
The first time my pain doctor wrote me a prescription for something called “compounded cream,” I had no idea what to expect. I picked up a small white tube at a specialty pharmacy that wasn't my regular drugstore. The label listed four active ingredients and a price tag that made me blink — $87, not covered by insurance. I went home, dabbed it on my feet, and waited to see if it worked.
That little tube turned into one of the most confusing conversations I've had with people in my support group. Some swear by their compounded cream. Others spent hundreds of dollars on tubes that did nothing. Some doctors enthusiastically prescribe them; others won't touch them. Insurance companies generally won't pay for them. And the research has produced wildly different results.
If you're trying to figure out whether a compounded pain cream is worth a try, this guide is the honest version. We'll walk through what these creams actually are, what's in them, what the evidence says (it's nuanced), what the safety considerations look like, and how to decide whether to bring it up with your doctor. The goal isn't to sell you on the idea or scare you off it — it's to help you make a real-information decision.
What “Compounded” Actually Means

A compounded medication is one that's mixed, by hand, at a specialty pharmacy according to a prescription written for you specifically. Unlike a manufactured drug — where every tube of the same brand contains the same ingredients in the same concentrations — a compounded cream is made to order. Your doctor writes the formula. The pharmacist mixes it.
That's the entire definition. There's nothing magic or mysterious about compounding itself. Pharmacists have been compounding medications for hundreds of years, well before mass-manufactured drugs existed. Compounding is still common when a patient needs a dose that isn't manufactured, an allergen-free version of something, a liquid for someone who can't swallow pills, or a custom topical formulation that combines several ingredients in one cream.
For neuropathy, the appeal is exactly that last category. Instead of taking three or four oral medications systemically (where they affect your whole body, including the parts that don't hurt), you can apply a single topical cream that delivers several active ingredients directly to the painful skin. In theory, that means more pain relief at the location and less side effect burden everywhere else.
In practice, the picture is more complicated. Active ingredients have to actually penetrate the skin to do anything. Some do well, some poorly. And mixing several ingredients into one base doesn't always preserve the effectiveness of each. This is the gap between the theory and the evidence — and it matters when you're spending real money out of pocket.
What's Usually in a Compounded Neuropathy Cream
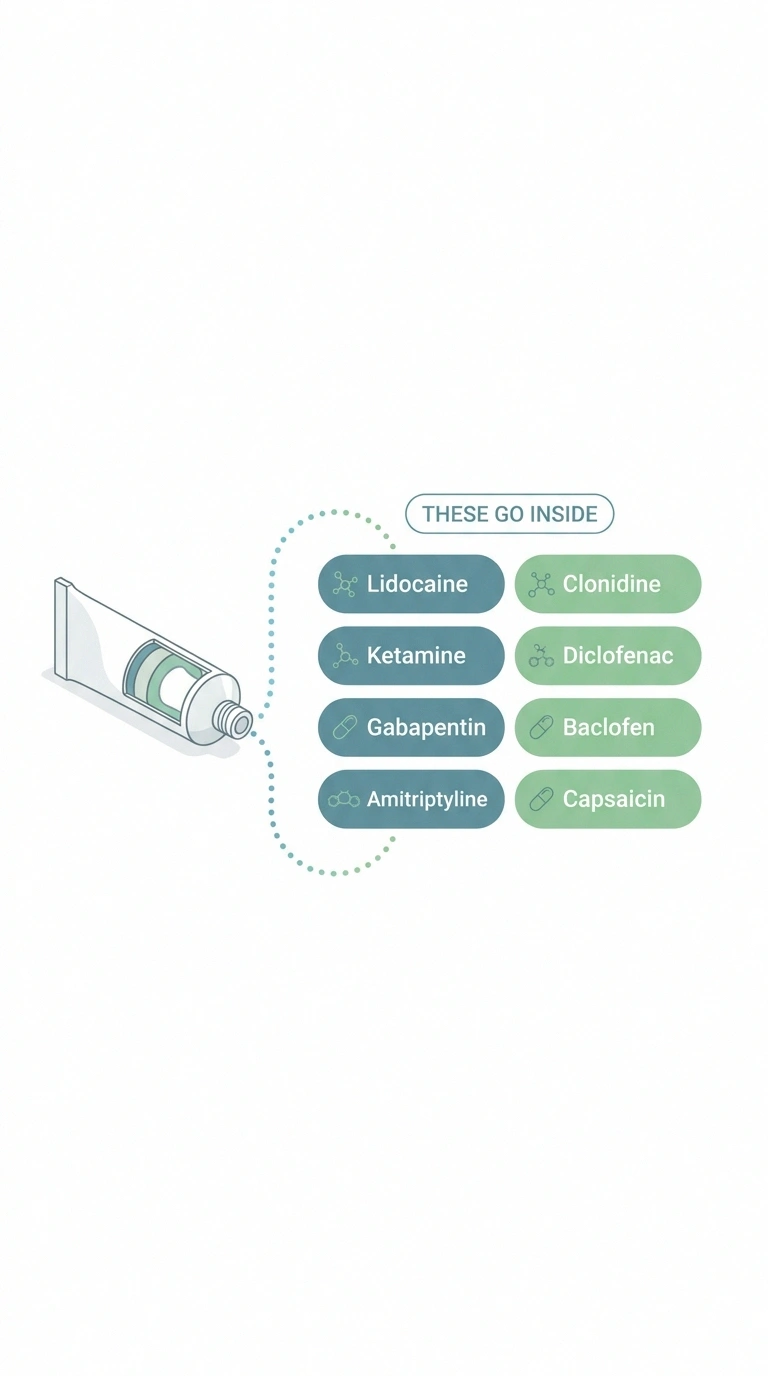
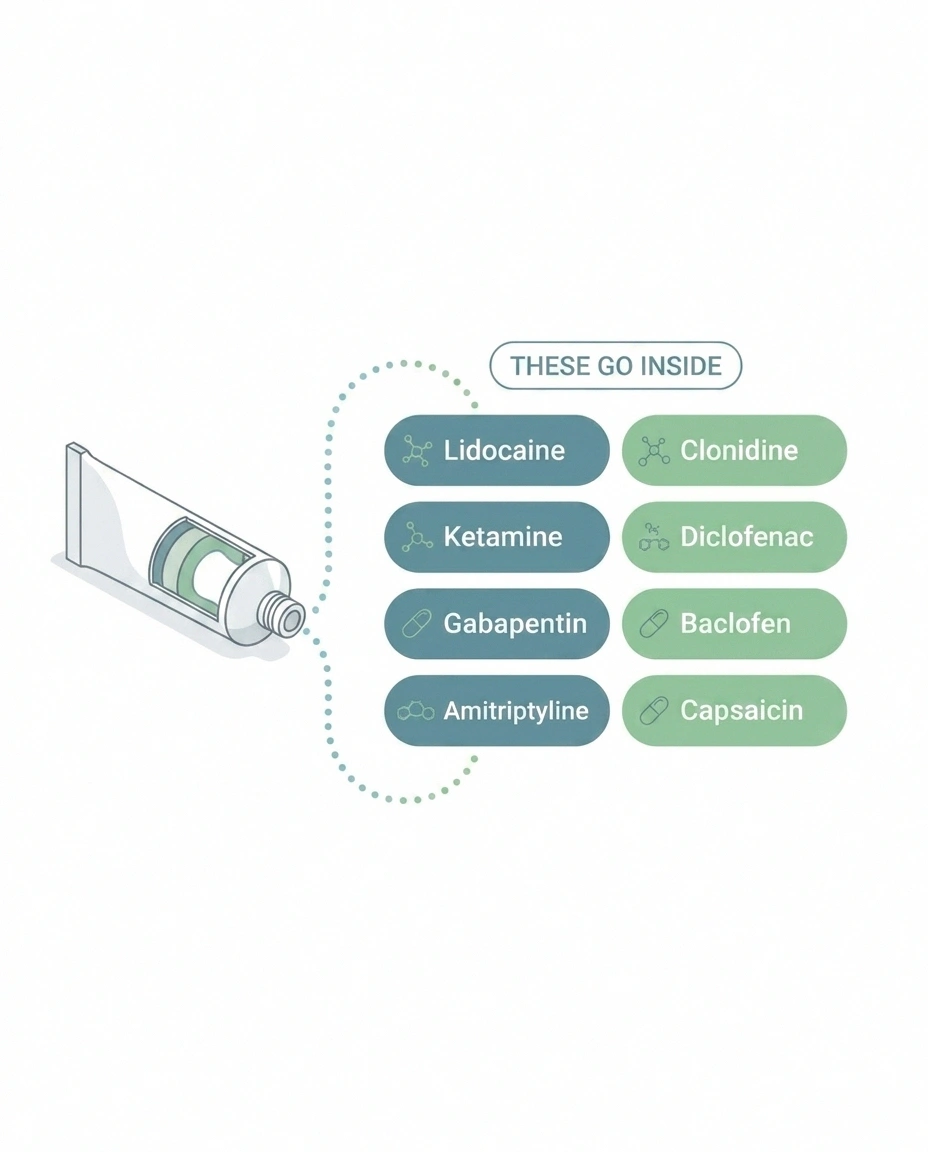
The ingredient mix varies, but most compounded neuropathy creams pull from a fairly small list. Each ingredient targets a different mechanism of nerve pain, and the formula is built around what your specific pain looks like.
Common Compounded Cream Ingredients
| Ingredient | What It Does | Typical % |
|---|---|---|
| Lidocaine | Numbs the area by blocking sodium channels — strongest evidence base of any topical | 2–10% |
| Ketamine | NMDA receptor antagonist; modulates pain signaling. Mixed evidence, real safety considerations | 5–10% |
| Gabapentin | Calms overactive nerve signaling. Skin penetration is limited; weaker than oral | 5–10% |
| Amitriptyline | Tricyclic; modulates pain at multiple levels. Often paired with ketamine for synergy | 2–5% |
| Clonidine | Specific evidence for diabetic neuropathy. Watch for blood pressure interactions | 0.2% |
| Diclofenac | NSAID. Better for inflammation-driven pain than pure neuropathy. OTC version available | 1–5% |
| Baclofen | Muscle relaxant. Added when nerve pain comes with muscle spasm | 2% |
| Capsaicin | Depletes substance P. Causes initial burning. FDA-approved 8% patch is most studied | 0.025–0.075% |
Key Takeaway
A compounded pain cream is custom-mixed by a specialty pharmacy from a doctor's prescription — usually 2–4 active ingredients in one base. The evidence is mixed: not a miracle, not snake oil. Best for localized neuropathic pain when FDA-approved topicals haven't been enough.
Lidocaine. A local anesthetic that blocks sodium channels in nerve fibers. Numbs the area. The most well-evidenced topical for neuropathic pain. Concentrations in compounded creams typically range from 2 to 10 percent. (For comparison, the FDA-approved topical lidocaine patch is 5 percent.)
Ketamine. An NMDA receptor antagonist that interferes with how nerves transmit pain signals. Used systemically (by IV) for severe pain and depression. In topical form for neuropathy, evidence is mixed but real for some patients. Concentrations are typically 5 to 10 percent. Has the most safety considerations of the common ingredients (more on that below).
Gabapentin. An anticonvulsant that calms overactive nerve signaling. Effective orally for neuropathic pain. Topical gabapentin has weaker evidence than oral, partly because penetration through skin is limited. Concentrations range from 5 to 10 percent.
Amitriptyline. A tricyclic antidepressant that affects pain signaling at multiple levels. Often paired with ketamine in topical formulations for synergy. Concentrations are typically 2 to 5 percent.
Clonidine. An alpha-2 adrenergic agonist. Used orally for blood pressure; topically, has small but real evidence for diabetic neuropathy specifically. Concentrations are typically 0.2 percent.
Diclofenac. An NSAID. Most useful for inflammation-driven pain, less so for pure neuropathic pain. The FDA-approved topical version (1 percent gel, sold as Voltaren) is available without a prescription.
Baclofen. A muscle relaxant. Sometimes added when nerve pain is accompanied by muscle spasm.
Capsaicin. Derived from chili peppers. Depletes substance P, a pain-signaling neurotransmitter. The FDA-approved 8 percent patch (Qutenza) is the most studied. Lower-concentration creams (0.025 to 0.075 percent) are available over the counter — see our capsaicin cream guide for the details on how it works and why it sometimes burns at first.
A typical compounded neuropathy cream combines two to four of these. Common combinations include ketamine plus lidocaine plus amitriptyline; or gabapentin plus diclofenac plus amitriptyline plus ketamine; or lidocaine plus clonidine for diabetic foot neuropathy specifically. The exact formula your doctor prescribes will depend on the type of nerve pain you have and what they think is most likely to help.
What the Evidence Actually Shows

This is where the picture gets honest. Compounded pain creams are not a clear win in the research, and they're not a clear loss either. The data depends on which study you read, which formulation, which kind of pain, and how the trial was designed.
Research Says
A 2019 randomized controlled trial of nearly 400 patients with chronic localized pain found that compounded creams reduced pain by 1.4 points on a 10-point scale — while placebo creams reduced it by 1.3 points. The 0.1-point difference was clinically meaningless.
However, a 2025 evidence-informed review in Pain Medicine concluded that topical lidocaine has good evidence for localized neuropathic pain, topical clonidine has small-but-significant evidence for diabetic neuropathy, and combination creams may help selected patients even when individual ingredients have weaker stand-alone evidence. Translation: the right formula for the right patient can help; it's just not most formulas for most patients.
The biggest negative result. A 2019 randomized controlled trial enrolled nearly 400 patients with chronic localized pain (including neuropathic pain) and compared three different compounded cream formulas to placebo creams that contained no active ingredients. After a month of treatment, the active creams reduced pain by an average of 1.4 points on a 10-point scale. The placebo creams reduced pain by 1.3 points. That's a 0.1-point difference — clinically meaningless. The study concluded that compounded creams worked no better than the cream base alone.
The smaller positive results. Several smaller, less rigorous studies have shown real benefit. A 2012 retrospective study of patients using a lidocaine-plus-ketamine cream for neuropathic pain found that 8 of 11 (73 percent) reported meaningful pain reduction. A 2025 evidence-informed review in Pain Medicine concluded that topical lidocaine has good evidence for localized neuropathic pain, that topical clonidine has small-but-significant evidence for diabetic neuropathy, and that combination creams may help selected patients even when individual ingredients have weaker stand-alone evidence.
What this means. The honest synthesis is something like: compounded creams are unlikely to be a miracle for most people, but a meaningful minority do experience real relief. The benefit is most likely when:
- The pain is localized — confined to feet, hands, or one specific area, not widespread
- The pain has a clear neuropathic component (burning, tingling, electric shocks)
- The formula includes lidocaine as a core ingredient
- You've already tried and failed FDA-approved topicals (lidocaine patch, diclofenac gel, capsaicin)
- The skin where you'll apply it is intact (no open wounds or broken skin)
For widespread neuropathy in both feet and hands, or for predominantly numbness without pain, compounded creams are unlikely to be the right tool. Other approaches probably make more sense.
Cost and Insurance Reality
This is the part that surprises people. Compounded medications are almost never covered by health insurance. The FDA approval process specifically applies to manufactured drugs, and most insurance companies use FDA approval as their threshold for coverage. A compounded cream — even when prescribed by a board-certified pain specialist — is treated as an out-of-pocket purchase.
💰 The Cash-Pay Reality
Two compounding pharmacies in the same city can charge dramatically different prices. Always price-shop.
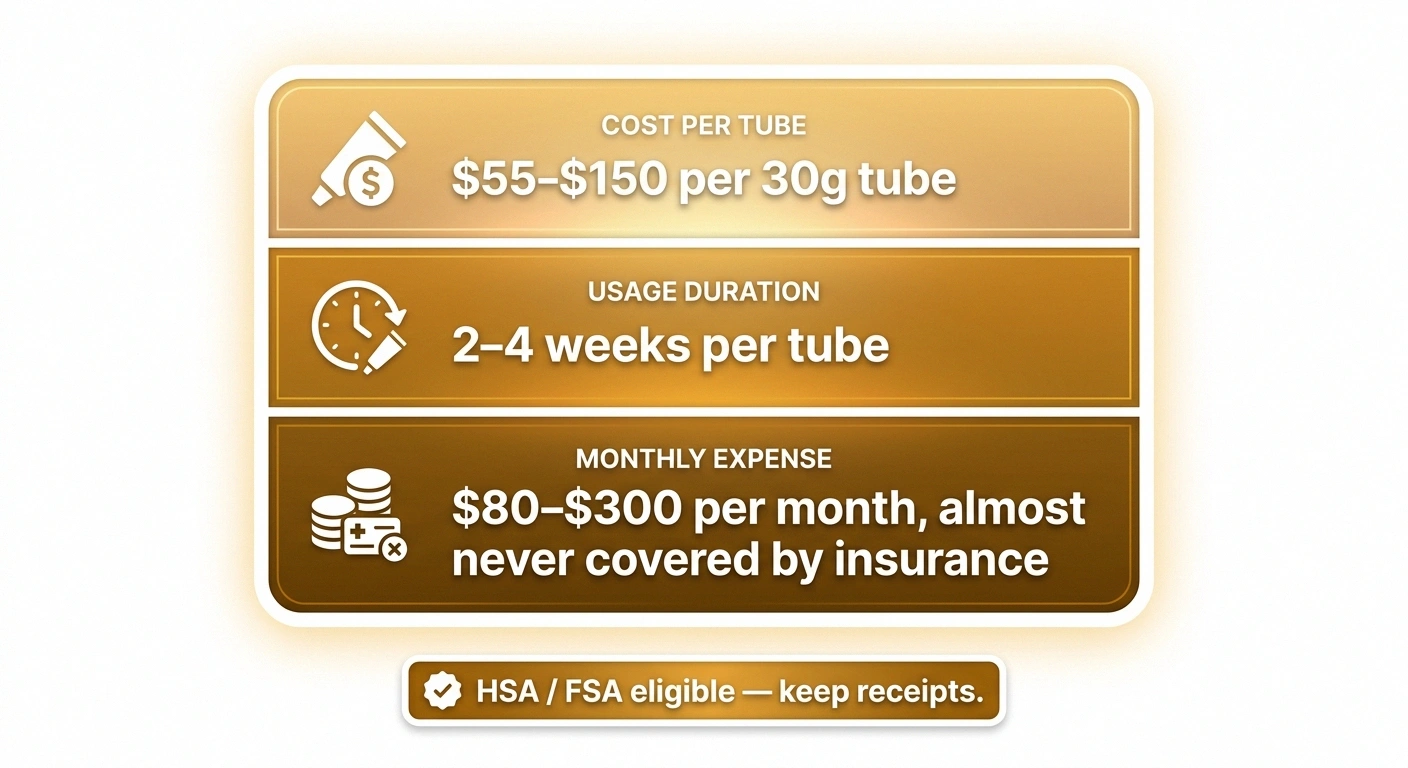
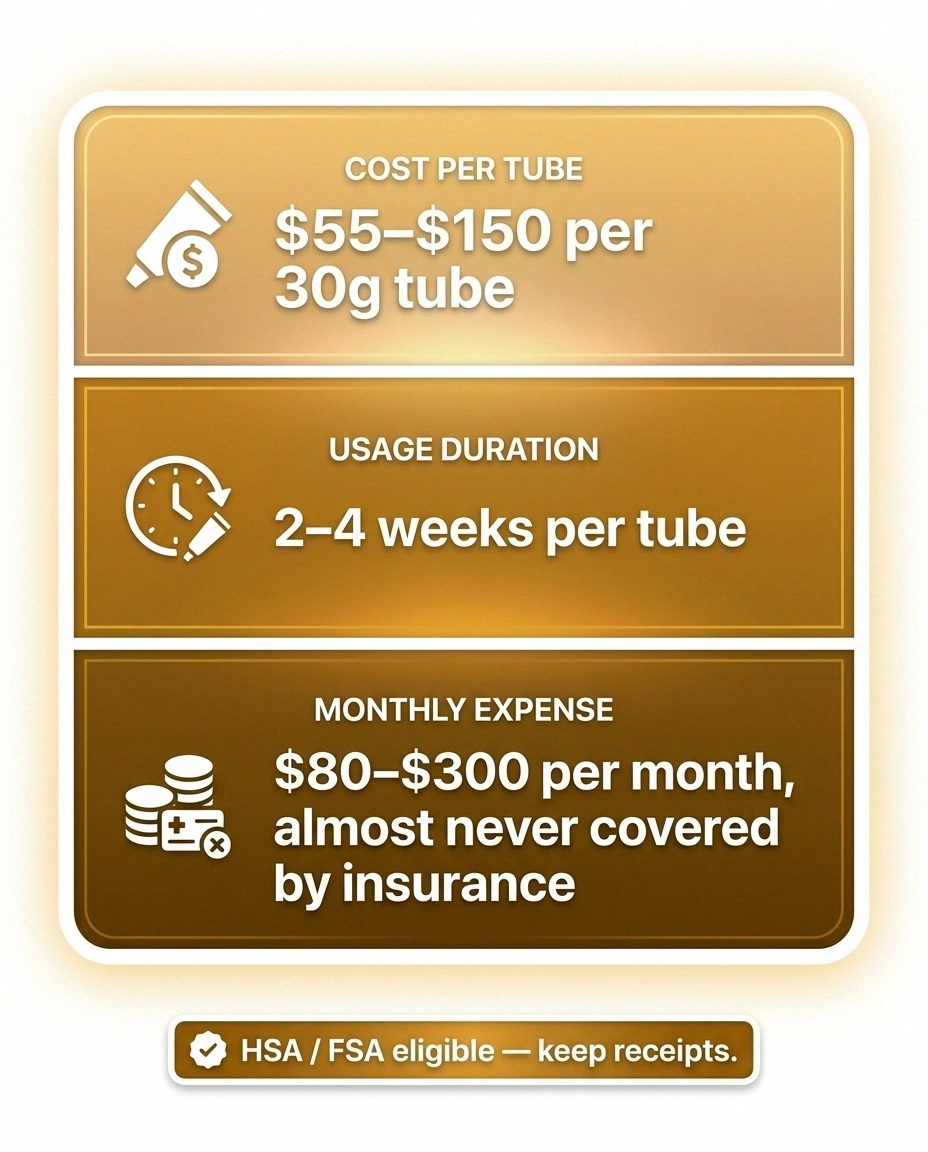
What that looks like in practice: a 30-gram tube of a typical four-ingredient compounded neuropathy cream costs $55 to $150, depending on the pharmacy, the ingredients, and the concentrations. A 30-gram tube usually lasts two to four weeks if you're applying twice a day to both feet. That works out to roughly $80 to $300 per month.
Some compounding pharmacies offer:
- Cash pricing tiers based on quantity (a 60-gram tube may be cheaper per gram than two 30-gram tubes)
- Subscription discounts for monthly auto-refill
- HSA/FSA reimbursement — the cream qualifies for tax-advantaged spending in most cases (keep receipts)
- Patient assistance programs for some specific formulations, particularly through larger compounding chains
Before committing, get the actual price from the pharmacy that will be filling the prescription. Two compounding pharmacies in the same city can charge dramatically different prices for the same formula. If your doctor doesn't know which pharmacy will be cheapest, the receptionist or your insurance's pharmacy benefits manager often can.
Safety: What to Watch For
Topical doesn't mean systemic-free. Active ingredients applied to the skin do enter the bloodstream — typically in much smaller amounts than oral medication, but enough to matter for some drugs. The concentration of the active ingredient, the size of the area you're applying it to, and how often you reapply all change how much gets into your system.
Topical Doesn't Mean Risk-Free
Active ingredients applied to skin do enter the bloodstream. Stop and call your doctor if you notice:
- Confusion, slurred speech, or feeling spacey
- New irregular heartbeat or palpitations
- Significant dizziness, especially on standing
- Drowsiness that's out of character
- Skin rash, redness spreading, blistering
- Burning that doesn't fade after a few minutes
Universal rules: never apply more than your doctor prescribed, never to broken skin, and never under plastic wrap or bandages unless specifically directed. Occlusion can dramatically increase systemic absorption.
The ingredients with the most documented systemic effects in compounded creams:
Ketamine. The most concerning ingredient from a systemic-absorption standpoint. Case reports exist of confusion, drowsiness, hallucinations, and (rarely) more serious effects from compounded creams with ketamine concentrations of 10 percent or more, particularly when applied over large areas or under occlusion (covered with plastic wrap or a bandage to enhance absorption). Current expert guidance recommends keeping ketamine concentrations below 10 percent.
Lidocaine. Generally well-tolerated, but lidocaine toxicity is real and can cause confusion, irregular heartbeat, seizures, and (very rarely) death — particularly when high-concentration creams are applied over large areas. Two adult deaths have been documented from misuse of compounded lidocaine and tetracaine creams. Stay within the dose your doctor prescribes; never apply more than directed in the hope of better relief.
Clonidine. Can cause low blood pressure, slow heart rate, and drowsiness if absorbed systemically. Worth knowing about if you're already on blood pressure medication.
Diclofenac. An NSAID, so all NSAID warnings apply — kidney effects, bleeding risk if you're on blood thinners, GI effects in higher doses.
Symptoms to call your doctor about after starting a compounded cream:
- Confusion, slurred speech, or feeling spacey
- New irregular heartbeat or palpitations
- Significant dizziness, especially on standing
- Drowsiness that's out of character
- Skin rash, redness spreading beyond the application area, blistering
- Burning that doesn't fade after a few minutes
And the universal rules: don't apply to broken skin or open wounds, don't cover with plastic wrap or bandages unless your doctor specifically tells you to (occlusion can dramatically increase absorption), wash your hands after application, and keep the cream away from children and pets — what's a therapeutic dose for you can be dangerous for a small body.
How to Choose a Compounding Pharmacy

Not all compounding pharmacies are equal. Quality, accuracy, and consistency vary significantly. The cream you get can be subtly different from one batch to the next at a low-quality pharmacy, or from one pharmacy to another for the same prescription.
Compounding Pharmacy Quality Checklist
Things to look for:
- PCAB accreditation. The Pharmacy Compounding Accreditation Board is a voluntary third-party accreditation. Pharmacies that go through it have demonstrated quality controls. Not all good pharmacies have it, but it's a positive signal.
- USP <795> or <797> compliance. These are the U.S. Pharmacopeia standards for compounding. Reputable pharmacies will tell you they follow them.
- State licensure. Confirm the pharmacy is licensed in your state. The state's pharmacy board website will list this.
- Willingness to discuss the formula. A good compounding pharmacist should be able to explain the formulation, the base they're using, the expected stability period, and storage requirements without hesitation.
- Consistent prescribers. Pharmacies that work regularly with pain specialists and neurologists tend to know what they're doing. Ask your doctor which pharmacy they'd recommend.
If something seems off — the cream looks or smells different from a previous batch, the consistency is suddenly different, the price changed without explanation — call the pharmacy and ask. Reputable pharmacies will explain. Less reputable ones may not.
When a Compounded Cream Makes Sense (and When Something Else Probably Does)
After all of this, the practical question is: should you ask your doctor about a compounded cream for your neuropathy?
Should I Try a Compounded Cream?
✅ Probably Worth Considering If …
- Pain is localized (one or both feet, one hand, the post-shingles strip)
- Oral neuropathic meds didn't work or were intolerable
- FDA-approved topicals helped partially but not enough
- You can sustain $80–300/month out of pocket
- Your doctor has experience prescribing them
❌ Probably Not the Right Tool If …
- Neuropathy is widespread — both feet, both hands, up the legs
- Dominant symptom is numbness, not pain
- You haven't tried OTC topicals first (lidocaine patch, Voltaren, capsaicin)
- The cost would create financial stress
- Your doctor is reluctant — they often have good reasons
💡 If You Try It: Start with one small tube. Use as directed for 2–4 weeks. Track pain levels honestly. If you see real benefit, continue. If not, stop and save the money.
It probably makes sense to consider one if:
- Your pain is localized to a specific area (one or both feet, one hand, the post-shingles strip)
- You've tried oral neuropathic medications (gabapentin, pregabalin, duloxetine, amitriptyline) and either they didn't work well enough or the side effects were intolerable
- You've tried FDA-approved topicals first — a 5% lidocaine patch, a 1% diclofenac gel, an 0.075% capsaicin cream — and they helped a little but not enough
- You can afford the out-of-pocket cost ($80-300/month) sustainably
- Your doctor has experience prescribing them and can match the formula to your pain pattern
It probably doesn't make sense if:
- Your neuropathy is widespread — both feet and both hands and up the legs
- Your dominant symptom is numbness, not pain (these creams don't restore sensation)
- You haven't tried the FDA-approved over-the-counter topicals first
- The cost would create financial stress
- Your doctor is reluctant — there are reasons reluctant doctors are reluctant
The best mental frame is: a compounded cream is one tool in a toolkit. It's not a cure, it's not a replacement for managing the underlying cause of your neuropathy, and it's not the right tool for every type of nerve pain. For some patients with localized neuropathic pain that hasn't responded to easier options, it's a genuine help. For others, it's an expensive disappointment. The way to find out which group you're in is a careful trial — not a long-term commitment until you know.
Ask your doctor for a single small tube to start with. Apply it as directed for two to four weeks. Track your pain levels honestly. If you see real benefit, continue and consider larger refills. If you don't, stop and put the experience in the same category as everything else you've tried — useful information, not a failure on your part. The right combination of tools for your neuropathy is usually built one careful experiment at a time.
Frequently Asked Questions
What's actually in a compounded pain cream for neuropathy?
Most compounded neuropathy creams combine two to four active ingredients in a single base. Common ingredients include lidocaine (a numbing anesthetic), ketamine (which interferes with pain signaling at NMDA receptors), gabapentin (which calms overactive nerves), amitriptyline (a tricyclic that modulates pain at multiple levels), clonidine (with specific evidence for diabetic neuropathy), diclofenac (an anti-inflammatory), and sometimes baclofen or capsaicin. The specific formula your doctor prescribes depends on the type and location of your nerve pain.
Do compounded pain creams actually work?
The evidence is mixed and depends on the specific formulation and the type of pain. A large 2019 randomized controlled trial found that compounded creams worked no better than placebo cream for general chronic localized pain. However, smaller studies of specific neuropathic pain have shown meaningful benefit for some patients, particularly with combinations including lidocaine. Compounded creams are most likely to help when the pain is localized, has a clear neuropathic component (burning, tingling, electric shocks), and the formula includes lidocaine.
Are compounded pain creams covered by insurance?
Almost never. Compounded medications generally fall outside the FDA approval framework that most insurance companies use to determine coverage. Expect to pay out of pocket. A 30-gram tube typically costs $55 to $150 and lasts two to four weeks of twice-daily application, putting monthly cost in the $80 to $300 range. HSAs and FSAs usually cover the expense. Compare prices between local compounding pharmacies because they can vary significantly.
Are compounded pain creams safe?
Generally well-tolerated when used as directed, but topical doesn't mean risk-free. The active ingredients enter the bloodstream in smaller amounts than oral medication, but in some cases enough to matter — particularly ketamine, lidocaine, and clonidine. Apply only the amount your doctor prescribes, never to broken skin, never under plastic wrap or bandages unless specifically directed (occlusion increases absorption), and stop and call your doctor if you notice confusion, irregular heartbeat, dizziness, or unusual drowsiness.
Should I try a compounded cream before or after FDA-approved topicals?
After. FDA-approved topicals — the 5% lidocaine patch, 1% diclofenac gel (Voltaren), and over-the-counter capsaicin cream — have stronger evidence, lower cost, and easier access. For localized neuropathic pain, work through these first. If they help partially but not enough, or if they don't help and your pain is still localized, that's the right time to ask about a compounded combination. Skipping the FDA-approved options usually means spending more money for results you could have gotten cheaper.
How do I find a good compounding pharmacy?
Ask your prescribing doctor which pharmacy they recommend — pain specialists and neurologists who prescribe compounded creams regularly know which pharmacies do the work well. Look for PCAB accreditation, USP <795> or <797> compliance, and clear willingness to discuss the formula and base they're using. Confirm state licensure on your state pharmacy board's website. Avoid pharmacies that are vague about what they're mixing or evasive about pricing.
How long does a compounded cream take to work?
Some patients notice numbing or pain reduction within 30 to 60 minutes of the first application (mostly from the lidocaine component). Sustained benefit, if it's going to happen, usually shows up within two to four weeks of consistent twice-daily application. If you've been using a cream as directed for a full month and you can't tell whether it's helping, it probably isn't. Stop, save the money, and try a different approach.


