Of all the medications that get prescribed for nerve pain, carbamazepine is the one with the most complicated reputation. For one specific kind of nerve pain — trigeminal neuralgia, that lightning-bolt facial pain — it's genuinely a wonder drug. Patients who have spent months unable to brush their teeth or chew on one side of their face describe it as life-changing. For most other neuropathies, it sits further down the list, used after gentler options have been tried.
And carbamazepine — sold under brand names like Tegretol, Tegretol-XR, Carbatrol, and Epitol — comes with a black-box warning that, frankly, scares some people off before they even ask their doctor about it. I want to walk you through the whole picture today: where this drug really shines, where it's a fallback, how the dosing works, what the serious risks actually are, and what the monitoring looks like. By the end, you should know whether it's worth a conversation with your doctor.
What Carbamazepine Is and Why It Works for Nerve Pain
Carbamazepine has been around since the 1960s. It was developed as an anticonvulsant — an epilepsy drug — and the FDA originally approved it for seizures and for trigeminal neuralgia. Later it picked up an indication for bipolar disorder. Everything else, including most of its use for peripheral neuropathy, is technically off-label, even though the practice is widespread enough to be well-supported by clinical guidelines.
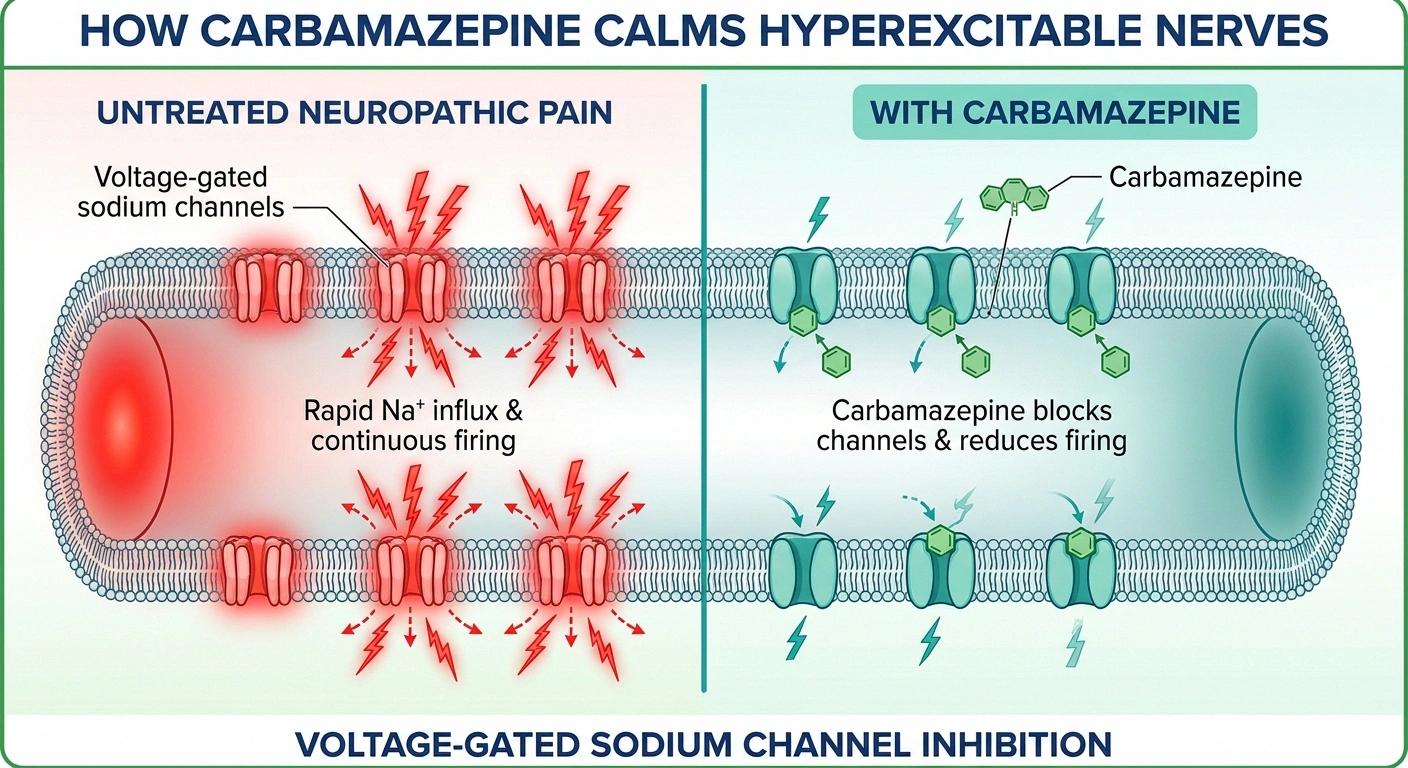
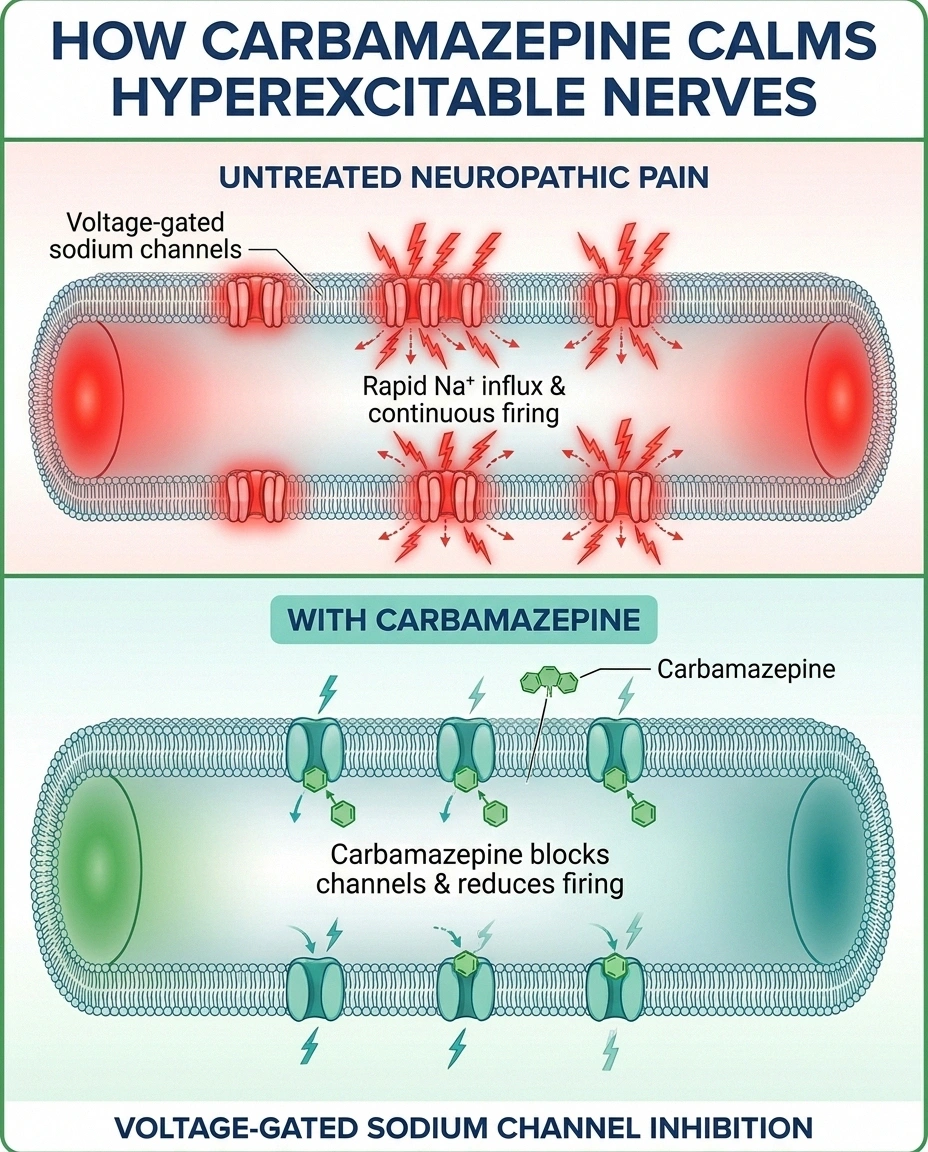
The way it works is what makes it valuable for nerve pain. Damaged nerves don't fire normally. They become hyperexcitable — like a wire with frayed insulation that sparks at the smallest touch. Carbamazepine quiets that hyperexcitability by blocking voltage-gated sodium channels on nerve cells. Sodium channels are how nerves transmit signals; when they fire too easily, you feel pain that isn't matched by what's actually happening to your skin or your muscles. Carbamazepine doesn't kill the nerves or numb anything. It just makes them stop misfiring.
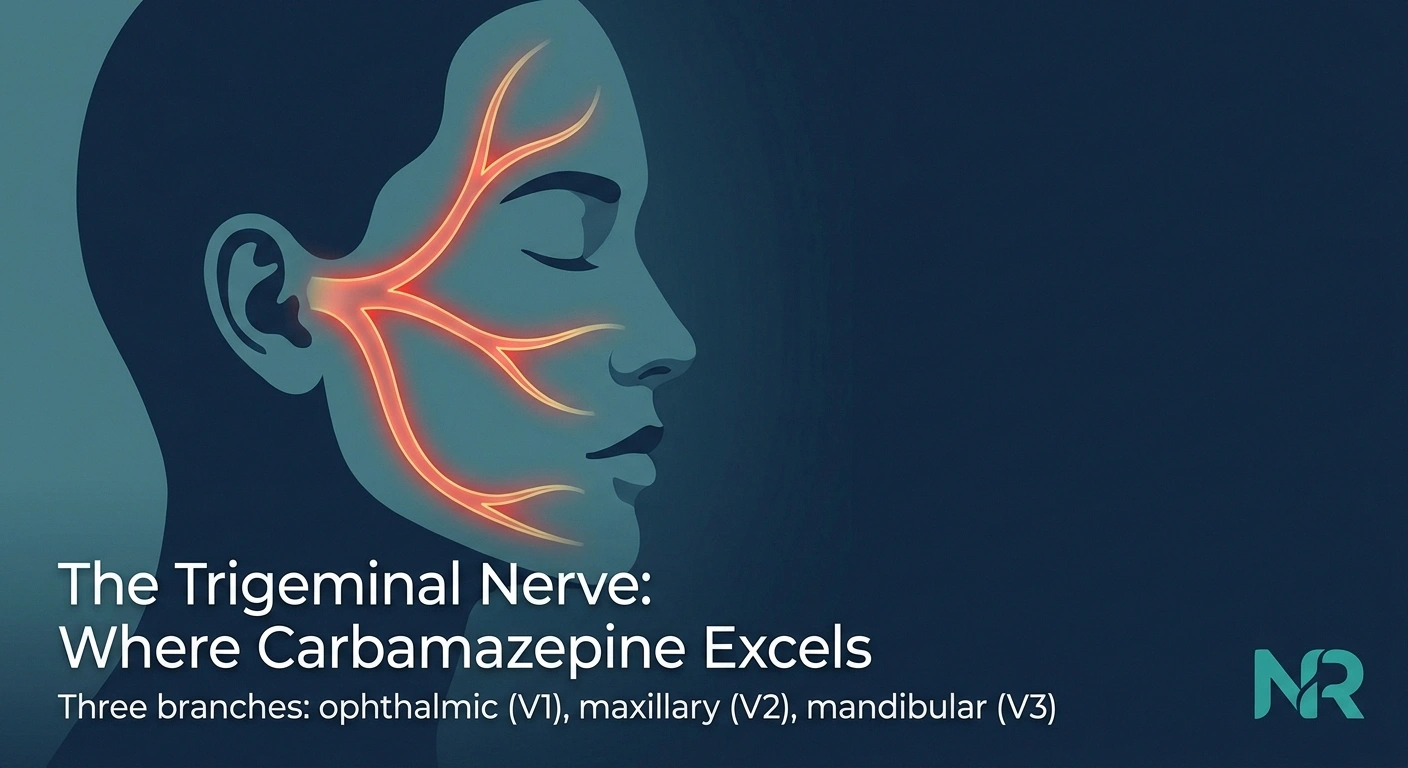
That mechanism is why it works so dramatically for trigeminal neuralgia — a condition where one of the cranial nerves in your face misfires and sends sudden, stabbing pain into your jaw, cheek, or forehead. It's also why doctors reach for it when nerve pain has that same sudden, electric, jolting quality, even when the diagnosis isn't classical trigeminal neuralgia.
Where Carbamazepine Really Shines: Trigeminal Neuralgia
I want to spend a minute here because, for trigeminal neuralgia specifically, carbamazepine is the standard. Every major guideline — the American Academy of Neurology, the European Federation of Neurological Societies — names it first-line. It carries the FDA indication. And in clinical practice, the response rates are striking.
Studies consistently show that around 70 percent of trigeminal neuralgia patients get meaningful pain relief from carbamazepine, often within days of reaching a therapeutic dose. That's an extraordinary number in the pain world. For comparison, most neuropathic pain medications have response rates closer to 40 to 50 percent for the conditions they treat.
If your nerve pain has that signature trigeminal pattern — sudden, brief, electric jolts in your face triggered by light touch, talking, eating, or wind — carbamazepine is the drug your doctor will almost certainly try first. Even if you've been told you have neuropathy of a different sort, if the symptom pattern includes brief lightning-strike sensations, it's worth asking whether a trial of carbamazepine might be appropriate.
Where It Sits for Other Neuropathies
For general peripheral neuropathy — the diabetic, chemotherapy-related, idiopathic, or compression types most readers here are dealing with — carbamazepine is not first-line. The American Academy of Neurology and most pain societies recommend starting with gentler options: gabapentin or pregabalin (Lyrica) in the gabapentinoid class, duloxetine or venlafaxine in the SNRI class, or low-dose amitriptyline or nortriptyline in the tricyclic class.
Where carbamazepine earns its place for non-trigeminal nerve pain is in two specific scenarios. First, when your symptoms include those electric shock-like sensations — the sudden, brief, lightning-strike feelings that gabapentinoids and SNRIs often don't touch. Sodium-channel blockers like carbamazepine are uniquely good at quieting that specific symptom. Second, after you've genuinely tried the first-line options and they haven't worked — when a doctor is reaching past the standard tools and into the next layer.
One worth-mentioning cousin: oxcarbazepine (Trileptal) is a close relative of carbamazepine with a similar mechanism but a noticeably gentler side-effect profile. Many doctors now reach for oxcarbazepine first when they want a sodium-channel blocker, reserving carbamazepine for patients who can't access oxcarbazepine or where the evidence specifically calls for it.
How Doctors Dose It
One of the most important things to understand about carbamazepine is that you do not start at a therapeutic dose. You build up. Starting full-strength is a fast track to dizziness, ataxia, and nausea so bad that patients quit the drug before it has a chance to work.
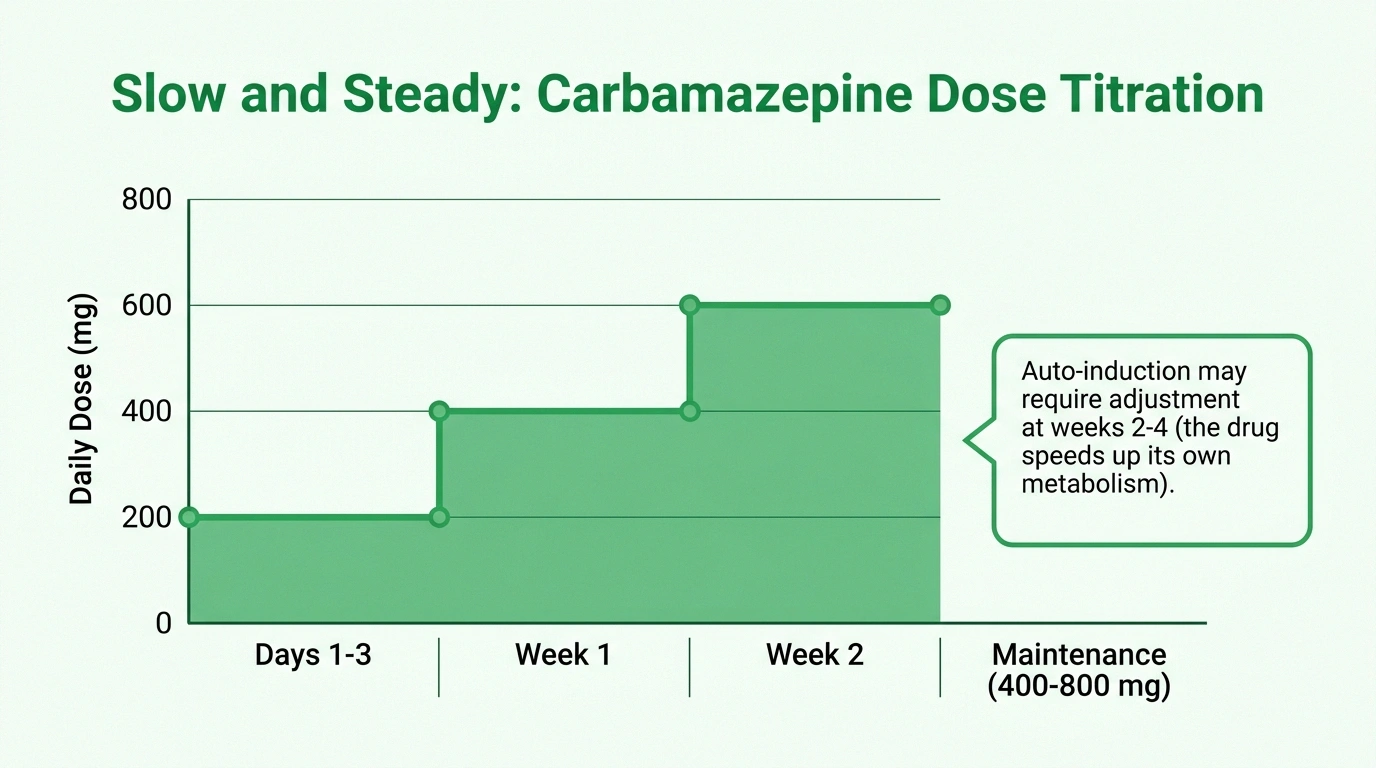
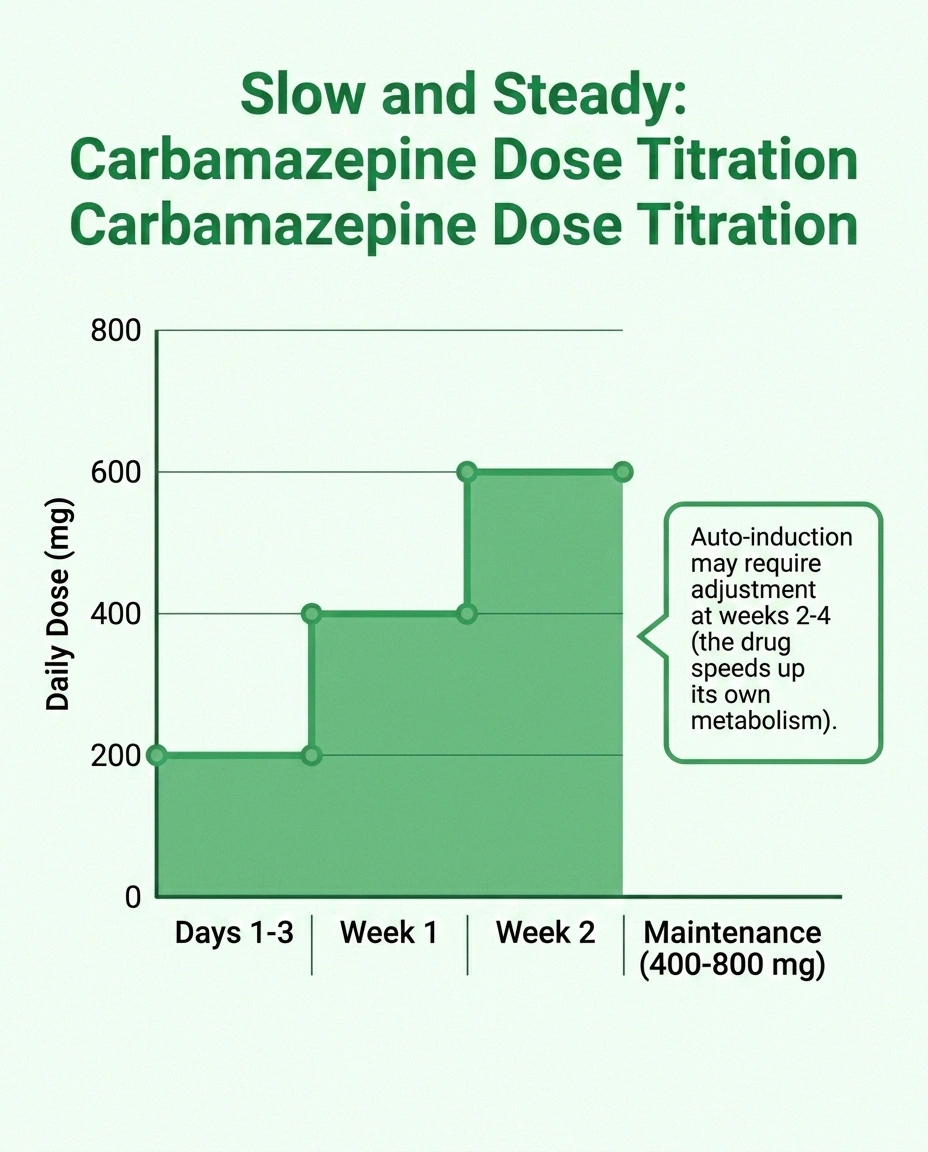
A typical schedule for trigeminal neuralgia or neuropathic pain looks something like this. The first few days, 100 mg twice a day — so 200 mg total per day. Every three or four days, the dose goes up by 100 to 200 mg per day, with the increase split across morning and evening doses. Most patients land somewhere between 400 and 800 mg per day in two or three divided doses. The maximum is generally around 1,200 mg per day, but many patients do well at much lower doses.
The extended-release versions — Tegretol-XR and Carbatrol — are usually dosed twice a day and tend to produce steadier blood levels with fewer peaks and troughs. That can mean fewer side effects for patients who feel the immediate-release version peaking and dropping. If you're going to be on carbamazepine for any length of time, asking about the XR formulation is reasonable.
There's one more quirk worth knowing about. Carbamazepine speeds up its own metabolism — a phenomenon called auto-induction. What that means in practice is that the dose that worked in week 2 may stop working as well by week 4 or 6, because your body is now clearing the drug faster. Doctors anticipate this. It's not failure; it's just the drug's chemistry, and an adjustment to the dose usually solves it.
The Black-Box Warning: What You Actually Need to Know
This is the part of the carbamazepine conversation that puts a lot of people off. The FDA box-warning labels Tegretol with two serious risks: severe skin reactions (Stevens-Johnson syndrome and toxic epidermal necrolysis) and rare blood-count problems. I want to walk through these calmly, because the reality is more manageable than the warning language sometimes makes it sound.
Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN) are catastrophic, full-body skin reactions in which the top layer of skin begins to separate and slough off. They are rare but life-threatening when they happen, and carbamazepine is one of the drugs most commonly associated with them. Critically, the risk is dramatically concentrated in people who carry a specific genetic variant called HLA-B*15:02. That allele is much more common in people of Han Chinese, Thai, Filipino, Malaysian, and South Asian ancestry than in people of European or African ancestry.
This is why the FDA labeling specifically directs doctors to genetic-test for HLA-B*15:02 before starting carbamazepine in patients with Asian ancestry. If the test comes back positive, carbamazepine is generally avoided unless the benefit clearly outweighs the risk. The test is a one-time blood test, increasingly covered by insurance, and it has prevented many serious reactions when it's actually ordered. If you have Asian ancestry and your doctor is considering carbamazepine, ask about HLA-B*15:02 testing before you fill the prescription.
For everyone on carbamazepine, regardless of ancestry, watch for the warning signs in the first 2 to 8 weeks of treatment: a developing rash, mouth sores, fever, sore throat, eye irritation, or any blistering. If any of those appear, stop the medication and call your doctor or get to urgent care the same day. Most rashes are not SJS, but it isn't worth waiting to find out.
Aplastic anemia and agranulocytosis are the blood-count risks named in the box warning. These are also rare but serious — they mean your bone marrow stops making enough blood cells. Doctors monitor with periodic complete blood counts, more frequently in the first few months. Symptoms to watch for include unusual bruising, bleeding gums, persistent infections, and unusual fatigue. If anything like that develops, your doctor needs to know.
DRESS syndrome — Drug Reaction with Eosinophilia and Systemic Symptoms — is another delayed hypersensitivity reaction that can appear 2 to 8 weeks after starting carbamazepine. It looks like a rash, fever, and signs of inflammation in the liver, kidneys, or other organs. Like SJS, it's the kind of thing where stopping the drug fast and getting medical evaluation matters.
The Quieter Risks You Should Also Know About
Beyond the box-warning risks, carbamazepine has a few side effects that are far more common and worth talking about.
Hyponatremia — low blood sodium — is probably the most common medically important side effect, especially in older adults. The drug nudges the kidneys to retain water, which dilutes the sodium in your blood. Mild hyponatremia causes fatigue, brain fog, and headaches; severe hyponatremia can cause confusion, seizures, and worse. Doctors check baseline sodium and recheck periodically, especially in the first few months and any time the dose changes.
Liver enzyme elevations are common but usually mild. Baseline and periodic liver function tests catch the rare cases where the elevation crosses into something needing attention.
Drowsiness, dizziness, and ataxia — the unsteady, off-balance feeling — are extremely common in the first weeks. For most patients, these symptoms fade as the body adjusts, which is why the slow dose-escalation matters so much. For older adults or anyone with existing balance issues, the falls risk during this adjustment period is real, and grab bars, careful walking, and avoiding driving until you know how you respond are reasonable precautions. The connection to neuropathy-related balance problems means this side effect deserves extra respect in our community.
Double vision (diplopia) tends to show up at higher doses and can be a sign that you've hit the ceiling of what your body tolerates.
The Drug Interaction Conversation Most Patients Don't Have
Of all the practical things I want you to know about carbamazepine, this section is the one I'd save and reread. Carbamazepine is one of the most aggressive enzyme inducers in pharmacy. It revs up a liver enzyme called CYP3A4 — and a few others — that metabolize an enormous number of other medications. When it speeds up metabolism, the blood levels of those other medications go down. Sometimes way down.

Drugs whose levels carbamazepine can drop significantly include:
- Hormonal birth control pills — and yes, this can absolutely cause unplanned pregnancies. Many people have had this happen because no one warned them.
- Warfarin and the newer direct oral anticoagulants like apixaban, rivaroxaban, and dabigatran — meaning your blood-thinning effect drops and your clot risk rises.
- Most statins.
- Many antidepressants, including SSRIs and tricyclics.
- Some opioid pain medications.
- Many immunosuppressants used after organ transplants.
- HIV antiretroviral medications.
- Many anti-rejection medications and chemotherapy agents.
The hormonal contraception interaction is the one I want you to walk away remembering. If you take oral birth control pills and start carbamazepine, the pill may stop being reliable. Have a frank conversation with your prescriber and your gynecologist before you start, not after — you may need a non-hormonal backup method, a higher-dose pill, or a different contraceptive entirely. This is one of the most preventable failures in medicine and it happens far too often.
The flip side is also true: many medications affect carbamazepine levels in either direction. Erythromycin, certain antifungals, and grapefruit juice can all raise carbamazepine levels and tip you into toxicity. A pharmacist who knows your full medication list — and not just your prescriber — is the right person to call before starting any new medication while you're on carbamazepine.
What Monitoring Actually Looks Like
If you and your doctor decide carbamazepine is the right call, here's what a reasonable monitoring schedule typically includes.
Before starting: complete blood count, liver function tests, basic metabolic panel (including sodium), and — for patients with Asian ancestry — HLA-B*15:02 genetic testing. For women who could become pregnant, a pregnancy test and a conversation about contraception.
First two months: rechecks of CBC, LFTs, and sodium at 2 and 6 weeks. Higher-frequency monitoring catches the early hyponatremia, the rare blood-count problems, and the liver enzyme rises before they become symptomatic.
Once stable: every 3 to 6 months on the same labs. Doctors may also check a serum carbamazepine level if there's a question about whether the dose is too low (no relief), too high (toxicity), or being affected by an interaction.
That sounds like a lot, but most of it is a quick blood draw your doctor would order anyway for any chronic medication. The bigger commitment is the patient-side awareness — knowing what symptoms to flag, calling fast when something seems off, never adding new medications without checking, and keeping the lab visits.
If You're Already Taking It: A Few Practical Notes
For readers who are already on carbamazepine, a handful of practical points are worth keeping in mind.
Don't stop suddenly. If carbamazepine is part of your seizure control as well as your pain management, stopping abruptly can trigger a seizure even in people who haven't had one in years. If your prescriber decides to stop the drug, it should be tapered down gradually.
Take it with food. Carbamazepine absorbs more reliably and with less nausea when taken with a meal. Most patients tolerate it better split between breakfast and dinner.
Skip the grapefruit juice. Grapefruit blocks the enzymes that metabolize carbamazepine, which can push levels up into toxicity. Stick to other citrus.
Notice the early symptoms of toxicity. If you've been stable and you start feeling unusually unsteady, double-visioned, or extremely drowsy, those are the early signs your level may have crept too high. Call your prescriber — sometimes a new medication, dehydration, or a change in liver function has shifted your blood level.
Always carry your medication list. Especially if you go to a different doctor, the emergency room, or a dentist. Carbamazepine's interaction profile is so broad that it changes which medications are safe to prescribe for anything else you might need.
The Honest Bottom Line
Carbamazepine is one of those medications where the right framing changes everything. For trigeminal neuralgia, it's the gold standard — the first-line treatment, with a remarkable response rate and the potential to genuinely transform someone's quality of life. If you have classical trigeminal neuralgia, carbamazepine should be near the top of the conversation, not buried in it.
For general peripheral neuropathy, it's a second- or third-line option. It earns a look when the pain has that lightning-strike quality, when gentler medications haven't worked, or when a sodium-channel mechanism is suspected. In the broader hierarchy of neuropathic-pain medications, it isn't where most patients start — but it's a real tool when it's needed.
The risks are real and the monitoring matters, but they are also manageable for the patients who genuinely need this medication. A good prescriber will walk you through them, order the right baseline tests, give you a slow-and-steady dose schedule, and stay engaged with the lab work. A great prescriber will also have the contraception conversation up front, ask about your ancestry before deciding on HLA testing, and remind you about the medication-interaction landscape every time something changes.
If carbamazepine is on your treatment list — or if your doctor has raised it as an option — bring this article with you to your next visit. The right questions, asked early, save trouble down the road.
Frequently Asked Questions
How long does it take for carbamazepine to start working?
For trigeminal neuralgia, pain relief often begins within a few days of reaching the right dose — sometimes within 24 to 48 hours. For peripheral neuropathy, the response is generally slower and more modest, with several weeks of titration before you'll have a clear answer. Plan on giving any nerve-pain medication, including carbamazepine, at least 4 to 6 weeks at a therapeutic dose before deciding whether it's helping.
Why does my doctor want a blood test before I start?
Standard baseline labs before starting carbamazepine include a complete blood count, liver function tests, and a basic metabolic panel to check your sodium. These give your doctor a reference point in case anything changes later. If you have Asian ancestry, you should also be tested for the HLA-B*15:02 gene variant, which is strongly linked to severe skin reactions on carbamazepine. The test is a one-time blood draw and increasingly covered by insurance.
What's the difference between carbamazepine and oxcarbazepine?
Oxcarbazepine (Trileptal) is a chemical cousin of carbamazepine with a very similar mechanism but generally a gentler side-effect profile. It tends to cause less drowsiness, less liver enzyme induction, and fewer drug interactions. Many doctors now reach for oxcarbazepine first when they want a sodium-channel blocker, reserving carbamazepine for situations where it's specifically indicated or where oxcarbazepine isn't covered by insurance. Both can cause hyponatremia, and oxcarbazepine actually causes it slightly more often.
Can I drink alcohol on carbamazepine?
Alcohol and carbamazepine both depress the central nervous system, and the combination can intensify drowsiness, dizziness, and falls risk. Alcohol can also affect carbamazepine blood levels and add stress to your liver. Most prescribers recommend either avoiding alcohol entirely or keeping it to very occasional, light use. Talk to your doctor about what's safe for your situation.
Will carbamazepine make me drowsy?
Often, yes — especially during the first few weeks while your body is adjusting to the dose. The drowsiness usually fades within 2 to 4 weeks. During the adjustment period, don't drive or operate machinery until you know how the medication affects you, and be especially cautious about falls. Patients with neuropathy already have a higher falls risk, and the drowsiness from any new medication compounds it.
What should I do if I miss a dose?
If you remember within a few hours of your usual time, take the missed dose. If it's close to the time for the next dose, skip the missed one and take the next dose as scheduled — don't double up. Missing one dose occasionally won't usually cause problems, but missing multiple doses can drop your blood level enough that pain control breaks through. Set phone alarms or use a weekly pillbox to help with consistency.
Can carbamazepine cause weight gain?
Compared to gabapentin and pregabalin, carbamazepine is less likely to cause weight gain. Some patients do report a modest increase, but it's not a defining feature of the medication. If weight changes are a major concern for you when choosing among neuropathy medications, this is a reasonable thing to ask your prescriber about.
How long can I stay on carbamazepine?
Patients are routinely on carbamazepine for years, especially when treating trigeminal neuralgia or seizures. With consistent monitoring — periodic blood counts, sodium checks, and liver function tests — long-term use is generally manageable. Some patients eventually try to taper down if their pain has stabilized; others stay on a steady maintenance dose indefinitely. The right answer depends on the underlying condition and how the medication is performing for you.


