When a friend in my support group mentioned she was about to start dry needling for her neuropathy, the first thing I asked was: “Did your PT explain what it's actually going to do — and what it isn't going to do?” She paused. The answer was no. She had a vague impression it was “kind of like acupuncture” and that it might help her feet. By the time she'd done four sessions and gotten frustrated that her burning toes hadn't improved, she was about to write off something that might have genuinely helped her in a different way.
Dry needling has earned a place in physical therapy clinics across the country, and a lot of people with neuropathy end up trying it. But it's frequently misunderstood — sometimes oversold by enthusiastic practitioners, sometimes confused with acupuncture, sometimes pursued for problems it was never designed to solve. The honest story sits somewhere in the middle: dry needling is a real tool with a specific use case. For some neuropathy patients, it can help meaningfully. For others, it's the wrong tool entirely.
Let's separate what it is, what it's not, and where it fits in a neuropathy care plan.
What Dry Needling Actually Is
Dry needling is a technique developed in Western physical therapy and sports medicine. A trained practitioner inserts thin solid needles — the same filiform needles used in acupuncture — into specific spots in skeletal muscle called myofascial trigger points. These are the “knots” you can feel in a tight muscle, the tender bands that radiate pain when pressed. The goal of dry needling is to deactivate those trigger points, releasing the muscle from its locked, painful state.
Dry needling is a Western physical therapy technique that targets muscle trigger points — not nerve damage. It's a real tool with real evidence for musculoskeletal pain, but it was never designed to treat peripheral neuropathy itself.
The “dry” in dry needling refers to the fact that nothing is injected through the needle. There's no medication, no saline, no anesthetic. The needle itself is the entire treatment. Compare this to a “wet” needling technique, like a trigger point injection, where a physician injects lidocaine, saline, or sometimes a corticosteroid into the same kind of spots. Same target, different method.
The history is relatively young. The modern technique was developed in the 1970s and 80s, largely by physicians like Janet Travell and physical therapists like Karel Lewit, who were building on observations about trigger point science. It was originally framed as a Western, anatomically grounded alternative to acupuncture — a way to get the muscle-relaxing benefits of needling without the traditional Chinese medicine framework. Whether that framing has held up is part of the story we'll get to.
In the United States, dry needling is most commonly performed by physical therapists, with some chiropractors and athletic trainers also offering it depending on state regulations. The certification process is much shorter than acupuncture training — typically a 50-100 hour weekend course series — and the regulatory framework varies by state. Some states explicitly permit PTs to dry needle; others require additional licensure or outright prohibit it.
How Dry Needling Differs from Acupuncture
This is the first question almost everyone asks, so let's answer it head-on. The needles are similar. The insertion technique looks similar from the table. But the theory, the targets, and the training are different.
(usually a PT or chiropractor)
(plus state licensure + national exam)
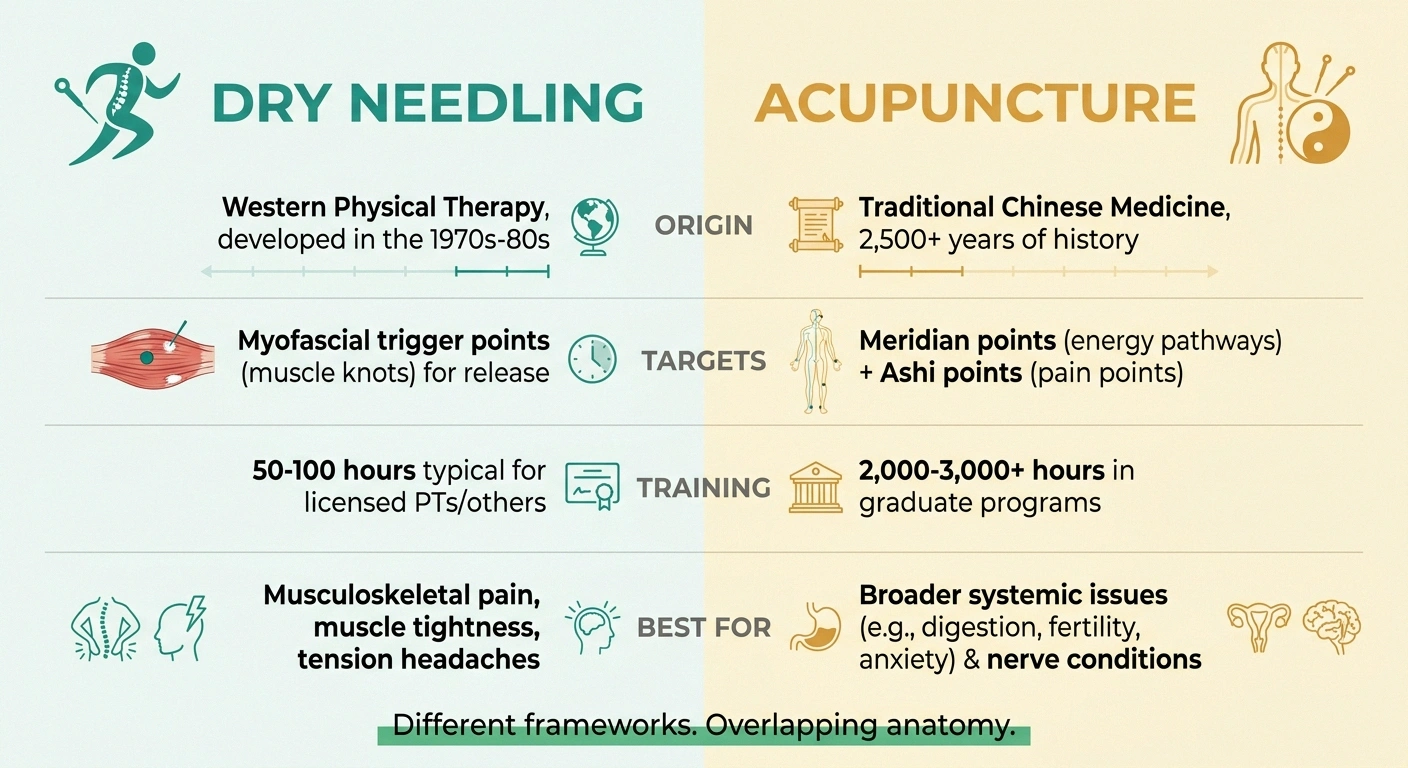
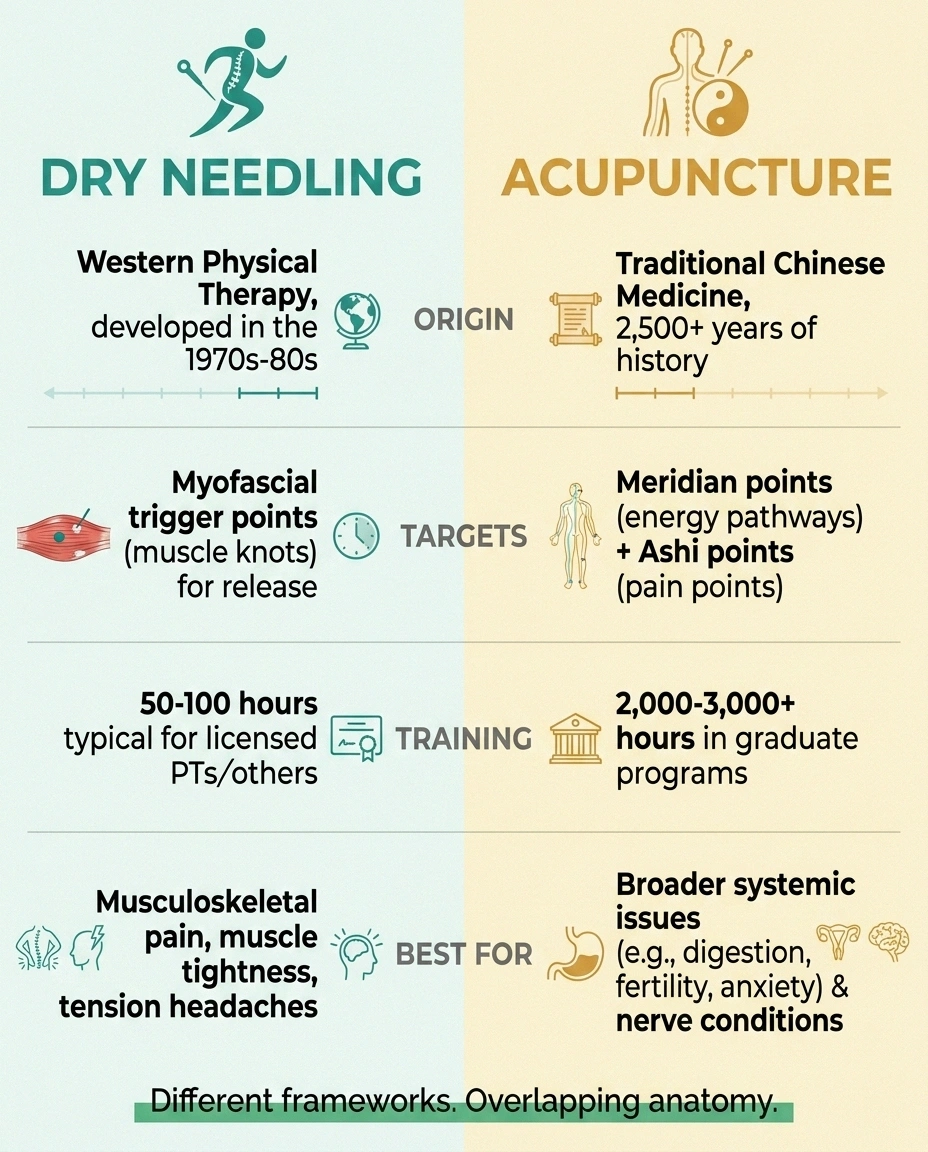
Acupuncture comes from traditional Chinese medicine, with a documented history stretching back more than 2,500 years. It targets specific points along what TCM describes as meridians — energetic pathways that connect organs and systems. There are roughly 365 classical points plus several thousand “extra” points. The goal is to restore balance to the flow of qi (vital energy). A licensed acupuncturist in the United States typically completes 2,000 to 3,000 hours of training and passes a national certification exam to become licensed.
Dry needling targets trigger points — specific palpable spots within skeletal muscle that produce a characteristic pattern of pain. The theoretical basis is muscle physiology and neuromuscular dysfunction, not energy meridians. The training is shorter and the framework is explicitly Western.
Here's the wrinkle that academics have been pointing out for years: traditional Chinese medicine has always recognized something called Ashi points — literally “ouch points” — which are tender spots that don't correspond to the standard meridian map. Acupuncturists have been needling Ashi points for centuries, and Ashi points look an awful lot like trigger points. So the two techniques may be operating on overlapping, sometimes identical, anatomical territory while explaining what they're doing in completely different languages.
What does this mean practically? If you're choosing between an experienced licensed acupuncturist and a recently certified PT doing dry needling, the bigger difference is often the depth of training in needling itself, not the philosophical framework. Acupuncture for neuropathy has been more thoroughly studied in published clinical trials, especially for chemotherapy-induced and diabetic neuropathy. Dry needling has its own evidence base, but it leans more toward musculoskeletal conditions than nerve conditions.
What Dry Needling Was Designed to Treat
This is where understanding the tool matters. Dry needling was developed to treat myofascial pain — pain coming from muscle dysfunction. Tight muscles. Restricted muscles. Trigger points that radiate pain in characteristic patterns away from the muscle itself. The clinical evidence is strongest for:

- Chronic neck and shoulder pain from muscle tension
- Mechanical low back pain (when muscle origin is the issue)
- Tension-type headaches with muscular trigger points
- Plantar fasciitis
- Tennis elbow and other tendon-related conditions
- Sports injuries with muscle component
Notice what's not on that list: nerve damage. Dry needling was not designed to treat peripheral neuropathy. The underlying nerve pathology — the destruction of small nerve fibers in your skin, the damage to longer axons heading to your feet — isn't a muscle problem. Needling muscles will not regrow nerves, repair myelin, or undo the damage caused by years of high blood sugar or chemotherapy. Anyone telling you otherwise is overpromising.
Where Dry Needling Might Actually Help a Neuropathy Patient
This is the part that gets missed in most clinic conversations. People with chronic neuropathy often develop a layer of secondary muscle pain on top of their nerve pain — and that secondary layer is exactly what dry needling is designed for.
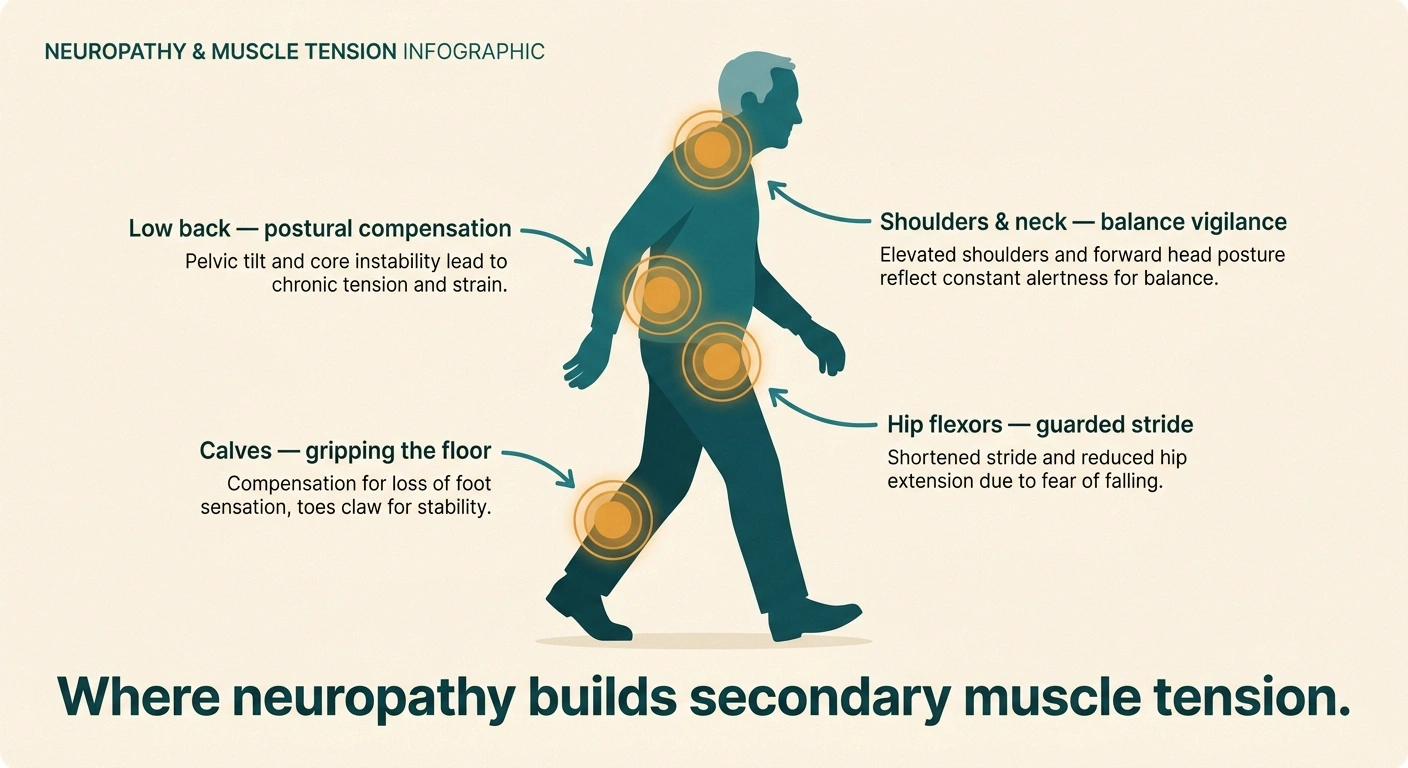
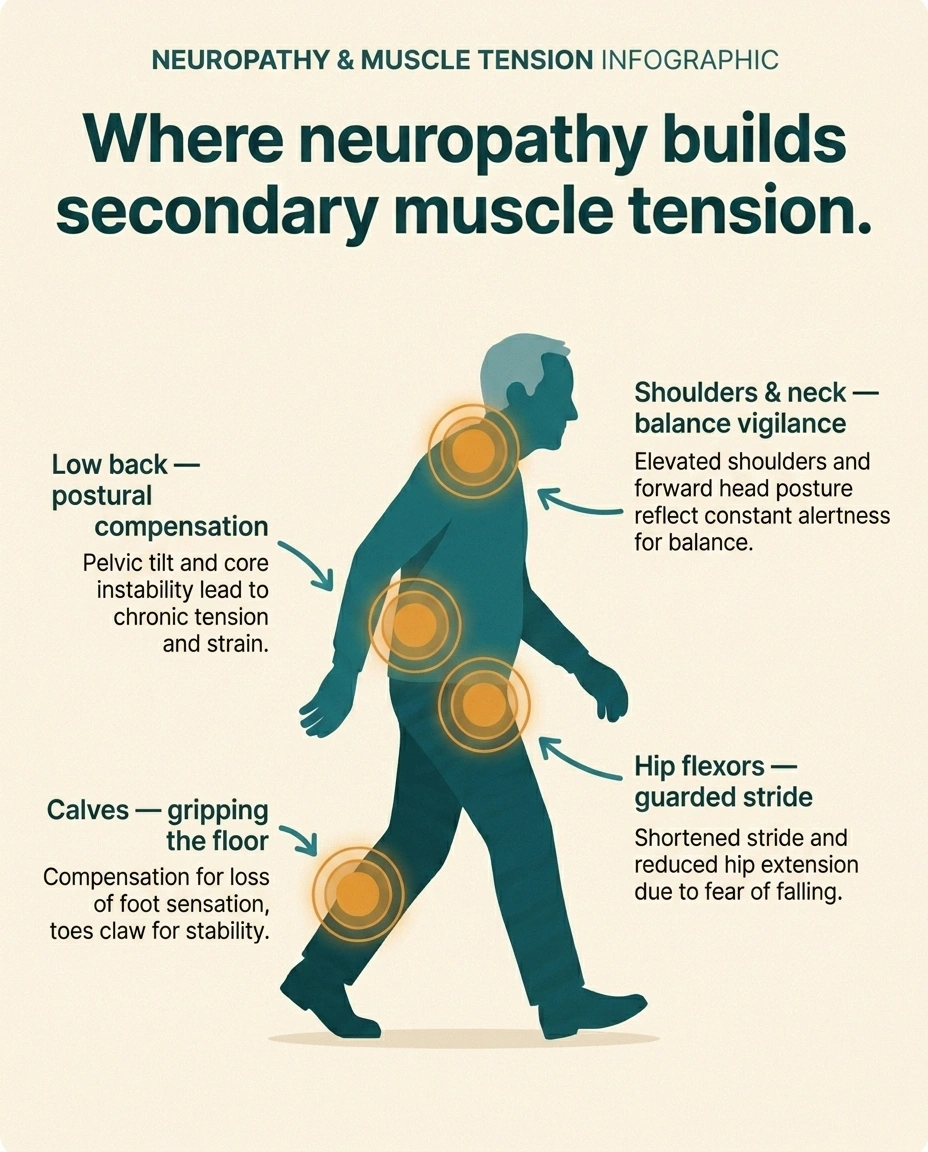
Think about how neuropathy changes how you move. If your feet hurt and feel unstable, you walk differently. You shorten your stride. You grip the floor with your toes. You shift your weight toward whichever side feels more reliable. Over months and years, those subtle compensations build up. Your calf muscles get chronically tight from gripping. Your hip flexors shorten from a guarded walking pattern. Your low back tightens from carrying tension you've never released. Your shoulders ride up from balance vigilance.
These compensatory muscle patterns can generate their own pain — real, often significant pain that has nothing to do with the underlying nerve damage. It's musculoskeletal pain layered on top of neuropathic pain, and it responds to musculoskeletal treatment.
This is where dry needling can have a meaningful place. A trained PT can identify the chronic muscle tension patterns you've built up, target the trigger points with needling, and often release tension that's been there for years. The relief doesn't extend to the nerve symptoms — your toes will still tingle when the session ends — but the compensatory pain layer often improves significantly. For some patients, that improvement in the muscular pain layer makes a substantial difference in how they feel overall.
There's a second potential use case: nerve entrapment patterns. If a tight muscle is compressing a nerve as it passes through — piriformis syndrome compressing the sciatic nerve, tight scalenes compressing the brachial plexus, tight forearm flexors aggravating hand symptoms — releasing the muscle can take pressure off the nerve. This isn't treating the neuropathy itself; it's reducing a secondary entrapment that's making things worse.
What the Evidence Actually Says
I want to be honest about the research because the marketing around dry needling sometimes outruns what the trials have actually shown.
Systematic reviews show dry needling provides a modest, real benefit over sham needling for trigger-point musculoskeletal pain — roughly similar to acupuncture in head-to-head comparisons. High-quality randomized trials of dry needling specifically for peripheral neuropathy are essentially absent. The technique helps the muscle layer that often sits on top of neuropathy, not the nerve damage underneath.
For myofascial trigger point pain, the systematic reviews are mixed. Some studies show dry needling outperforms sham (fake) needling, but the difference is often modest. The most rigorous reviews tend to conclude that there's a real effect, but it's smaller than enthusiastic clinic websites would have you believe, and it's roughly similar to the effect of acupuncture for the same conditions. Direct comparison between dry needling and trigger point injection (the “wet” version) generally shows no meaningful advantage to either approach — the needle itself appears to do most of the work.
For peripheral neuropathy specifically, the high-quality clinical trial evidence for dry needling is essentially absent. The technique simply wasn't designed for nerve conditions, and the studies haven't been done. What evidence exists comes mostly from case reports, small uncontrolled series, and extrapolation from the musculoskeletal evidence. That's not nothing — practitioners do treat neuropathy patients with reasonable results, especially for the secondary muscle pain — but it's also not the same as a high-quality randomized controlled trial showing benefit.
If someone tells you dry needling is “proven to treat neuropathy,” they're going beyond the published evidence. The fair statement is: dry needling has reasonable evidence for some musculoskeletal problems that frequently accompany neuropathy, and it can help that layer of the pain experience. That's a real benefit. It's just not a nerve treatment.
What a Session Is Actually Like
If you've never had dry needling, here's roughly what to expect. The practitioner — usually a physical therapist — will do a hands-on assessment first, palpating the muscles in the area you're treating to find the trigger points. They'll mark the spots, then clean the skin with alcohol. The needles are thin, sterile, single-use, and pulled from a sealed package right in front of you.

Insertion itself is usually painless or close to it. The needles are much finer than the ones used for injections or blood draws. What you may feel is a brief, localized “twitch” when the needle hits a trigger point — your muscle contracts involuntarily for a fraction of a second. That twitch is actually the goal. Practitioners describe it as the marker that the trigger point has been engaged. It can feel like a brief deep ache, a cramping sensation, or sometimes a sharp pinprick. Most people find it tolerable; some find it uncomfortable but brief.
A typical session involves anywhere from 4 to 15 needles, left in place for a few minutes (or briefly inserted and withdrawn, depending on the practitioner's protocol). Sessions usually last 30 to 45 minutes including assessment. Most patients are advised to drink water afterward, expect some soreness for 24 to 72 hours that feels like a hard workout, and to plan around that — don't schedule a session the day before a wedding.
A full course of treatment usually runs 6 to 12 sessions, often weekly, sometimes paired with traditional PT exercises in the same visit. Cost varies widely. Insurance coverage is inconsistent — some commercial plans cover it as part of PT, some don't. Out-of-pocket pricing typically runs $50 to $150 per session in the United States. Acupuncture coverage through Medicare and many private plans is sometimes actually broader for certain diagnoses, including chronic low back pain.
Side Effects, Risks, and Who Should Be Careful
Dry needling is generally safe when performed by a trained practitioner with single-use sterile needles, but it's not risk-free. The common side effects to expect:
- You take blood thinners (warfarin, apixaban, rivaroxaban, dabigatran, daily aspirin)
- You have lymphedema in the limb being treated
- You have an open wound, infection, or skin condition at the site
- You're pregnant (some practitioners avoid certain points)
- You're significantly immunocompromised
- You have significant sensory loss — you can't feel warning signals normally, so the practitioner must adjust
- Soreness at the needling site for 24-72 hours (most common)
- Mild bruising
- Brief fatigue after the session
- Occasional lightheadedness or vasovagal response — about 1-3% of patients
The serious but rare risks:
- Pneumothorax — a partially collapsed lung — is a documented risk when needling muscles of the upper chest, upper back, or shoulder region. It's uncommon but reported. Make sure your practitioner is properly trained for chest-region needling, and report any sudden shortness of breath or chest pain after a session.
- Bleeding is more of a concern if you're taking blood thinners. Tell your PT if you take warfarin, apixaban, rivaroxaban, dabigatran, or even daily aspirin. Dry needling is generally not contraindicated on blood thinners, but the practitioner may use different sites or be more cautious.
- Infection is extremely rare with sterile single-use needles. If your practitioner is reusing needles, walk out.
- Nerve injury can happen if a needle hits a nerve directly. The risk is low with trained practitioners, but it's why anatomy training matters.
There's one consideration that's specific to neuropathy patients and gets overlooked: if you have significant sensory loss in the area being needled, you may not feel pain or pressure that would normally tell you something is wrong. The practitioner can't rely on your feedback in the same way. Make sure your PT understands the extent of your sensory loss and adjusts their approach. For severe foot neuropathy, needling in the feet themselves carries higher risk than needling proximal muscles like the calf.
Situations to discuss with your provider before starting:
- Active anticoagulation or significant bleeding disorder
- Lymphedema in the limb being treated
- Active local infection or open wounds
- Pregnancy (some practitioners avoid certain points)
- Significant immunocompromise (organ transplant, chemotherapy)
- Severe needle phobia (it doesn't help anyone if you're white-knuckling the table)
- Skin conditions in the area being treated
Realistic Expectations
Here's the conversation I wish my friend had had before she started:
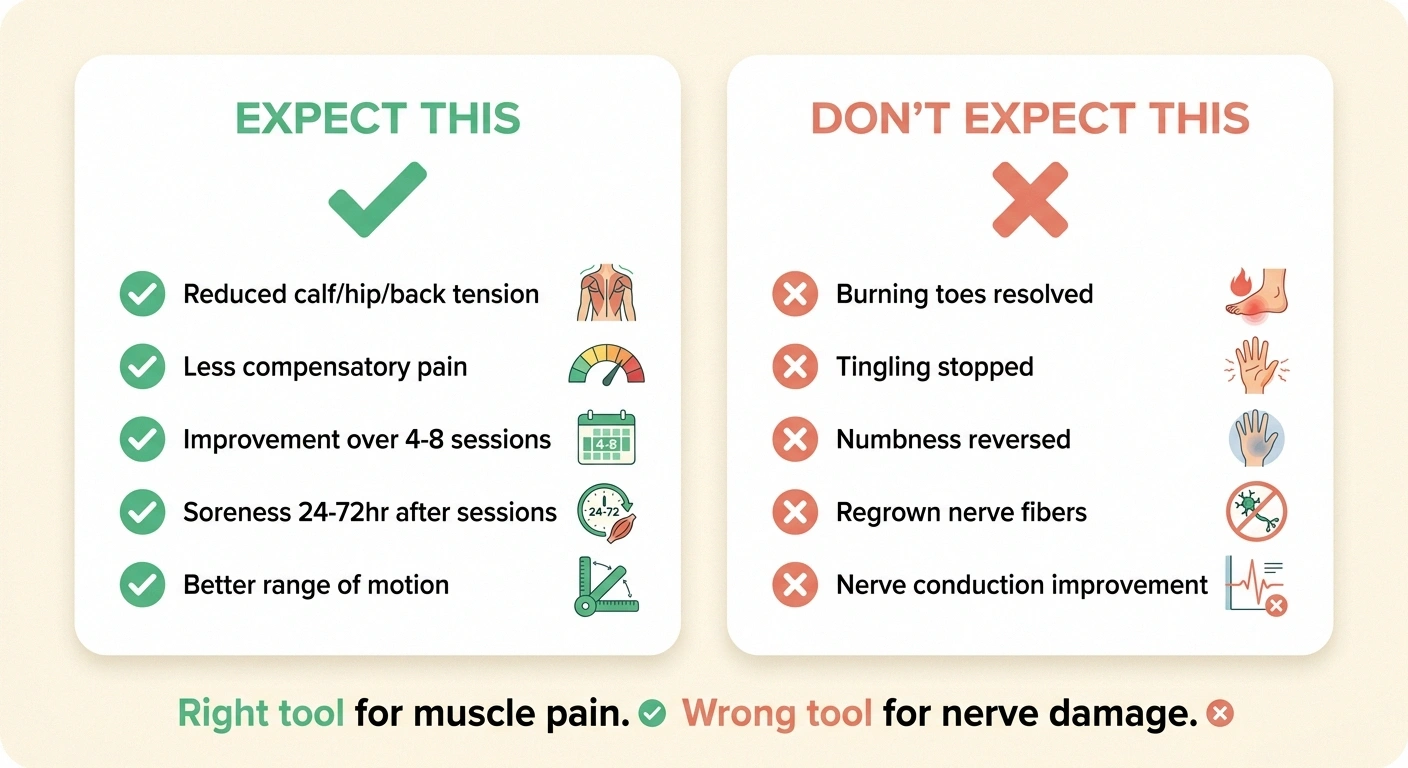
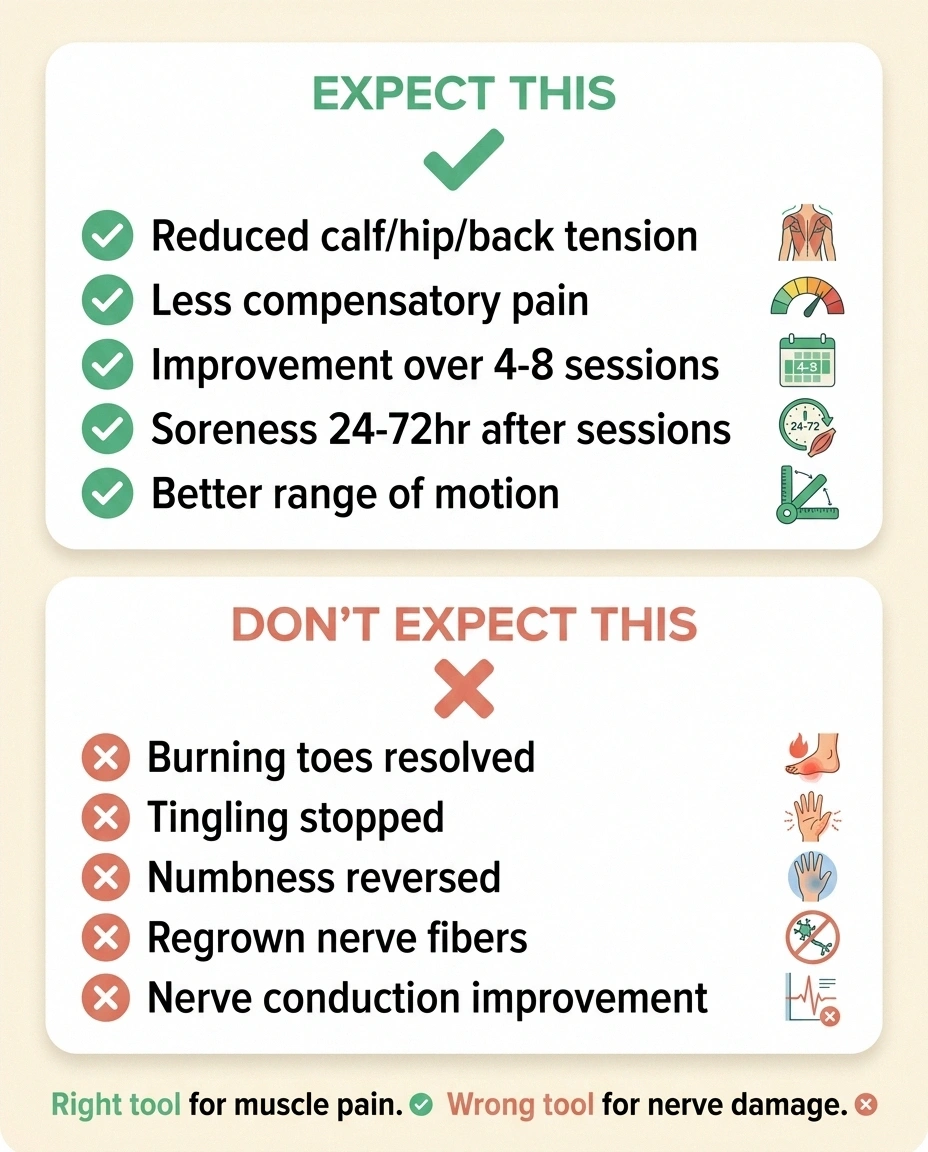
- Dry needling will most likely not change the burning, tingling, numbness, or electric-shock sensations of your actual neuropathy. Don't expect that.
- Dry needling may meaningfully reduce the secondary muscle pain you've built up from compensating — tight calves, locked-up hips, tense shoulders, tension headaches. Expect that.
- The first session often produces only mild improvement. Real benefit usually shows up over 4-8 sessions if it's going to.
- If you don't see any improvement in your muscular complaints by session 6, it's reasonable to stop. Continuing past that point with no progress is throwing money at the wrong tool.
- Soreness afterward is expected, not a sign something is wrong.
- Dry needling pairs well with regular physical therapy exercises. The needling releases the muscle, the exercises keep it released. Without the second part, the muscles often re-tighten.
Choosing a Practitioner
Not every PT who offers dry needling has the same training, and the difference matters. Questions to ask before booking:
- What's your dry needling certification, and how many hours of training did it involve?
- How many years have you been practicing dry needling?
- Have you treated patients with peripheral neuropathy before?
- Do you needle the affected limb directly, or focus on proximal muscles?
- What's your protocol for patients on blood thinners?
- How will you adjust if I have significant sensory loss in the area?
You're not being difficult by asking. A confident, well-trained practitioner will welcome the questions and have specific answers. If the answers are vague, that tells you something.
How It Fits in a Neuropathy Plan
If I were sketching out where dry needling sits in a thoughtful neuropathy care plan, it would look something like this. The core of the plan is still the things that address the underlying problem: blood sugar control or treatment of whatever's causing the neuropathy, prescription medications appropriate to your case (gabapentinoids, SNRIs, tricyclics, sometimes topicals), evidence-backed supplements where appropriate, and the lifestyle structure — exercise, sleep, footwear, balance work, natural remedies for the milder days.

Dry needling earns its place when there's a meaningful musculoskeletal tension layer sitting on top of the neuropathy — tight calves, locked hips, balance-vigilant shoulders. For pure length-dependent diabetic neuropathy without that secondary layer, acupuncture has more direct nerve-pain evidence. Match the tool to the job.
Around that core sit modalities that target specific layers of the experience. TENS units for the nerve-pain layer through gate-control mechanisms. Foot massage for circulation and the touch-comfort layer. Compression for swelling and certain symptom patterns. And dry needling — when there's a meaningful muscle-tension layer on top of the neuropathy — for that specific piece.
The patients I've seen benefit most from dry needling were the ones whose neuropathy had developed clear compensatory patterns: the foot-pain patient with calves of stone, the hand-symptom patient with neck and shoulder tension she didn't know she was carrying, the gait-altered patient whose hip flexors had locked up. Releasing those layers didn't fix their neuropathy, but it took a chunk of pain out of their day, and that chunk mattered.
For the patient with classic length-dependent diabetic neuropathy and no significant musculoskeletal component? Dry needling probably isn't the right place to spend money or sessions. Traditional acupuncture, with its broader systemic approach and more relevant clinical trial evidence in neuropathic conditions, may be a better fit if you want to try needling for the nerve symptoms themselves.
Tools have right uses. Dry needling is a real tool. Using it for the job it was designed for is how it earns its place. Asking it to do something it wasn't built for — like undoing nerve damage — is how good treatments get blamed for not working.
Frequently Asked Questions
Does dry needling actually help neuropathy?
Dry needling does not directly treat the nerve damage underlying peripheral neuropathy. It can meaningfully help the secondary muscle tension and trigger-point pain that often builds up in neuropathy patients from years of compensatory walking and posture changes. For patients with significant musculoskeletal pain layered on top of their nerve symptoms, dry needling targeting calves, hips, neck, or shoulders can reduce that musculoskeletal layer. The burning, tingling, or numbness of the actual neuropathy will not improve. Set your expectations accordingly.
What's the difference between dry needling and acupuncture?
Dry needling uses the same kind of thin solid needles as acupuncture but is based on Western muscle physiology — specifically the targeting of myofascial trigger points to release tight muscles. Acupuncture comes from traditional Chinese medicine with a 2,500-year history, targets points along energetic meridians, and has a much broader treatment philosophy. Acupuncturists complete 2,000-3,000+ hours of training; physical therapists doing dry needling typically complete 50-100 hours. The techniques overlap anatomically (acupuncture's Ashi points are essentially trigger points), but the frameworks and training depths differ substantially.
Is dry needling more scientific than acupuncture?
Both modalities have research bases, but the picture is more nuanced than the “Western equals scientific” framing suggests. Dry needling has more research in musculoskeletal conditions. Acupuncture has more research in nerve-related conditions, including chemotherapy-induced and diabetic peripheral neuropathy, where the clinical trial evidence is actually stronger for acupuncture than for dry needling. For pure muscle pain, dry needling has the edge in studied conditions. For nerve pain or whole-body conditions, acupuncture has more direct research. Neither has miracle-level evidence.
How many dry needling sessions until it works?
Most practitioners expect to see some improvement within 4 sessions if the technique is going to help, with a typical course running 6 to 12 sessions, often weekly. The first session usually produces only mild relief and significant soreness afterward. By sessions 4 to 6, patients who are responding to dry needling often report meaningful improvement in the muscle tension component of their pain. If you have not seen improvement by session 6, continuing usually does not change the outcome — it's reasonable to stop and try a different approach.
Does dry needling hurt?
Insertion of the thin needles is usually painless or close to it — much less than an injection or blood draw. The distinct sensation comes when the needle reaches a trigger point and elicits what is called a local twitch response, which can feel like a brief deep ache or cramping sensation for a fraction of a second. Most patients describe it as uncomfortable but tolerable. After the session, soreness in the treated muscles is normal for 24 to 72 hours and feels like the soreness from a hard workout. Bruising can also occur.
Is dry needling safe if I take blood thinners?
Dry needling is not absolutely contraindicated on anticoagulants like warfarin, apixaban, rivaroxaban, or dabigatran, but it requires more caution. You should always tell your practitioner what blood thinners you take, including daily aspirin. Bruising is more likely and may be larger. Most experienced practitioners will adjust their approach by needling fewer sites, choosing less vascular target areas, or avoiding certain anatomical regions altogether. If your INR is unstable on warfarin or you have a known bleeding disorder, defer the conversation to your prescriber before scheduling.
Does insurance cover dry needling?
Insurance coverage for dry needling is inconsistent and varies by state, plan, and the credential of the provider performing it. Some commercial insurance plans cover it as part of a physical therapy visit; many do not. Medicare typically does not cover dry needling specifically, though it covers physical therapy visits and acupuncture for certain diagnoses like chronic low back pain. Out-of-pocket costs typically run $50 to $150 per session. Always verify coverage with your specific plan before starting, and ask the clinic for the exact billing code they will submit so you can confirm.
Can dry needling cause nerve damage?
Nerve injury from dry needling is rare in the hands of properly trained practitioners but is documented. The risk depends on the anatomical region being needled and the practitioner's training in surface and deep anatomy. Areas near major peripheral nerves require careful technique. Patients with existing peripheral neuropathy do not appear to be at higher risk of needle-induced nerve damage, but the sensory loss from their condition may mask warning sensations that would normally protect them. Choose a practitioner with substantial training and experience, and disclose all your conditions during the assessment.