The first time someone in my support group told me she'd booked a Qutenza appointment, I had to ask her to repeat the name. I'd seen the over-the-counter capsaicin creams at the drugstore — the ones derived from hot peppers that you rub on twice a day. I hadn't realized those creams had a high-octane prescription cousin: a single patch, applied once in a doctor's office, that could quiet nerve pain for up to three months.
Qutenza isn't a daily medication. It isn't a pill you take. It's a one-time, in-office procedure — a thirty-minute patch application that resets nerve activity for weeks at a time. For the right patient, it's one of the most interesting tools in the modern neuropathy toolkit. For the wrong patient, it's expensive, uncomfortable, and probably not the right answer.
I want to walk you through it honestly today — what it is, how it works, what an appointment is actually like, what it costs, where it's been FDA-approved, where it hasn't, and what the response rates look like in real patients. By the end, you should have enough information to decide whether to ask your doctor for a referral.
What Qutenza Is, In Plain Language
Qutenza is a roughly 5.5-by-7.9-inch (14-by-20-centimeter) patch that delivers a single, large dose of 8 percent capsaicin directly into the skin over a 30-minute application. To put that concentration in perspective: the over-the-counter capsaicin creams you can buy at any drugstore typically contain between 0.025 and 0.075 percent capsaicin. Qutenza is roughly 100 to 300 times more concentrated. That's why it cannot be used at home and why it's classified as a prescription medical procedure.
One patch contains 179 milligrams of capsaicin. The active ingredient is exactly the same compound that puts the heat in chili peppers. But the delivery system, the concentration, and the way it interacts with damaged nerves are completely different from what's in your medicine cabinet.
It's marketed by Averitas Pharma (formerly through Acorda Therapeutics in the U.S.), and it sits in an unusual category — a topical, non-systemic, non-opioid nerve pain treatment delivered by a healthcare professional. There is nothing else quite like it on the market.
How It Works: The Nerve “Reset” Mechanism
Here's where Qutenza gets genuinely fascinating, and where it's worth understanding the difference between this patch and any cream you can buy at the drugstore.
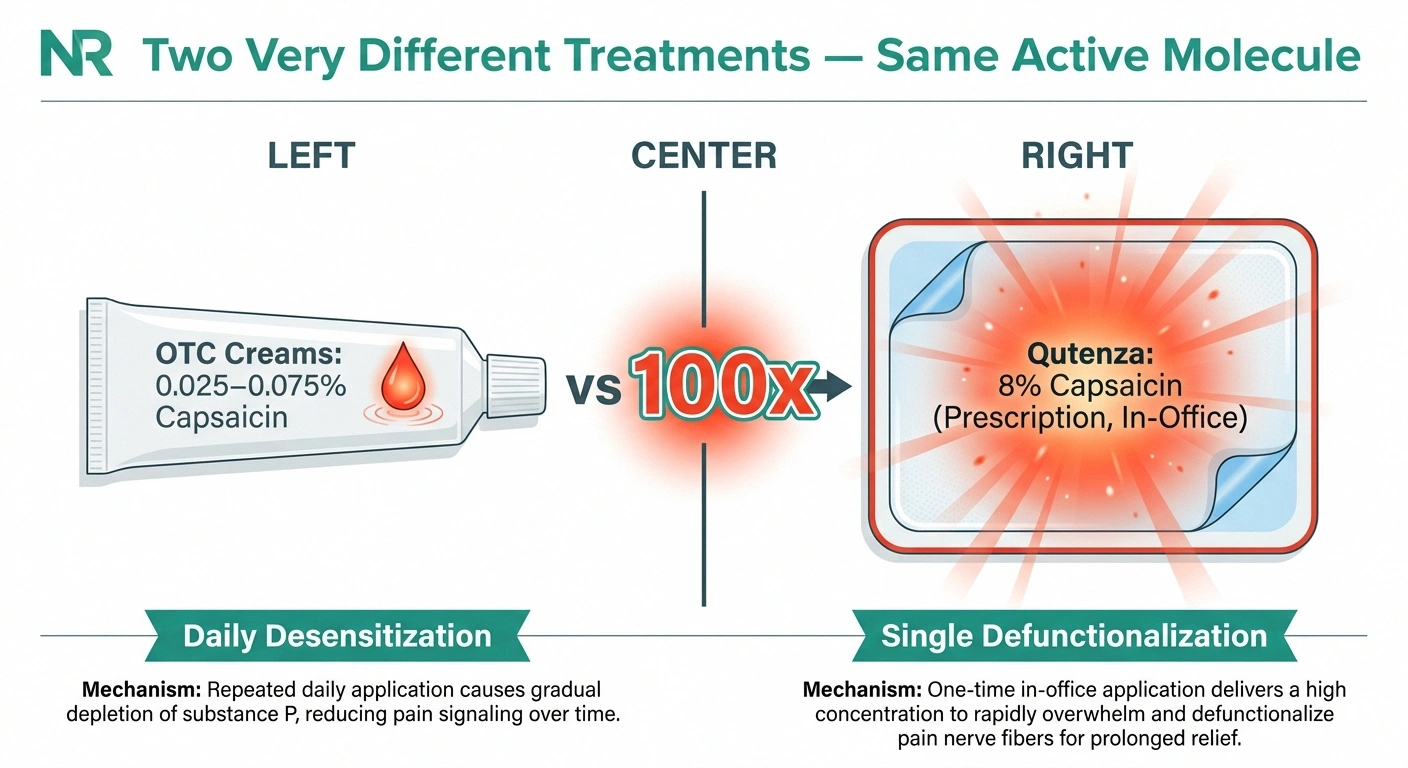
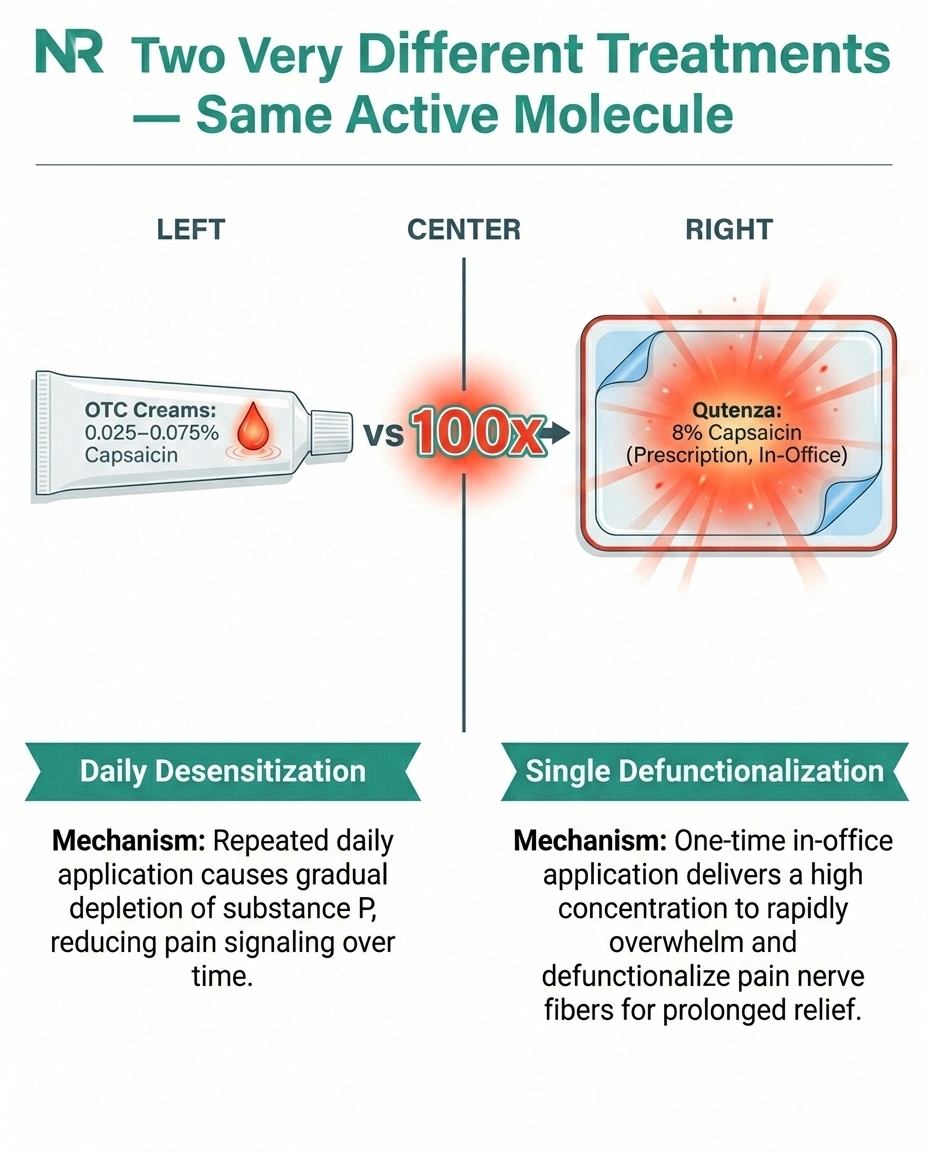
Capsaicin activates a receptor on nerve endings called TRPV1. The TRPV1 receptor is what tells your brain that something is hot or painful. When you eat a chili pepper or rub OTC capsaicin cream on a sore knee, capsaicin triggers TRPV1 — and your nerves report burning, even though nothing is actually burning. Over time, repeated low-dose exposure depletes a chemical called substance P that pain nerves use to send signals, which is how OTC creams produce gradual desensitization.
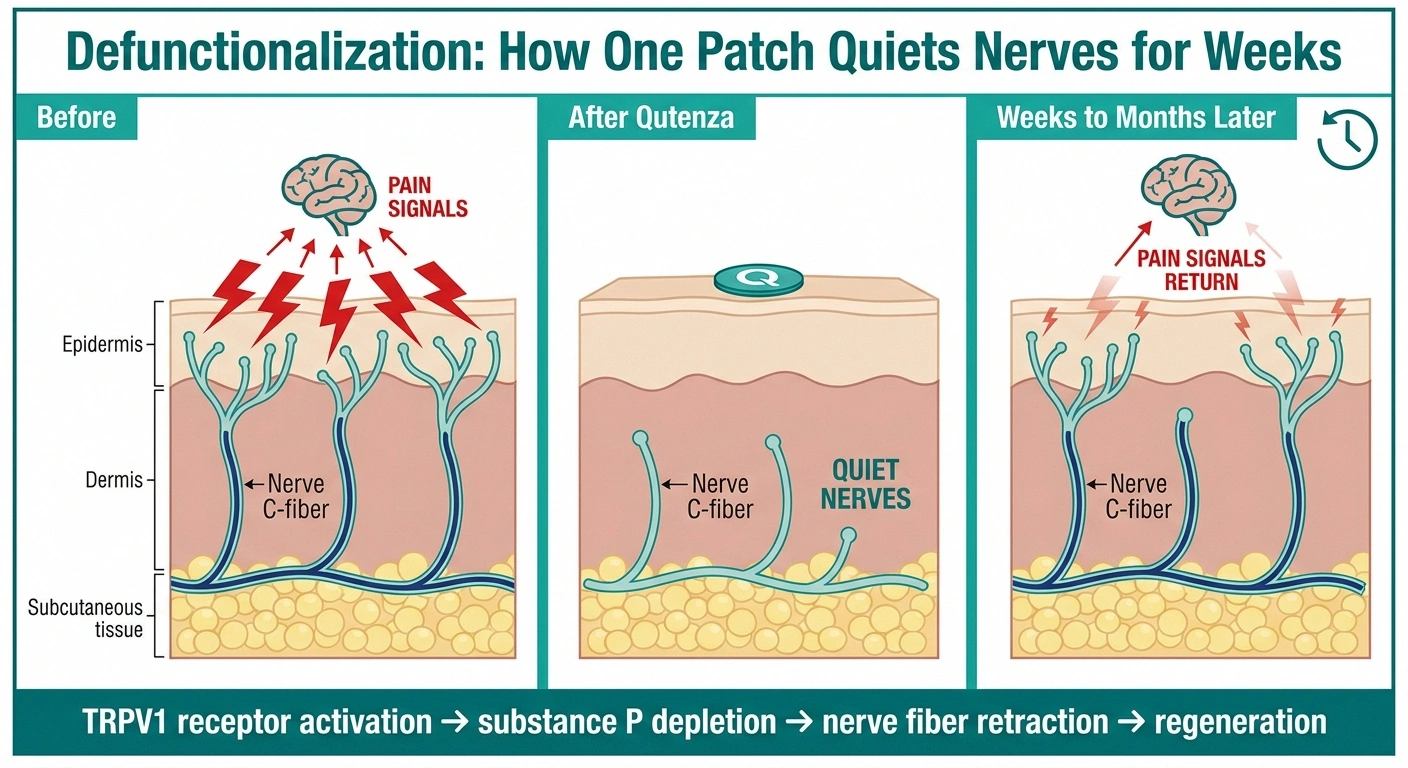
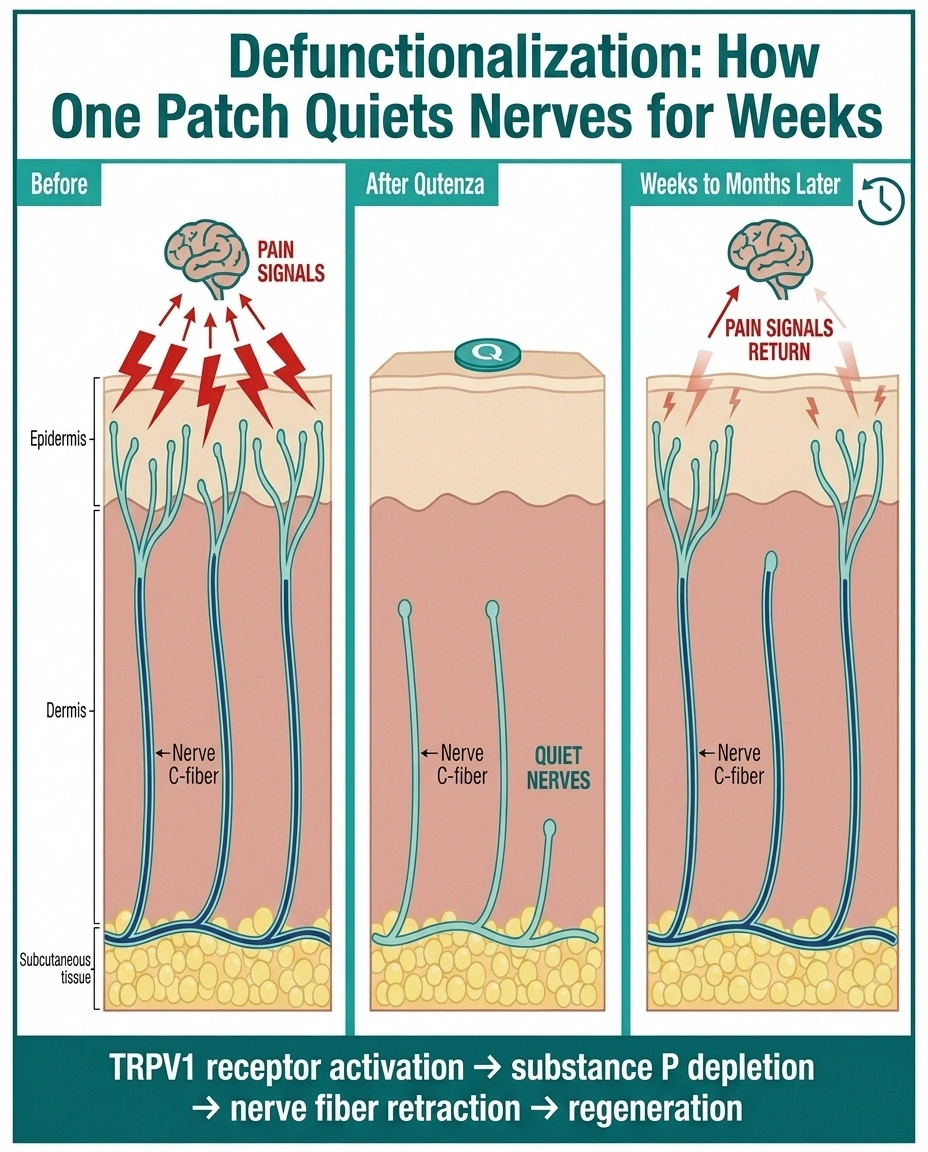
The 8 percent patch does something different and more aggressive. A single, intense exposure causes a process called defunctionalization. The pain-carrying nerve fibers in the upper layer of skin — the small, unmyelinated C-fibers responsible for most chronic burning nerve pain — retract from the epidermis. They essentially withdraw their endings from the surface of the skin. Over the following weeks and months, those nerve endings regenerate. But during that window — anywhere from a few weeks to a few months — the surface-level signal-sending machinery is quiet, and the pain reduces.
This is reversible. The nerves grow back. That's why a single Qutenza treatment lasts for months instead of permanently, and it's why retreatment is allowed and sometimes scheduled at three-month intervals. It's also why Qutenza doesn't damage your underlying ability to feel touch or temperature — it specifically affects the small pain-carrying fibers, not the larger fibers that carry normal sensation.
What It's FDA-Approved For (And What It Isn't)
Qutenza has two FDA-approved indications, and the difference between them matters.
Post-herpetic neuralgia — the nerve pain that lingers after a shingles outbreak — was the first approved indication, granted in 2009. Post-herpetic neuralgia is a difficult condition. Many patients don't respond to gabapentin, pregabalin, or tricyclic antidepressants, and the pain can persist for years. Qutenza has solid evidence for this population.
Painful diabetic peripheral neuropathy of the feet — the burning, tingling, and shooting nerve pain in the feet that's so common in long-standing diabetes — was added as an FDA-approved indication in 2020. This is the indication most readers here will be most interested in. It's specifically for the feet; the patch is applied to the soles and tops of the feet during the procedure.
What Qutenza is not FDA-approved for is also worth knowing. The manufacturer applied for an HIV-associated distal sensory polyneuropathy indication and was turned down by the FDA in 2012. An advisory committee voted almost unanimously against the expanded indication, even though pooled meta-analyses showed some signal for benefit. The committee felt the HIV-specific data wasn't strong enough. So while you may read older articles or off-label descriptions suggesting Qutenza is used for HIV neuropathy, it carries no FDA approval for that use.
Beyond the FDA-approved uses, some specialty pain and neurology practices use Qutenza off-label for small-fiber neuropathy, post-surgical nerve pain, lumbosacral radiculopathy, and other focal neuropathic pain syndromes. There's active research in these areas, and individual responses to off-label use have been encouraging in some studies. But if you're being offered Qutenza off-label, ask specifically about what evidence supports that use for your condition.
What an Actual Qutenza Appointment Is Like
Because Qutenza is unfamiliar to most patients, I want to walk through what a real appointment looks like start to finish. Knowing what to expect makes a big difference.
Before the appointment, the office will usually ask you to take an over-the-counter pain reliever — typically acetaminophen or ibuprofen — about an hour beforehand. Some offices recommend a light meal. If you're prescribed a short-acting opioid for severe pain, your provider may suggest taking one before the appointment, since the patch application itself can be uncomfortable.
When you arrive, a clinician examines the painful area and uses a marker to outline exactly where the patch will go. For diabetic foot neuropathy, that's the soles, the tops of the feet, or both. The skin is cleaned and prepared, and any topical lidocaine (a 4 percent cream) is applied to numb the area. Most clinics let the lidocaine work for about an hour, which is the longest part of the appointment.
The lidocaine is wiped off, and the patch is applied. For diabetic peripheral neuropathy of the feet, the patch stays on for 30 minutes. For post-herpetic neuralgia on the body, it stays on for 60 minutes. The clinician usually stays nearby because the application can be uncomfortable — burning, stinging, or significant pain at the patch site is common, and many offices use cooling devices or cold packs to make the experience more tolerable.
After the patch comes off, the area is cleansed with a special cleansing gel that's included with the Qutenza kit. The cleansing gel neutralizes residual capsaicin so it doesn't continue stinging. You'll usually be observed for another 15 to 30 minutes while the worst of the application discomfort settles.
The whole visit typically takes 2 to 3 hours. You should plan to have a ride home, especially if you took any pain medication beforehand. You'll likely have some lingering burning sensation at the application site for the rest of the day and possibly into the next day; this fades.
How Quickly It Works and How Long It Lasts
This is where I want to set realistic expectations, because Qutenza doesn't work overnight and that surprises people.
Pain relief typically begins to emerge in the first one to two weeks after the application. The peak effect usually shows up around weeks two through four. From there, the benefit gradually fades over the following weeks. Most patients see meaningful pain reduction for somewhere between 8 and 12 weeks from a single application.
This is a different rhythm than a daily pill. With a daily medication, you adjust the dose and feel the effect day to day. With Qutenza, you have one good day in the office, several days to a week of feeling about the same as before, then a slow build into real relief over the next month, then a slow taper over the following two months. Retreatment is allowed every three months for patients who respond.
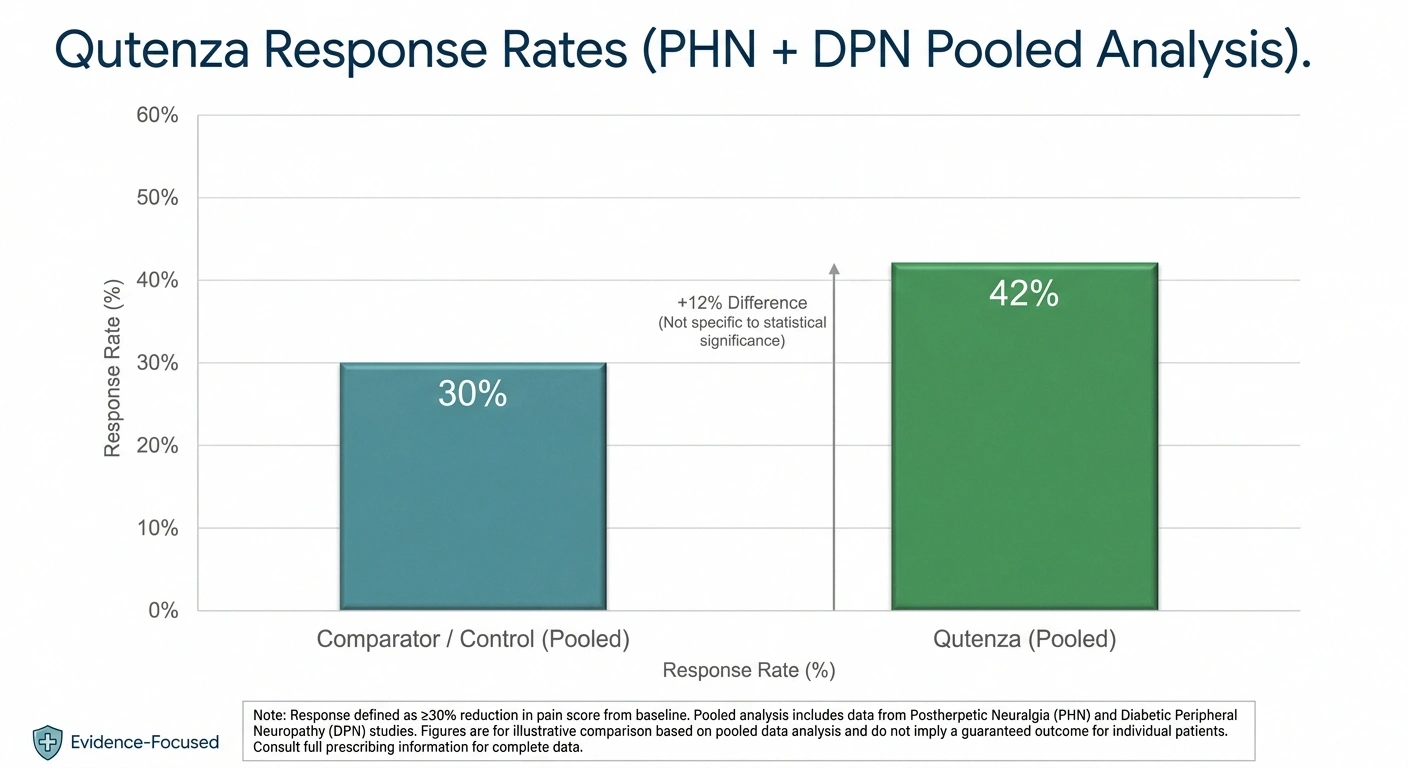
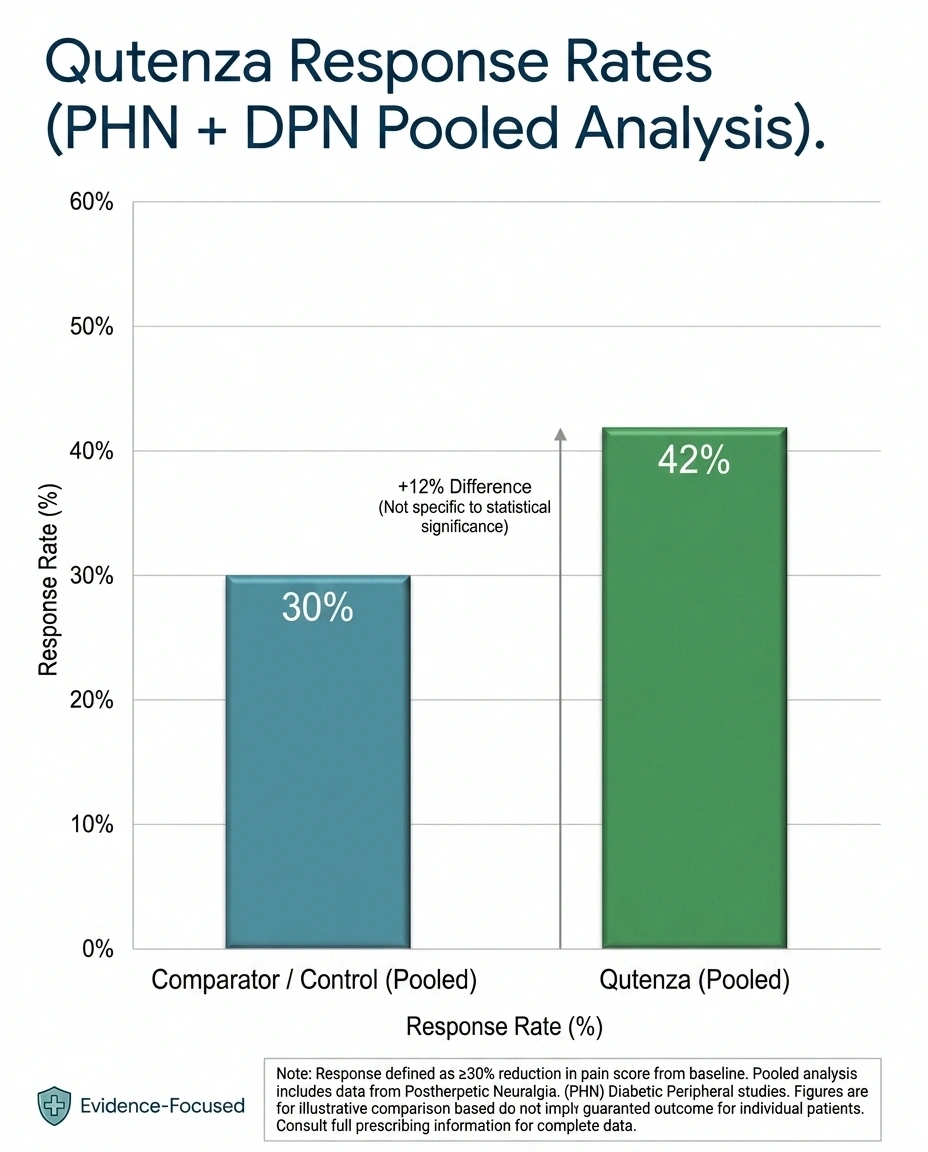
In the clinical trials, response rates have been meaningful but not transformational. A frequently-cited pooled analysis showed about 43 percent of treated patients achieving at least 30 percent pain reduction lasting 2 to 12 weeks, compared to about 34 percent in the control group. For the specific diabetic peripheral neuropathy of the feet indication, mean pain reduction was around 2 points on a 10-point pain scale, with roughly half of patients hitting the 30 percent response threshold at week 12.
Those aren't miraculous numbers. They're real, modest improvements over placebo for a difficult-to-treat condition. The honest framing: a meaningful minority of patients get real relief, the rest don't, and the only way to know which group you're in is to try it.
Side Effects and Safety
Because Qutenza is topical, the systemic side effect picture is much smaller than what you'd see with an oral medication. There's essentially no drug-interaction concern, because so little capsaicin gets into the bloodstream that it doesn't affect liver enzymes or other medications you might take. That alone makes it appealing for older patients already on multiple medications.
The local side effects are real and worth knowing about. Application-site burning, redness, and pain are the most common — almost every patient experiences some discomfort during application and for a few hours afterward. Transient sensory changes in the treated area — usually mild numbness or hypoesthesia — are common and tend to fade. Itching at the application site is also common.
One safety consideration that catches people off-guard: Qutenza can cause a transient rise in blood pressure during application and for a short period afterward, driven by the pain response itself. For most patients this is mild and clinically insignificant, but for patients with uncontrolled hypertension or recent cardiovascular events, providers will want to assess the risk carefully. Make sure your prescriber knows your full cardiovascular history.
Qutenza is not applied over broken skin, open foot ulcers, infections, or areas with significant skin damage. This is a critical safety point for patients with diabetic foot ulcer history. If your feet have areas of skin breakdown, those areas have to be excluded from treatment or healed first.
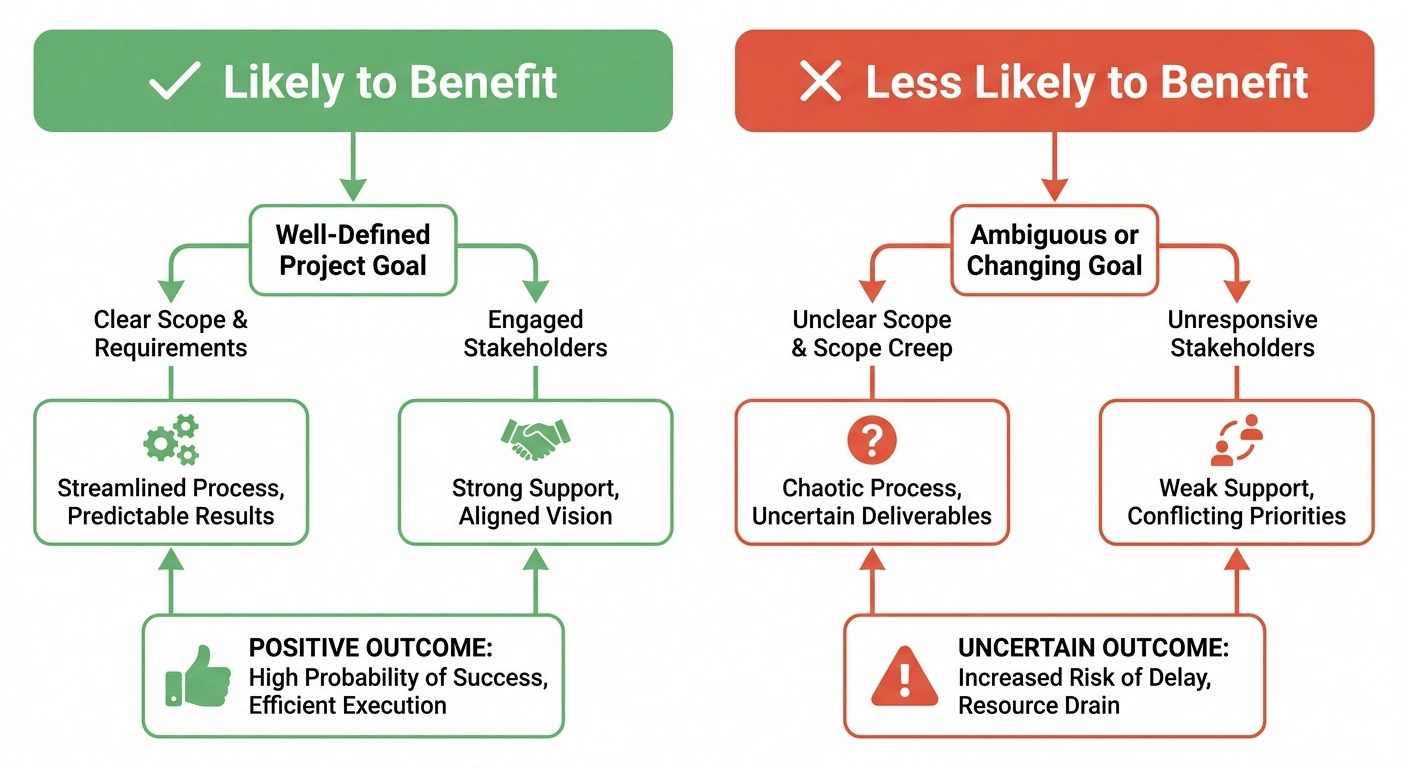
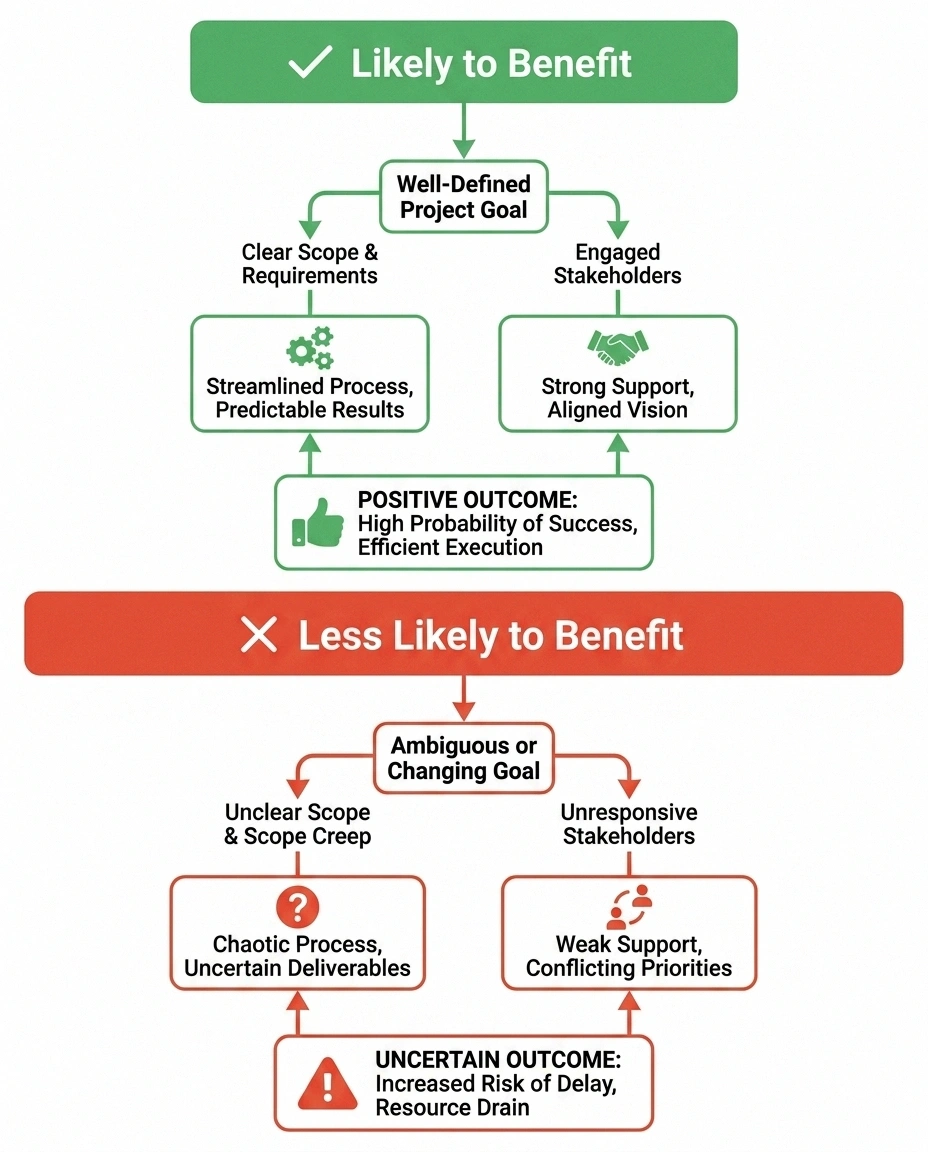
Who Tends to Benefit Most
From the trial data and from talking with people who've used it, certain patient profiles tend to do better with Qutenza than others.
Focal or limited-area pain tends to respond better than diffuse, body-wide pain. A patient with burning concentrated in one foot, or a clear band of trunk pain after shingles, has a better area-to-patch ratio than someone whose pain is everywhere.
Patients who have tried and failed standard oral medications — gabapentin, pregabalin, duloxetine, tricyclics — and who don't want or can't tolerate more pills are natural candidates. Qutenza adds a tool without adding a daily medication.
Older patients with polypharmacy concerns often benefit from Qutenza specifically because it doesn't introduce drug interactions. If your medication list is already long, adding a treatment that doesn't change your blood levels of anything else has real value.
Patients with fall-prone neuropathy may benefit because Qutenza doesn't cause the sedation, dizziness, or unsteadiness that oral neuropathic-pain medications often do. For a patient where every drowsy moment is a fall risk, that matters.
Who Probably Shouldn't Bother
Equally honest: Qutenza isn't for everyone, and some patients are unlikely to benefit.
• Failed oral medications (gabapentin/pregabalin/SNRIs)
• Older patients with polypharmacy concerns
• Patients where sedation/dizziness from oral meds is a fall risk
• Active foot ulcers or broken skin
• Established central sensitization
• Cannot tolerate the application discomfort
Patients with truly diffuse, whole-body neuropathic pain often can't get enough skin area covered to see meaningful relief. The patch can only target so much surface area in a single application.
Patients with significant foot ulceration or active wound healing often have to defer treatment until skin is intact.
Patients with established central sensitization — where the pain has migrated from the peripheral nerves into the central nervous system — are less likely to benefit because the source of the pain is no longer just at the skin level. A more comprehensive treatment approach is usually more appropriate for these patients.
And patients who simply can't tolerate the procedure — the burning during application is a real obstacle for some — sometimes try one round and decide it isn't worth repeating.
The Cost and Coverage Picture
Qutenza is expensive. A single patch — the medication itself — typically wholesales in the $500 to $1,500 range, depending on the source and the practice's purchasing agreements. Layered on top of that are office-visit charges, the nursing time required during application, and any related infusion-center or procedure fees.

The good news is that for FDA-approved indications, coverage has improved substantially. Medicare Part B generally covers Qutenza for post-herpetic neuralgia and painful diabetic peripheral neuropathy when it's administered in a doctor's office, since it's classified as a medically administered drug rather than a self-administered prescription. Most commercial insurance plans also cover the approved indications, though many require prior authorization and documentation of failed prior treatments.
The practical bottleneck is often finding a clinic that stocks and applies it. Qutenza requires specific training, dedicated room time, and a willingness to manage the application discomfort. Interventional pain practices and many neurology practices have it; primary care does not. A specialty referral is almost always required.
Where Qutenza Fits in a Full Treatment Plan
I want to close on something I think gets lost in product-specific articles like this one. Qutenza is one tool. It is not a stand-alone answer to neuropathy, and it isn't designed to be.
In a thoughtful treatment plan, Qutenza usually sits alongside continued blood-sugar management (for diabetic patients), oral nerve-pain medications if they're helping at all, topical creams used between treatments, gentle exercise, and the lifestyle work that compounds. It can quiet the foreground burning enough that the rest of the plan finally gets a chance to work.
For some patients, it's life-changing. For others, it's a worthwhile experiment that doesn't move the needle much. The only way to know is to ask your specialist whether you're a candidate, line up the prior authorization, and try it. Three months later, you'll have an honest answer, and you can plan from there.
Frequently Asked Questions
Can I get Qutenza from my regular doctor?
Almost never. Qutenza requires specific training in application, dedicated room time, the proper personal protective equipment for handling high-concentration capsaicin, and clinical experience in managing the application discomfort. Primary care offices rarely carry it. Most patients need a referral to an interventional pain specialist, a neurology practice that offers it, or occasionally a podiatry practice. Ask your primary care doctor for a referral, or call larger pain or neurology groups in your area to ask whether they administer it.
Does the patch really hurt that much?
It varies. Some patients tolerate the 30-minute application easily, with only a mild warming sensation. Others find it genuinely painful and rate the burning intensity as severe. Most fall somewhere in the middle. Clinics that do Qutenza routinely have the experience to manage the discomfort — topical lidocaine before, cooling devices during, oral pain medication if needed. Ask the practice upfront what their comfort protocol is. A well-run Qutenza appointment is usually much more tolerable than the horror stories make it sound.
How is Qutenza different from over-the-counter capsaicin cream?
Concentration and mechanism. Qutenza contains 8 percent capsaicin and works through a single intense exposure that causes nerve endings to retract from the skin for weeks at a time. Over-the-counter creams contain 0.025 to 0.075 percent capsaicin and work through gradual desensitization with daily use. Both can help. But they aren't substitutes for one another — they're different treatments at very different intensity levels.
Can I drive home after a Qutenza appointment?
If you only took the recommended over-the-counter pain reliever and feel alert, you may be able to drive. But if you took any sedating pain medication, you should arrange a ride. Plus, if Qutenza was applied to your feet, you may be uncomfortable enough that driving is genuinely unsafe for a few hours. Many people find it easier to plan for a ride than to figure it out in the moment after the procedure.
Will I lose sensation in my feet permanently after Qutenza?
No. The defunctionalization specifically affects the small pain-carrying nerve fibers, and those fibers regenerate over weeks to months. Touch, vibration, and most other sensations remain intact. Some patients report mild, temporary numbness or altered sensation in the treated area for a few weeks; for most patients this is a welcome change rather than a problem, given that the alternative was constant burning pain.
How often can I have Qutenza repeated?
Retreatment is generally allowed every 3 months, based on whether your pain has returned and how well you tolerated the previous application. Many patients who respond well end up on a quarterly schedule. Some find that the duration of relief extends with successive treatments; others maintain the same approximate window each time.
What if Qutenza doesn't work for me?
If the first application doesn't help, many specialists recommend a second trial 3 months later, since responses can sometimes build over multiple applications. If two well-administered treatments don't help, you're probably not a Qutenza responder, and your specialist should pivot to other approaches — different oral medications, neuromodulation like spinal cord stimulation, or other interventional options.
Is Qutenza covered by Medicare?
Generally yes, under Medicare Part B, for the FDA-approved indications (post-herpetic neuralgia and painful diabetic peripheral neuropathy of the feet) when administered in a doctor's office. Because Qutenza is classified as a medically administered drug rather than a self-administered prescription, it falls under Part B rather than Part D. Coverage details vary by region, and prior authorization is often required, so confirm with the administering practice before scheduling.