
The first time I heard someone say their tingling feet were “just from the stress of living with Crohn's,” I bit my tongue. They had been told that by their gastroenterologist — a doctor they trusted and had seen for years. The trouble was, they'd been describing classic neuropathy symptoms for almost two years, and no one had ever ordered a single test to investigate.
If you have inflammatory bowel disease — Crohn's disease or ulcerative colitis — and you've started noticing numbness, tingling, burning, or weakness anywhere in your body, this article is for you. Peripheral neuropathy is a known and increasingly recognized complication of IBD. It is not “just stress.” It is not “just getting older.” And in many cases, it is treatable, especially when it's caught early.
Let me walk you through what the research actually shows, why IBD damages nerves through several different pathways, and what to ask your gastroenterologist or neurologist when you sit down to discuss it.
Why IBD and Neuropathy Are Connected
For decades, the textbooks treated nerve symptoms in IBD as rare curiosities. That has slowly changed. Population-based studies and reviews published in journals like Brain, the European Journal of Internal Medicine, and the World Journal of Gastroenterology now describe peripheral neuropathy as one of the more common neurologic manifestations of inflammatory bowel disease — alongside cerebrovascular disease and demyelinating central nervous system events.
Key Takeaway
People with Crohn's disease or ulcerative colitis are roughly four times more likely to develop peripheral neuropathy than the general population. Tingling, numbness, or burning in someone with IBD deserves a real workup — not a shrug.
How common is “common”? A press release from the American Academy of Neurology, summarizing one of the larger cohort analyses, reported that people with IBD were roughly four times more likely to develop neuromuscular conditions than people without IBD. That includes carpal tunnel syndrome and small fiber neuropathy — the kind that produces burning and numbness in the feet without obvious changes on standard nerve conduction studies.
The exact prevalence depends on how researchers define neuropathy and how aggressively they look for it. Studies that rely on patient self-report tend to find lower numbers; studies that include detailed neurologic examination and nerve testing find higher numbers — sometimes 10% or more of long-standing IBD patients have measurable nerve involvement.
The reason this surprises so many people is straightforward: gastrointestinal inflammation feels nothing like nerve pain. Patients tend to describe their IBD as “the gut thing” and their neuropathy as “the foot thing,” and the two are rarely connected in the conversation with their doctor unless someone specifically draws the line between them.
Three Pathways from Gut to Nerves
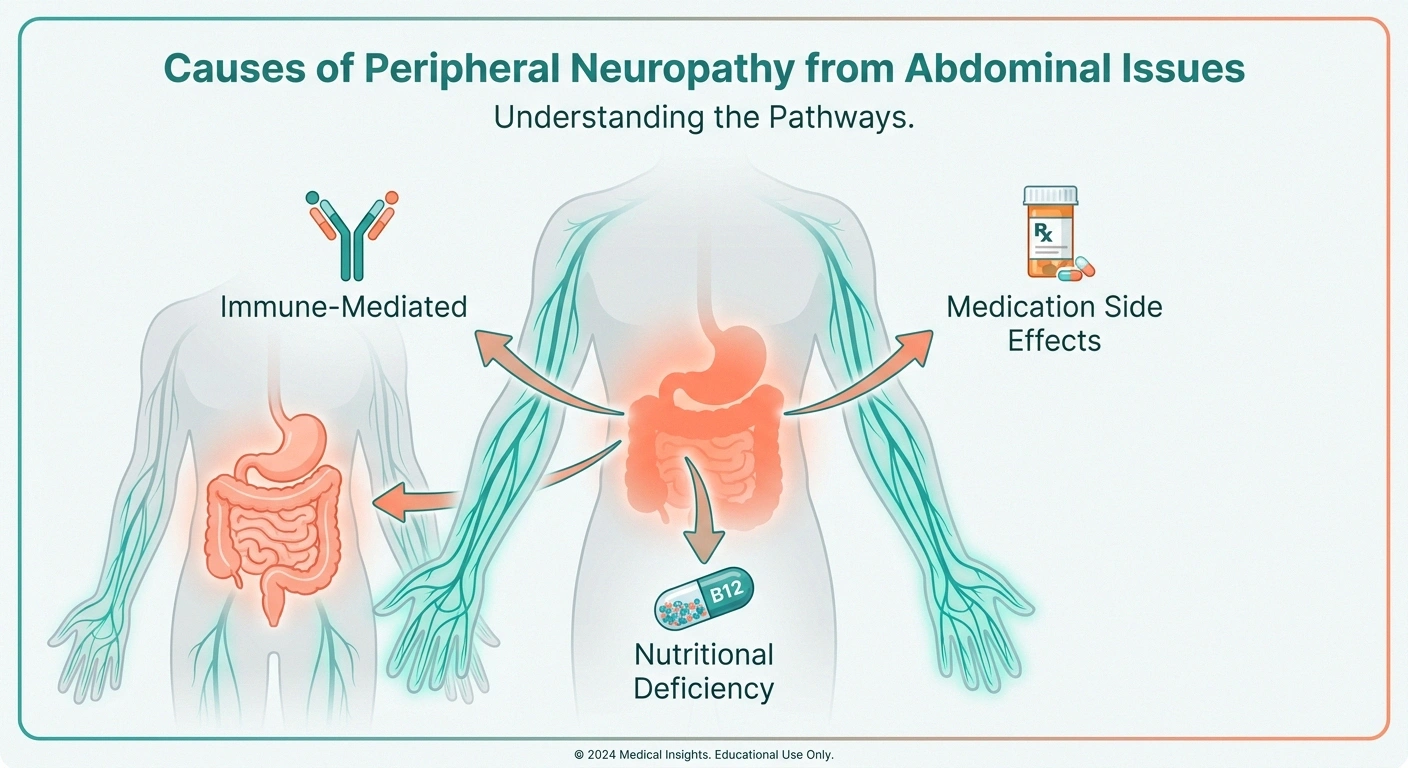
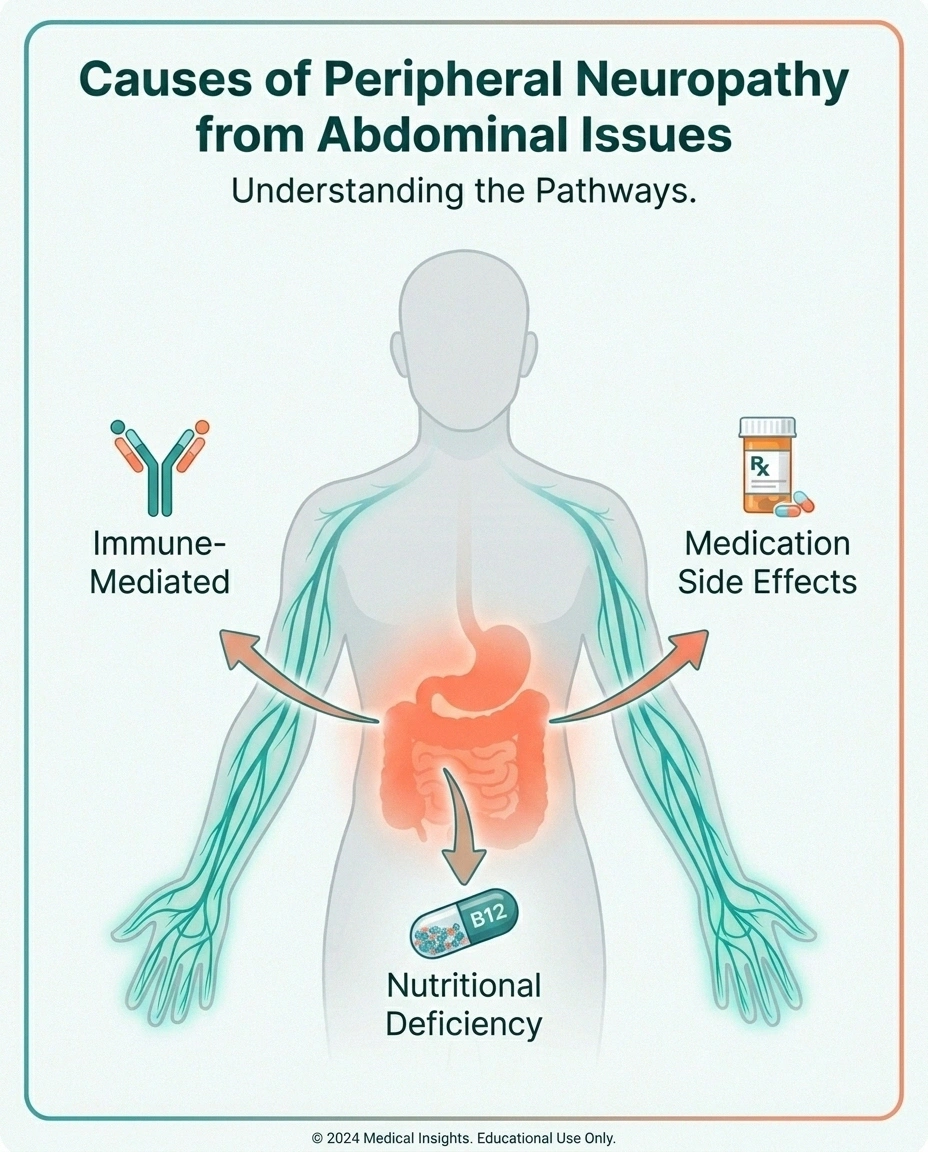
Researchers have identified three main mechanisms by which IBD causes nerve damage. Most patients who develop neuropathy have a combination of these factors at work. Understanding which one is driving your symptoms shapes the treatment.
Three Pathways From IBD to Nerve Damage
1. Immune-Mediated
The same immune dysregulation that inflames the gut attacks myelin, axons, or small blood vessels feeding nerves.
2. Nutritional Deficiency
Terminal ileum disease in Crohn's disrupts B12 absorption. Chronic diarrhea depletes folate, copper, thiamine, B6, vitamin E.
3. Medication Side Effects
Metronidazole (most common), anti-TNF biologics (rare demyelinating events), sulfasalazine, thalidomide.
Pathway 1: Immune-Mediated Damage
The most extensively studied mechanism is direct immune attack on peripheral nerves. IBD is fundamentally an autoimmune (or strongly immune-dysregulated) disease — the same misfiring of the immune system that inflames the colon or small intestine can also target the protective myelin sheath around nerves, the nerve fibers themselves, or the small blood vessels that feed them.
When the inflammation is in the myelin, it produces a demyelinating neuropathy that often looks like CIDP — chronic inflammatory demyelinating polyneuropathy. When it strikes the small blood vessels, it produces a vasculitic neuropathy that classically causes “mononeuritis multiplex” — patchy nerve damage that affects different nerves in different limbs at unpredictable times. When it preferentially affects the smallest unmyelinated fibers, you get small fiber neuropathy with burning, tingling, and autonomic symptoms.
The good news about immune-mediated IBD neuropathy is that it usually responds to immunotherapy. The same medications used to control gut inflammation — corticosteroids, IVIG, and in some cases plasma exchange — can stop and even partially reverse the nerve damage when started early enough.
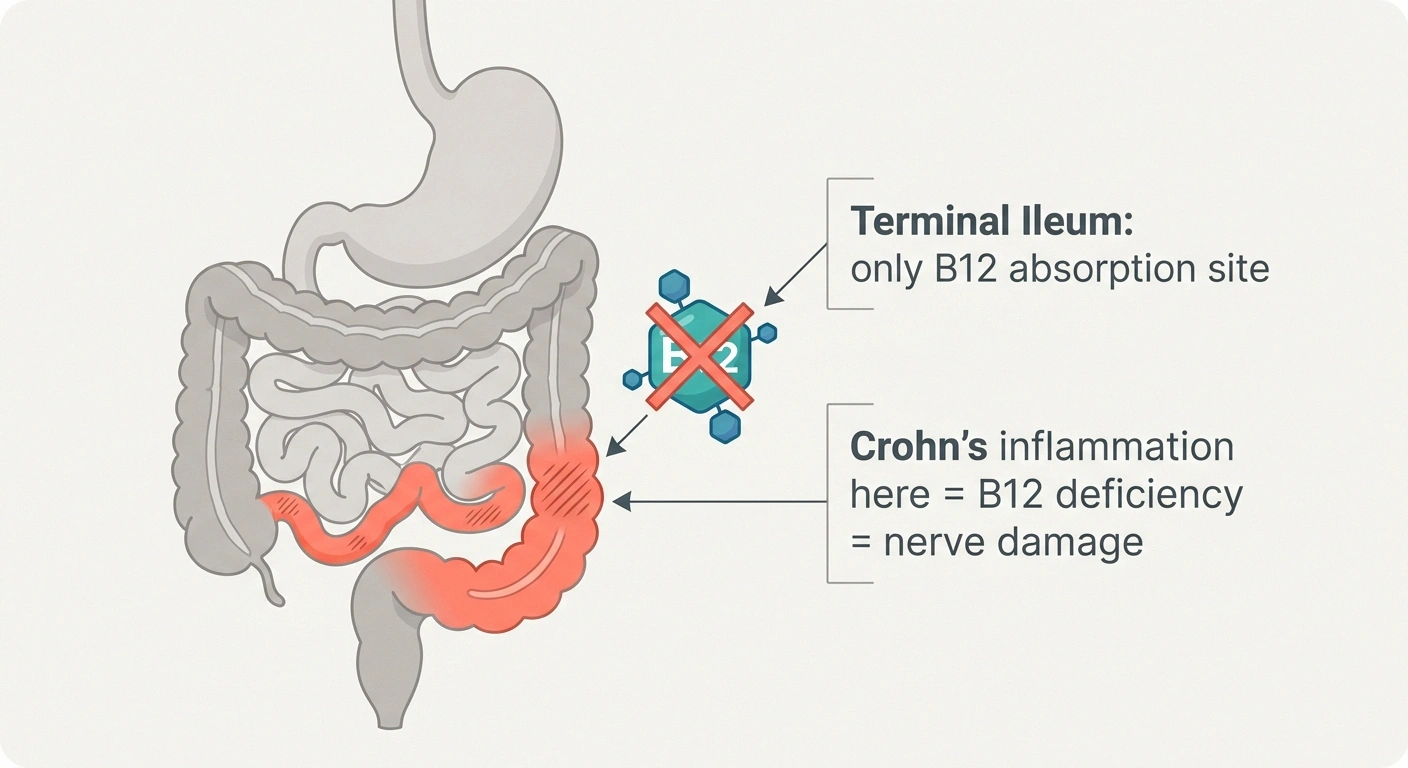
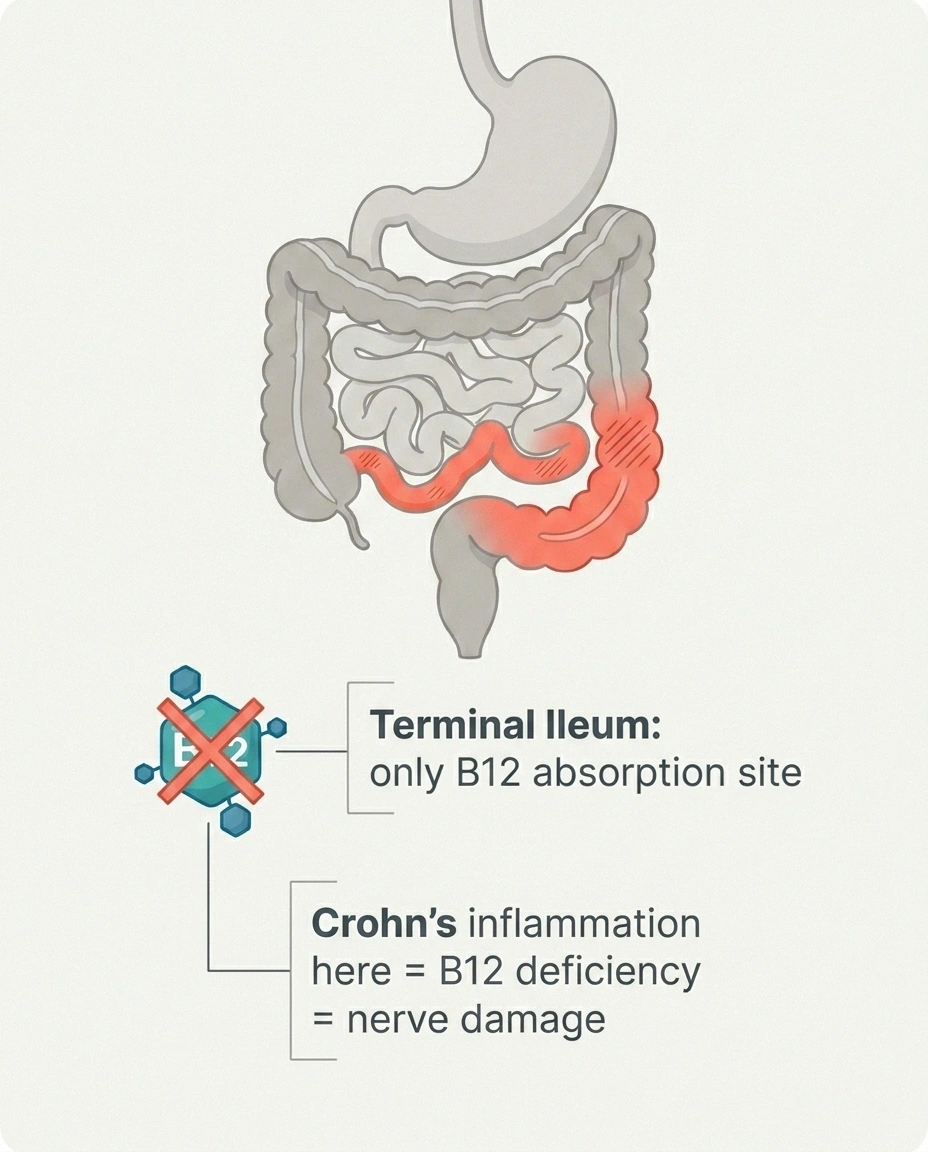
Pathway 2: Nutritional Deficiency
Crohn's disease loves to attack the terminal ileum, the very last segment of the small intestine. That's not a coincidence — it happens to be the only place in your body where you absorb vitamin B12. When the terminal ileum is inflamed, scarred, or surgically removed, B12 absorption drops, and B12 deficiency is one of the most well-documented causes of peripheral neuropathy in any patient population. (We have a full article on vitamin deficiencies that cause neuropathy if you want the broader picture.)
Ulcerative colitis tends to spare the small intestine, so isolated B12 deficiency is less common — but UC patients aren't off the hook. Chronic diarrhea, blood loss, and reduced food intake during flares can drive deficiencies in folate, copper, thiamine (B1), pyridoxine (B6), and vitamin E. Each of these deficiencies has a documented connection to neuropathy.
One particular trap to watch for: copper deficiency neuropathy in patients who have had bariatric surgery and who also take high-dose zinc supplements (zinc displaces copper). I've heard from readers who developed dramatic spinal cord and peripheral nerve symptoms from this exact combination.
Pathway 3: Medication-Related Damage
This is the pathway that most patients don't see coming because the medications causing it are often the same ones holding their IBD in remission. The big names to know:
Don't Stop a Medication On Your Own
Even if you suspect an IBD medication is causing nerve symptoms, do not stop it without speaking to your prescribing physician. Uncontrolled IBD has its own neurologic and systemic risks. Most patients can switch to a different agent and keep their disease in remission.
- Metronidazole (Flagyl) — A widely-used antibiotic for fistulas, abscesses, and pouchitis. Long courses are notorious for causing a sensory neuropathy that begins in the feet. The risk goes up sharply after 4 weeks of treatment and at higher cumulative doses. Most cases improve after stopping the drug, but not all of them — and recovery can take months or years.
- Anti-TNF biologics (infliximab, adalimumab, golimumab, certolizumab) — Rare but real demyelinating events have been reported, including peripheral demyelinating neuropathy and CNS demyelination resembling multiple sclerosis. The signal is small but recognized in the prescribing information.
- Sulfasalazine — Can cause a folate deficiency that leads to neuropathy if folate isn't supplemented.
- Thalidomide — Rarely used for refractory Crohn's, but it has well-known dose-dependent neuropathy as a side effect.
- Corticosteroids — Long-term steroids can cause a steroid myopathy that's sometimes mistaken for neuropathy. Worth distinguishing.
This is one reason I always tell readers: if you develop new nerve symptoms within weeks of starting any new IBD medication, it deserves a phone call to your gastroenterologist before you assume it's unrelated.
What IBD-Related Neuropathy Feels Like
Symptoms vary enormously depending on which pathway is driving the damage, which nerves are affected, and how long it's been going on. That said, certain patterns recur often enough that they've become the cluster I look for when someone describes their symptoms:
- Burning or tingling in the feet, often worse at night — the most common presentation. Feels like sock fibers in shoes that aren't there. (See: burning feet syndrome.)
- Numbness that creeps up the legs over months or years. Often described as “wearing thick socks all the time.”
- Tingling or weakness in the hands — often a sign of carpal tunnel, which is more common in IBD patients but can also indicate a more diffuse polyneuropathy.
- Sudden, asymmetric weakness or sensory loss — for example, foot drop on one side but not the other, or numbness in just one hand. This pattern points toward mononeuritis multiplex, which is more urgent and warrants prompt evaluation.
- Autonomic symptoms — lightheadedness on standing, abnormal sweating, sluggish or rapid heart rate, erectile dysfunction, bladder changes. These can be hard to separate from medication side effects but are real signs of small fiber and autonomic involvement.
- Episodes of weakness during flares that improve once the flare is treated — strongly suggests the immune-mediated pathway.
The single biggest mistake I see is assuming that nerve symptoms appearing during an IBD flare must be “from the stress of the flare.” Sometimes they are. But often the flare and the nerve symptoms share a common cause: the immune system is dysregulated, and it's hitting the gut and the nerves at the same time.
Getting the Right Workup
If you suspect IBD-related neuropathy, the testing is straightforward and most of it can be ordered by either your gastroenterologist or a primary care doctor — although a referral to a neurologist is the right move if findings are abnormal.
Your Workup Roadmap
Symptom log + medication list
When symptoms started, what makes them better or worse, every drug and supplement with start dates.
Bloodwork — nutritional + inflammatory
B12 with MMA, folate, copper, zinc, thiamine, B6, vitamin E, A1c, ESR, CRP, ANA, ANCA.
Neurology referral if abnormal
Especially for asymmetric weakness, suspected demyelinating disease, or unclear cause.
EMG/NCS or skin biopsy
Standard nerve testing for large-fiber disease; skin punch biopsy if small fiber neuropathy is suspected.
Treat the cause
Immune-mediated → immunotherapy. Nutritional → replacement. Medication → switch agents with prescriber.
🔎 Research Says
Studies published in Brain and the European Journal of Internal Medicine describe IBD-associated neuropathy as underreported — meaning the true prevalence is likely higher than published numbers. Cohort analyses found that patients with detailed neurologic exam and skin biopsy had nerve involvement rates above 10% in long-standing IBD.
The Bloodwork to Ask For
A reasonable starting panel includes:
The Single Most Useful Sentence
“Could my IBD be causing this nerve damage, and what's the right workup?”
Bring this question to your gastroenterologist. It signals you understand the connection and want it taken seriously.
- Complete blood count and metabolic panel
- Vitamin B12 (and methylmalonic acid if B12 is borderline)
- Folate
- Vitamin D
- Vitamin E
- Copper and zinc
- Thiamine (B1) — order specifically; it's not on a standard panel
- Pyridoxine (B6)
- Hemoglobin A1c (to rule out concurrent diabetic neuropathy, which can coexist)
- Thyroid panel (TSH, free T4)
- ESR and CRP (inflammation markers)
- ANA, ANCA, and rheumatoid factor (for vasculitis screen if symptoms are asymmetric)
This is roughly the panel I cover in the broader article on neuropathy lab tests, with the addition of vasculitis markers because IBD raises that risk specifically.
Nerve Testing
If symptoms or exam findings suggest a polyneuropathy, your neurologist will likely order an EMG and nerve conduction study. (We cover what to expect in our EMG guide.) Standard nerve conduction is good at detecting large-fiber neuropathies — demyelinating, axonal, or mixed — but it can miss small fiber neuropathy. If your symptoms sound like SFN (burning, autonomic features) and standard testing is normal, ask about skin punch biopsy to count intraepidermal nerve fiber density. That's the test that catches what standard EMG misses.
The Conversation to Have
Bring three things to your appointment:
- A symptom log: when symptoms started, how they've changed, what makes them better or worse, whether they came in alongside a flare or after starting a new medication.
- A complete medication list including doses and start dates — including supplements.
- A direct question: “Could my IBD be causing this nerve damage, and what's the right workup?”
That last sentence does most of the work. It signals to the doctor that you're aware of the connection, that you'd like the conversation to take it seriously, and that you're not just here for reassurance.
What Treatment Looks Like

Treatment of IBD-related neuropathy follows the cause. The good news, repeated in study after study, is that the majority of immune-mediated cases improve substantially with appropriate immunotherapy — often the same medications already in the IBD toolkit.
Realistic Recovery Timelines
If the Cause Is Immune-Mediated
Treatment options include:
- Corticosteroids — Often used acutely for vasculitic or demyelinating presentations. Prednisone tapers can produce dramatic short-term improvement.
- IVIG (intravenous immunoglobulin) — First-line for many demyelinating presentations including CIDP-like neuropathy. Works in roughly 60–70% of patients. Treatment is repeated as needed.
- Plasma exchange (plasmapheresis) — Used in severe or rapidly progressive cases, especially when antibodies are clearly driving the disease.
- Steroid-sparing immunosuppressants — Azathioprine, methotrexate, mycophenolate, and rituximab are sometimes used long-term, especially when the same agents are also helping the gut.
- Optimization of IBD control — In many cases, the strongest predictor of nerve recovery is how well the underlying IBD is controlled. Patients who achieve sustained remission tend to see their nerve symptoms stabilize or improve.
One of the most encouraging findings in the IBD-neuropathy literature is that patients with demyelinating subtypes have the best outcomes. Nearly all show meaningful improvement with treatment. Axonal and small fiber subtypes are slower and less complete responders, but they often still improve at least partially.
If the Cause Is Nutritional
This is the most fixable category — but recovery is rarely instant. Replacing missing vitamins or minerals corrects the deficiency in days to weeks, but nerve fibers regenerate slowly. Plan on:
- 3–6 months for partial improvement of mild deficiency-driven neuropathy
- 6–18 months for substantial recovery in long-standing cases
- Some persistent symptoms in patients with very long-standing or severe damage
If absorption is the limiting factor — common in Crohn's with terminal ileal involvement — oral supplements may not be enough. B12 injections, IV iron, or specialized formulations may be needed. Work with both your gastroenterologist and a registered dietitian who has IBD experience.
If the Cause Is Medication-Related
Stopping the offending medication is the obvious step, but it has to be balanced against the risk of an IBD flare. This is a conversation for your gastroenterologist, not a decision to make on your own. Many patients can switch to a different agent in the same class or a different mechanism without losing disease control. A few important specifics:
- Metronidazole-induced neuropathy generally improves once the drug is stopped, but recovery can take months. Severe cases may have residual symptoms.
- Anti-TNF demyelinating events typically resolve when the agent is discontinued. Switching to a different mechanism (vedolizumab, ustekinumab, or a Janus kinase inhibitor) is usually the next step.
- Don't stop a medication that's controlling your IBD until you've spoken with the prescribing physician, even if you suspect it of causing nerve symptoms. Uncontrolled IBD has its own neurologic and systemic risks.
Symptom Management While You Wait

Even when the cause is clearly identified and treated, symptoms typically take time to resolve. While that's happening, the toolkit for managing neuropathy pain and disturbance is the same one we use for any neuropathy:
- Standard neuropathic pain medications — gabapentin, pregabalin, duloxetine, amitriptyline. Discuss interactions with your IBD regimen.
- Topicals — lidocaine patches, capsaicin cream, compounded creams.
- Supportive care — supportive shoes, compression socks, foot care and inspection (especially important if circulation is also affected).
- Movement — walking and gentle exercises as tolerated.
- Mind-body — mindfulness and pacing approaches.
One quiet truth I've learned working with patients: managing the gut and managing the nerves are not separate projects. The body that's calmer in the gut tends to be calmer in the nerves. Sleep, stress, and inflammation feed both systems. Anything that improves one tends to nudge the other in the same direction.
Questions Worth Asking Your Gastroenterologist

If you suspect IBD-related neuropathy, here are the specific questions I'd bring to your next appointment. They're not confrontational — they signal partnership and direct attention where it needs to go.
- “Given my IBD, do my new nerve symptoms warrant a workup for peripheral neuropathy?”
- “Would you order a B12 with methylmalonic acid, folate, copper, zinc, and thiamine to start?”
- “Could any of my current medications — including [specific drug name] — be contributing to nerve symptoms?”
- “Should I be referred to a neurologist who has experience with autoimmune neuropathy?”
- “If we find something immune-mediated, would my current IBD treatment also help the nerve symptoms, or do we need a different approach?”
You are not asking your gastroenterologist to be a neurologist. You are asking them to acknowledge the connection and help you take the next step.
The Bigger Picture
The connection between IBD and neuropathy is one of those quiet medical truths that hasn't fully arrived in the exam room yet. Researchers know about it. Specialists who keep up with the literature know about it. But the average patient with Crohn's or UC and tingling feet has often had to advocate for themselves to get the workup.
If you take one thing from this article, take this: tingling, numbness, burning, or weakness in someone with inflammatory bowel disease is not “normal.” It deserves a real conversation, a basic workup, and — when needed — a referral. The treatments are real. The recovery, in most cases, is real. And the alternative — letting nerve damage progress for years before someone names it — is one of the most preventable kinds of suffering I see in this community.
You know your body. You know what's new and what's not. Trust that instinct, and bring it with you to your next appointment.
Frequently Asked Questions
Can Crohn's disease cause peripheral neuropathy?
Yes. Peripheral neuropathy is a recognized complication of Crohn's disease. The connection runs through three mechanisms — immune-mediated nerve damage, nutritional deficiencies (especially B12 from terminal ileum involvement), and medication side effects. Population-based studies have shown that people with IBD are roughly four times more likely to develop peripheral nerve conditions than the general population.
Does ulcerative colitis affect the nerves?
It can. Ulcerative colitis is less commonly associated with neuropathy than Crohn's disease because UC affects only the colon and doesn't typically interfere with vitamin absorption. But UC patients still develop immune-mediated neuropathies — including small fiber, demyelinating, and vasculitic forms — and can experience nutritional deficiencies during severe flares. The risk is lower than in Crohn's, but real.
Why do my feet tingle when my Crohn's flares?
There are a few possibilities. Most commonly, it reflects systemic inflammation hitting the small nerve fibers, producing burning or tingling that mirrors the gut flare. It can also indicate a developing small fiber or demyelinating neuropathy that becomes more symptomatic when overall inflammation rises. New tingling that recurs with flares deserves a workup — at minimum, blood tests for B12, folate, and inflammatory markers.
Is metronidazole-induced neuropathy reversible?
Most cases improve significantly after stopping the drug, but recovery can take weeks to months and is not always complete. The risk of permanent symptoms goes up with cumulative dose, longer treatment courses (more than 4 weeks), and pre-existing nerve vulnerability. If you develop new burning or tingling on metronidazole, alert your prescribing physician — continuing the drug after symptoms appear meaningfully increases the risk of lasting damage.
Can biologics like Humira or Remicade cause nerve damage?
Rarely, yes. Anti-TNF biologics including infliximab, adalimumab, golimumab, and certolizumab have been associated with rare cases of peripheral demyelinating neuropathy and central nervous system demyelination. The signal is small but recognized in the FDA prescribing information for these drugs. New nerve symptoms in someone on a biologic should prompt a careful review and a discussion about alternative agents.
Will treating my IBD also treat my neuropathy?
Often, yes. If your neuropathy is immune-mediated, the same immunosuppressive medications that control the gut inflammation can also calm the nerve inflammation. Patients who achieve sustained IBD remission tend to see their nerve symptoms stabilize or improve. If the cause is nutritional deficiency, however, treating the IBD won't directly fix the deficiency — you'll need to replace the missing vitamins or minerals separately.
Should I see a neurologist or my gastroenterologist first?
Start with your gastroenterologist for the conversation and the basic bloodwork. They know your IBD history, your medications, and your overall risk factors. If the bloodwork shows a deficiency that fits, your gastroenterologist can manage it. If exam findings or symptoms suggest a more complex picture — asymmetry, weakness, suspected demyelinating disease, or unclear cause — ask for a referral to a neurologist who has experience with autoimmune neuropathy.
Can I prevent IBD-related neuropathy?
You can lower the risk substantially. The core strategies are: maintain good IBD control with your gastroenterologist, monitor B12 and other key nutrient levels every 6 to 12 months (more often if you've had bowel resection), avoid prolonged courses of metronidazole when possible, and report new nerve symptoms early rather than waiting for them to become severe. Early recognition is the single most important predictor of recovery when neuropathy does develop.


