
If you or someone you love is facing chemotherapy — or already has chemotherapy-induced peripheral neuropathy (CIPN) — you've probably learned something heartbreaking: there is currently no FDA-approved treatment that prevents CIPN. We have medications that can ease the pain once nerves are damaged. We have lifestyle approaches. We have a handful of supplements with thin-but-real evidence. What we don't have is a drug given alongside chemo that says: this protects your nerves so they don't get damaged in the first place.
That gap is what an early-stage drug called SP16 is being designed to fill. It's in very early clinical trials right now, run by a small biotech called Dogwood Therapeutics and the original developer Serpin Pharma, funded by a $2.5 million grant from the National Cancer Institute. The FDA accepted its Investigational New Drug application in April 2026, and patient enrollment in the Phase 1b trial was projected to begin in mid-2026.
I want to walk through what SP16 actually is, what it's trying to do, why the prevention framing matters so much, and — being honest with you — how realistic any of this is for someone going through chemotherapy this year or next.
What CIPN Is, and Why Prevention Matters So Much
Chemotherapy-induced peripheral neuropathy is one of the most common, most disabling, and least well-treated side effects of modern cancer treatment. It's caused by chemotherapy drugs that, while killing cancer cells, also damage the long peripheral nerves that supply the hands and feet. The classes of chemo most associated with CIPN are:
- Taxanes (paclitaxel, docetaxel) — common in breast, ovarian, lung, prostate cancers
- Platinum compounds (oxaliplatin, cisplatin, carboplatin) — common in colorectal, ovarian, lung cancers
- Vinca alkaloids (vincristine, vinblastine) — common in lymphomas, leukemias
- Proteasome inhibitors (bortezomib) — common in multiple myeloma
Symptoms typically begin during treatment and can include numbness, tingling, burning pain, cold sensitivity, and weakness — usually starting in fingertips and toes and spreading inward. For many patients, the symptoms persist for months or years after chemotherapy ends. For some, they're permanent.
This isn't a minor side effect. CIPN is one of the leading causes of dose reduction and premature discontinuation of chemotherapy — meaning patients sometimes get a less-effective cancer treatment because their nerves can't tolerate the full course. It's also one of the leading complaints in long-term cancer-survivor quality-of-life surveys.
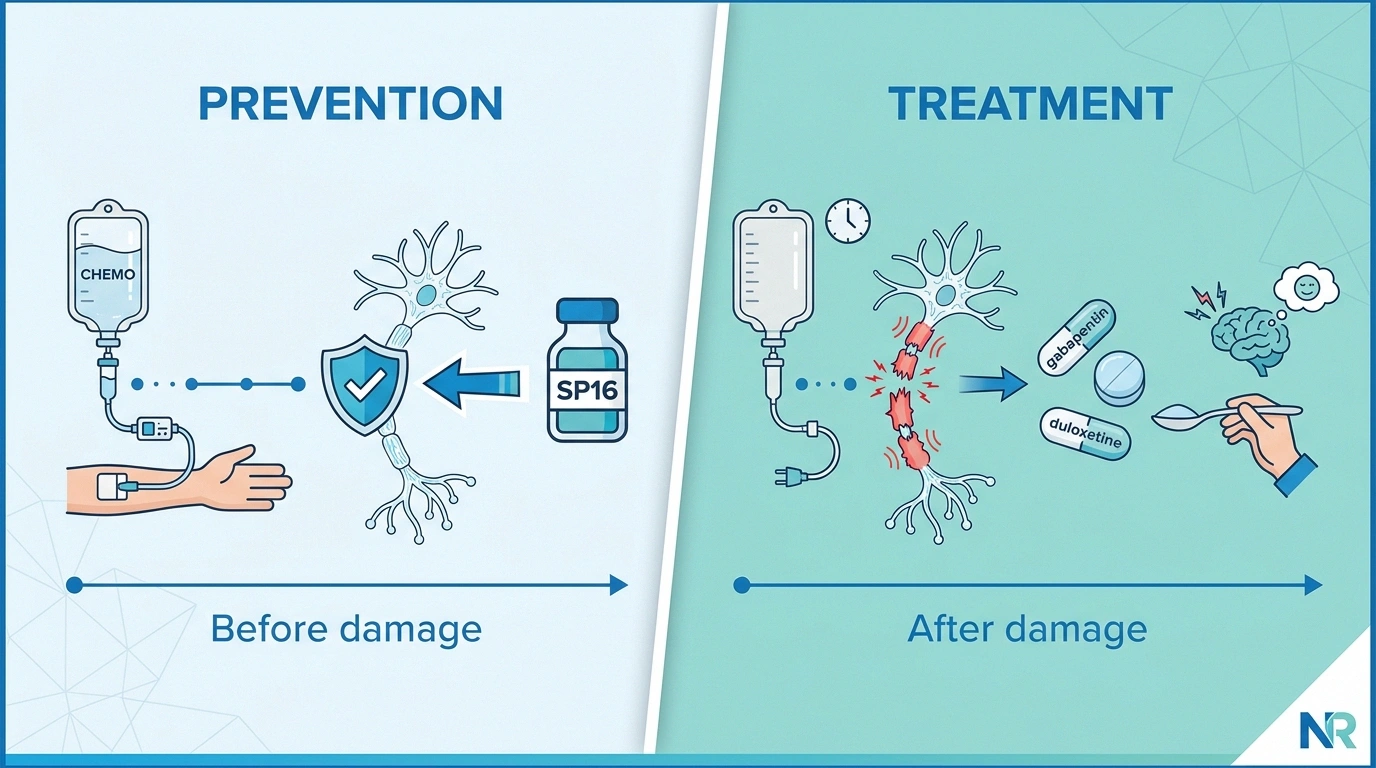
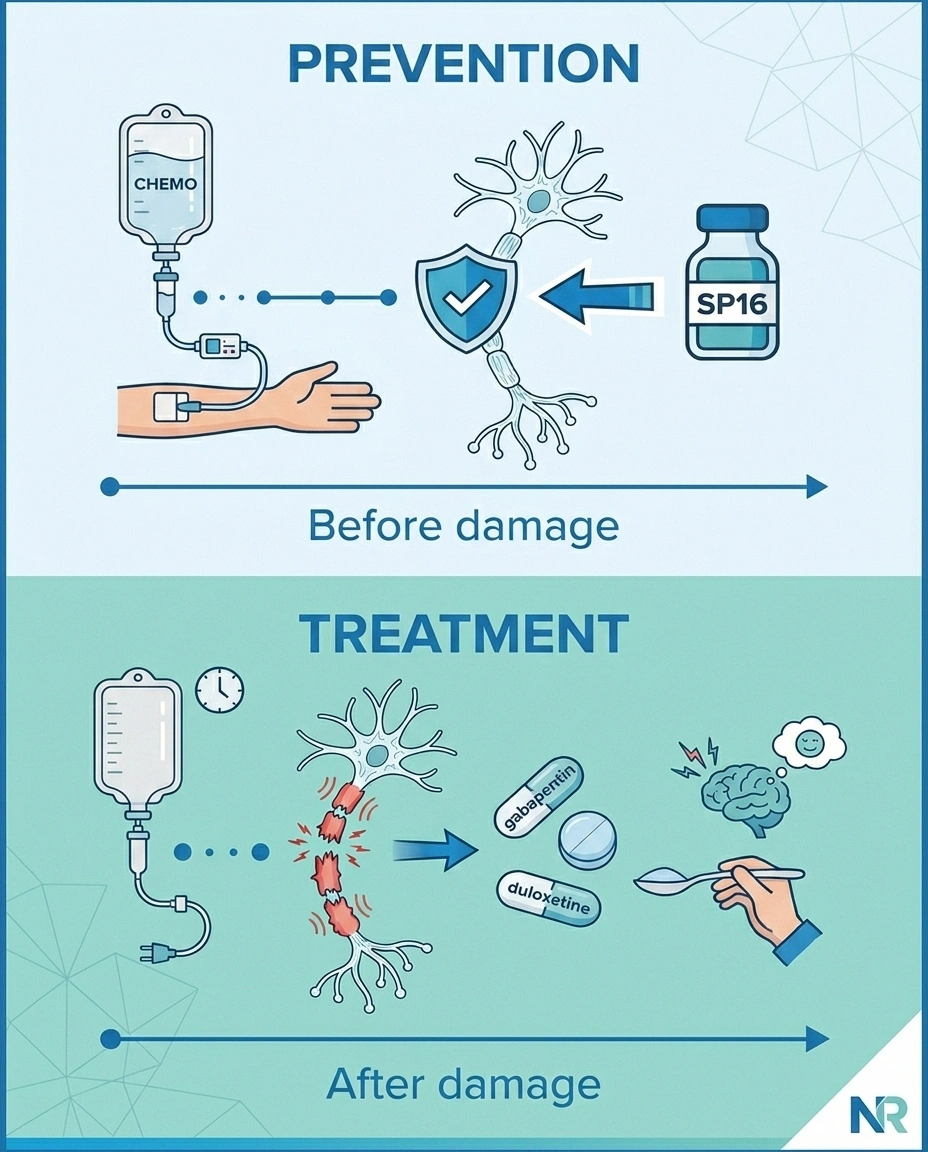
And here's the hard truth: the medications we have for CIPN — duloxetine being the only one with American Society of Clinical Oncology guideline endorsement, and even that for already-established painful CIPN — only address symptoms after nerve damage occurs. You can read more about that in our piece on chemo-induced neuropathy. None of our current tools prevents the damage.
SP16 belongs to a different category. It's a neuroprotective candidate — meaning it's being tested as a drug given alongside chemotherapy with the goal of preventing nerves from being damaged in the first place. That's a fundamentally different ambition.
What SP16 Is in Plain Language
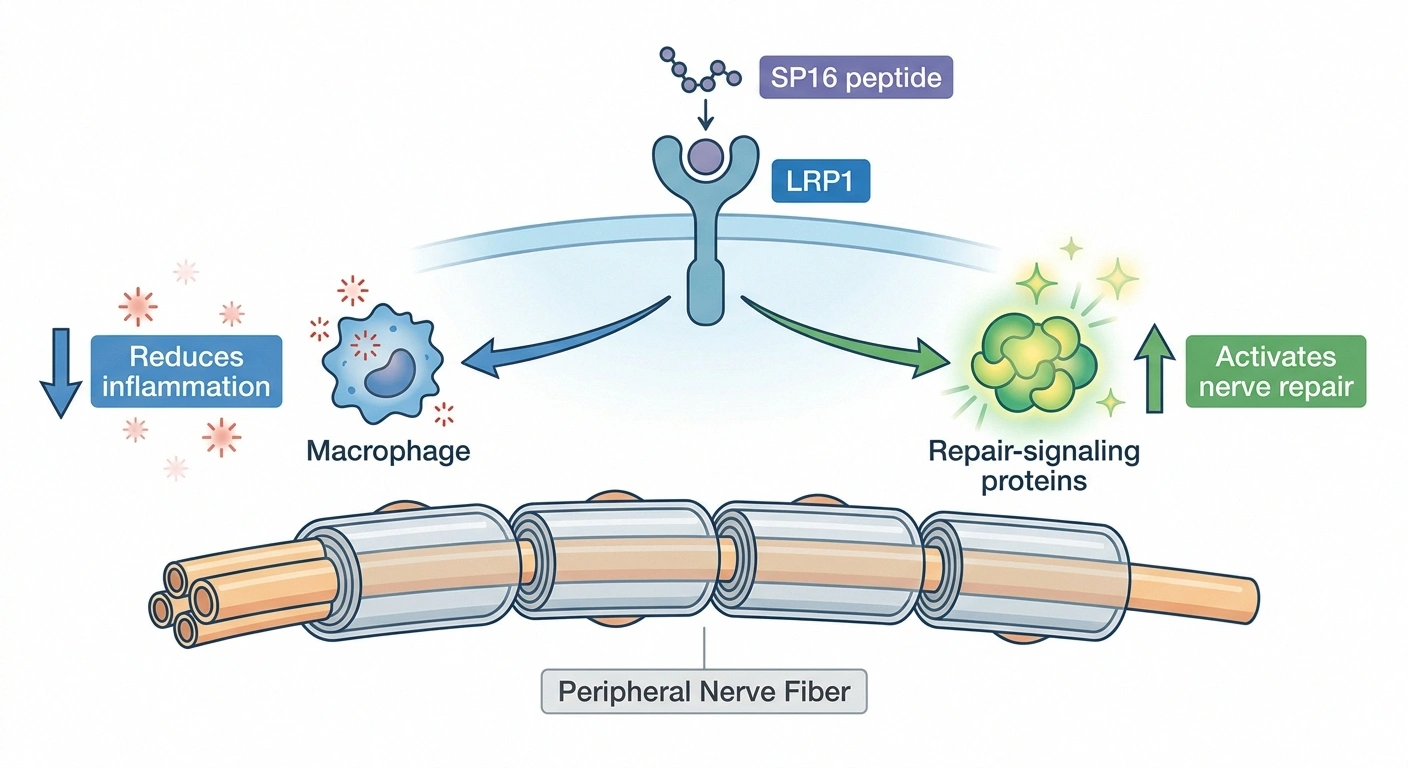
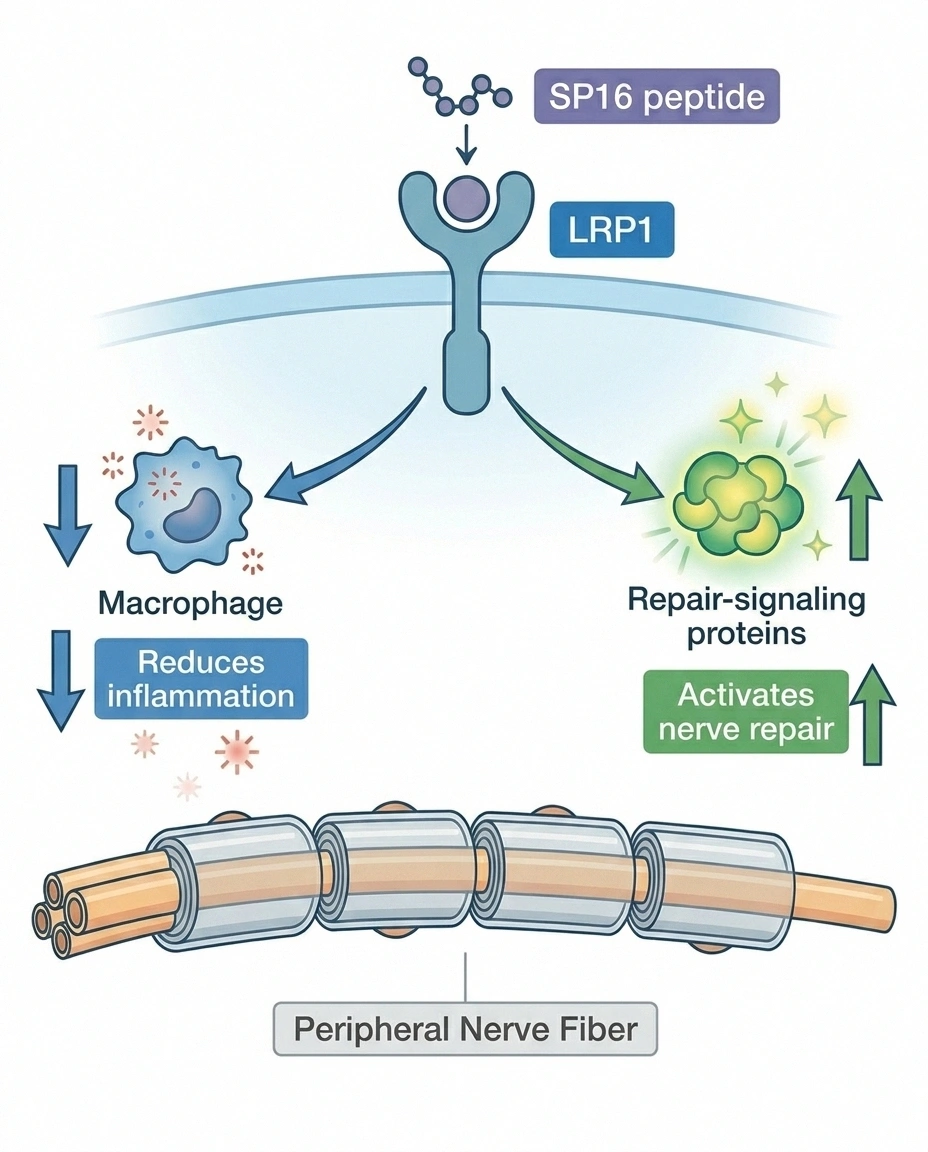
SP16 is a short peptide — a small chain of amino acids — designed to activate a receptor on cells called LRP1 (low-density lipoprotein receptor-related protein 1). It's given by intravenous (IV) infusion, the same way most chemotherapy is delivered.
Two things make SP16 interesting biologically:
- Anti-inflammatory action. When LRP1 is activated, it signals immune cells (especially macrophages — the inflammation-driving cells that flood damaged tissue) to switch from a damaging phenotype to a healing one. Less inflammation around vulnerable nerves means less collateral damage from chemo.
- Repair signaling. The same pathway activates tissue-repair signaling — encouraging surrounding cells to support and protect injured nerve fibers rather than letting damage accumulate.
If you put those together, the theoretical mechanism is: SP16 dampens the inflammatory cascade that chemotherapy triggers around peripheral nerves, while simultaneously activating cellular machinery that protects and repairs those nerves. The hope is that by infusing SP16 alongside (or before) chemotherapy, you give peripheral nerves a fighting chance to come through treatment less damaged.
Important clarification: This is a fundamentally different approach than the symptomatic neuropathy medications people are familiar with. Drugs like gabapentin, pregabalin, duloxetine, and amitriptyline don't change the underlying nerve damage — they reduce the pain signals being transmitted from already-damaged nerves. SP16 isn't competing with those drugs. It's trying to prevent you from ever needing them.
Who's Behind SP16 — the Quick Backstory
The science behind SP16 originated at Serpin Pharma, a small Virginia-based biotech that has spent years developing LRP1-targeted peptides for inflammatory and tissue-repair indications. The chemotherapy-induced neuropathy program is one of several therapeutic areas they've explored with this mechanism.
In September 2025, Dogwood Therapeutics (NASDAQ: DWTX) acquired a global, exclusive, royalty-free license from Serpin Pharma to develop and commercialize the IV formulation of SP16 specifically for cancer-related pain and CIPN. Serpin Pharma remains the holder of the IND and the regulatory sponsor of the program. The Phase 1b trial is fully funded by a $2.5 million grant from the National Cancer Institute — meaning the program isn't burning through investor capital to get the first patient dosed.
That non-dilutive NCI funding is a small but meaningful signal: it means an outside, federally funded review process concluded the mechanism was promising enough to support. It doesn't predict success, but it suggests the science isn't fringe.
The trial is being led by Dr. Patrick Dillon at the University of Virginia, an academic oncologist with a research focus on CIPN and supportive care for breast cancer patients. Initial enrollment is focused on breast cancer patients receiving chemotherapy.
The Phase 1b Trial — What It Will and Won't Tell Us
This part matters. People hear “FDA accepted the IND” or “first patient enrolled” and start hoping the drug is close. It's not — and understanding why protects you from disappointment.
Cannot show: Whether SP16 actually prevents CIPN with statistical confidence. That requires a larger Phase 2 (and ultimately Phase 3) trial. Anyone who claims Phase 1b “proved” prevention efficacy is overstating the evidence.
A Phase 1b trial in oncology supportive care has limited, specific goals:
- Safety. Does SP16 cause unexpected harm when given alongside chemotherapy? Are there interactions? Are there infusion reactions, allergic reactions, or organ-toxicity signals?
- Tolerability. Do patients tolerate the additional infusion alongside their chemo regimen? What are the side effects?
- Pharmacokinetics. How does the body process the drug — how fast is it cleared, what blood levels are achieved?
- Preliminary signal of activity. Is there any early sign that nerves are being protected? This is exploratory only — Phase 1b is not designed to prove efficacy, only to look for hints worth testing further.
What a successful Phase 1b looks like: a small group of patients (probably 10–30) safely complete the trial, the drug has a manageable side-effect profile, and there's a hint — not proof — that nerve symptoms are less severe than would be expected without SP16. That result would justify moving to a larger Phase 2 trial.
What a successful Phase 1b does NOT look like: a definitive “SP16 prevents CIPN” headline. The trial isn't statistically powered for that conclusion. Anyone who tells you Phase 1b “proved” anything about prevention efficacy is overstating the evidence.
Realistic Timeline to a Real Treatment
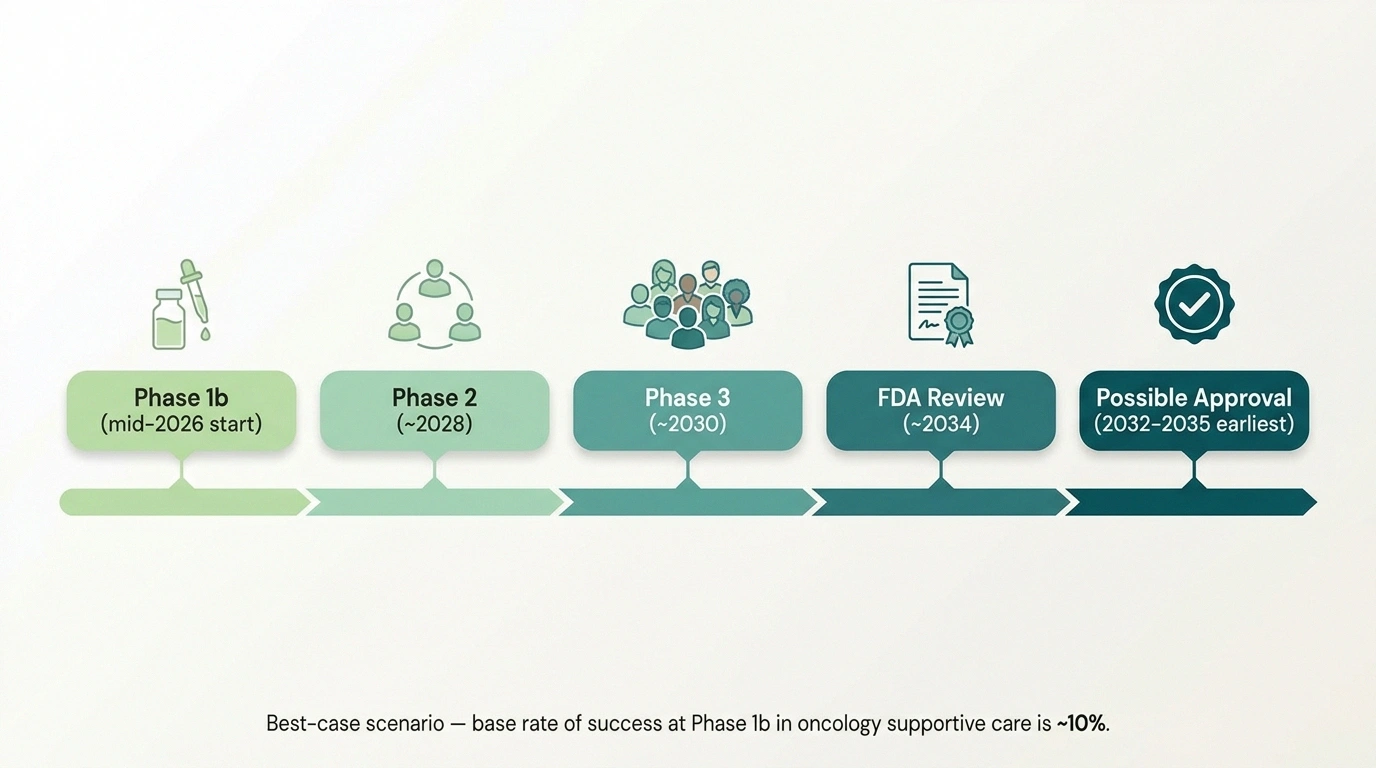
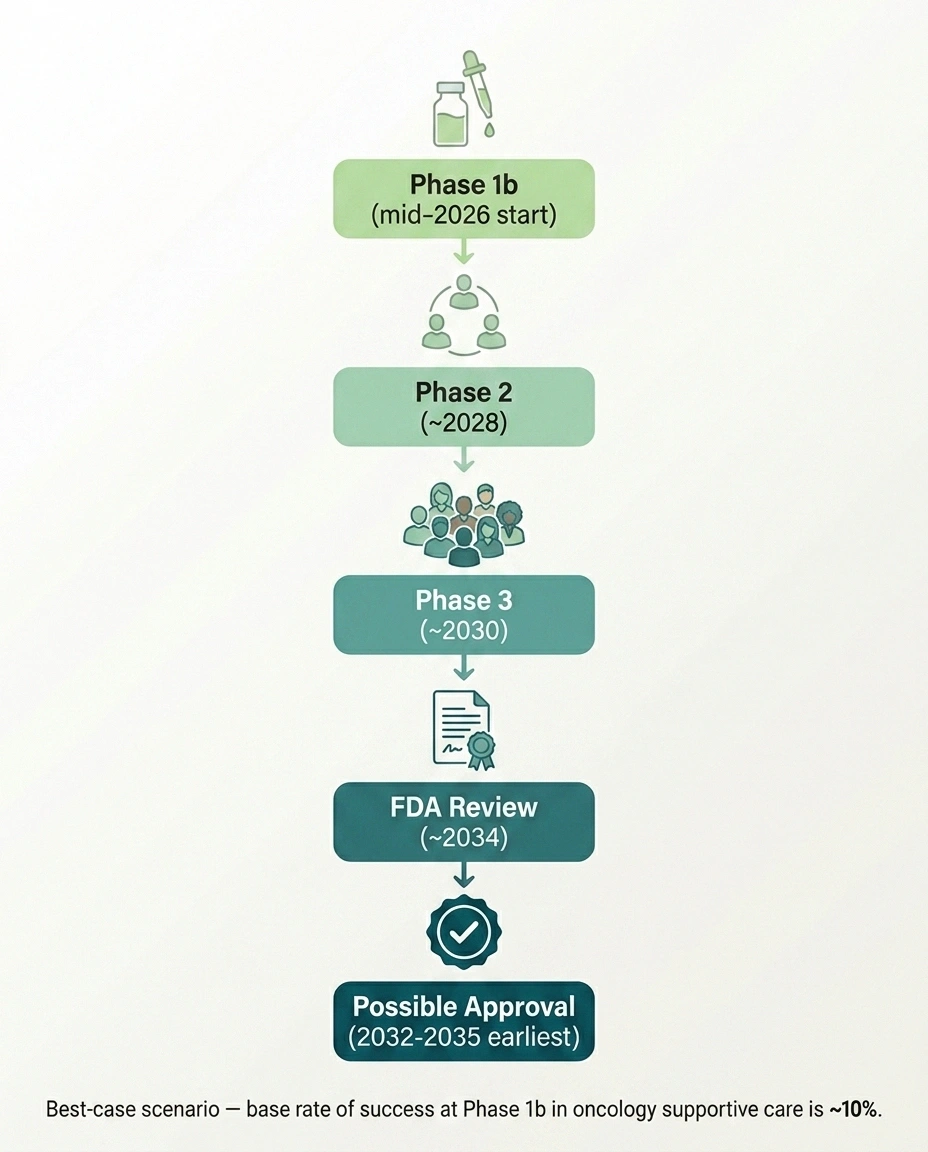
Here's the honest timeline if SP16 works as hoped at every stage — which is unusual; most drugs don't:
- Phase 1b: Patient enrollment beginning mid-2026, with results probably late 2027 or 2028.
- Phase 2: If Phase 1b is positive, a Phase 2 trial would take roughly 2–3 years to design, fund, enroll, run, and report.
- Phase 3: If Phase 2 is positive, a pivotal Phase 3 trial would take another 3–4 years.
- FDA review: 12–18 months after Phase 3 completion.
- Total best-case timeline: 6–9 years from the start of Phase 1b enrollment to FDA approval. So 2032–2035 as a realistic earliest approval window if every step succeeds.
And here's the honest base rate: of drugs that complete Phase 1b in oncology supportive care, only about 1 in 10 ultimately receive FDA approval. SP16 may well be one of them. It may not. We don't know yet.
So what should this mean for you, today, if you're facing chemo or already living with CIPN?
If you're starting chemotherapy in 2026 or 2027, SP16 will not be available to you as an approved treatment. The only way to access it is by enrolling in the Phase 1b clinical trial (at the University of Virginia initially, with possible additional sites added if expansion is approved). If you live near a trial site and meet eligibility criteria, that's a path worth discussing with your oncologist.
If you already have CIPN, SP16 is not designed to treat established damage. Its target is prevention. The current science for already-existing CIPN points to duloxetine (with guideline support) and lifestyle/symptomatic strategies, not investigational drugs in early trials.
How SP16 Fits Into the Broader CIPN Prevention Picture

SP16 is the most novel mechanism with the most recent FDA progress, but it's not the only prevention candidate being studied. Other approaches under research:
- Cryotherapy / cooling caps for extremities — wearing frozen gloves and socks during taxane infusions to reduce blood flow and chemo exposure to peripheral nerves. Some encouraging evidence but practical challenges and discomfort limit adoption.
- Compression therapy — similar mechanism (reducing chemo distribution to extremities) using tight gloves/socks during infusion.
- Exercise and sensorimotor training — supervised activity programs during chemo with modest evidence for reducing CIPN severity.
- Supplement candidates — alpha-lipoic acid, acetyl-L-carnitine, vitamin E, omega-3 fatty acids — all studied with mixed or modest results.
- Other drug candidates — including renin-angiotensin system inhibitors and antioxidant compounds being investigated in smaller trials.
The reason SP16 has generated specific excitement is the mechanism. The drugs and devices already being explored for prevention work mostly through indirect means — limiting chemo exposure to nerves, reducing oxidative stress, or generally supporting tissue health. SP16 directly engages a receptor (LRP1) with anti-inflammatory AND repair signaling — that's a more targeted intervention than anything else currently in development for CIPN prevention.
If you want a broader sense of what's coming, our roundup of new neuropathy treatments in 2026 covers the pipeline more comprehensively. And our piece on preventing CIPN — what works in 2026 covers the currently-available preventive strategies you can actually use today.
What This Means for You Right Now

If you're starting chemotherapy, here are the practical takeaways:
- Talk to your oncologist about CIPN risk and currently available prevention strategies. Cooling, compression, exercise, and supplement options should be on the table — none are magical, but the cumulative effect of using several may matter.
- Ask whether you would qualify for the SP16 Phase 1b trial if you're near a trial site (initially the University of Virginia). Even if you're not eligible, knowing about the option puts it on your oncologist's radar.
- Monitor nerve symptoms carefully throughout treatment. Catching CIPN early gives your oncology team a chance to consider dose adjustments — which can sometimes prevent symptoms from becoming permanent.
- Don't put your active life on hold waiting for SP16. The realistic timeline is years. The strategies that help right now — glycemic control if you're also diabetic, symptomatic management with first-line drugs, lifestyle protection of nerves — matter more in the meantime.
If you have established CIPN already, your treatment path is different. Duloxetine has the strongest evidence base for symptomatic relief — see our deep dive on duloxetine (Cymbalta) for neuropathy. Supplements with the most consistent supportive evidence include alpha-lipoic acid and acetyl-L-carnitine. Physical therapy and balance work can help reduce fall risk if your sensation is impaired.
Why I'm Watching This Anyway

Reading this, you might wonder: if SP16 is years from approval, why am I writing about it now? Two reasons.
First, drugs that genuinely target the prevention of chemotherapy nerve damage have been a missing category for decades. We have effective cancer treatments. We have CIPN management drugs. We don't have a tool that says “take this and your nerves won't get hit as hard.” A successful prevention drug would change cancer-treatment quality of life in ways most people don't appreciate until they live with permanent CIPN themselves. That makes early-pipeline candidates worth understanding, even if approval is far off.
Second, knowing that something serious is being developed changes how you talk to your oncology team. It tells you the field hasn't given up on prevention — even though current standard-of-care doesn't include any preventive drug. That's a meaningful piece of context to carry into your treatment decisions.
I'll keep an eye on the trial as it enrolls and publishes data. If SP16 succeeds, it'll be one of the genuinely transformative additions to cancer care this decade. If it doesn't, the LRP1 mechanism may still inform what comes next. Either way, the conversation about CIPN prevention is moving forward in a way it wasn't five years ago.
Frequently Asked Questions
What is SP16 and what is it designed to do?
SP16 is an investigational peptide drug that activates the LRP1 receptor, producing anti-inflammatory and tissue-repair signaling. It's being developed by Dogwood Therapeutics under license from Serpin Pharma. Its specific goal is to prevent chemotherapy-induced peripheral neuropathy by protecting peripheral nerves from chemotherapy damage during cancer treatment, rather than treating nerve damage after it occurs.
Is SP16 FDA-approved?
No. SP16 is investigational. The FDA accepted the Investigational New Drug application in April 2026, which permits a Phase 1b clinical trial to begin in patients. The drug is not available by prescription, not available through compounding pharmacies, and not available outside of the formal clinical trial. Approval, if it occurs, would be several years away after Phase 2 and Phase 3 trials.
Who makes SP16?
SP16 was originally developed by Serpin Pharma, a Virginia-based biotech. In September 2025, Dogwood Therapeutics (NASDAQ: DWTX) acquired a global exclusive license to develop and commercialize the IV formulation for cancer-related pain and chemotherapy-induced neuropathy. Serpin Pharma remains the holder of the IND application and the regulatory sponsor. The Phase 1b trial is funded by a $2.5 million grant from the National Cancer Institute.
How is SP16 different from gabapentin or duloxetine?
Gabapentin and duloxetine reduce pain signals from already-damaged nerves. They are symptomatic treatments. SP16 is being developed as a prevention drug — given alongside chemotherapy with the goal of stopping nerve damage from occurring in the first place. It would not replace symptomatic treatments. It is intended to be used during chemotherapy treatment for patients at risk of developing CIPN, while symptomatic drugs are used after CIPN has already developed.
Can I enroll in the SP16 trial?
The Phase 1b trial began enrollment in mid-2026 at the University of Virginia under the supervision of Dr. Patrick Dillon. Initial enrollment focuses on breast cancer patients receiving chemotherapy. To learn whether you qualify, search ClinicalTrials.gov for SP16 or chemotherapy-induced peripheral neuropathy trials, discuss with your oncologist, and contact the trial coordinator directly. Eligibility criteria typically include a confirmed cancer diagnosis, a specific chemotherapy regimen, and meeting inclusion and exclusion criteria.
When could SP16 be available as an approved treatment?
Realistically, if Phase 1b, Phase 2, and Phase 3 all succeed sequentially, FDA approval could be possible in the early 2030s — six to nine years from the start of Phase 1b enrollment. That is the best-case scenario and assumes every trial phase succeeds, which is unusual. The base rate for drugs at the Phase 1b stage in oncology supportive care reaching FDA approval is about 10 percent. Approval timing for any individual patient should not factor into current treatment decisions.
Does SP16 work for established CIPN?
No. SP16 is being developed as a prevention drug, given alongside chemotherapy to protect nerves before damage occurs. It is not designed to treat nerves that have already been damaged. If you already have CIPN, your treatment path involves symptomatic management with currently available options — duloxetine being the only treatment with American Society of Clinical Oncology guideline support for painful established CIPN.
Which chemotherapy drugs cause CIPN?
The chemotherapy classes most associated with CIPN are taxanes (paclitaxel, docetaxel), platinum compounds (oxaliplatin, cisplatin, carboplatin), vinca alkaloids (vincristine, vinblastine), and proteasome inhibitors (bortezomib). These drugs damage long peripheral nerves, producing symptoms that typically start in fingertips and toes and may persist for months or years after treatment ends. The initial SP16 trial focuses on breast cancer patients receiving chemotherapy, but the LRP1 mechanism could potentially extend to other neurotoxic regimens if early trials show promise.


