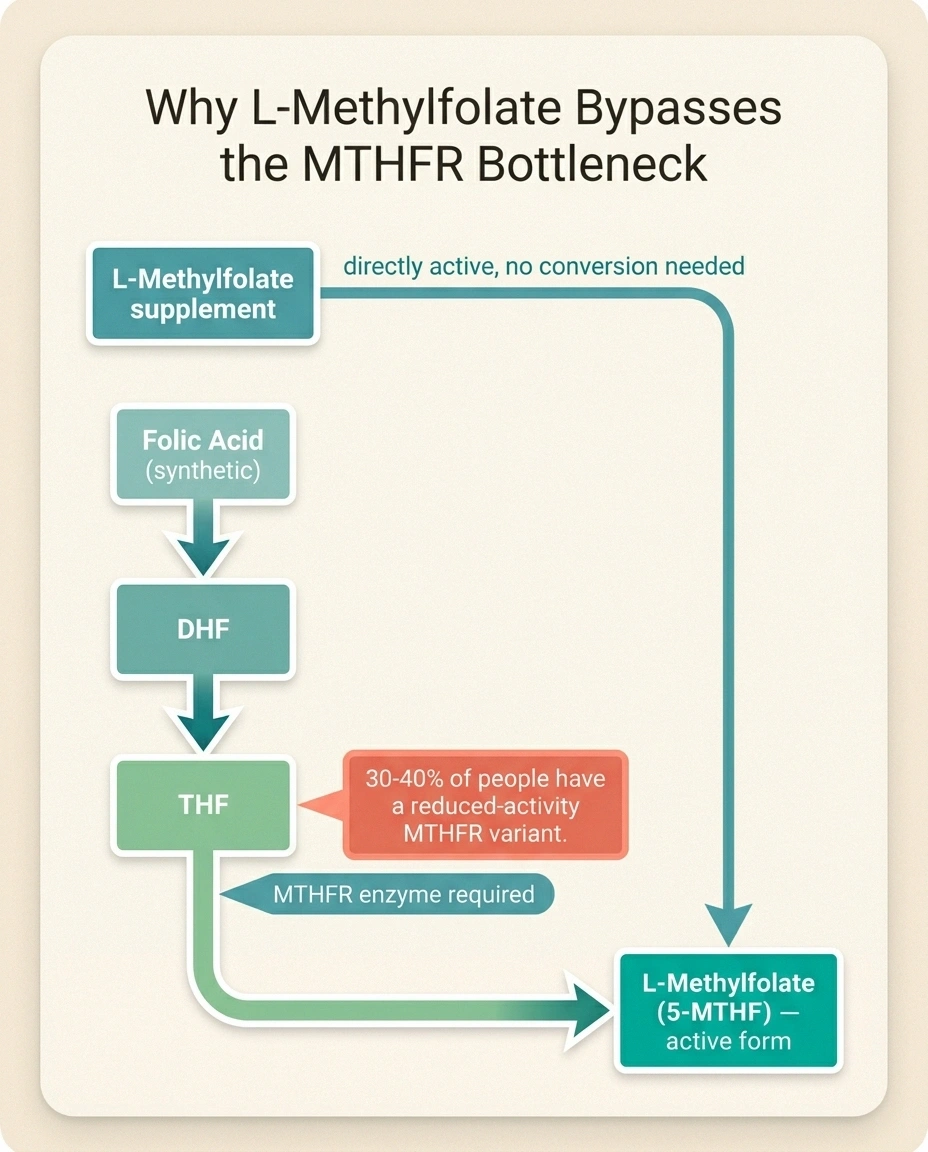
The Folate Pathway — Why MTHFR Matters
Step 1: Folic Acid (synthetic, in most multivitamins)
Cannot be used directly — requires multiple conversions.
Step 2: DHF → THF (intermediate forms)
Several enzyme conversions happen here.
Step 3: THF → L-Methylfolate (the active form)
This step requires the MTHFR enzyme. People with MTHFR C677T variants do this step at 30-70% reduced efficiency.
L-Methylfolate Supplement → bypasses Steps 1-3
Already in active form. Crosses the blood-brain barrier. No conversion required. Works for everyone, especially MTHFR variants.
Folic acid, the form found in nearly every multivitamin and added to fortified breads and cereals, is synthetic. Your body cannot use it directly. It has to be converted through several steps before it becomes the active form, 5-methyltetrahydrofolate (also called 5-MTHF or L-methylfolate), which is the only form that actually crosses the blood-brain barrier and gets used by cells.
The final conversion step depends on an enzyme called methylenetetrahydrofolate reductase — abbreviated MTHFR. And here's where genetics enters the picture: an estimated 30 to 40 percent of the general population carries at least one copy of a common MTHFR gene variant called C677T. About 10 to 15 percent are homozygous (two copies). The variant reduces MTHFR enzyme activity:
- One copy of C677T → about 30 to 40 percent reduction in enzyme activity
- Two copies of C677T → about 70 percent reduction
Translation: a meaningful chunk of the population converts folic acid to active folate poorly. They can take a multivitamin every day for years and still not get adequate active folate to their nerves. The unconverted folic acid can also build up in the blood as “unmetabolized folic acid,” which has its own emerging concerns.
L-methylfolate (the supplement form) skips that conversion entirely. It's the active form already, ready for the body to use. For people with MTHFR variants, this can be the difference between a B-vitamin doing nothing and a B-vitamin actually working.
Who Most Likely Benefits
L-methylfolate isn't going to help everyone with neuropathy. The people most likely to see real benefit:
L-Methylfolate Most Likely Helps If You Have:
- A documented MTHFR variant (especially homozygous C677T)
- Diabetic peripheral neuropathy (the strongest evidence base)
- Long-term metformin use (depletes B12 and folate)
- Elevated homocysteine on bloodwork
- Low or low-normal folate or B12 levels
- Tried regular folic acid B-complex without benefit
- People with documented MTHFR variants (C677T or A1298C, especially homozygous or compound heterozygous)
- People with diabetic peripheral neuropathy — this is where the strongest clinical evidence sits
- People taking metformin long-term — metformin depletes both B12 and folate over years; restoring active forms often helps
- People with elevated homocysteine on bloodwork — a sign that folate (or B12, or B6) isn't keeping up
- People with low or low-normal folate or B12 levels
- People with neuropathy who haven't gotten relief from regular folic acid in a B-complex
If you have well-controlled diabetes, normal folate and B12 status, no MTHFR variant, and no homocysteine elevation — L-methylfolate is unlikely to be a game-changer. It's not magic. It's correction of a specific deficiency or processing problem.
The Evidence: What Metanx Actually Showed
The most-cited clinical study on L-methylfolate for neuropathy used a prescription product called Metanx. Each Metanx capsule contains:
The Metanx Trial — What It Showed
24-week RCT, 214 patients with type 2 diabetes + neuropathy. Half got Metanx (3 mg L-methylfolate + 2 mg methylcobalamin + 35 mg P-5-P twice daily); half got placebo.
Results: Statistically meaningful improvement in vibration perception, neuropathy symptom scores, and quality of life. Did NOT improve nerve conduction velocity (suggesting symptom relief, not nerve regeneration).
Honest read: modest, real, symptomatic relief — not a cure. Best as part of a broader plan including good blood sugar control and nerve pain medications.
- 3 mg of L-methylfolate (as the calcium salt, Metafolin)
- 2 mg of methylcobalamin (active B12)
- 35 mg of pyridoxal-5′-phosphate, P-5-P (active B6)
This combination is sometimes called the “methylation triad” because all three vitamins work together in the methylation cycle that maintains nerve health and clears homocysteine.
The pivotal trial, published in 2013, was a 24-week randomized double-blind placebo-controlled study of 214 patients with type 2 diabetes and peripheral neuropathy. Half got Metanx twice daily; half got placebo. Results:
- Statistically meaningful improvement in vibration perception (a measure of large-fiber nerve function)
- Improvement in patient-reported neuropathy symptom scores
- Improvement in quality-of-life measures
- Did not improve nerve conduction velocity (suggesting it relieved symptoms rather than regrowing nerves)
- Generally well tolerated, with side effects similar to placebo
The honest read on this: it's modest, real, symptomatic relief for diabetic neuropathy — particularly meaningful for patients who weren't getting enough from prescription nerve pain medications alone. It's not a cure and shouldn't be sold as one. It is a legitimate addition to the toolkit. A 2026 narrative review in Endocrine Practice reached similar conclusions: best benefit in patients with confirmed deficiencies, MTHFR variants, metformin use, or elevated homocysteine.
L-Methylfolate vs the Other Folate Forms
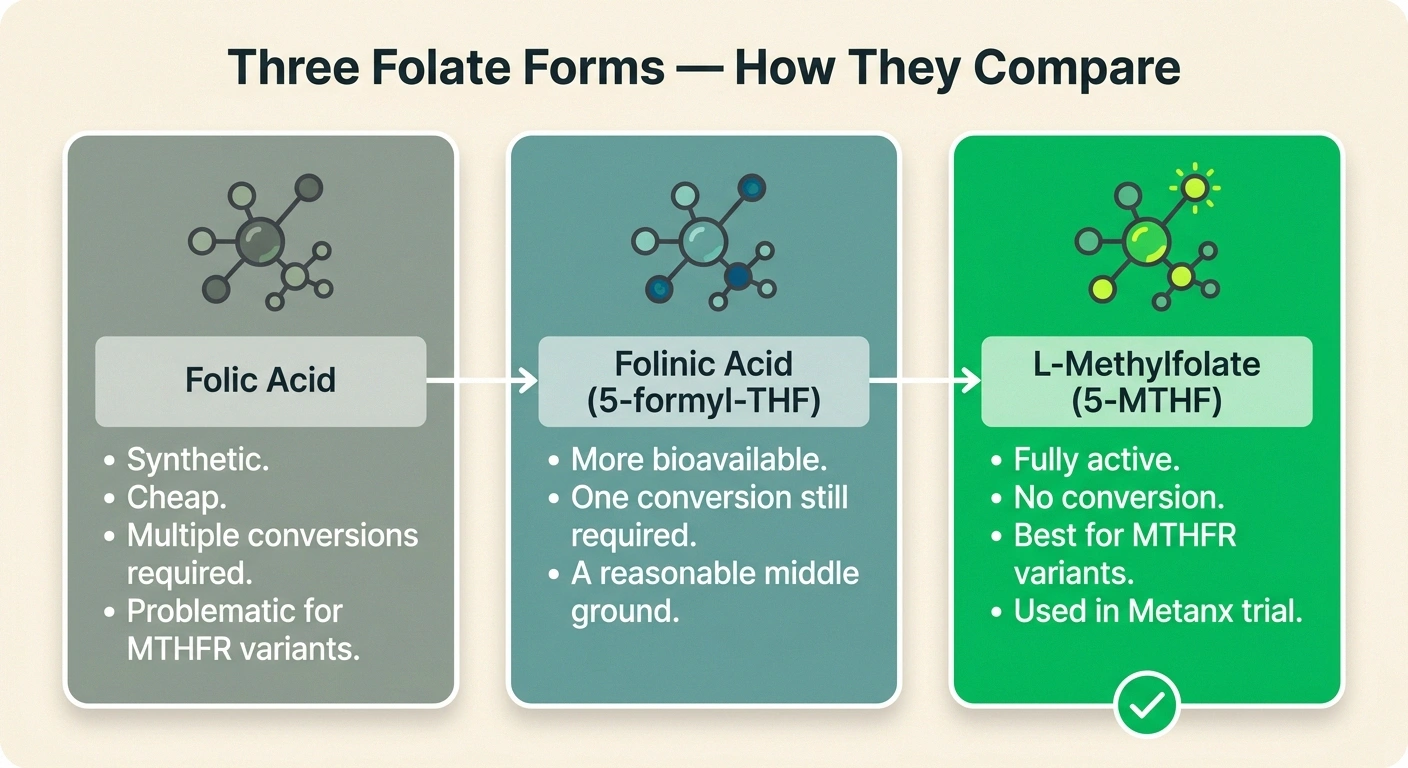
You may see several different folate forms on supplement labels. Here's how they compare:
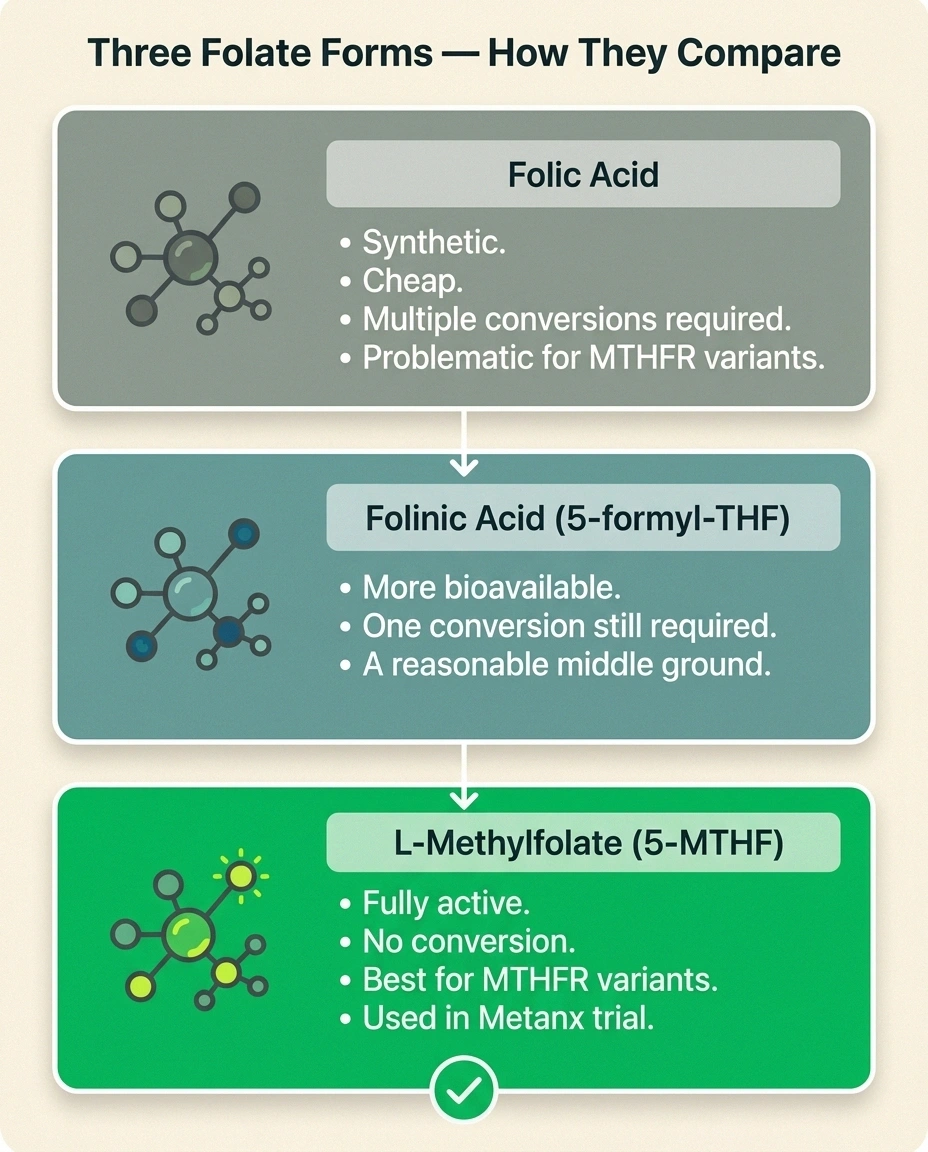
- Folic acid: Synthetic. Cheap. Found in most multivitamins and fortified foods. Requires multiple conversion steps to become useful. Problematic for people with MTHFR variants. Some concerns about unmetabolized folic acid building up in blood with high intakes.
- Folinic acid (5-formyl-THF, leucovorin): A more bioavailable form than folic acid. Partially active — still requires one conversion step. A reasonable middle ground. Used medically alongside methotrexate and certain chemo regimens.
- L-methylfolate (5-MTHF, L-5-MTHF, Metafolin, Quatrefolic): The fully active form. No conversion needed. The form best suited for MTHFR variants and the form used in the Metanx clinical trial.
If you're going to invest in this, pay for the active form. The price difference between a folic-acid B-complex and an L-methylfolate B-complex is small in real-money terms.
Dosing: Start Low, Go Slow

L-methylfolate is one of the supplements where more is not always better. Sensitive individuals can over-methylate and experience anxiety, irritability, headache, or insomnia. Here's a sensible approach:
L-Methylfolate Dosing Reference
Metanx prescription
1 capsule twice daily — 6 mg L-methylfolate + 4 mg methylcobalamin + 70 mg P-5-P total per day
OTC equivalent for neuropathy
L-methylfolate 1-7.5 mg/day + methylcobalamin 1-5 mg + P-5-P 25-50 mg
Conservative starting point
1 mg L-methylfolate daily for 2 weeks → 2-3 mg if tolerated → titrate up if needed
Why start low
Sensitive individuals can over-methylate — anxiety, headache, insomnia. Starting low identifies your tolerance cleanly.
- Metanx prescription dosing: 1 capsule twice daily (= 6 mg L-methylfolate, 4 mg methylcobalamin, 70 mg P-5-P daily total)
- Over-the-counter equivalent for neuropathy: 1 to 7.5 mg L-methylfolate daily, paired with 1 to 5 mg methylcobalamin and 25 to 50 mg P-5-P
- Conservative starting point: 1 mg L-methylfolate daily for the first two weeks; if tolerated, increase to 2-3 mg; if needed and tolerated, work up further
- For MTHFR-related miscarriage workup or pregnancy planning: different rules entirely — talk to a specialist
- For depression dosing: 7.5 to 15 mg daily is sometimes used, but this is a different application from neuropathy
The “start low” principle protects you from over-methylation symptoms. If you start at 5 mg and feel anxious or wired the first few days, you can't tell whether it's the dose or just adjustment. Starting at 1 mg gives you a clean baseline to titrate from.
Side Effects to Watch For
Most people tolerate L-methylfolate well. The side effects that do show up are mostly related to the methylation system being more active than your body is used to:
- Anxiety, irritability, or feeling “wired”
- Headache
- Insomnia
- Mild GI upset
- Rash (uncommon)
- Mood instability — particularly in people with bipolar disorder, where methylation supplements can sometimes destabilize mood
If you start L-methylfolate and your mood worsens within a few days, stop and discuss with your doctor before resuming at a lower dose. The “start low” approach minimizes this risk but doesn't eliminate it. A small percentage of people simply don't tolerate methyl donors well at any dose, and that's information worth having.
Drug Interactions to Know About

L-methylfolate isn't a passive supplement. It interacts meaningfully with several common medications:
Talk to Your Doctor First If You Take:
- Methotrexate (rheumatoid arthritis, psoriasis, cancer) — methylfolate can interfere
- Sulfasalazine — another folate antagonist
- Anticonvulsants (phenytoin, carbamazepine, valproate, phenobarbital)
- Trimethoprim, pyrimethamine (folate-antagonist antibiotics)
- Bipolar disorder medications (high-dose methylation can destabilize mood)
Bring your full supplement list to your next appointment. Pharmacists are particularly good at catching these.
- Methotrexate — used for rheumatoid arthritis, psoriasis, and some cancers. Methotrexate works partly by blocking folate metabolism. High-dose methylfolate may interfere with methotrexate's effectiveness. Always discuss with the prescribing rheumatologist or oncologist before starting.
- Sulfasalazine — also a folate antagonist. Same conversation needed.
- Anticonvulsants — phenytoin, carbamazepine, valproate, phenobarbital all reduce folate levels and can be affected by supplementation. Coordinate with your neurologist.
- Trimethoprim and pyrimethamine — folate antagonists used for infections.
- Metformin — depletes B12 and contributes to folate inadequacy. Adding methylated B vitamins is often appropriate but worth flagging to your doctor.
Bring your supplement list to your next appointment. Pharmacists are particularly good at catching these interactions.
Don't Forget the Other Methylation Players
L-methylfolate doesn't work alone. The methylation cycle that keeps your nerves healthy also depends on:
- Methylcobalamin (active B12). Folate and B12 work in tandem. If you take high-dose folate without enough B12, you can mask a B12 deficiency while neuropathy continues to worsen. Always pair them.
- Pyridoxal-5′-phosphate (active B6). The third member of the trio. Helps complete the methylation cycle.
- Riboflavin (B2). Required as a cofactor for the MTHFR enzyme itself.
- Choline and betaine. Provide methyl groups through alternative pathways.
This is why a comprehensive B-complex with all the active forms (methylated B12, P-5-P, riboflavin) is often a smarter purchase than L-methylfolate alone. Look for products that specifically state they use the active forms — not just “B12” but “methylcobalamin,” not just “B6” but “P-5-P” or “pyridoxal-5′-phosphate.” Our broader guide to neuropathy supplements for nerve health covers how all these pieces fit together.
Should You Get MTHFR Testing?
This is a genuine question without a clean answer. The arguments for testing:
- It tells you whether you should pay extra for L-methylfolate vs ordinary folic acid
- It can explain why certain medications or supplements have worked poorly
- It informs decisions for women planning pregnancy
- Many commercial DNA testing services (23andMe, AncestryDNA via third-party tools) include MTHFR variants
The arguments against:
- L-methylfolate is generally safe to try without testing — if it works, it works
- MTHFR testing can lead to over-medicalization and supplement stacking that isn't needed
- Most insurance won't cover MTHFR testing in the absence of specific clinical indications
For most people with neuropathy considering L-methylfolate, my practical advice is: a careful trial of an active-form B-complex including L-methylfolate is reasonable without genetic testing first. If it helps, you've got your answer. If you have a strong personal or family history of vascular disease, miscarriage, or psychiatric illness, the testing may be more useful.
How to Try It Sensibly
If you and your doctor decide L-methylfolate is worth a trial, here's a sensible approach:
A Sensible 12-Week Trial
- Baseline labs: folate, B12, homocysteine, methylmalonic acid, HbA1c, CBC
- Pick the right product — active-form B-complex with L-methylfolate, methylcobalamin, P-5-P
- Start at 1 mg/day for 2 weeks; if tolerated, increase to 2-3 mg
- Track symptoms weekly in a simple diary (burning, numbness, sleep, function)
- Recheck labs at 3 months — folate up, homocysteine down if it was elevated
- Decide: meaningful improvement = continue; nothing changed at adequate dose = stop, no taper needed
- Get baseline labs first. Folate, B12, homocysteine, methylmalonic acid (a more sensitive B12 marker), HbA1c if diabetic, CBC, and a basic chemistry panel. This gives you a starting point to measure change against.
- Pick the right product. Either Metanx by prescription, or a quality OTC active-form B-complex with L-methylfolate, methylcobalamin, and P-5-P. Avoid anything with just folic acid.
- Start low. 1 mg L-methylfolate daily for the first two weeks. If tolerated, increase to 2-3 mg.
- Track symptoms. Keep a simple neuropathy symptom diary for 8 to 12 weeks — burning intensity, numbness, sleep quality, function. Hard data beats memory.
- Recheck labs at 3 months. Folate level should be higher; homocysteine should be lower if it was elevated at baseline.
- Decide. If symptoms have improved meaningfully and labs have moved appropriately, continue. If nothing has changed in 3 months at adequate dose, it's not the answer for you and you can stop without taper.
The Honest Place to Land
L-methylfolate isn't going to fix every neuropathy. It's not going to regrow nerves that have died. It's not going to make a poorly controlled diabetes manageable on its own. What it can do, for a meaningful subset of people — particularly those with MTHFR variants, on metformin, with elevated homocysteine, or with documented diabetic peripheral neuropathy — is take the edge off symptoms and support the underlying methylation chemistry that keeps nerves functioning.
It's the kind of intervention I'd put in the same category as alpha-lipoic acid or benfotiamine: real evidence, modest benefit, low risk for most people, worth a thoughtful trial under medical supervision. Combined with good blood sugar control, the right prescription medications, gentle movement, and the other levers we talk about, it can be one of several small wins that add up.
Ellen, the friend on the porch with the iced tea? She's been on a quality active-B complex for two years now. Her homocysteine dropped from 14 to 8. Her A1c is steady. She still has neuropathy — but the burning that used to wake her up at 3 a.m. doesn't anymore, and her last vibration test showed slight improvement. She'll take it. So would I.
Frequently Asked Questions
What is L-methylfolate and how is it different from folic acid?
L-methylfolate (5-methyltetrahydrofolate, or 5-MTHF) is the biologically active form of folate that your body actually uses. Folic acid, the synthetic form found in most multivitamins and fortified foods, has to be converted through several steps before it becomes L-methylfolate. The final conversion depends on the MTHFR enzyme, which a meaningful portion of the population (30 to 40 percent with at least one C677T variant) produces in reduced amounts. L-methylfolate skips the conversion entirely, making it more usable for people with MTHFR variants and generally more efficient for everyone else too.
Does L-methylfolate help with neuropathy?
The strongest evidence is for diabetic peripheral neuropathy. A 24-week randomized placebo-controlled trial of Metanx (which combines L-methylfolate with methylcobalamin and pyridoxal-5′-phosphate) in 214 patients with type 2 diabetes and neuropathy showed improvement in vibration perception, neuropathy symptom scores, and quality of life compared to placebo. It did not improve nerve conduction velocity, suggesting symptomatic relief rather than nerve regeneration. The benefit is modest but real, and is most pronounced in patients with MTHFR variants, on metformin, or with elevated homocysteine.
What is Metanx and do I need a prescription?
Metanx is a prescription “medical food” product containing 3 mg of L-methylfolate, 2 mg of methylcobalamin (active B12), and 35 mg of pyridoxal-5′-phosphate (active B6) per capsule, taken twice daily. Because it's a medical food rather than a drug, it's prescribed by your doctor for the dietary management of diabetic peripheral neuropathy. It can be expensive, especially without insurance coverage. Quality over-the-counter active-form B-complex supplements with similar ingredients at similar doses are available at a fraction of the cost — discuss with your doctor whether either is right for you.
What dose of L-methylfolate is typical for neuropathy?
Most clinical use for neuropathy falls in the range of 1 to 7.5 mg daily, often paired with 1 to 5 mg of methylcobalamin and 25 to 50 mg of pyridoxal-5′-phosphate. The Metanx prescription delivers 6 mg of L-methylfolate per day (3 mg twice daily). A sensible OTC starting point is 1 mg daily for two weeks, increasing to 2 to 3 mg if tolerated. Higher doses (7.5 to 15 mg) are sometimes used for depression but are a different application than neuropathy. Always start low and titrate up to identify your tolerance and effective dose.
Are there side effects of L-methylfolate?
Most people tolerate it well. The side effects that do occur are mostly related to over-methylation in sensitive individuals: anxiety, irritability, feeling “wired,” headache, insomnia, and sometimes mild GI upset. Rash is uncommon. People with bipolar disorder should be cautious as methylation supplements can sometimes destabilize mood. Starting at a low dose (1 mg daily) and titrating up gradually allows you to identify side effects early. If mood worsens noticeably within the first few days, stop and discuss with your doctor before considering a lower dose.
Should I get tested for MTHFR variants before taking L-methylfolate?
Not necessarily. Genetic testing for MTHFR can be informative if you have a strong personal or family history of vascular disease, recurrent miscarriage, or psychiatric illness — and many commercial DNA testing services include MTHFR variants. But for most people considering L-methylfolate for neuropathy, a careful trial of an active-form B-complex without testing is reasonable. If symptoms improve over 8 to 12 weeks and homocysteine drops, you have your answer. If it does nothing, you can stop without consequence. Most insurance does not cover MTHFR testing without specific clinical indications.
Can I take L-methylfolate with my other medications?
Most of the time yes, but several important interactions exist. Methotrexate (used for rheumatoid arthritis and some cancers) and sulfasalazine work partly by blocking folate metabolism, so high-dose methylfolate may interfere — always coordinate with the prescribing doctor. Anticonvulsants like phenytoin, carbamazepine, and valproate reduce folate levels and can be affected by supplementation. Metformin depletes B12 and folate, so adding methylated B vitamins is often appropriate but should be flagged. Bring your full supplement and medication list to your next appointment so your doctor or pharmacist can spot anything important.
How long does it take to see results from L-methylfolate for neuropathy?
Allow at least 8 to 12 weeks at an adequate dose before deciding whether it's working. The Metanx trial measured outcomes at 24 weeks, and the most consistent symptom improvements were apparent by the 12-week mark. Track symptoms in a simple diary so you can compare honestly against baseline rather than relying on memory. If your homocysteine was elevated at baseline, recheck it at 3 months — a meaningful drop suggests the methylation pathway is responding even if symptom changes are subtle. If nothing has changed at 3 months on adequate dose, it's reasonable to conclude this isn't the answer for you and stop.


