
Celiac Disease and Neuropathy: How Gluten Damages Nerves
If you've been diagnosed with celiac disease and are experiencing tingling, numbness, or burning in your hands and feet, you're not imagining things — and it's not just anxiety. Research consistently shows that peripheral neuropathy is one of the most common neurological complications of celiac disease, affecting an estimated 10% of celiac patients. Yet many people go years without connecting their nerve symptoms to their gut condition.
The relationship between gluten and nerve damage is more complex than most people realize. It involves nutrient malabsorption, autoimmune attacks on nerve tissue, and inflammatory processes that can damage nerves even before the classic digestive symptoms of celiac disease appear. Understanding this connection can help you get the right diagnosis, protect your nerves, and make sense of symptoms your doctors may have been treating in isolation.
The Celiac-Neuropathy Connection: What We Know
Celiac disease is an autoimmune condition in which eating gluten — a protein found in wheat, barley, and rye — triggers an immune response that damages the lining of the small intestine. The tiny finger-like projections called villi that line the intestine become flattened and inflamed, which impairs the body's ability to absorb nutrients from food.
The neurological complications of celiac disease have been recognized since the 1960s, but research has accelerated significantly in recent decades. A landmark study published in the journal Neurology by researchers at Columbia University found that celiac disease was present in approximately 2.5% of all neuropathy patients evaluated at their center — and in 8% of patients with neuropathy that had normal nerve conduction studies (suggesting small fiber neuropathy).
A large Swedish population-based study published in JAMA Neurology followed over 28,000 biopsy-verified celiac disease patients and found a significantly elevated risk of developing neuropathy after diagnosis — with the risk being most pronounced in the first five years. The three most common neuropathy types seen in celiac patients were chronic inflammatory demyelinating polyneuropathy (CIDP), autonomic neuropathy, and mononeuritis multiplex.
How Gluten Damages Nerves: Three Pathways
The nerve damage in celiac disease isn't caused by a single mechanism. Research points to at least three overlapping pathways, and you may be affected by more than one simultaneously:
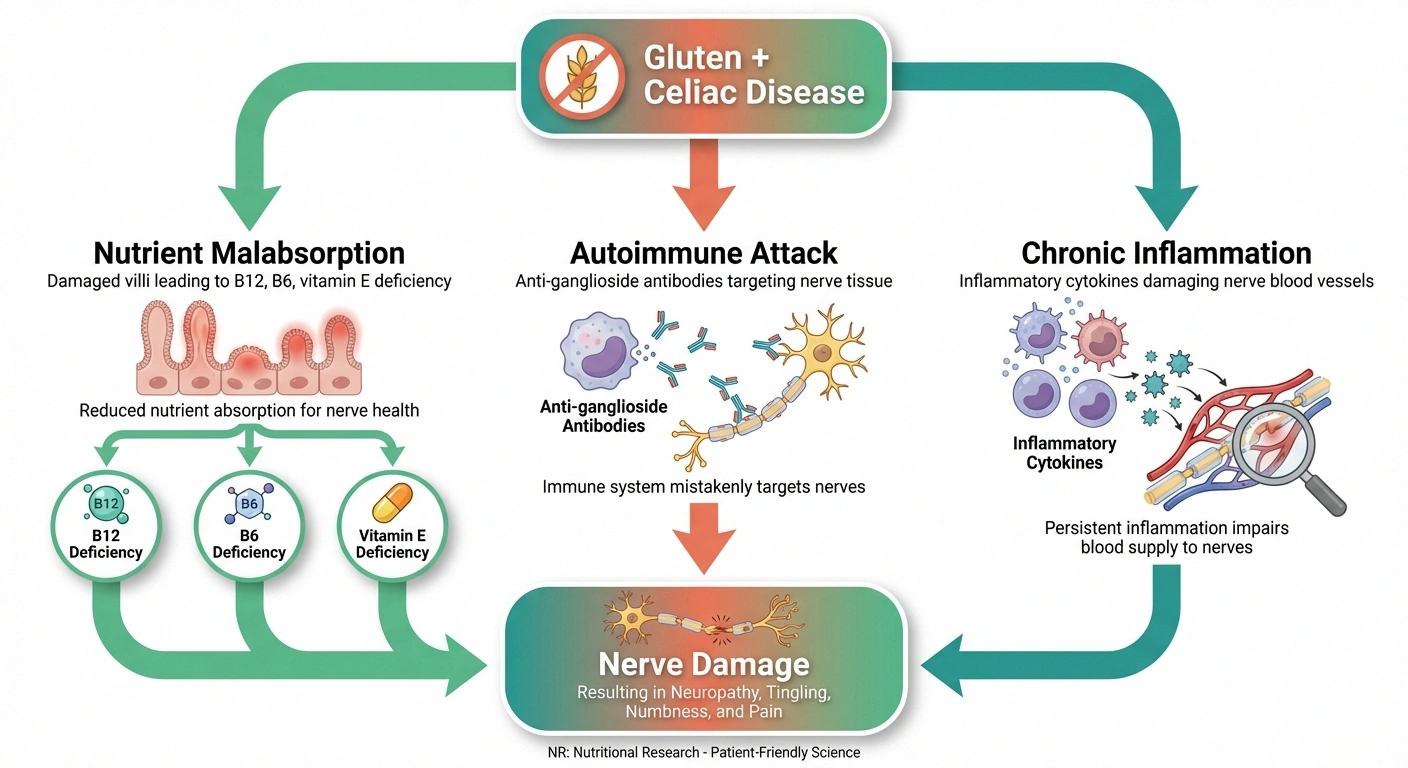
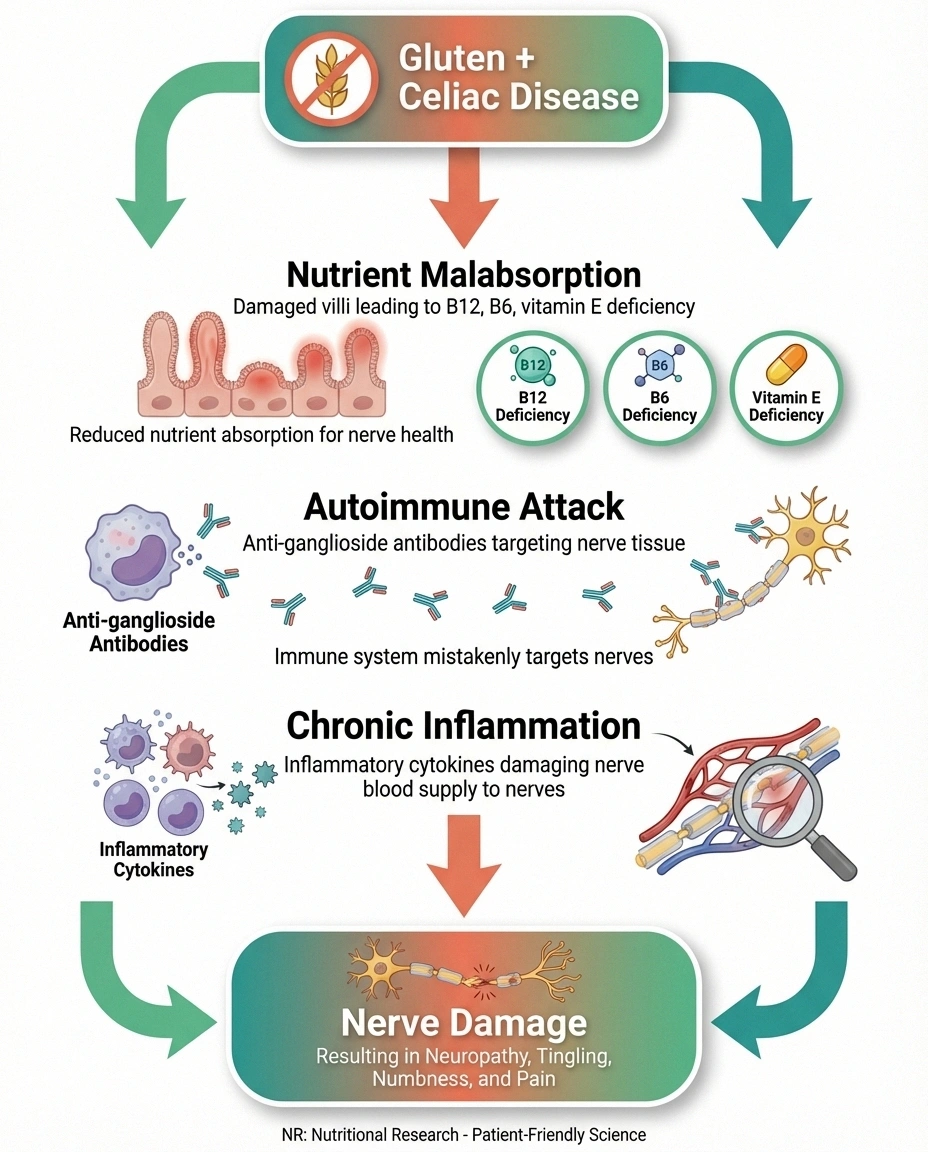
Pathway 1: Nutrient Malabsorption
Damaged intestinal villi can't absorb nutrients properly, leading to deficiencies in vitamins and minerals that are critical for nerve health. The most relevant deficiencies include:
- Vitamin B12 — essential for maintaining the myelin sheath that insulates nerve fibers. B12 deficiency is one of the most well-established causes of peripheral neuropathy and is common in celiac patients due to impaired absorption in the ileum (lower small intestine).
- Vitamin B6 (pyridoxine) — involved in neurotransmitter synthesis and nerve signal transmission. Both deficiency and excess of B6 can cause neuropathy.
- Vitamin B1 (thiamine) — critical for nerve cell energy metabolism. Thiamine deficiency causes beriberi, which includes polyneuropathy as a primary symptom.
- Vitamin E — an antioxidant that protects nerve cell membranes. Severe vitamin E deficiency (which can result from fat malabsorption in celiac disease) causes a progressive neuropathy.
- Copper — less commonly discussed but increasingly recognized as a cause of neuropathy when deficient. Celiac-related malabsorption can deplete copper stores.
This nutrient pathway is the most straightforward to address: identify the deficiency, supplement it, and the nerve damage may stabilize or even partially reverse — especially if caught early.
Pathway 2: Autoimmune Attack on Nerves
Celiac disease is an autoimmune condition, and autoimmune diseases tend to cluster. The same immune dysregulation that causes your body to attack intestinal villi in response to gluten can also generate antibodies that attack nerve tissue directly.
Research has identified anti-ganglioside antibodies in up to 65% of celiac patients with neuropathy. Gangliosides are components of nerve cell membranes, and antibodies against them can directly damage peripheral nerves. This autoimmune mechanism helps explain why some celiac patients develop neuropathy even without significant nutrient deficiencies — their immune system is directly targeting nerve tissue.
This pathway also explains why strict adherence to a gluten-free diet is essential beyond just gut healing: reducing the autoimmune trigger (gluten) may reduce the production of these nerve-damaging antibodies over time.
Pathway 3: Chronic Inflammation
Celiac disease creates a state of chronic systemic inflammation that extends beyond the gut. Elevated inflammatory cytokines (particularly TNF-alpha, interleukin-6, and interleukin-1beta) circulate throughout the body and can damage the small blood vessels (vasa nervorum) that supply peripheral nerves with oxygen and nutrients. When these tiny vessels become inflamed or damaged, the nerves they feed begin to deteriorate.
This vasculitic mechanism may explain why some celiac patients develop mononeuritis multiplex — a pattern of nerve damage that affects individual nerves in a patchy, asymmetrical distribution, consistent with focal blood vessel damage.
Symptoms of Celiac Neuropathy
The neuropathy associated with celiac disease typically presents as a sensory-predominant polyneuropathy, meaning it primarily affects your ability to feel rather than your ability to move. The most common symptoms include:

- Tingling, numbness, or “pins and needles” in the hands and feet
- Burning or stinging pain, especially in the feet
- A feeling of wearing invisible socks or gloves
- Increased sensitivity to touch (allodynia)
- Balance problems, particularly in the dark
- Difficulty with fine motor tasks like buttoning clothes
A particularly important finding: in some patients, neuropathic symptoms appear before the classic gastrointestinal symptoms of celiac disease. The Celiac Disease Foundation notes that peripheral neuropathy may be the presenting symptom that leads to a celiac diagnosis in some patients. This is why neuropathy experts increasingly recommend testing for celiac disease in patients with unexplained neuropathy, especially when other common causes have been ruled out.
Small Fiber Neuropathy: The Most Common Type in Celiac Disease
The Columbia University study found that a significant proportion of celiac neuropathy patients had normal nerve conduction studies but abnormal skin biopsies — indicating small fiber neuropathy (SFN). Small fiber neuropathy affects the thin, unmyelinated nerve fibers responsible for pain, temperature sensation, and autonomic function.
This is clinically important because small fiber neuropathy doesn't show up on standard nerve conduction tests. If your doctor orders a standard EMG/NCS and it comes back normal, that doesn't mean you don't have neuropathy. A skin biopsy measuring intraepidermal nerve fiber density (IENFD) is the gold standard for diagnosing SFN.
Who Should Be Tested?
Given the significant overlap between celiac disease and neuropathy, testing for celiac disease should be considered in specific clinical scenarios:
- Unexplained neuropathy — if you have neuropathy and no clear cause has been identified (idiopathic neuropathy), celiac testing is warranted. The Columbia study found celiac in 2.5% of all neuropathy patients, making it a more common cause than many neurologists realize.
- Small fiber neuropathy with normal nerve conduction — the 8% prevalence rate in this subgroup makes celiac testing especially important
- Neuropathy plus GI symptoms — any combination of neuropathy with chronic diarrhea, bloating, weight loss, or abdominal pain should prompt celiac screening
- Neuropathy plus nutrient deficiencies — unexplained vitamin deficiencies (especially B12, folate, iron, or vitamin D) alongside neuropathy may indicate malabsorption
- Family history of celiac disease — first-degree relatives of celiac patients have a 10-15% chance of having the condition
- Neuropathy with other autoimmune conditions — if you already have Type 1 diabetes, thyroid disease, or another autoimmune condition plus neuropathy, celiac screening is appropriate
Diagnosis: Testing for Celiac Disease
The diagnostic process for celiac disease involves blood tests and, in most cases, an intestinal biopsy:
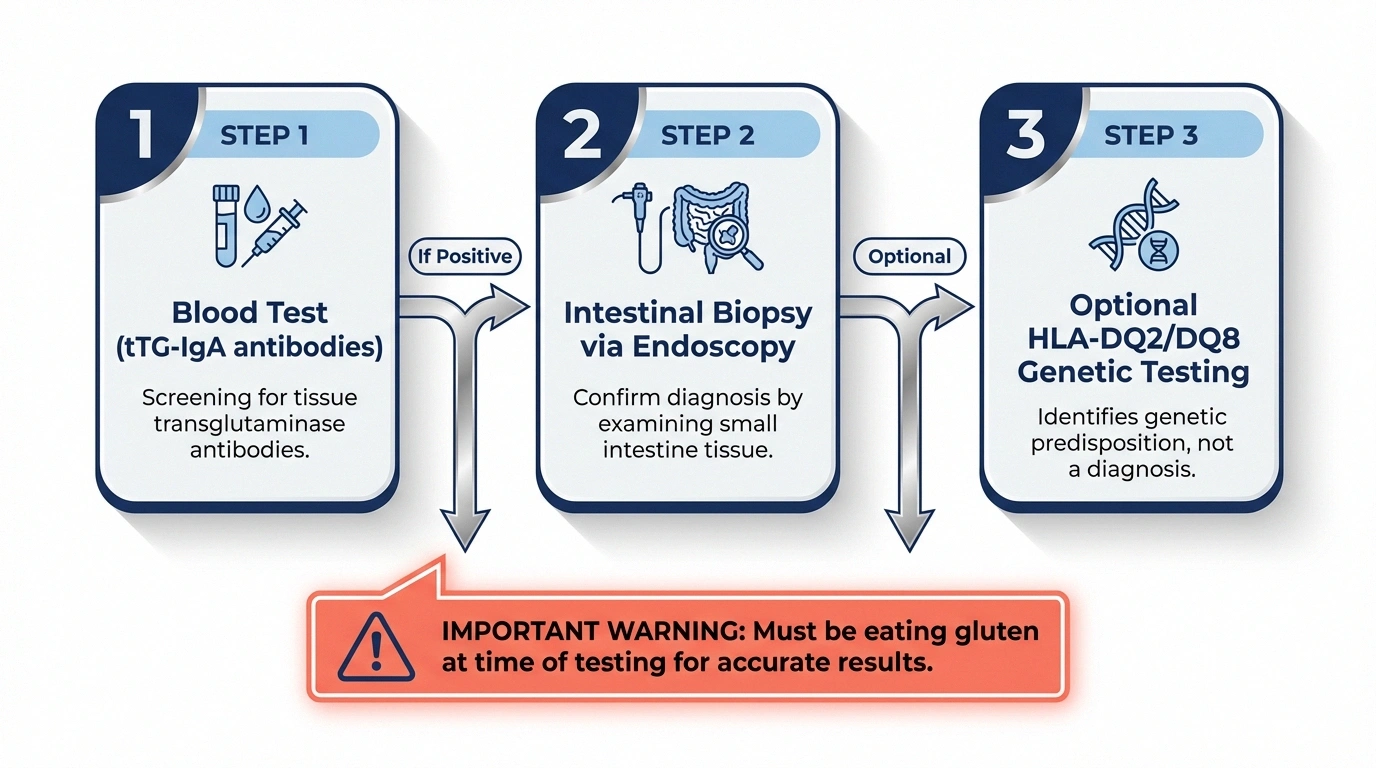
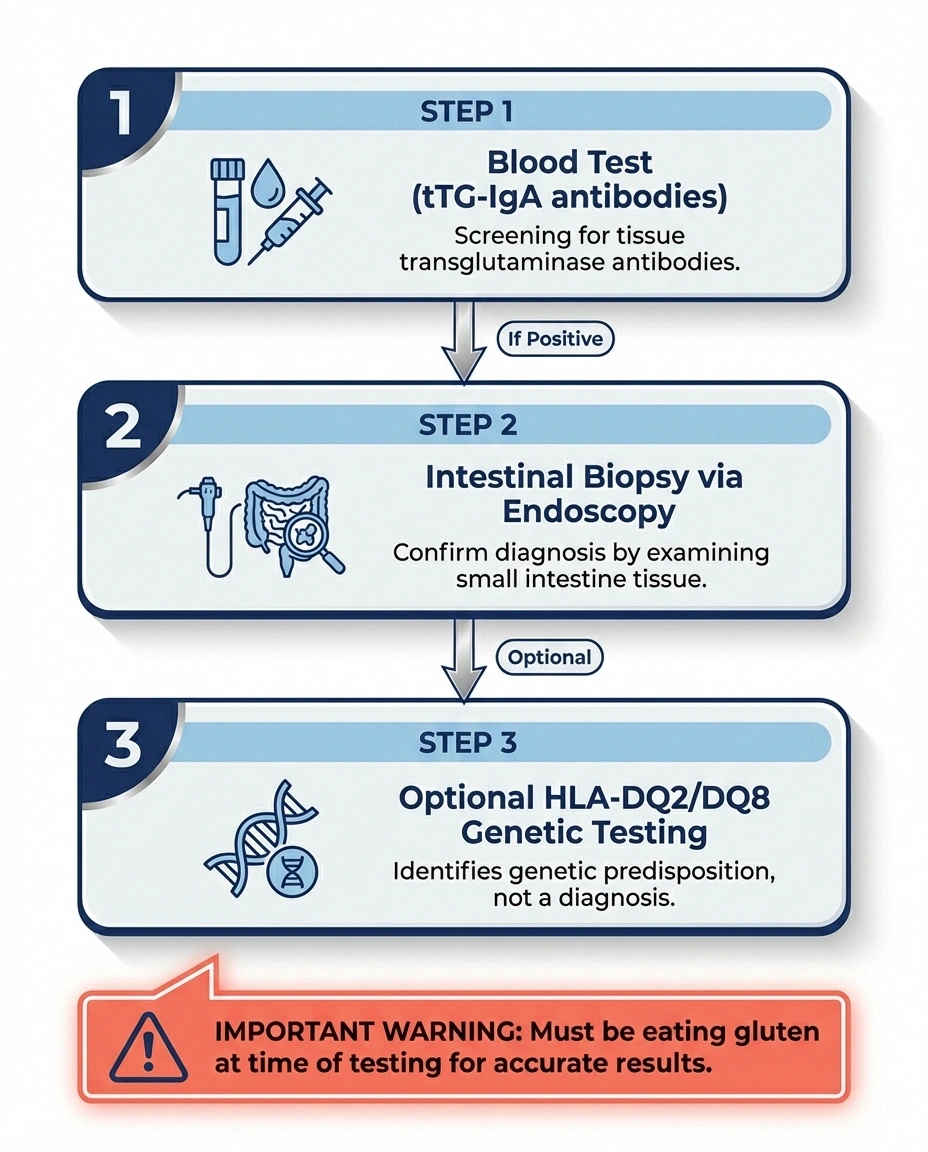
Blood tests (serology): The initial screening involves testing for tissue transglutaminase antibodies (tTG-IgA) and total IgA levels. The tTG-IgA test is highly sensitive and specific for celiac disease. Deamidated gliadin peptide (DGP) antibodies may also be tested, particularly in patients with IgA deficiency.
Important: You must be eating gluten at the time of testing for accurate results. If you've already started a gluten-free diet, the antibody levels may have dropped to normal, producing a false negative. Doctors typically recommend eating gluten for at least 6-8 weeks before testing.
Intestinal biopsy: If blood tests are positive, an upper endoscopy with small intestinal biopsy is the gold standard for confirming the diagnosis. The biopsy looks for villous atrophy (flattened or damaged villi) — classified by the Marsh scoring system, with Marsh 3 (villous atrophy with crypt hyperplasia) being diagnostic of celiac disease.
Genetic testing: HLA-DQ2 and HLA-DQ8 genetic markers are present in virtually all celiac patients. However, these genes are also present in about 30-40% of the general population, so a positive genetic test doesn't confirm celiac disease — it only confirms susceptibility. A negative genetic test, however, essentially rules out celiac disease.
Treatment: Protecting Your Nerves
If you have celiac disease and neuropathy, treatment targets multiple pathways simultaneously:
Strict Gluten-Free Diet
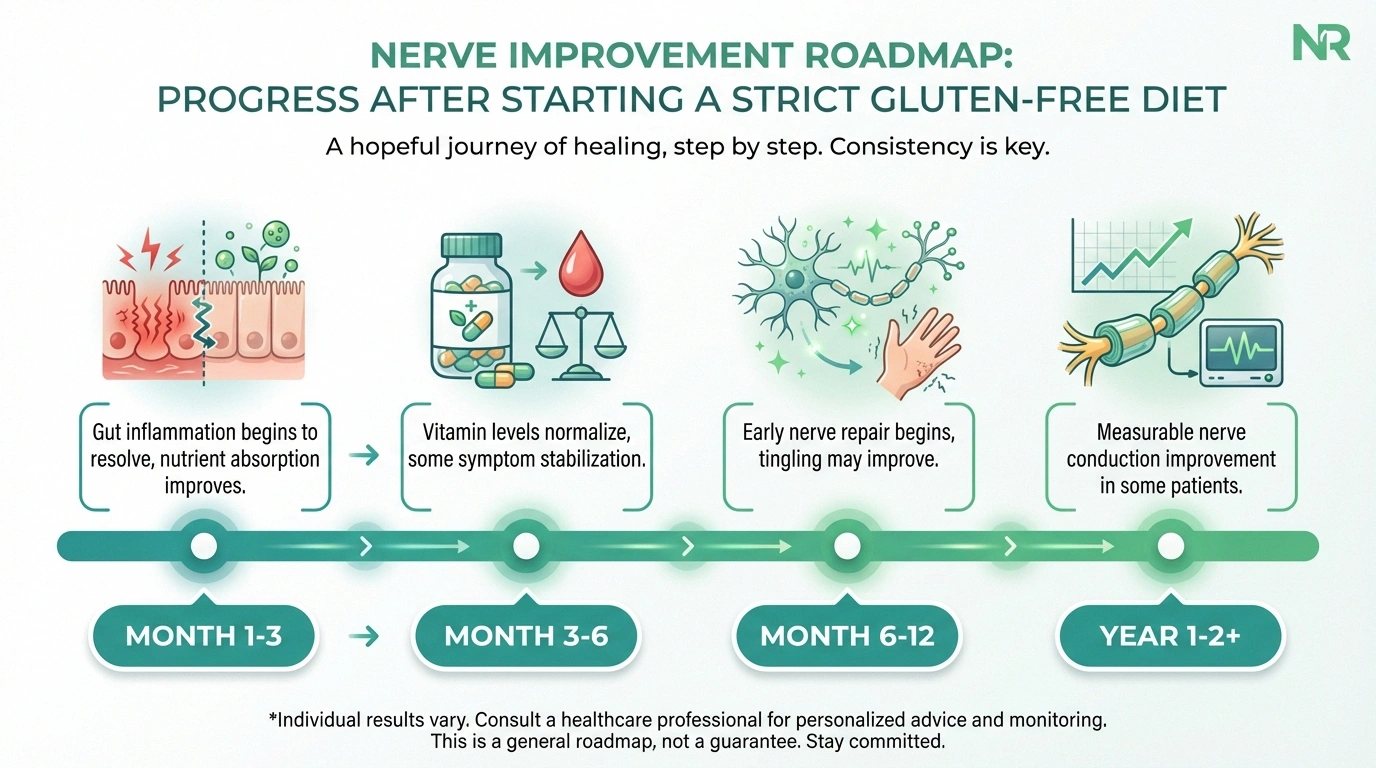
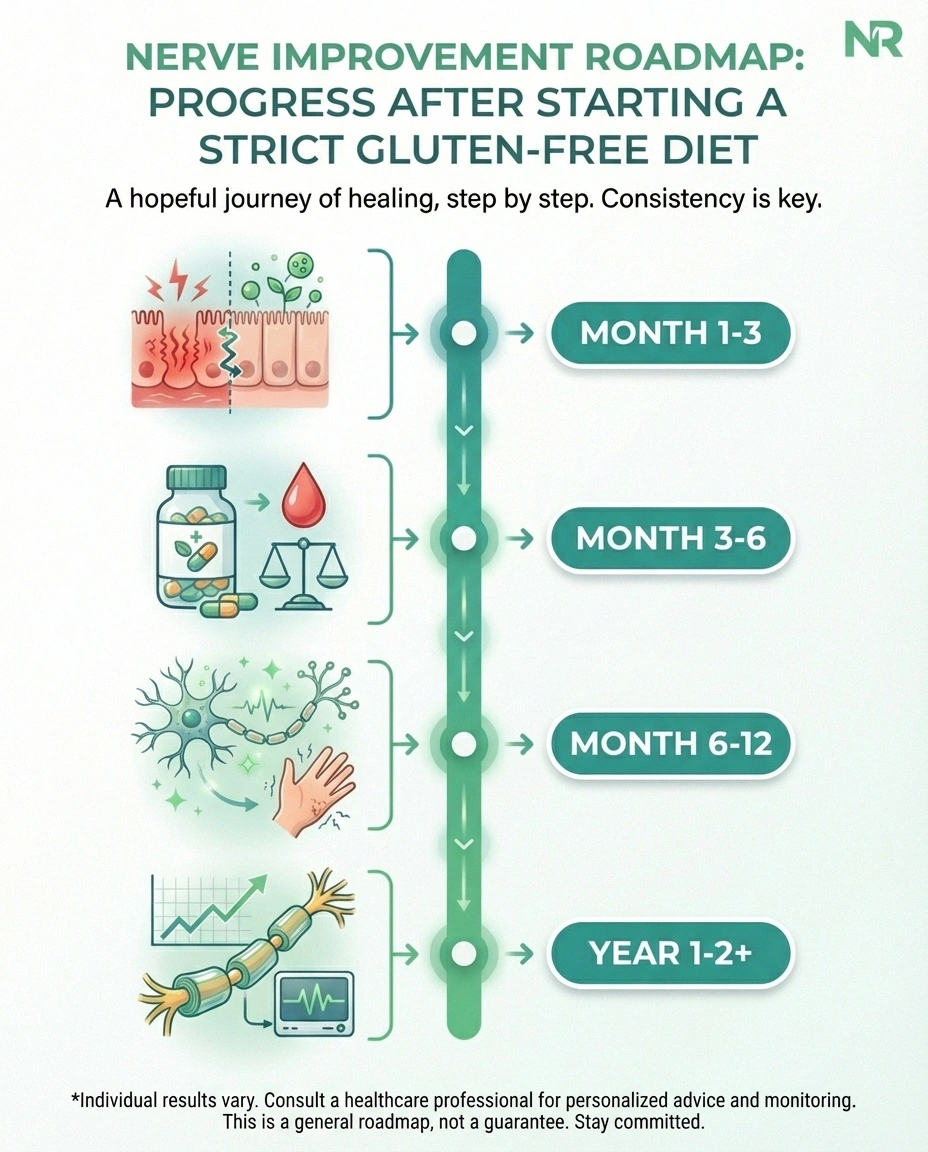
A lifelong, strict gluten-free diet is the foundational treatment for celiac disease. For neuropathy specifically, the gluten-free diet serves two purposes: it allows the intestinal lining to heal (restoring nutrient absorption) and it reduces the autoimmune inflammatory cascade that may be directly attacking nerves.

The Celiac Disease Foundation notes that while a gluten-free diet may not completely prevent neuropathy from developing, it appears to slow the progression of neuropathic symptoms. The earlier you achieve strict gluten elimination, the better your chances of stabilizing or improving nerve function.
“Strict” means strict. Even small amounts of gluten — as little as 50 milligrams (about 1/100th of a slice of bread) — can trigger the immune response and intestinal damage. This means reading every food label, being careful about cross-contamination in kitchens, and learning which ingredients contain hidden gluten.
Nutrient Repletion
Correcting nutrient deficiencies is critical. Your doctor should test levels of B vitamins (especially B12, B6, and folate), vitamin E, vitamin D, iron, copper, and zinc. Supplementation should be guided by documented deficiencies, not guesswork — both deficiency and excess of certain vitamins (particularly B6) can cause neuropathy.
For B12 deficiency, injections may be necessary initially since oral supplementation depends on intestinal absorption, which is impaired in active celiac disease. As the intestinal lining heals on a gluten-free diet, absorption typically improves and oral supplementation may become sufficient.
Neuropathy Symptom Management
While the gluten-free diet and nutrient repletion address the root causes, you may still need treatment for neuropathy symptoms. Standard neuropathy medications like gabapentin, pregabalin, or duloxetine can help manage pain. Topical treatments like capsaicin cream or lidocaine patches may provide additional relief. Physical therapy for balance and strength is also recommended, especially if neuropathy is affecting your gait.
Immunotherapy for Refractory Cases
In cases where neuropathy progresses despite strict gluten elimination and nutrient correction, immunotherapy may be considered. This is more common when the neuropathy pattern suggests an active autoimmune process (particularly CIDP or mononeuritis multiplex). Options may include intravenous immunoglobulin (IVIG), plasma exchange, or corticosteroids, depending on the specific neuropathy subtype.
Non-Celiac Gluten Sensitivity and Neuropathy
An area of active research is the link between gluten sensitivity (without celiac disease) and neuropathy. Some people test negative for celiac disease antibodies and have normal intestinal biopsies, yet experience neurological symptoms including peripheral neuropathy that improve on a gluten-free diet.
Researchers at the Royal Hallamshire Hospital in Sheffield, UK — led by Dr. Marios Hadjivassiliou, one of the foremost experts on gluten-related neurological disease — have proposed the term “gluten neuropathy” to describe peripheral neuropathy associated with anti-gliadin antibodies in the absence of celiac disease. Their research suggests that gluten sensitivity can damage nerves through direct immune mechanisms even without intestinal involvement.
This remains somewhat controversial, and not all neurologists accept gluten sensitivity as a proven cause of neuropathy. However, if you have unexplained neuropathy and elevated anti-gliadin antibodies, a monitored trial of a gluten-free diet — with documented neurological assessment before and after — may be worth discussing with your doctor.
Living With Celiac Disease and Neuropathy
Managing both conditions simultaneously requires attention to multiple fronts:

- Diet compliance monitoring: Regular follow-up with your gastroenterologist to check tTG antibody levels and ensure intestinal healing. Persistent antibody elevation may indicate hidden gluten exposure.
- Nutrient monitoring: Annual blood work to check B12, folate, iron, vitamin D, and other nutrients, with more frequent testing if deficiencies are identified.
- Neurological follow-up: Periodic neurological assessment to track whether neuropathy is stable, improving, or progressing. This helps guide treatment decisions and catch any new developments early.
- Foot care: If neuropathy affects sensation in your feet, daily foot inspections and proper footwear are essential to prevent unnoticed injuries.
- Emotional support: Managing a strict gluten-free diet while living with chronic nerve pain is genuinely difficult. Support groups for both celiac disease and neuropathy can provide practical tips and emotional validation. The emotional impact of chronic pain shouldn't be minimized or ignored.
Frequently Asked Questions
Can celiac disease cause neuropathy even without digestive symptoms?
Yes. In some patients, neuropathy and other neurological symptoms appear before any gastrointestinal symptoms develop. Studies have shown that peripheral neuropathy can be the presenting symptom of celiac disease, sometimes preceding digestive complaints by years. This is why unexplained neuropathy should prompt celiac testing even when digestive symptoms are absent.
Will a gluten-free diet reverse my neuropathy?
A gluten-free diet may stabilize neuropathy and slow progression, and in some cases symptoms partially improve, especially when nutrient deficiencies are corrected. However, nerve damage that has already occurred may not fully reverse. The earlier celiac disease is diagnosed and treated, the better the chances of preserving nerve function. Strict dietary compliance is essential for the best possible outcome.
How common is neuropathy in celiac disease?
Approximately 10 percent of celiac disease patients develop neurological complications, with peripheral neuropathy and ataxia being the most common. Among patients evaluated at specialized neuropathy clinics, celiac disease is found in about 2.5 percent of all neuropathy cases and up to 8 percent of small fiber neuropathy cases.
Should I get tested for celiac disease if I have unexplained neuropathy?
Yes, especially if no other cause for your neuropathy has been identified. Testing is a simple blood draw for tissue transglutaminase antibodies. Given the treatable nature of celiac disease and its underdiagnosis in the United States, where approximately 83 percent of cases are undiagnosed, screening neuropathy patients is considered good clinical practice by many neurologists.
What type of neuropathy does celiac disease usually cause?
The most common pattern is a sensory-predominant polyneuropathy with pain, tingling, and numbness in the hands and feet. Small fiber neuropathy is particularly common. Other patterns seen in celiac patients include autonomic neuropathy, chronic inflammatory demyelinating polyneuropathy, and mononeuritis multiplex.
Can gluten sensitivity cause neuropathy without celiac disease?
Research suggests it may. Some patients with anti-gliadin antibodies but without celiac disease develop neuropathy that improves on a gluten-free diet. This is sometimes called gluten neuropathy. The evidence is still emerging, but if you have unexplained neuropathy and elevated anti-gliadin antibodies, a supervised trial of gluten elimination may be worth discussing with your neurologist.
Taking Action
The connection between celiac disease and neuropathy is well-established but still underrecognized. An estimated 83% of Americans with celiac disease are undiagnosed or misdiagnosed, according to the Foundation for Peripheral Neuropathy — and some of those people are being treated for “unexplained neuropathy” when a treatable cause is sitting right there, waiting to be found.

If you have celiac disease, pay attention to nerve symptoms and report them to your doctor. If you have unexplained neuropathy, ask about celiac testing — it's a simple blood draw that could change everything. And if you've been diagnosed with both, commit to the strictest possible gluten-free diet, get your nutrient levels tested and corrected, and work with both a gastroenterologist and a neurologist to manage both conditions comprehensively.
Your nerves and your gut are more connected than most people realize. Understanding that connection puts you in the best position to protect both.


