
If you've been following the search for new non-opioid nerve pain medications, the name Vertex Pharmaceuticals has probably come up. They're the company behind suzetrigine — sold under the brand name Journavx — which became the first new non-opioid mechanism approved for pain in about 20 years when the FDA cleared it in early 2025 for acute pain. That was a big moment for the field.
What may be less familiar is the drug Vertex hoped would be its follow-up: VX-993. It belongs to the same drug class as suzetrigine — both are sodium-channel blockers targeting a channel called Nav1.8. The idea was straightforward: if suzetrigine works on this pathway, a next-generation cousin might work even better, or work in conditions where suzetrigine showed only modest results.
I want to give you a clear-eyed picture of where VX-993 actually stands as of mid-2026 — including a Phase 2 setback in acute pain that has reshaped expectations, and an ongoing Phase 2 trial in diabetic peripheral neuropathy that is still genuinely unresolved. This is not a hyped news article. The story is more complicated than the headlines suggest, and the readers who deserve the most honest version are the ones managing nerve pain today and weighing whether to hope for it.
What VX-993 Is
VX-993 is an investigational, oral, small-molecule drug being developed by Vertex Pharmaceuticals. Like suzetrigine, it's designed to block the Nav1.8 sodium channel — a key relay station in the way pain signals travel from injured or damaged tissue, through peripheral sensory nerves, toward the spinal cord and brain.
Three things are worth knowing up front:
- It's a pill. Once daily, taken orally. No injections, no infusions.
- It's non-opioid. Same mechanism class as suzetrigine — no opioid receptor activity, no euphoria, no respiratory depression risk, no expected dependence based on what's been seen in trials so far.
- It is investigational. Not FDA-approved, not available by prescription, and currently being tested in clinical trials only.
The Mechanism — What “Nav1.8 Blocker” Means in Plain Language
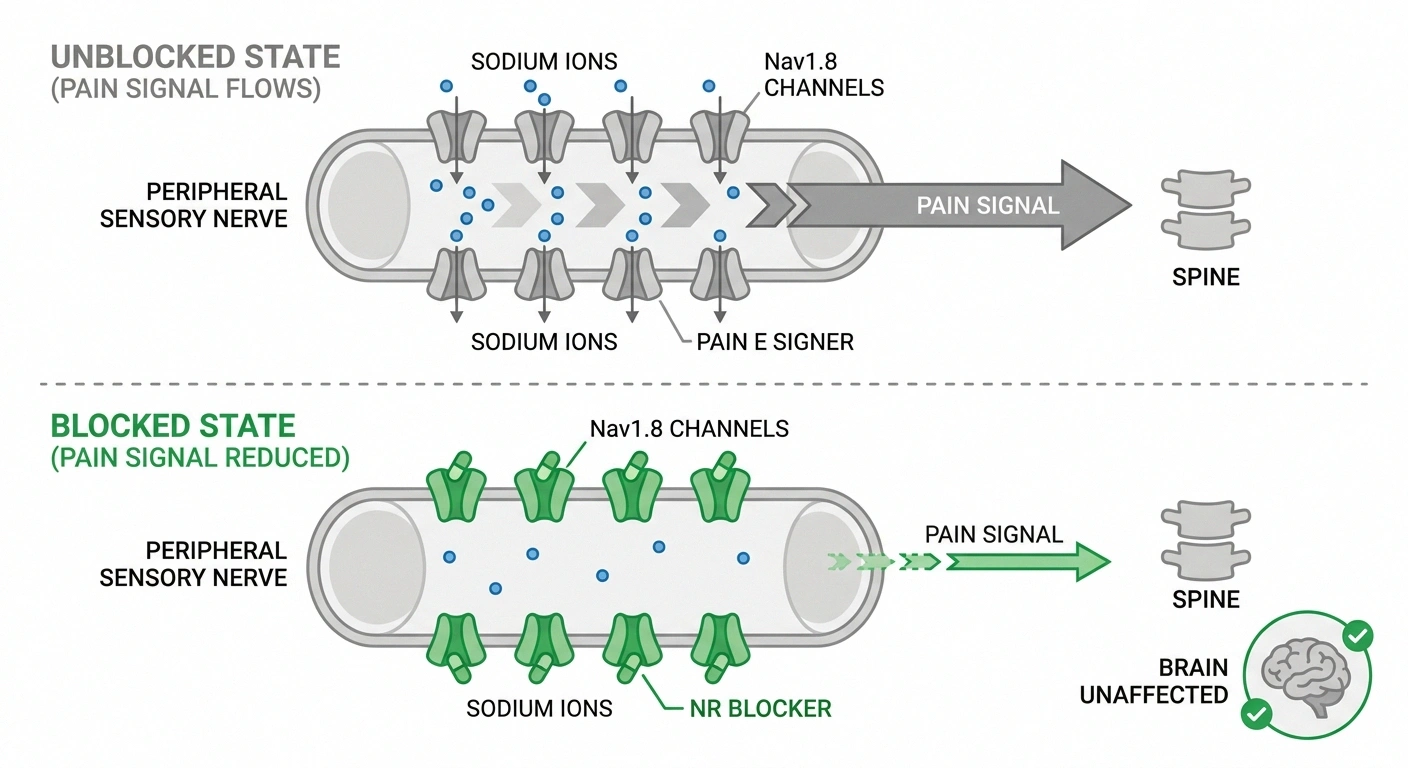
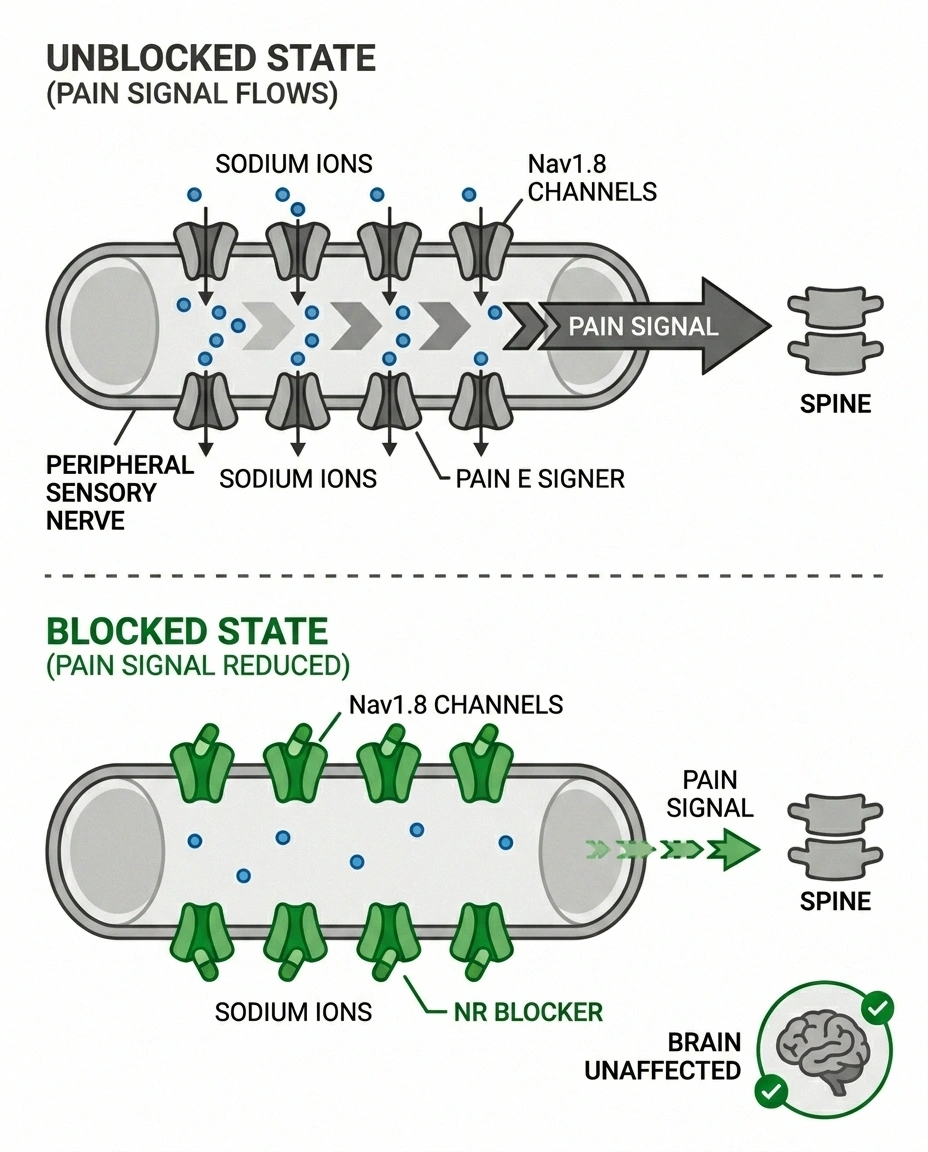
Nav1.8 is a voltage-gated sodium channel — a tiny molecular gate that sits in the membrane of certain nerve cells, particularly in peripheral sensory neurons. When pain-related stimuli (injury, inflammation, nerve damage) cause those cells to fire, sodium has to flow through Nav1.8 channels to keep the signal moving along.
If you block Nav1.8, you don't shut off the entire nerve. You reduce the strength and frequency of pain signals being transmitted. Importantly, Nav1.8 is found mostly in peripheral nerves — the ones outside the brain and spinal cord. So drugs that block it don't have the central nervous system effects of opioids: no sedation, no euphoria, no respiratory slowing.
This is the reason the Nav1.8 class has generated so much excitement. For the first time in a generation, there's a non-opioid mechanism that targets pain signaling at the peripheral level. Suzetrigine proved the concept could work — it's now approved for acute pain. VX-993 was designed to push the concept further: potentially higher potency, potentially better tolerability, potentially effective in conditions where suzetrigine has shown only mixed signals.
The Acute-Pain Trial — What Went Wrong

In August 2025, Vertex reported topline results from a Phase 2 study testing VX-993 in acute pain after bunionectomy surgery. This kind of trial — using a standardized post-surgical pain model — is a proof-of-concept test the field uses to see whether a new analgesic can show meaningful pain reduction in a controlled setting.
The result: VX-993 did not significantly outperform placebo. The drug failed to clear the bar required to advance into a larger pivotal Phase 3 trial in acute pain. Vertex announced it would not advance VX-993 in the acute pain indication.
It is important to understand what this means and what it does not mean:
- What it means: In this specific patient population (post-surgical acute pain), VX-993 did not show a clinically meaningful effect over placebo. That's a real result and it deserves to be reported honestly. Drug development is full of failures, and not every promising mechanism succeeds in every indication.
- What it does not mean: VX-993 is dead, or the Nav1.8 mechanism is invalidated. Suzetrigine succeeded in acute pain on the same mechanism — so Nav1.8 blockade clearly can work for that indication. And acute pain and chronic neuropathic pain are biologically different. A drug that fails in one can succeed in the other, because the underlying pain biology, dosing requirements, and trial design differ substantially.
Vertex chose to continue developing VX-993 specifically for painful diabetic peripheral neuropathy. That decision tells you what they believe about the chronic-pain potential — but it doesn't guarantee anything.
The Diabetic Neuropathy Trial — What's Being Tested
The Phase 2 trial in painful diabetic peripheral neuropathy is the active and most consequential study for nerve-pain patients. Some specifics, as of public information through mid-2026:
- ClinicalTrials.gov registration: NCT06619860
- Indication: Pain associated with diabetic peripheral neuropathy in adults.
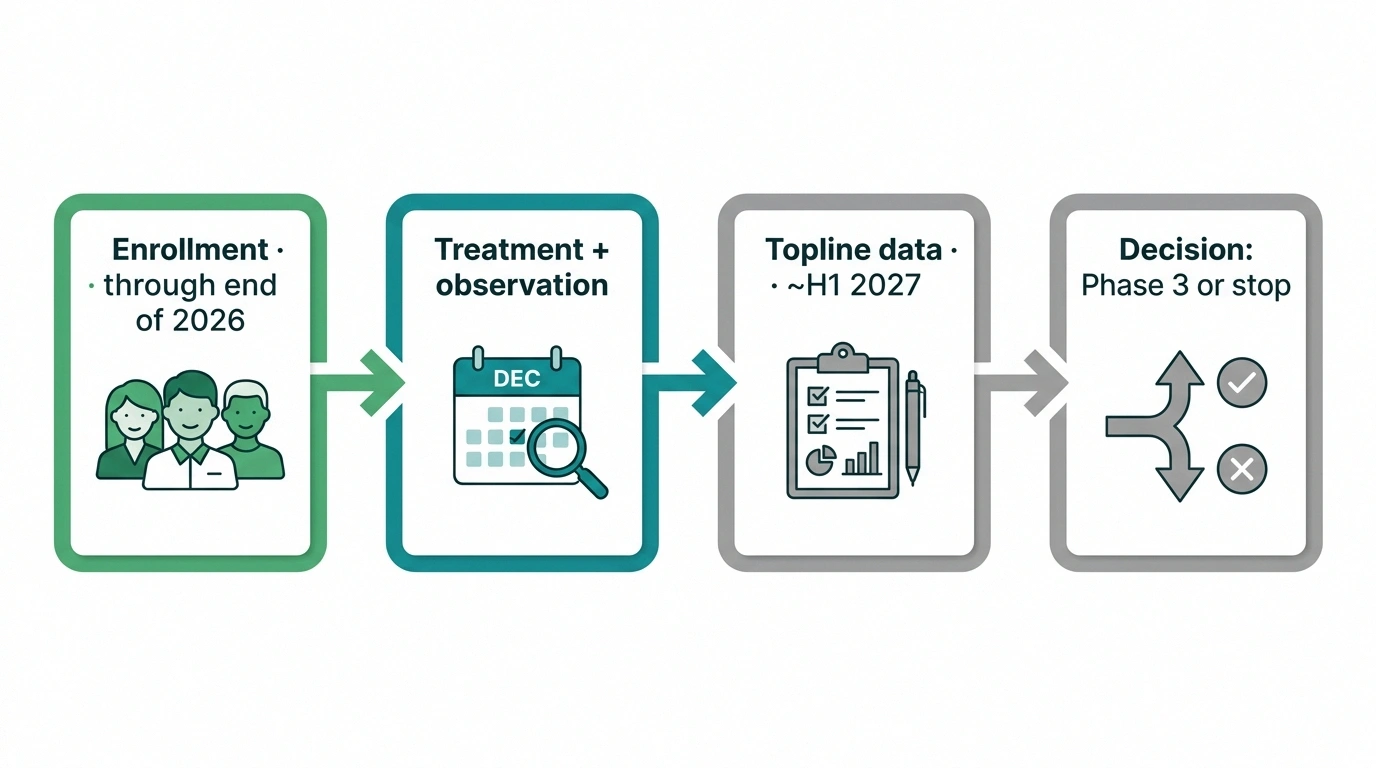
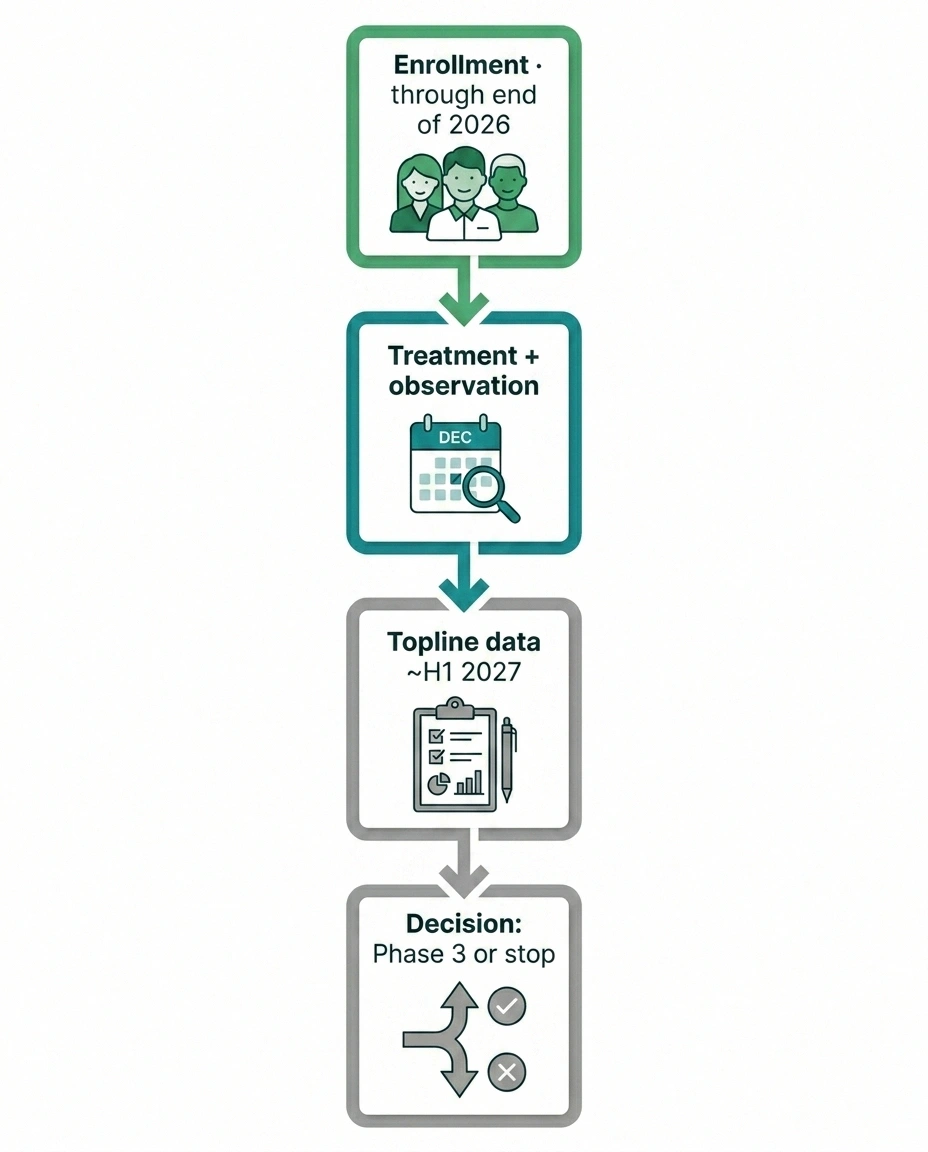
- Design: Placebo-controlled, randomized study evaluating efficacy, safety, and tolerability of VX-993.
- Enrollment status: Active; Vertex has stated enrollment is expected to complete by the end of 2026.
- Topline readout: Would follow enrollment completion — realistically in the first half of 2027.
This is the trial that matters. It will either show that VX-993 reduces chronic neuropathic pain in diabetic neuropathy — or it won't. There is no third option that gets the drug closer to approval, and no amount of speculation between now and the readout changes that.
Why This Trial Matters Beyond One Drug
VX-993 sits at an interesting strategic moment. Several things are happening at once in the Nav1.8 space:
Suzetrigine itself is in trials for chronic neuropathic pain, including diabetic neuropathy. Earlier readouts on suzetrigine in DPN have been characterized as mixed — the drug appeared to show some benefit but did not deliver a definitive signal as clean as the acute-pain results. Vertex is continuing development.
If VX-993 fails in DPN, the broader Nav1.8 approach for chronic neuropathic pain becomes harder to validate. If VX-993 succeeds, it strengthens the case that the Nav1.8 mechanism can address chronic nerve pain — and could open paths for related drugs in other neuropathies.
For patients, the practical implication is this: VX-993's DPN trial result is going to shape industry investment in this whole drug class for years. A positive result accelerates the entire field. A negative result slows it.
How VX-993 Compares to Other Diabetic Neuropathy Options

To make sense of where VX-993 might fit — if approved someday — it helps to look at what is currently available and at what else is in development.
| Drug | Mechanism | DPN Status |
|---|---|---|
| Duloxetine | SNRI | Approved |
| Pregabalin | Calcium-channel modulator | Approved |
| Gabapentin | Calcium-channel modulator | Off-label |
| Suzetrigine | Nav1.8 blocker | Trials ongoing · mixed early signals |
| Pilavapadin | AAK1 inhibitor | Phase 3 starting |
| VX-993 | Nav1.8 blocker | Phase 2 enrolling |
For approved options today, the major FDA-approved diabetic peripheral neuropathy drugs are limited to duloxetine (Cymbalta) and pregabalin (Lyrica), with gabapentin (Neurontin) widely used off-label. Tapentadol is approved but is a controlled opioid-class drug that most clinicians try to avoid.
For other investigational options in development, the picture is fuller than it's been in a long time:
- Suzetrigine (Journavx) — already approved for acute pain, in ongoing trials for chronic neuropathic pain including DPN.
- Pilavapadin (LX9211) — heading to Phase 3 for DPN, oral, works on a different target (AAK1).
- ST-503 — a one-time gene therapy targeting Nav1.7 for idiopathic small-fiber neuropathy, in Phase 1/2.
VX-993 is currently the earliest-stage candidate among the Nav1.8 group specifically for DPN. Our new neuropathy treatments 2026 article goes deeper on the wider pipeline.
Side-Effect and Safety Profile So Far
Across earlier Phase 1 and the acute-pain Phase 2 study, the side effects most commonly reported with VX-993 were generally mild to moderate. Dizziness, headache, and nausea showed up at typical rates for an oral analgesic in trial settings. Discontinuation rates due to side effects were modest.
Importantly, no opioid-like signals have been observed: no euphoria, no respiratory depression, no withdrawal pattern when patients stopped the drug. That's consistent with what the Nav1.8 mechanism would predict and is one of the central reasons this whole drug class is being pursued.
Cardiovascular signals — sometimes a concern with sodium-channel-active drugs because of structural similarities between Nav1.8 and the cardiac Nav1.5 channel — have not been flagged in trials disclosed so far. The drug class as a whole was designed for Nav1.8 selectivity.
What we don't yet know:
- Long-term safety at the doses that work for chronic neuropathic pain. Phase 2 trials of 12-week treatment can detect a lot, but a 12-week window doesn't capture issues that take 6 months or longer to emerge.
- How VX-993 will interact with the many medications people with diabetes typically take. Insulin, metformin, blood pressure drugs, cholesterol drugs, antiplatelet medications — the picture gets complicated. Drug-interaction data accumulates with bigger trials.
- Which patients respond best. As with every neuropathic-pain medication, some patients will likely get substantial benefit, some will get partial benefit, and some won't respond at all. Predicting response in advance is still mostly trial-and-error.
What This Means for You Right Now

VX-993 cannot be prescribed today. It cannot be obtained outside the clinical trial. Any product marketed online as VX-993 is not the real drug. Period.
- ✓ Tighten blood sugar control with your endocrinologist
- ✓ Confirm current medication doses are actually optimized
- ✓ Track daily pain for at least 2 weeks to establish a real baseline
- ✓ Consider Phase 2 enrollment (search ClinicalTrials.gov for NCT06619860)
- ✓ Don't bet on one drug — multiple mechanisms are in development
If you're currently managing painful diabetic neuropathy and you find yourself watching headlines about pipeline drugs, here's what I'd suggest as practical action:
- Get the basics right. Tight blood sugar control remains the single most powerful factor in slowing the progression of diabetic neuropathy. The medications people get most excited about treat the symptoms; blood sugar management addresses the cause. Our diabetic neuropathy primer and complete diabetic neuropathy treatment guide cover this thoroughly.
- Make sure you've tried current options at adequate doses. Many patients are taking duloxetine or gabapentin at doses that are too low to know whether the medication actually works for them. A real trial means an effective dose, not whatever was prescribed initially. Talk to your prescriber about titration.
- Consider a clinical trial seriously. If your DPN pain has not responded to multiple medications and a Phase 2 or Phase 3 trial of an investigational drug opens near you, enrollment is a way to potentially access investigational treatments while contributing to the data that helps everyone. Our clinical trials guide walks through how to find and join trials.
- Track your pain. A symptom diary over weeks and months is the single most useful tool you can bring to any specialist appointment. It also gives you a real baseline to compare against if you ever do try a new medication.
- Don't bet your hope on one drug. VX-993's DPN Phase 2 could succeed or fail. Pilavapadin's Phase 3 could succeed or fail. Suzetrigine's DPN trials could deliver clean results or stay mixed. The most likely future is that some of these mechanisms work, some don't, and access takes longer than anyone hopes. Hope is fine. Planning around any single one is not.
The Honest Bottom Line
VX-993 is one of several investigational drugs that, in a different timeline, could become a meaningful new option for people with painful diabetic neuropathy. Right now, it's a single Phase 2 trial in chronic nerve pain after a clear Phase 2 failure in acute pain. The next consequential data point — the DPN trial readout — is realistically the first half of 2027 at the earliest. Even a positive result would require Phase 3 trials taking 1 to 3 more years before any FDA decision.
What's encouraging is the broader landscape. After 20 years of stagnation in neuropathic pain drug development, multiple non-opioid mechanisms are being tested simultaneously. The probability that some of them succeed is higher than ever. The probability that any one specific drug — VX-993 included — makes it through is genuinely uncertain.
I'll update this article as the DPN trial milestones land. If you want the wider context, our nerve regeneration research article covers what else is being studied, and our complete neuropathy medications guide stays current on what's actually approved today.
Frequently Asked Questions
What is VX-993 and how does it work?
VX-993 is an oral, investigational, non-opioid drug being developed by Vertex Pharmaceuticals. It blocks the Nav1.8 sodium channel, which is involved in transmitting pain signals from peripheral sensory nerves toward the spinal cord. By reducing the strength and frequency of these signals, the drug aims to lower chronic pain without the central nervous system effects of opioids.
Is VX-993 approved by the FDA?
No. VX-993 is investigational and not approved. The only legal way to access it currently is through enrollment in the Vertex-sponsored Phase 2 clinical trial in diabetic peripheral neuropathy. It is not available by prescription, not available for import, and not available through any compounding pharmacy.
Did VX-993 fail a clinical trial?
Yes — in one indication. In August 2025, Vertex reported that VX-993 did not significantly outperform placebo in a Phase 2 trial in acute pain after bunionectomy surgery. Vertex stopped developing VX-993 for acute pain as a result. However, Vertex continued the separate Phase 2 trial of VX-993 in painful diabetic peripheral neuropathy, which is a different patient population with different underlying pain biology.
Is VX-993 the same as Journavx?
No. Journavx is the brand name for suzetrigine (development name VX-548), which received FDA approval in early 2025 for acute pain. VX-993 is a separate investigational drug from the same maker (Vertex), in the same drug class (Nav1.8 blockers), but it is a different molecule. Suzetrigine is the approved one. VX-993 is still in trials.
When will we know if VX-993 works for diabetic neuropathy?
Vertex has stated that enrollment in the Phase 2 diabetic neuropathy trial is expected to complete by the end of 2026. Topline results would follow enrollment completion, realistically in the first half of 2027. Even if results are positive, a Phase 3 program would be needed before any potential FDA approval, which typically takes 1 to 3 more years.
How does VX-993 compare to gabapentin or pregabalin?
Gabapentin and pregabalin work by calming overactive nerve cell excitability through a calcium-channel-related pathway. VX-993 works on a completely different target — the Nav1.8 sodium channel in peripheral sensory neurons. A different mechanism means VX-993 could potentially help people who don't respond to gabapentin or pregabalin, but until the diabetic neuropathy Phase 2 reports out, that potential remains unproven.
Will VX-993 be addictive?
Based on the mechanism and clinical data so far, no. VX-993 has not produced opioid-like effects in trials. There have been no signals of euphoria, no respiratory depression, and no withdrawal pattern when patients stop the drug. The Nav1.8 mechanism does not engage opioid receptors. Longer-term studies and real-world use would continue to confirm this profile if the drug were to be approved.
How can I find a VX-993 clinical trial?
Search ClinicalTrials.gov for the trial registration NCT06619860 or for “VX-993 diabetic neuropathy.” The site lists current trial locations, eligibility criteria, and contact information for trial coordinators. Eligibility typically requires a confirmed diabetic peripheral neuropathy diagnosis, a specified pain severity, and meeting other inclusion and exclusion criteria. Talking with your neurologist or endocrinologist about your interest is a useful first step.
