
If you live with small-fiber neuropathy that no one can pin a cause to — the kind doctors call “idiopathic” — you've probably had a sentence said to you that doesn't sit well. Something like: “There's no specific treatment for your condition. We can try to manage the pain.” For many people with idiopathic small-fiber neuropathy (iSFN), that conversation has been the ceiling of medical care for decades.
I want to walk you through an investigational therapy that might one day shift that ceiling. Its development name is ST-503. It's an experimental gene therapy from Sangamo Therapeutics that takes a fundamentally different approach to nerve pain: instead of taking a pill every day to dampen pain signals, ST-503 is a one-time injection designed to turn DOWN the gene responsible for producing a key pain-signaling protein called Nav1.7. The U.S. Food and Drug Administration has cleared its Investigational New Drug application, and a Phase 1/2 clinical trial is currently enrolling patients.
I want to be honest from the start: this is early-stage, ambitious, invasive, and unproven in humans for this condition. It is not available outside the trial. It will not be available in a pharmacy anytime soon. The earliest realistic timeline for any FDA approval is well into the 2030s, and that's assuming the trials succeed. But if you have iSFN, or you love someone who does, this is one of the most scientifically interesting things happening in the neuropathy world right now, and you deserve a careful, honest explainer.
What ST-503 Actually Is
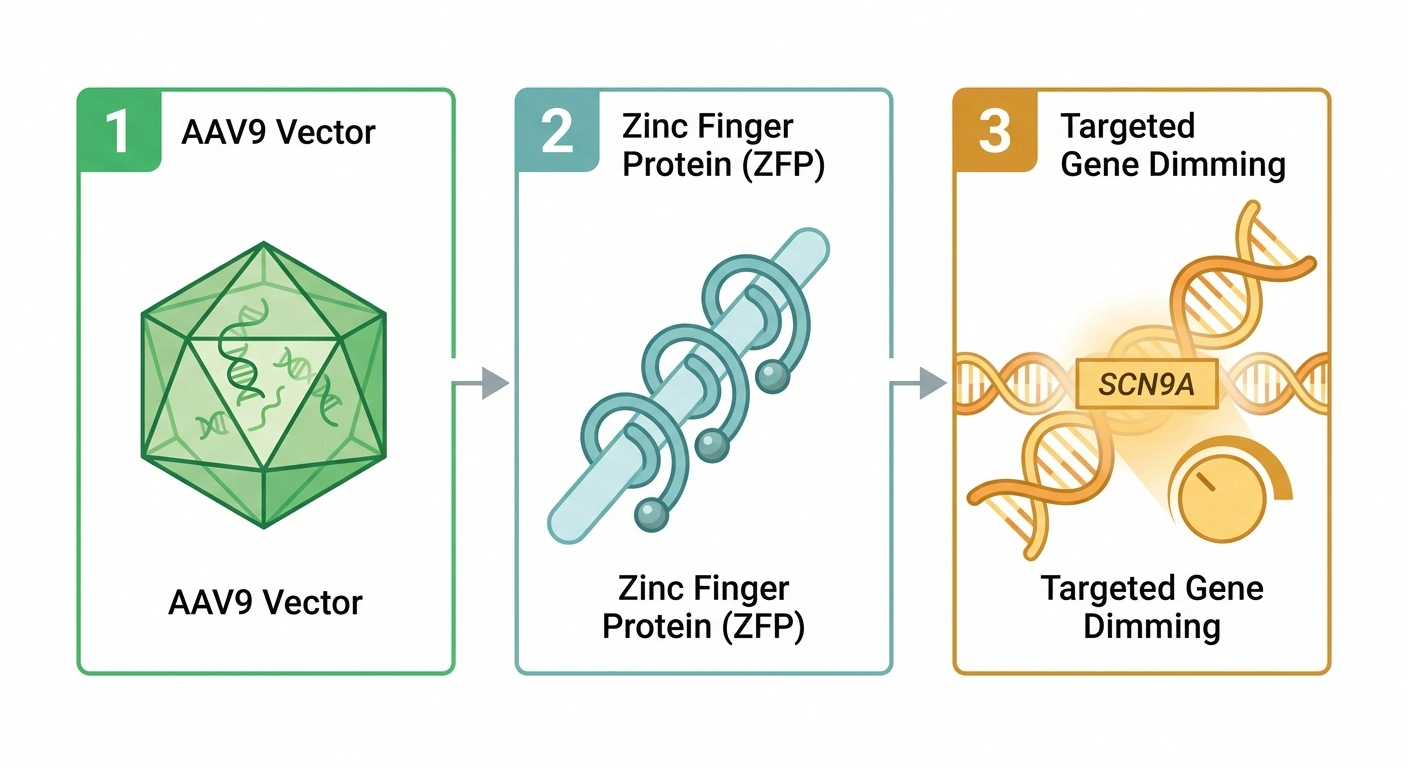
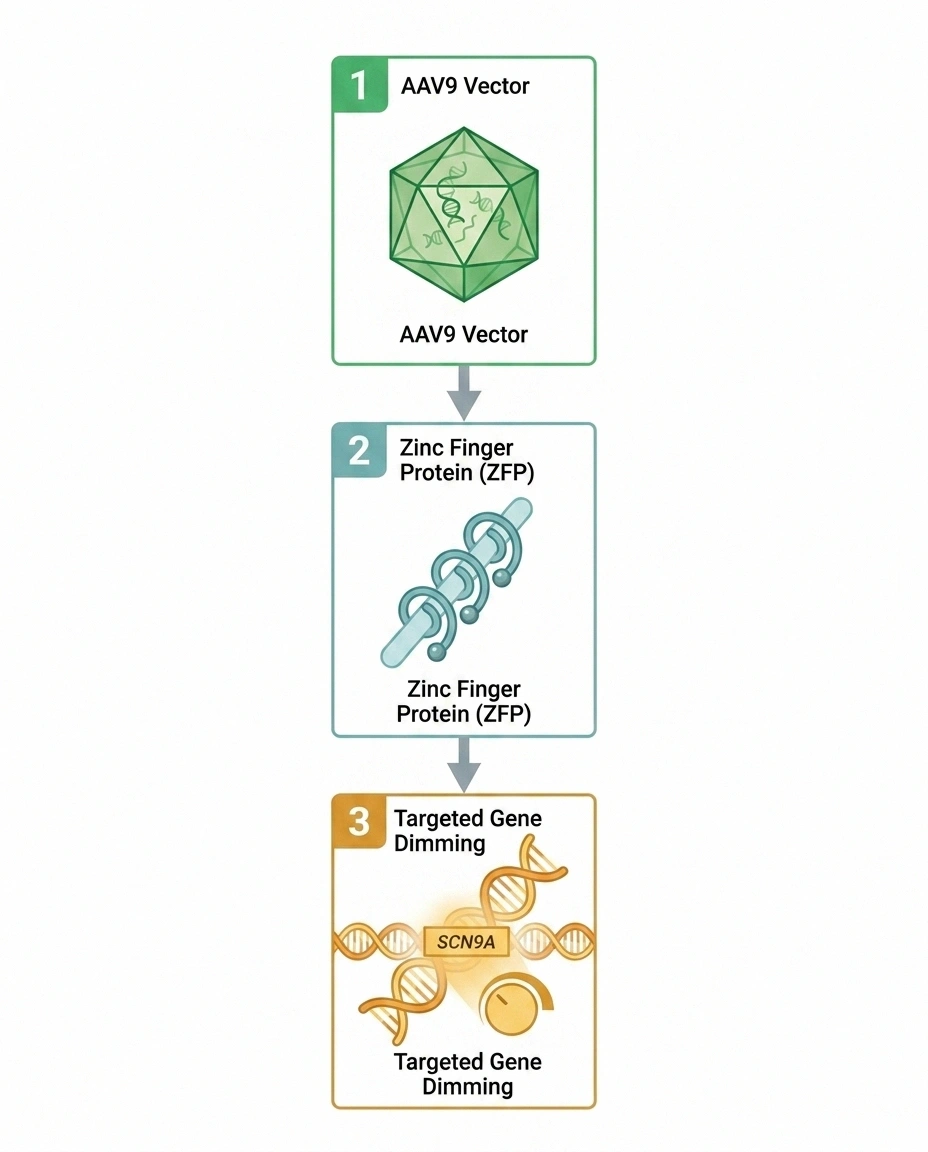
ST-503 is an investigational gene therapy being developed by Sangamo Therapeutics. Three pieces of vocabulary unlock what it does — let me translate them in order.
“Gene therapy” means the treatment changes how a gene behaves rather than supplying a drug to block a protein. In ST-503's case, the goal is to reduce — not eliminate, not remove — the activity of a specific gene called SCN9A in sensory nerve cells.
“Zinc finger repressor” is the molecular tool ST-503 uses to do that turning-down. Think of it as a very precise switch that recognizes the SCN9A gene and dampens its activity, the way a dimmer reduces light without turning it off completely.
“AAV9” is the delivery vehicle. AAV stands for “adeno-associated virus,” and the number 9 refers to a specific subtype that is good at reaching nerve cells. The AAV9 used in ST-503 is a modified, non-disease-causing virus that has been used as a delivery vehicle in other FDA-approved gene therapies. It carries the zinc finger repressor into the sensory neurons where Nav1.7 is made.
Put together: a one-time injection delivers a precise molecular dimmer into your sensory nerve cells, which then turns down the volume on a single, specific pain-signaling protein. That's the whole concept.
Why Nav1.7 — The Story of a Pain Gene
Researchers didn't pick Nav1.7 at random. The choice of target came from something remarkable: human beings born with rare mutations in the SCN9A gene who have given scientists a natural experiment.
Some people are born with what's called congenital insensitivity to pain. They have a mutation that essentially turns off Nav1.7. They are otherwise neurologically normal — they can think, move, feel touch, feel temperature, feel pleasure. They can detect that something is hot or cold. What they cannot feel is physical pain. (This is dangerous, by the way — people with this condition often have unnoticed injuries and require constant vigilance. Pain has a purpose.)
Other people are born with the opposite kind of mutation — one that makes Nav1.7 hyperactive. They develop a condition called inherited erythromelalgia, with episodes of burning, lightning-like pain in the feet and hands that look almost identical to severe small-fiber neuropathy.
What this told researchers is profound: Nav1.7 is essentially the pain-volume knob for the peripheral nervous system. Turn it down — you reduce pain. Turn it up — you cause pain that feels exactly like what iSFN patients describe.
That biological validation is one of the strongest cases in modern pain research for a specific target. Pharmaceutical companies have spent more than a decade trying to design small-molecule pills that selectively block Nav1.7 — and they have largely failed, because Nav1.7 is structurally so similar to other sodium channels (Nav1.5 in the heart, Nav1.4 in skeletal muscle) that selective blocking has been extraordinarily difficult. Gene therapy elegantly sidesteps the selectivity problem because it acts only where the gene is expressed — in peripheral sensory neurons.
How Idiopathic Small-Fiber Neuropathy Fits the Picture

Small-fiber neuropathy affects the smallest, unmyelinated nerve fibers in the skin — the ones that carry temperature sensation and a particular kind of burning, prickling, electric pain. About 30 to 50 percent of small-fiber neuropathy cases are idiopathic, meaning despite a thorough workup, no specific cause is identified. Other cases are tied to diabetes, certain autoimmune conditions, viral infections, or genetic conditions. Our small-fiber neuropathy overview walks through the condition in depth.
What iSFN patients tell their doctors — and what they tell me in support groups — sounds like a thesaurus of bad sensations: burning, prickling, stabbing, lightning, electric, glass-shard, sandpaper-feet. Some patients describe a sensation of standing on hot coals or stepping on broken glass when their feet are perfectly normal looking.
Right now, there are no FDA-approved disease-modifying treatments specifically for idiopathic small-fiber neuropathy. Patients are typically prescribed medications that were developed for other types of neuropathic pain — gabapentin, pregabalin, duloxetine, amitriptyline, lidocaine patches — and many find only partial relief. The unmet need is enormous, and ST-503 is one of the only investigational therapies trying to address the underlying biology rather than just dampen symptoms.
What the Phase 1/2 Trial Is Actually Testing

The current ST-503 study is a Phase 1/2 open-label trial. Some specifics:
- Open-label means there is no placebo group — every enrolled patient receives the actual investigational therapy. This is common in early gene therapy trials because the intervention is invasive and one-time, making placebo controls ethically complex.
- Single intrathecal injection. The treatment is delivered via lumbar puncture (a spinal-tap-style procedure) into the cerebrospinal fluid, which lets the AAV9 vector reach the dorsal root ganglia where Nav1.7 is expressed.
- Primary endpoints are safety and tolerability — the basics of “is this safe enough to keep developing?” This is standard for Phase 1.
- Secondary endpoints include pain reduction (typically measured on a numerical rating scale) and changes in small-fiber density on skin biopsy, which is the gold-standard test for confirming small-fiber neuropathy.
The trial is enrolling adults with severe idiopathic small-fiber neuropathy whose pain has not responded to multiple standard medications. Pre-existing immunity to AAV9 — which some adults have from natural exposure — is likely to be a disqualifying screening criterion, since neutralizing antibodies could destroy the AAV9 vector before it delivers its cargo.
If you or someone close to you might be interested in trying to enroll, our guide to neuropathy clinical trials covers how to search ClinicalTrials.gov, what questions to ask the study coordinator, and what informed consent should look like.
The Preclinical Evidence — What Sangamo Has Shown So Far
Sangamo's published and disclosed preclinical work has shown three things worth knowing:
First, in non-human primates, a single intrathecal dose of ST-503 produced substantial, durable reductions in Nav1.7 expression in the dorsal root ganglia — the cluster of sensory nerve cell bodies just outside the spinal cord that ST-503 is designed to reach.
Second, the reduction in Nav1.7 was accompanied by reduced pain-related behavior in animal pain models. This is a translational marker — animal pain models don't perfectly predict human pain outcomes, but they're the standard preclinical evidence base.
Third — and this matters for safety — Sangamo has reported that off-target gene effects were not observed in nonhuman primate safety studies. Off-target activity (where a gene-editing or gene-repression tool accidentally affects genes other than the one it's designed to target) is one of the central safety concerns in gene therapy. The preclinical data is reassuring on this point but obviously doesn't replace human safety data.
This package of preclinical evidence is what supported the FDA clearing Sangamo's Investigational New Drug application to begin the Phase 1/2 human trial.
The Honest Reality Check — What's Different About Gene Therapy
I want to spend real time here because it's where ST-503 differs most from every other neuropathy treatment I've written about.
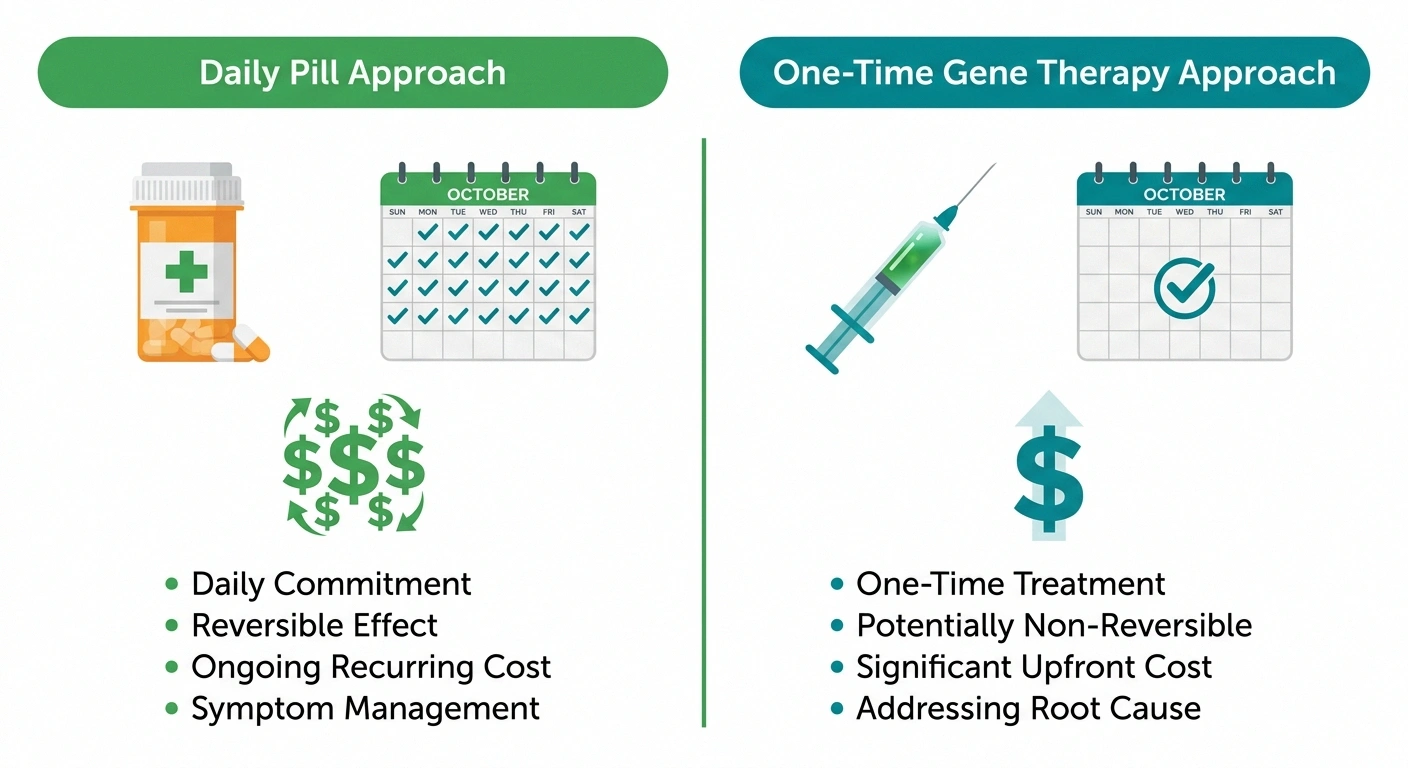
Gene therapy is, for practical purposes, not reversible. If you take gabapentin and have side effects, you stop the pill and the drug clears your system within days. If you receive ST-503 and the zinc finger repressor durably reduces Nav1.7, there is no “off switch.” Sangamo has designed ST-503 to be long-lasting — that's a feature, not a flaw, because the goal is years of pain relief from a single dose. But it also means a serious adverse event from the therapy could not be undone the way you stop a pill.
The procedure itself is invasive. An intrathecal injection — even a properly done one — carries the same risks as a spinal tap: post-lumbar-puncture headache, infection, bleeding, rare nerve injury. For a one-time treatment, these are usually tolerable risks. For a daily pain medication, they would be unacceptable. The risk-benefit calculus is just different from anything you'd compare to a pill.
Reducing pain is not the same as eliminating all pain. Nav1.7 is one of multiple sodium channels involved in pain signaling. Other channels (Nav1.8, Nav1.9, others) carry pain signals too. Reducing Nav1.7 by some percentage is expected to reduce chronic neuropathic pain, but acute protective pain — the kind that tells you you've stepped on something sharp or burned your hand — is mediated by multiple channels and would likely still work. Patients in trials need to know this in advance: you should still feel acute injury pain, and that's by design.
Cost is going to be a major access issue if it ever reaches the market. Other AAV-based gene therapies that are FDA-approved have launched at prices ranging from roughly $850,000 (Luxturna, for an inherited retinal condition) to over $3 million (Hemgenix, for hemophilia B). One-time gene therapies are priced as one-time treatments, not as monthly prescriptions. Insurance coverage at launch is typically limited and improves over years. If ST-503 succeeds, it will not be the affordable option — at least not initially.
Pre-existing immunity excludes some patients. AAV9 is closely related to viruses that circulate in the human population. Many adults have been naturally exposed and carry neutralizing antibodies. Those antibodies can destroy the AAV9 vector before it delivers its cargo, making the therapy ineffective. Screening for anti-AAV9 antibodies will likely be a standard part of eligibility.
How ST-503 Compares to Other Approaches in the Pipeline

For a fuller picture of what's being studied for neuropathic pain, it helps to see ST-503 in the context of other late-stage non-opioid approaches. Our guide to new neuropathy treatments in 2026 covers this landscape, but here's the short version.
The recently approved suzetrigine (Journavx) blocks a different sodium channel, Nav1.8. It is approved for acute pain and is being studied for chronic neuropathic pain. It's a daily pill — convenient and reversible — but its effect on each dose lasts only as long as you keep taking it.
Pilavapadin (LX9211), also covered on our site, is heading to Phase 3 for diabetic neuropathy. It works on a different target called AAK1 and is also a daily oral pill.
VX-993 is another Nav1.8 blocker in earlier development for diabetic neuropathy.
What sets ST-503 apart is its potential to be a one-time treatment — receive the therapy once, and theoretically experience reduced pain for years or potentially longer. No drug-drug interactions to manage. No daily pill burden. No falling off treatment when your prescription runs out. That's the dream. The price of that dream is invasiveness, irreversibility, and cost.
Who Is This For — Realistically

If ST-503 succeeds in trials and is eventually approved, it is unlikely to be a first-line treatment for everyone with neuropathy. The risk-benefit profile of a one-time, invasive, expensive gene therapy makes the most sense for people who:
- ✓ Severe pain that interferes with sleep, mobility, or daily life
- ✓ Failed adequate trials of multiple oral neuropathy medications
- ✓ A confirmed small-fiber neuropathy diagnosis (typically via skin biopsy)
- ✓ No pre-existing AAV9 immunity (a screening blood test)
- ✓ Comfort with the irreversibility of a gene therapy intervention
- Have severe, function-limiting neuropathic pain — pain that interferes with sleep, mobility, work, or basic daily activities.
- Have tried and failed adequate trials of multiple oral medications.
- Have a clear small-fiber neuropathy diagnosis (typically confirmed by skin biopsy or quantitative sensory testing). Our neuropathy diagnosis guide covers what those tests look like.
- Don't have pre-existing AAV9 immunity that would block the therapy.
- Understand and accept the irreversibility of the intervention.
The neuropathy population is heterogeneous — diabetic neuropathy, chemotherapy-induced neuropathy, idiopathic small-fiber neuropathy, autoimmune neuropathies, and many others. ST-503 is currently being studied specifically in idiopathic small-fiber neuropathy. Whether the Nav1.7-reduction approach would work for diabetic or chemo neuropathy hasn't been tested in humans yet. Sangamo has discussed potential expansion into other neuropathic pain conditions if Phase 1/2 results are positive.
What I'll Be Watching
The realistic timeline for ST-503 depends on a long series of milestones. Here's what I'll be tracking and updating in this article as news comes:
- Phase 1/2 enrollment progress. Sangamo will publish periodic updates on how many patients have been treated.
- Initial safety data from the first treated patients. This is the most consequential near-term milestone. Gene therapy programs sometimes stop here because of unexpected adverse events.
- First efficacy signal. Even with small numbers, the first reports of pain reduction (or no pain reduction) in treated patients will be major news.
- Decision to advance to Phase 3. If safety and early efficacy support it, a larger pivotal Phase 3 trial would follow — likely years away.
- Eventual FDA review. Even with a successful program, FDA approval is realistically in the 2030s.
For readers who want to follow the wider research landscape, our nerve regeneration research guide covers what's being studied beyond gene therapy. And if you're trying to make sense of your own neuropathy symptoms in the meantime, the “what does neuropathy feel like” article can help you describe what you're experiencing to your care team.
A Closing Thought
I've lived with neuropathy long enough to be cautious about anything described as a “breakthrough.” Most things called breakthroughs aren't. Some are. The honest truth about ST-503 is that no one yet knows which category it belongs to — and we won't know for several years.
What I can say is that the scientific reasoning is sound. The target is validated. The delivery technology has worked in other approved gene therapies. The patient population it's designed for has been waiting a very long time for something better than partial symptom control.
It might work. It might not. It might work for some people and not others. The only way we'll find out is for careful, thoroughly consented patients to enroll in well-designed trials and for researchers to report what happens honestly. That process is underway — and that, in itself, is more than iSFN patients have had in a generation.
Frequently Asked Questions
Is ST-503 available now?
No. ST-503 is investigational. It is not approved by the FDA and cannot be prescribed. The only legal way to receive it currently is through enrollment in the Phase 1/2 clinical trial Sangamo is conducting. Anything offered as ST-503 outside that approved trial is not the real therapy.
Is gene therapy reversible?
Not in any practical sense. ST-503 is designed to durably reduce Nav1.7 production in sensory neurons after a single dose. That is intentional — the goal is years of pain relief from one treatment. But it also means a serious adverse effect from the therapy could not be reversed the way stopping a pill ends a drug's effect. This is one of the most important considerations for any patient evaluating gene therapy.
Will ST-503 make me unable to feel any pain?
No, and that's by design. Nav1.7 is one of several sodium channels involved in pain signaling. Reducing it is expected to reduce chronic neuropathic pain while preserving acute protective pain — the kind that warns you about injury, burns, or sharp objects. Other sodium channels (Nav1.8, Nav1.9) carry those signals. Phase 1/2 trials will test how well this distinction holds up in humans.
Who can enroll in the Phase 1/2 trial?
The trial is enrolling adults with severe idiopathic small-fiber neuropathy whose pain has not responded to multiple standard medications. Specific eligibility requirements include a confirmed diagnosis (often via skin biopsy), pain severity criteria, and screening for pre-existing AAV9 immunity. Talk to your neurologist if you think you might be a candidate, and search ClinicalTrials.gov for the current site list.
How does ST-503 differ from a Nav1.7 pill?
Pharmaceutical companies have spent more than a decade trying to develop small-molecule pills that selectively block Nav1.7. The challenge is that Nav1.7 is structurally similar to Nav1.5 (in the heart) and Nav1.4 (in skeletal muscle), making it extremely hard to design a pill that hits Nav1.7 without also affecting the others. Gene therapy avoids this problem because it works at the gene level — only in cells that express that gene, which means peripheral sensory neurons. So far no oral Nav1.7-selective drug has made it through development.
How long does the effect last?
This is one of the biggest open questions. Animal studies suggest durable, multi-year effects. Whether that translates to humans, and exactly how many years, can only be confirmed by long-term human follow-up data — which doesn't exist yet. Realistic patient communication about ST-503 should emphasize that durability beyond the trial period is theoretical until proven.
What does intrathecal injection involve?
Intrathecal injection is delivery of medication into the cerebrospinal fluid via a needle inserted between the vertebrae in the lower back — similar to a spinal tap or epidural. It's done in a hospital or clinical setting by a trained physician. The procedure typically takes less than an hour. Common after-effects can include post-lumbar-puncture headache, mild back soreness, and rarely more serious complications.
If ST-503 succeeds, how much will it cost?
Pricing has not been announced and would not be until close to approval. Other FDA-approved AAV-based gene therapies have launched at prices ranging from roughly $850,000 to over $3 million per treatment. Insurance coverage for one-time gene therapies has historically been very limited at launch and improved over time. Patient assistance programs and value-based payment models exist for some gene therapies, but none of this is settled for ST-503.