Tapentadol — sold under the brand name Nucynta — is one of the medications that turns up in neuropathy conversations the way an exit ramp turns up after a long drive. People reach for it when the more familiar roads aren't getting them where they need to go. It has a story that's a little unusual in the opioid family, and a place in the diabetic neuropathy treatment ladder that's worth understanding clearly — both for what it can offer and for the very real things it asks of you in return.
I want to walk through tapentadol the way I'd want it walked through for me: what makes it different from the older opioids, where the evidence actually lives, who it's for, who it's not for, and what to ask before you ever fill that first prescription. This isn't a recommendation. It's the briefing.
What Tapentadol Actually Is
Tapentadol is a prescription pain medication first approved by the FDA in 2008 for moderate-to-severe acute pain (the immediate-release tablets, simply called Nucynta) and later, in 2012, for the long-term treatment of pain associated with diabetic peripheral neuropathy (the extended-release tablets, called Nucynta ER). That second approval matters. As of this writing, tapentadol ER is the only opioid the FDA has specifically approved for nerve pain from diabetic neuropathy. Every other opioid being used for nerve pain is being used off-label.
Tapentadol ER (Nucynta ER) is the only opioid the FDA has specifically approved for nerve pain from diabetic neuropathy. It's a Schedule II controlled substance — same regulatory category as oxycodone and morphine — and it sits toward the back of the treatment ladder, not the front.
It is a Schedule II controlled substance, which puts it in the same regulatory category as oxycodone, morphine, and hydrocodone. That scheduling tells you something important about how the DEA views its potential for dependence and misuse. The benefits-versus-risks conversation around tapentadol is real and serious, and it's the conversation your prescriber should be having with you before this medication ever enters the picture.
That said, tapentadol is not “just another opioid.” The mechanism is what makes it interesting for neuropathy specifically.
Why It's Called “A Different Kind of Opioid”
Most opioids — morphine, oxycodone, hydrocodone, codeine — work essentially through one main route. They bind to mu-opioid receptors in the brain and spinal cord and turn down the volume on pain signals. They're very good at acute pain — the broken bone, the post-surgical recovery, the kidney stone. They're considerably less good at neuropathic pain, the burning and electric-shock and pins-and-needles pain that comes from damaged nerves themselves. Pure opioids treat that kind of pain inconsistently, and the doses required often come with side effects that outweigh the benefit.
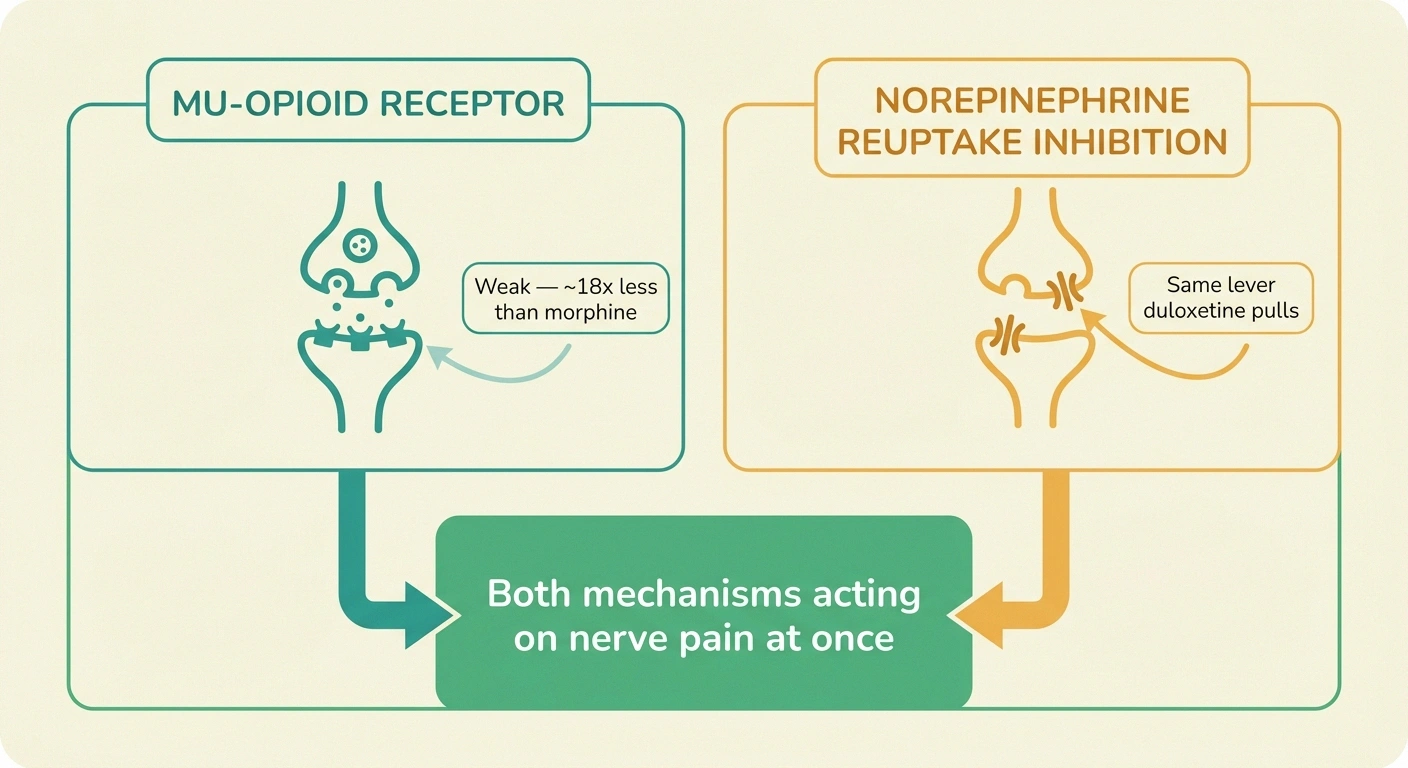
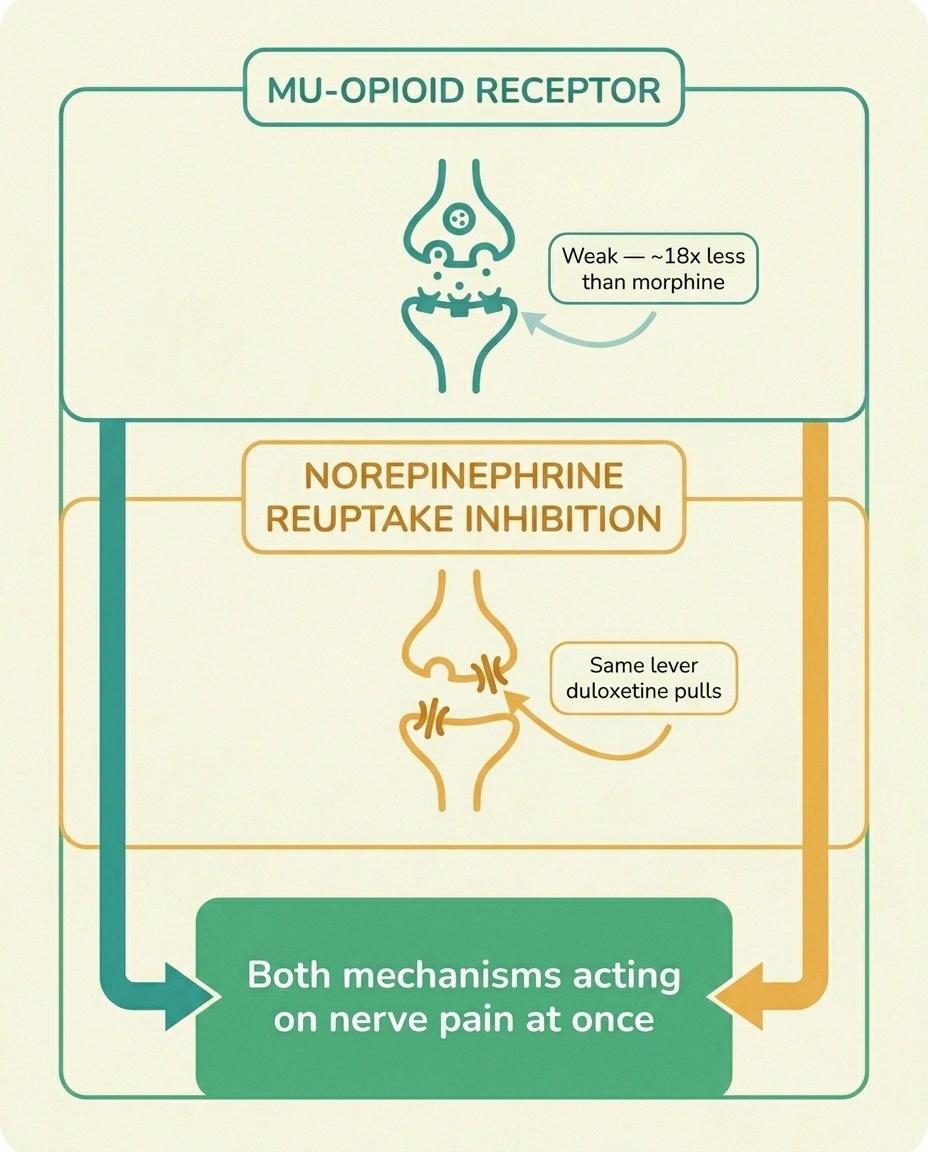
Tapentadol does two things at once. First, it does the classic opioid thing — it binds to mu-opioid receptors. But it binds weakly, about 18 times weaker than morphine. By itself, that wouldn't be enough to control significant pain. The second thing is what changes the math: tapentadol also blocks the reuptake of norepinephrine in the spinal cord. Norepinephrine is one of your body's own pain-suppressing chemicals. When tapentadol prevents it from being reabsorbed, more of it stays in circulation, and the descending pain-control pathways in your spinal cord get a steady boost.
That second mechanism is the same one that duloxetine (Cymbalta) uses to treat nerve pain — except in duloxetine it's the whole drug, and there's no opioid component at all. In tapentadol, the norepinephrine effect and the mild opioid effect work together. The result is a medication that hits nerve pain through two different doorways simultaneously.
This dual mechanism is also why tapentadol is sometimes compared to tramadol, which has a similar idea — opioid plus monoamine reuptake. But tapentadol has cleaner pharmacology. It doesn't rely on the body's CYP2D6 liver enzyme to activate, so it works the same way in everyone (tramadol doesn't, which is why some people get no benefit from it). It doesn't carry the seizure risk that comes with tramadol. And it has a much smaller serotonin component, which lowers the risk of serotonin syndrome when combined with other medications.
The Evidence for Tapentadol in Diabetic Neuropathy
The FDA didn't approve tapentadol ER for diabetic peripheral neuropathy on a hunch. The approval rested on two large randomized trials run between 2009 and 2011, plus an open-label maintenance study, that together enrolled several hundred patients with painful diabetic neuropathy.
In the FDA-approval trials of Nucynta ER for diabetic peripheral neuropathy, patients who continued the medication maintained significantly better pain control over 12 weeks compared to those randomized to placebo — a roughly one-point reduction on the 0-to-10 pain scale. That magnitude is comparable to pregabalin, gabapentin, and duloxetine in their own DPN trials. Tapentadol is not dramatically more effective. It offers a different mechanism for patients first-line agents haven't reached.
The study design worked like this: patients with at least moderate diabetic nerve pain were started on Nucynta ER and titrated up to a tolerated dose over three weeks. Patients who got at least a one-point pain reduction (on a 0-to-10 scale) were then randomized — half continued on their effective tapentadol dose for another 12 weeks, the other half were quietly switched to placebo. The ones who continued tapentadol kept their pain control. The ones who got placebo lost it. The size of the effect translates roughly to about a one-point greater pain reduction over placebo on the 0-10 scale, which is real but modest.
To put that in context: pregabalin (Lyrica) and gabapentin show similar magnitudes of pain reduction in their diabetic neuropathy trials. So does duloxetine. So do the tricyclic antidepressants like amitriptyline. Tapentadol is not dramatically more effective than the first-line non-opioid options. What it offers is a different mechanism for people who haven't gotten enough relief from those first-line drugs — or who can't tolerate them.
For diabetic neuropathy specifically, the evidence is reasonable. For other types of neuropathic pain — chemotherapy-induced, postherpetic, idiopathic small-fiber — the evidence base is much thinner. Some pain specialists do prescribe tapentadol for those conditions, but they're using their clinical judgment, not following an FDA-approved indication.
Where Tapentadol Sits in the Treatment Ladder
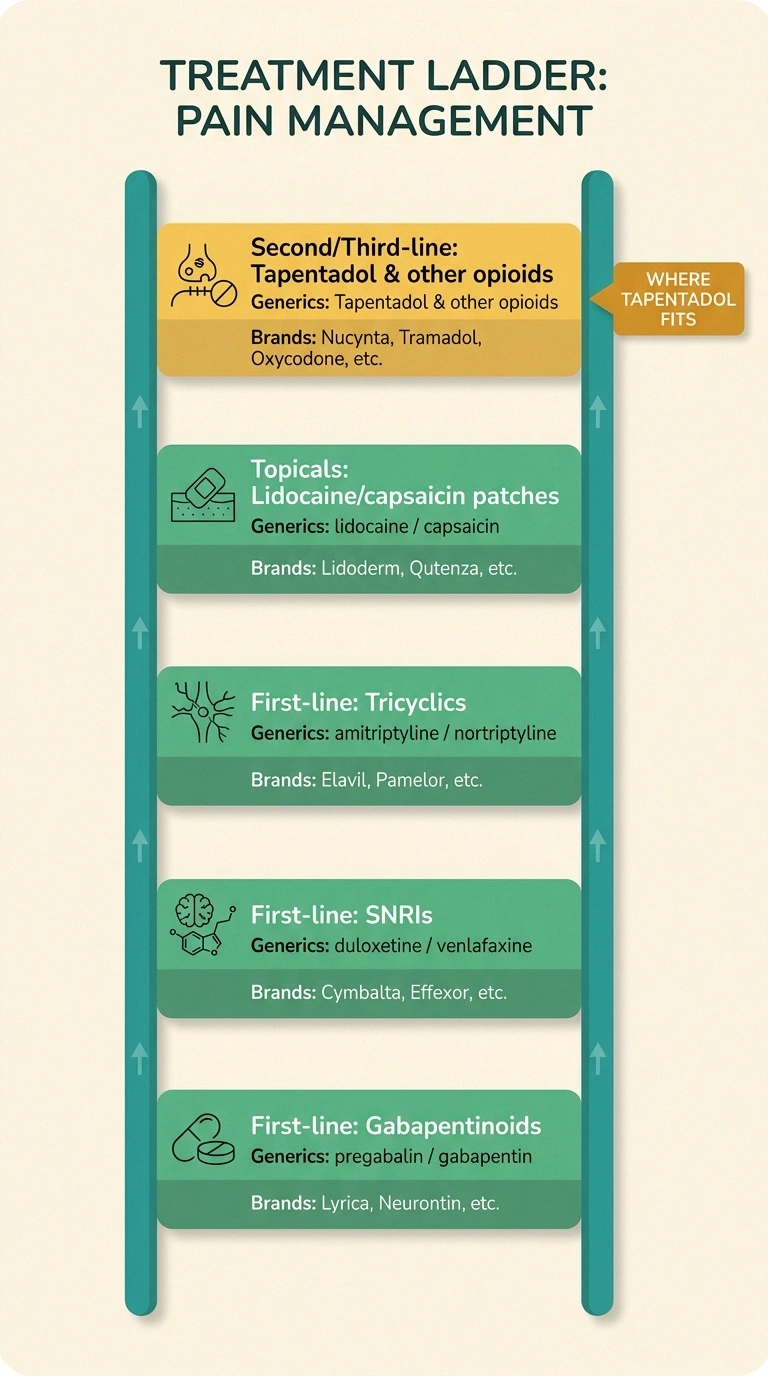
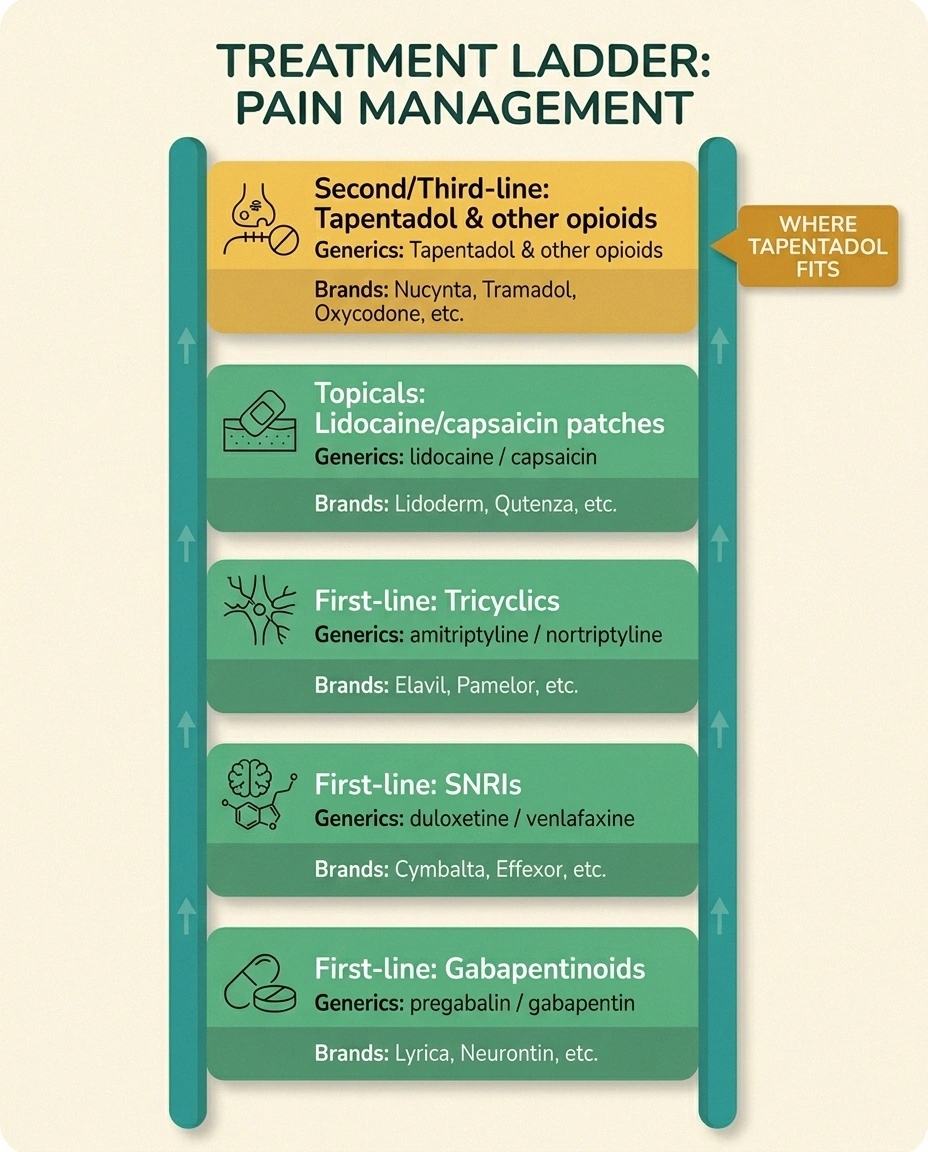
Pretty much every major guideline for treating diabetic neuropathy puts opioids in general — and tapentadol with them — toward the back of the line. The American Academy of Neurology, the American Diabetes Association, the European Federation of Neurological Societies, and the international NeuPSIG consensus all rank these treatments first:
than morphine
(the duloxetine mechanism)
- Gabapentinoids: pregabalin (Lyrica) and gabapentin
- SNRIs: duloxetine (Cymbalta) and venlafaxine (Effexor)
- Tricyclic antidepressants: amitriptyline and nortriptyline (often off-label)
- Topical options: high-dose capsaicin patches and lidocaine patches
Opioids — including tapentadol — typically enter the picture only when those first-line options have been tried and either didn't work well enough or weren't tolerated. The CDC opioid prescribing guidelines explicitly discourage opioids as first-line treatment for chronic non-cancer pain, and most pain specialists try hard to avoid them when there's a reasonable non-opioid alternative.
That doesn't mean tapentadol is a last resort. For patients who already need a long-acting pain medication, the FDA's approval makes tapentadol ER a more thoughtful choice than a pure opioid for diabetic nerve pain — because at least it's working through the noradrenergic mechanism that matches the underlying problem. But for a patient just starting their neuropathy journey, the first stop is not Nucynta. The first stop is gabapentin or duloxetine or sometimes a combination, possibly paired with the non-medication tools you'll find in our natural remedies guide and the right footwear and movement strategy.
Dosing — How Tapentadol Is Actually Taken
This is for context only. Your prescriber owns the actual dosing decisions.
Nucynta ER (extended-release) is the form approved for diabetic neuropathy and is typically taken every 12 hours. It comes in 50, 100, 150, 200, and 250 milligram tablets. Patients usually start at 50 mg twice daily and titrate up by 50 mg every three days as tolerated, with a maximum dose of 250 mg twice daily. The ER tablets must be swallowed whole — crushing, chewing, or splitting them releases the entire dose at once, which can be dangerous. They cannot be used for breakthrough pain.
Nucynta IR (immediate-release) is approved for acute pain, not chronic neuropathy. It's 50, 75, or 100 milligrams every 4-6 hours, with a maximum of 600 mg per day. Some neuropathy patients are prescribed a small dose of IR for breakthrough flares on top of their ER baseline — that decision lives with the prescribing pain specialist.
Switching from another opioid to tapentadol, or from tapentadol to something else, is not a do-it-yourself project. The conversion ratios are tricky, and abrupt stops produce withdrawal. This is one of the strong arguments for having an established pain medicine specialist if you're going to be on an opioid for chronic neuropathy — they manage transitions safely.
Side Effects, Real-World
The side effect profile of tapentadol is one of its more interesting selling points. In the clinical trials, the most common complaints were nausea, vomiting, dizziness, somnolence, constipation, headache, and fatigue — the same general list as any opioid. What's different is the rates. Compared to oxycodone at equivalent pain relief, tapentadol consistently shows lower rates of nausea, vomiting, and constipation. That's not a small thing. Constipation alone drives more people off opioids than almost any other side effect.
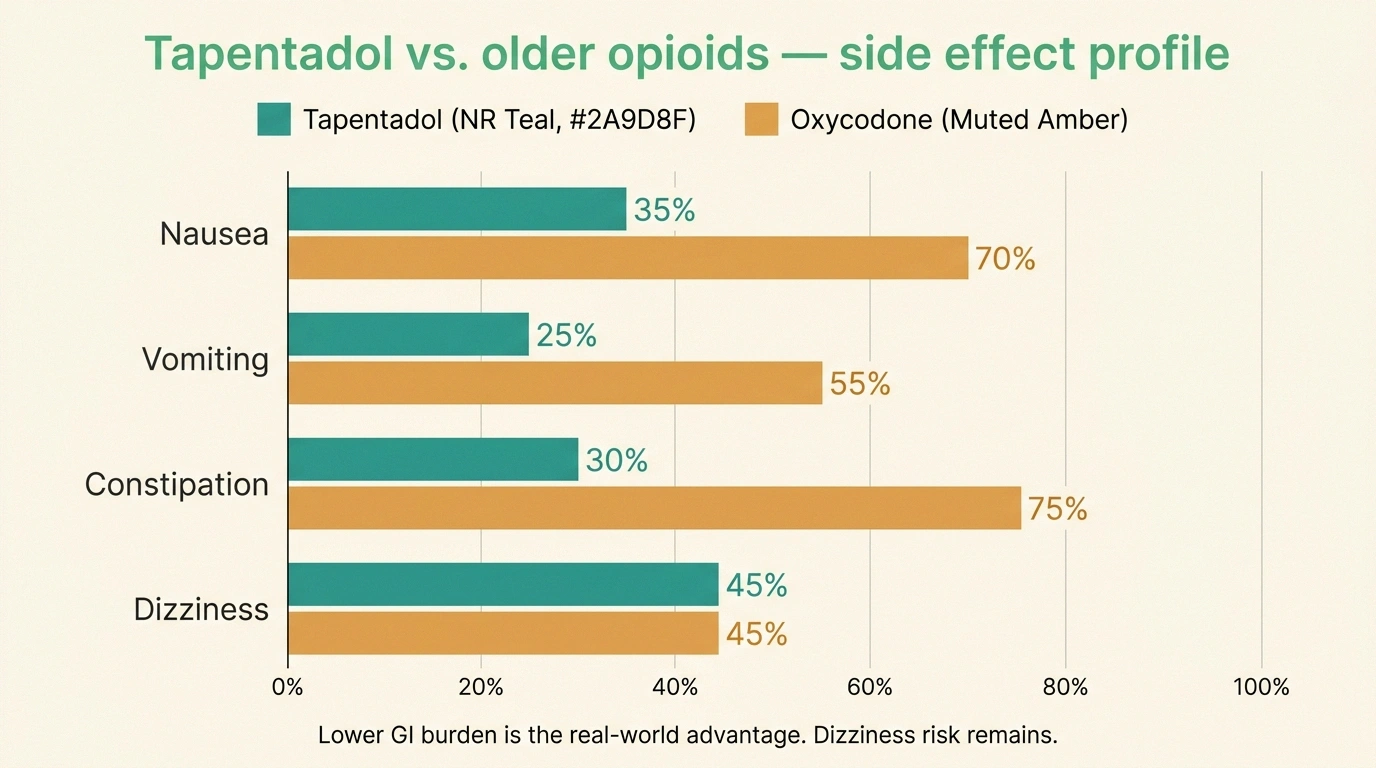
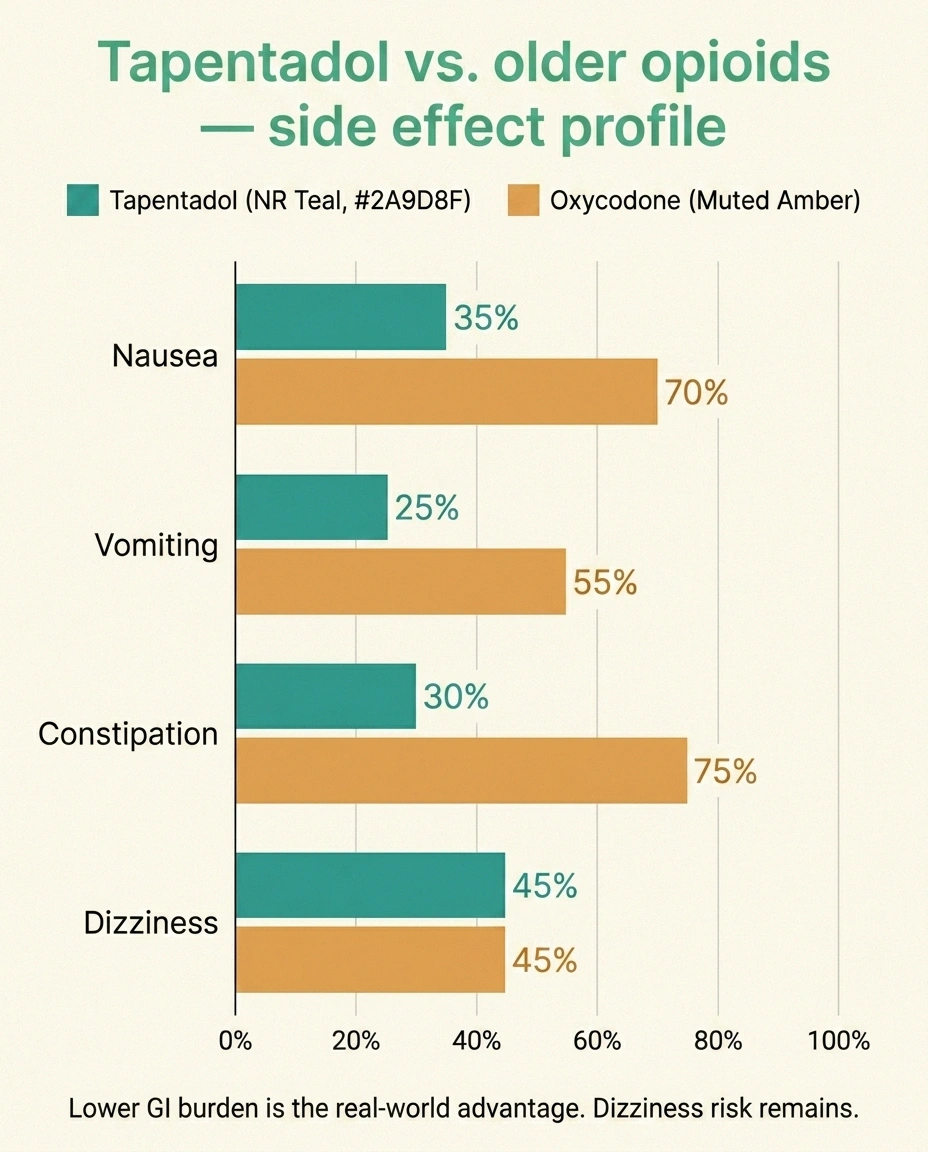
The “less GI side effect burden” is the practical advantage tapentadol claims over older opioids. It is not the same as “no side effects.” A meaningful number of patients in the DPN trials dropped out because of nausea or dizziness, especially during the titration phase. Older patients seem more sensitive to the dizziness, which raises real concerns about fall risk in patients who already have balance problems from their neuropathy. This is a serious consideration. Adding a medication that increases dizziness on top of an existing balance deficit can be the difference between an independent life and a hip fracture.
Urinary retention shows up with tapentadol too, and that matters especially for people who already have autonomic features to their neuropathy — bladder issues, constipation, blood pressure swings. Layering more anticholinergic-adjacent effects on top of autonomic neuropathy can be miserable.
The Risks Nobody Should Skim Over
Tapentadol carries two FDA Black Box Warnings that are mandatory reading.
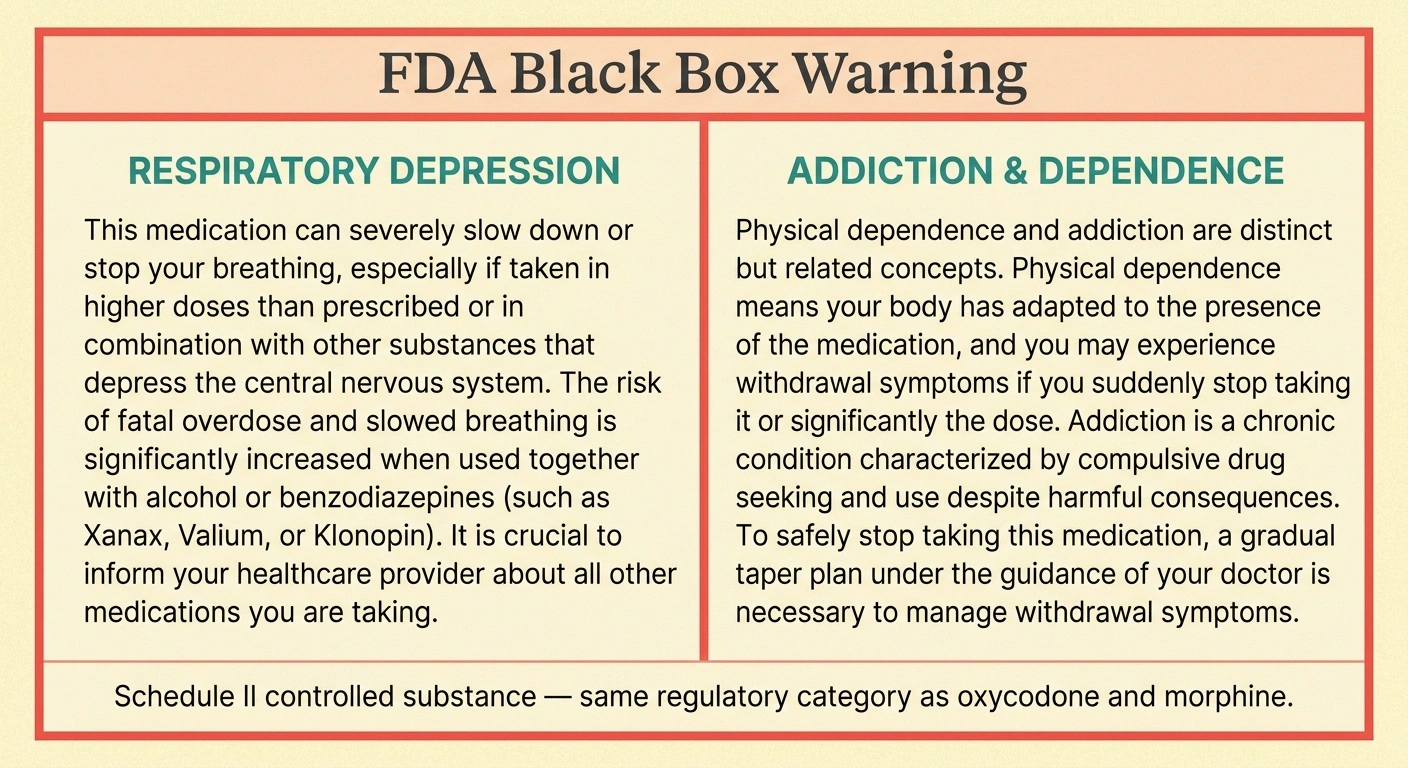
Opioids slow breathing. The danger multiplies when combined with benzodiazepines (Xanax, Ativan), sleep medications (Ambien), or alcohol. Never combine without explicit medical guidance.
Physical dependence develops in essentially every long-term patient. Withdrawal symptoms appear within 12-24 hours of stopping abruptly. The taper is part of the medication, not optional.
Respiratory depression. Opioids slow breathing. At therapeutic doses in healthy adults, this is mild and tolerated. At higher doses, or in people with sleep apnea, or in people who combine the opioid with other respiratory depressants — alcohol, benzodiazepines like Xanax or Ativan, sleep medications like Ambien — breathing can slow to the point of stopping. This is the mechanism of opioid overdose. Tapentadol is a weaker mu-opioid agonist than morphine, which lowers but does not eliminate this risk. The combination with benzodiazepines and alcohol is the most dangerous one and is responsible for a high fraction of opioid deaths.
Addiction, abuse, and dependence. Tapentadol has real abuse potential, which is why it's Schedule II. The risk is not zero, and it's higher in people with a personal or family history of substance use disorder, in adolescents and young adults, and in people taking it for prolonged periods. Physical dependence — meaning the body adjusts to having the medication and reacts when you stop — develops in essentially every patient on long-term opioids and is different from addiction. But the experience of withdrawal is unpleasant and clinically important. Stopping tapentadol abruptly causes withdrawal symptoms within hours: anxiety, sweating, runny nose, restless legs, gut cramping, diarrhea. The taper is part of the medication, not optional.
Other situations to know about:
- Pregnancy: Tapentadol crosses the placenta. Babies born to mothers taking it can develop neonatal opioid withdrawal syndrome, which is a medical emergency requiring NICU treatment.
- MAOIs: Patients taking monoamine oxidase inhibitors (a class of older antidepressants and Parkinson's medications) cannot use tapentadol — within 14 days of the MAOI, the combination can cause a hypertensive crisis or serotonin syndrome.
- Combinations: Adding tapentadol to duloxetine, venlafaxine, or other SNRIs requires care — the additive noradrenergic effect, while small, can raise heart rate and blood pressure. Adding to benzodiazepines is the high-risk combination already mentioned. Adding to gabapentin or pregabalin is generally done but increases drowsiness and fall risk.
The Cost and Access Reality
Here's the part patients are surprised by: tapentadol is expensive. As of 2026, there is no generic version of Nucynta ER available in the United States at many of the commonly used strengths, which keeps the brand price high. A 30-day supply of Nucynta ER without insurance can run $400-800 depending on strength and pharmacy. With insurance, the picture varies enormously — Medicare Part D plans typically cover it but often require a prior authorization, meaning the prescriber has to document that you've tried first-line options first.
If you're staring at a Nucynta prescription and thinking about cost, three practical moves: ask your prescriber whether a manufacturer copay card is available (they often are for brand-name pain medications), ask your pharmacist to run a GoodRx or similar discount price, and ask the prescriber whether tapentadol IR (which has generic options) is a reasonable alternative even though it's off-label for chronic use. Talk through whether other FDA-approved DPN options — pregabalin, duloxetine — make sense before committing to Nucynta.
Who Tapentadol Is For, Practically
Reading between the lines of the evidence and the guidelines, the patient who benefits most from a tapentadol trial usually looks something like this:
- Confirmed diabetic peripheral neuropathy with significant chronic pain (not occasional discomfort)
- Adequate trials of at least two first-line agents — typically a gabapentinoid and an SNRI like duloxetine — without enough relief
- No active substance use disorder and no recent history of one
- No untreated sleep apnea
- Not currently on benzodiazepines or other CNS depressants
- An established prescriber (often pain medicine or a neurologist) who will monitor consistently
- A clear understanding of the dependence and taper realities
Patients for whom tapentadol is a poor fit:
- People with severe baseline dizziness or a history of falls — adding an opioid to a fall-risk patient is a serious decision
- People with significant constipation issues already (autonomic gut involvement)
- People who have not yet given a first-line agent a real trial at an adequate dose
- People with active or recent substance use concerns
- People in the first trimester of pregnancy or planning pregnancy
- People who cannot reliably store a controlled medication safely (grandchildren in the house, history of theft)
Questions to Ask Before Filling a Tapentadol Prescription
If a tapentadol prescription is in front of you and you want to walk into the pharmacy with your eyes open, here are the questions I'd take to the conversation:
- Have we exhausted the first-line, non-controlled options? Specifically — full trials of gabapentin or pregabalin and an SNRI like duloxetine, at adequate doses, for adequate time. If the answer is “not really,” that's worth pausing on.
- What's the plan for re-evaluation? Tapentadol is not a “set it and forget it” medication. Most thoughtful prescribers re-assess every three months. If your prescriber hasn't talked about that, ask.
- What's the taper plan if this doesn't work? Knowing how you'll get off the medication is part of knowing how to start it.
- How do we manage breakthrough days? Some prescribers add a small dose of IR for flares; some don't.
- What do I tell my other prescribers? Your dentist, your surgeon if you have surgery, your urgent-care doctor — all of them need to know you're on a Schedule II opioid.
- What about the rest of my plan? Tapentadol works better as part of a coordinated approach — tight blood sugar control, physical therapy, the evidence-backed supplements that pair well with prescription treatment, balance training. Not as the whole plan.
The Honest Bottom Line
Tapentadol is a real medication with a real role. It is the only opioid the FDA has specifically approved for diabetic neuropathic pain, and its dual mechanism gives it a more thoughtful match to nerve pain than older opioids. For some patients who have not gotten relief from the first-line agents, it makes a meaningful difference in pain and in the ability to function.

Tapentadol is a real tool for nerve pain that hasn't responded to first-line treatment — but the opioids belong toward the end of the conversation, not the beginning. If your prescriber suggests it after you've worked through gabapentinoids and SNRIs, that's a reasonable medical conversation. If someone reaches for it without exhausting those options first, slow down and ask why.
It is also a Schedule II controlled substance with respiratory depression risk, dependence risk, expense, fall risk in older patients, and a taper requirement when you eventually come off. It does not undo the underlying nerve damage. It does not replace the disease-modifying work — controlling blood sugar, addressing nutritional deficiencies, treating the underlying cause when one is identifiable. It is a tool for managing the pain while that other work is happening.
If your neurologist or pain specialist suggests tapentadol after you've worked through the first-line options without enough relief, that's a reasonable medical conversation. If someone is reaching for it without exhausting those options first, slow down and ask why. The opioids belong toward the end of the conversation, not the beginning.
Either way: walk in informed. The medication will do what it does. The patient who understands it walks the rest of the road more steadily.
Frequently Asked Questions
Is tapentadol stronger than tramadol?
Tapentadol is roughly two to three times stronger than tramadol on a milligram-for-milligram basis and carries a higher controlled-substance scheduling (Schedule II versus Schedule IV). It also has cleaner pharmacology than tramadol, meaning it does not depend on a liver enzyme to activate, has lower seizure risk, and has less serotonin-related interaction risk. The two drugs are mechanistically similar — both combine opioid activity with monoamine reuptake inhibition — but tapentadol is the more refined version. For diabetic nerve pain, tapentadol ER is FDA-approved while tramadol use for nerve pain is off-label.
Can I take tapentadol with duloxetine or gabapentin?
Both combinations are used clinically but require care. Tapentadol plus duloxetine produces additive noradrenergic effects, which can raise heart rate and blood pressure and increase nausea, especially during titration. The theoretical serotonin syndrome risk is low because tapentadol has minimal serotonin reuptake inhibition. Tapentadol plus gabapentin or pregabalin is a common combination but increases drowsiness, dizziness, and fall risk, especially in older patients. Either combination should be managed by a prescriber who knows your full medication list and is watching for problems.
How long does it take tapentadol to work for nerve pain?
The immediate-release form starts working within an hour for acute pain. The extended-release form, which is the one used for diabetic neuropathy, typically takes several days to reach a steady level in the body and several weeks to titrate to an effective dose. In the clinical trials, patients were given a three-week titration period to find their dose, and pain reduction continued to improve over the subsequent twelve weeks for patients who responded. If you do not see meaningful improvement after a full titration and 4-6 weeks at an effective dose, the medication probably is not the right tool for you.
Does tapentadol cause withdrawal?
Yes. Physical dependence develops in essentially every patient on long-term tapentadol, and abrupt discontinuation produces withdrawal symptoms within 12 to 24 hours. Withdrawal can include anxiety, sweating, runny nose, restless legs, gut cramping, diarrhea, muscle aches, and significant insomnia. Dependence is different from addiction — it is a normal physiological adaptation, not a behavioral disorder. The standard approach to stopping tapentadol is a gradual taper over weeks, supervised by the prescriber. Never stop tapentadol cold turkey without medical guidance.
Will tapentadol show up on a drug test?
Tapentadol is detectable on specialized opioid screening but typically does not show up on standard 5-panel or 10-panel workplace drug tests that look for morphine, codeine, oxycodone, and heroin metabolites. Tapentadol is structurally different and is usually only detected on tests specifically designed to find it. If you take prescribed tapentadol and need to undergo any kind of testing — pre-employment, court-ordered, sports — bring documentation of your prescription. Always disclose the medication when asked, because failing to disclose a prescribed controlled substance can have its own consequences.
Why is tapentadol so expensive?
Tapentadol remains brand-name only in the United States at most commonly used strengths because generic competition has been delayed by patent litigation and manufacturing complexity. A 30-day supply of Nucynta ER can cost $400 to $800 at retail without insurance. Medicare Part D and most commercial insurance plans cover it but typically require prior authorization, meaning your prescriber must document that you have tried first-line non-opioid options first. Manufacturer copay cards may bring out-of-pocket costs down significantly for commercially insured patients but typically cannot be used with Medicare.
Can tapentadol cause permanent nerve damage?
There is no evidence that tapentadol causes peripheral nerve damage. It is used to treat existing nerve pain, not to cause it. Some opioids in general have been associated with rare hormonal effects with very long-term use, including reduced testosterone and irregular menses, but these are not nerve-related effects. If you develop new neurological symptoms while taking tapentadol — new weakness, new patterns of numbness, sudden changes — report them to your prescriber. They are more likely related to progression of the underlying condition than to the medication itself.
What is the maximum dose of tapentadol ER for diabetic neuropathy?
The FDA-approved maximum dose of Nucynta ER for diabetic peripheral neuropathic pain is 250 milligrams twice daily, for a total of 500 milligrams per day. Most patients who respond to tapentadol find their effective dose somewhere between 100 and 200 milligrams twice daily during the titration. Going above 250 mg twice daily does not reliably add more pain relief in the trials but does add more side effects. If you reach the maximum dose without enough relief, your prescriber will usually consider transitioning to a different approach rather than pushing the dose higher.