
I first heard about hyperbaric oxygen therapy from a woman at our support group named Diane. She had driven two hours each way, three times a week, for forty sessions inside a clear acrylic chamber the size of a large coffin, breathing pure oxygen at twice atmospheric pressure. It cost her twelve thousand dollars out of pocket, because her insurance refused to cover it. And she swore it gave her back her feet.
That story sent me down a rabbit hole. Hyperbaric oxygen therapy — HBOT — is one of those treatments that lives in a strange middle space. It's well-established for some conditions (decompression sickness in divers, carbon monoxide poisoning, certain non-healing wounds) and at the same time heavily marketed for an exhausting list of off-label uses. Between those two extremes sit conditions like peripheral neuropathy, where the evidence is genuinely interesting but doesn't quite live up to the marketing.
If someone is suggesting HBOT to you for nerve pain — or you've seen the ads and wondered whether to try it — this article walks through what HBOT actually does, what the research has found, what it costs in time and money, and how to decide if it's worth pursuing.
What Is Hyperbaric Oxygen Therapy?
The basic concept of HBOT is straightforward. You sit or lie inside a sealed chamber. The chamber is pressurized — typically to between 2.0 and 2.4 times normal atmospheric pressure (referred to as 2.0 to 2.4 ATA, or “atmospheres absolute”). While inside, you breathe 100% oxygen, often through a mask or hood.
Key Takeaway
HBOT is FDA-approved for 13 specific conditions — peripheral neuropathy alone is not on that list. A 2024 meta-analysis shows real benefit for diabetic peripheral neuropathy, but it remains an off-label, mostly out-of-pocket treatment with significant time and cost commitment.
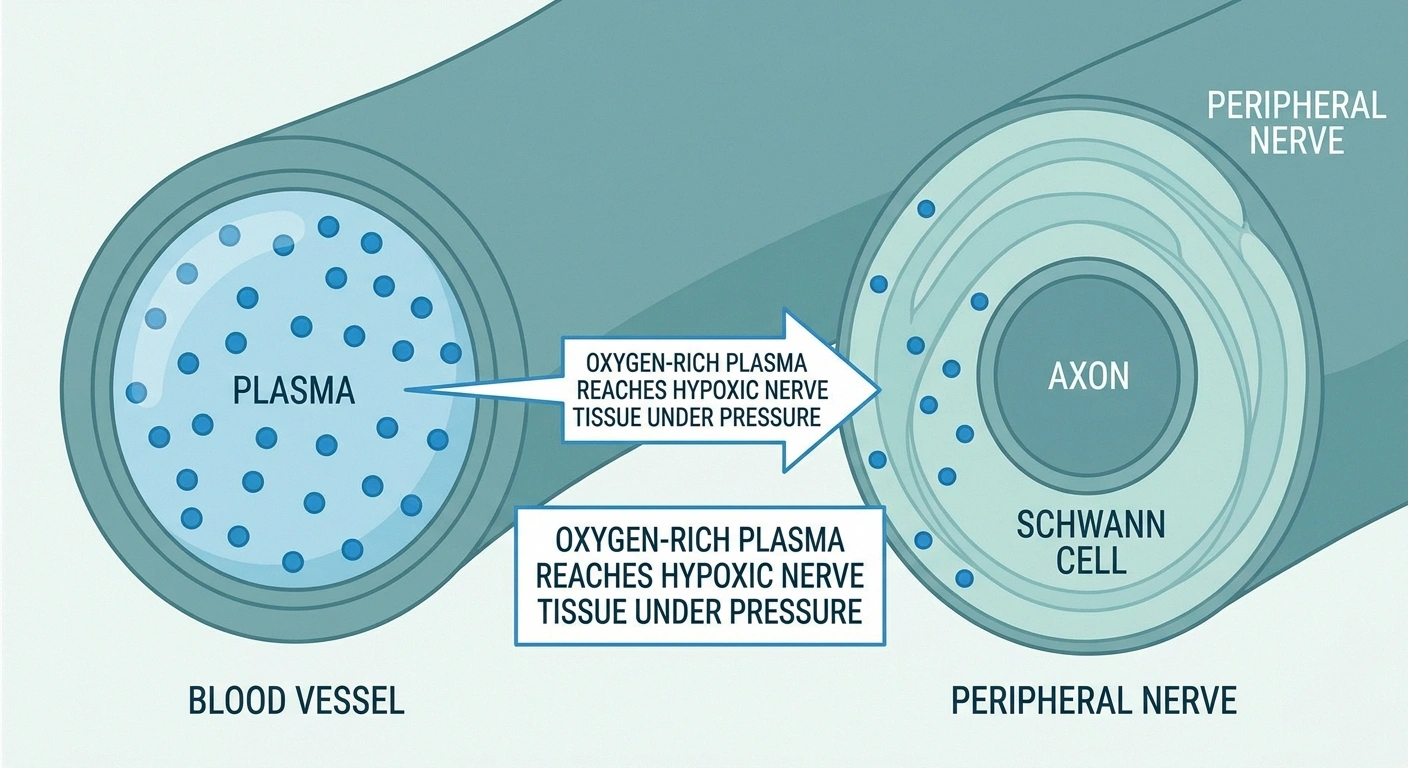
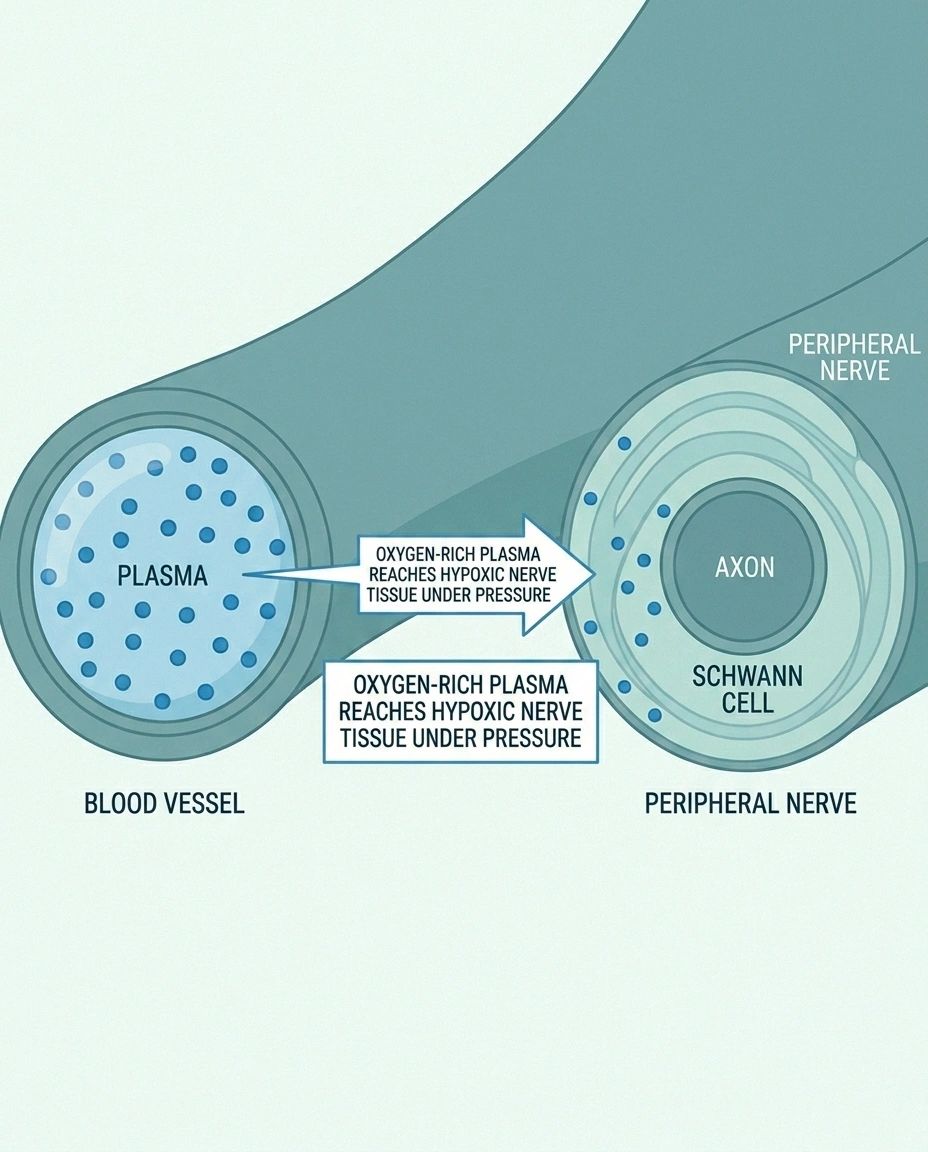
The combination of high pressure and pure oxygen forces a much larger amount of oxygen to dissolve into your blood plasma than you can ever get at normal pressure breathing room air. That oxygen-rich plasma can reach areas where blood flow is poor or where nerves and tissues are starved for oxygen — like the small vessels around damaged peripheral nerves.
A typical HBOT course for neuropathy involves 20 to 40 sessions of 60 to 90 minutes each. Sessions are usually scheduled three to five times per week. The total course can take 6 to 12 weeks to complete.
FDA-Approved Uses (And What's Not on the List)
This is where it pays to be precise, because the marketing around HBOT often glosses over an important detail.
The FDA recognizes HBOT as a primary or adjunctive treatment for thirteen specific conditions, including air or gas embolism, decompression sickness, carbon monoxide poisoning, severe anemia, certain bone infections, radiation tissue injury, thermal burns, and chronic non-healing wounds — including diabetic foot ulcers of Wagner Grade 3 or higher.
What's not on that list: peripheral neuropathy. Plain diabetic peripheral neuropathy without a non-healing foot ulcer is not an FDA-approved indication. Idiopathic neuropathy isn't either. Chemotherapy-induced peripheral neuropathy isn't. Small fiber neuropathy isn't.
That doesn't mean HBOT can't help these conditions — it means clinics offering it for neuropathy are doing so off-label, and your insurance is unlikely to cover it. The 13-condition FDA list is also tightly tied to Medicare coverage, which we'll come back to.
What Does the Research Show for Neuropathy?
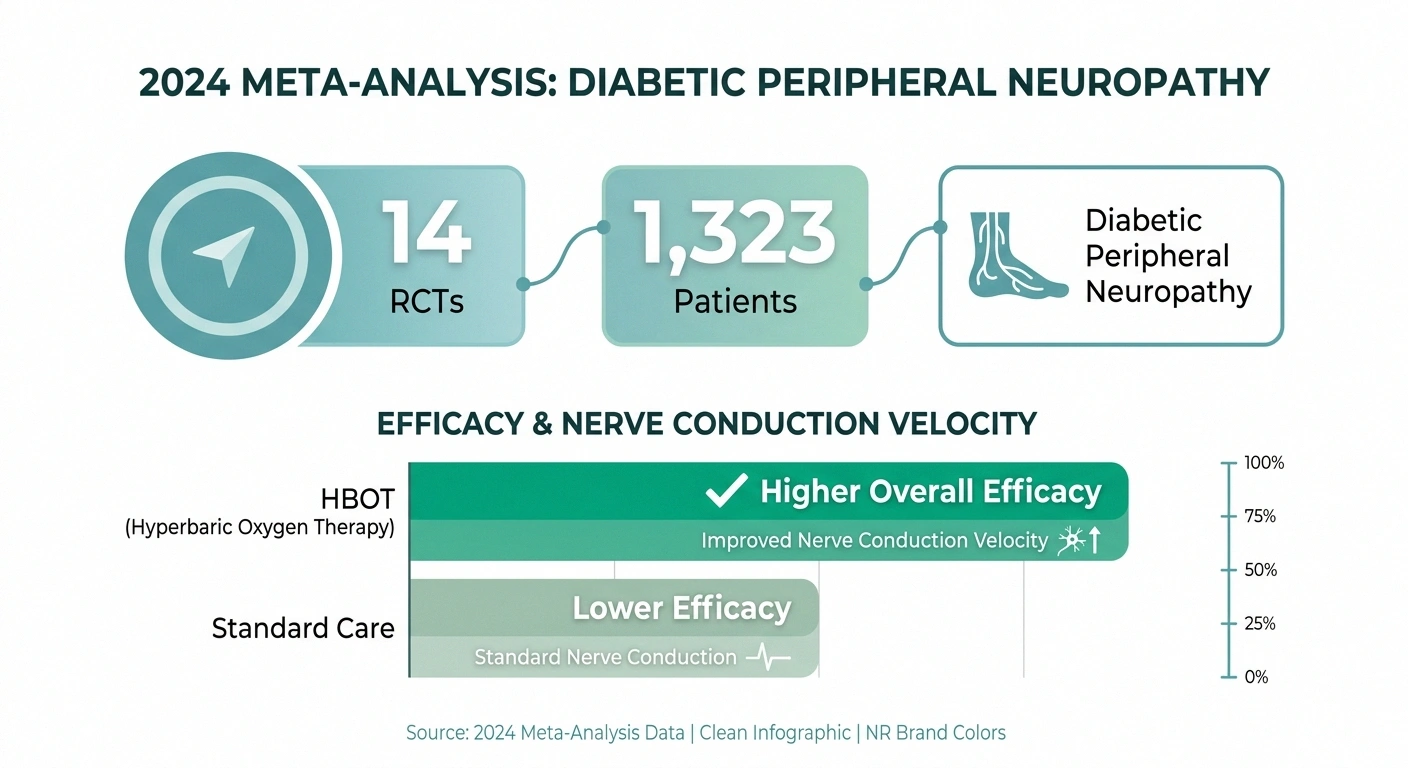
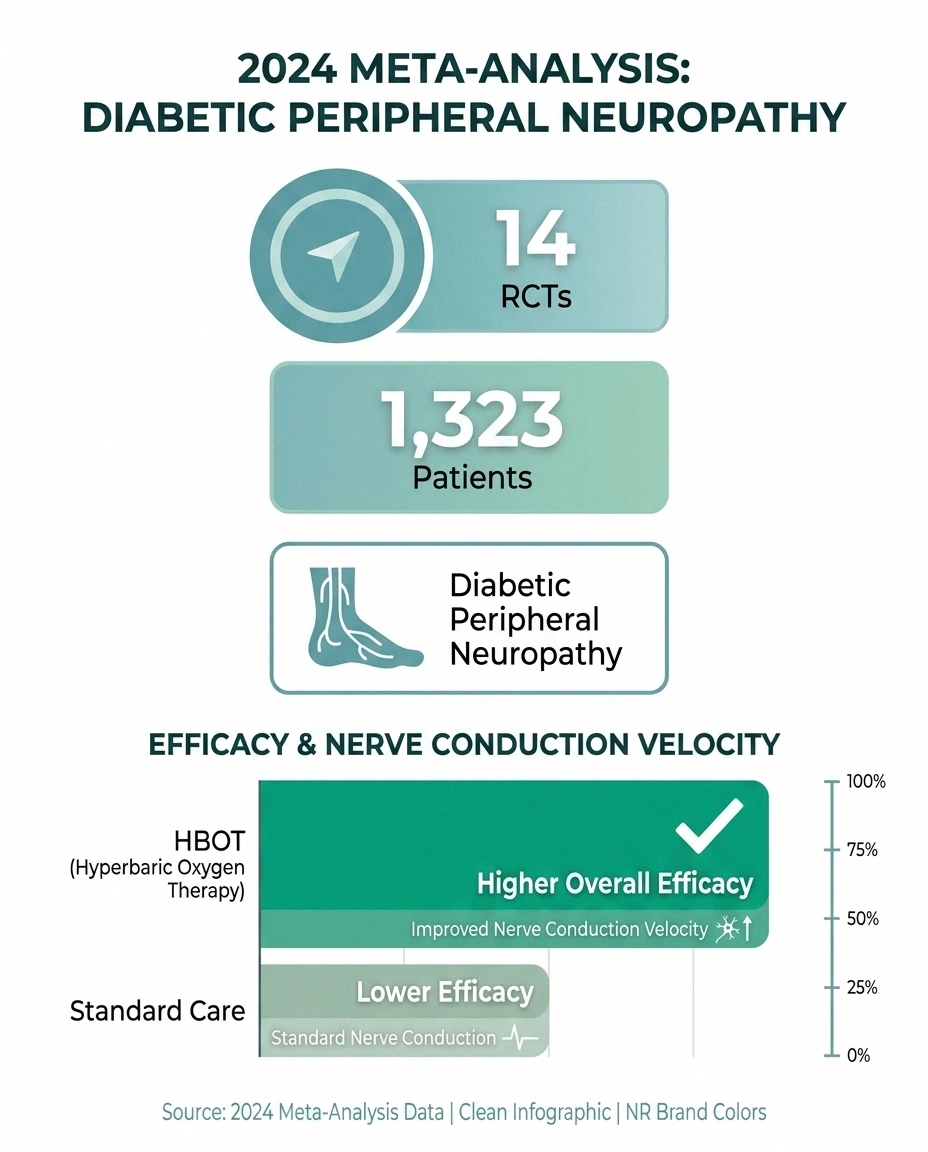
The most important piece of recent research is a 2024 systematic review and meta-analysis published in the journal Medicine that pooled 14 randomized controlled trials with a combined 1,323 patients with diabetic peripheral neuropathy. The reviewers compared HBOT plus standard care to standard care alone.
🔎 Research Says
A 2024 meta-analysis (Medicine journal) pooled 14 RCTs and 1,323 patients with diabetic peripheral neuropathy. HBOT plus standard care produced significantly higher overall efficacy and improved nerve conduction velocity vs. standard care alone — though authors call for higher-quality trials before standardizing.
The results were genuinely interesting:
- The HBOT group showed significantly higher overall treatment efficacy
- Improvements in motor and sensory nerve conduction velocity (a measurable, objective outcome)
- Six adverse events in the HBOT group versus zero in the standard care group, but the difference was not statistically significant
The authors' conclusion is worth quoting carefully: HBOT enhances treatment efficacy and nerve conduction velocity in diabetic peripheral neuropathy, but the conclusions require further validation through high-quality, rigorously designed RCTs to provide more robust scientific evidence.
That's a careful way of saying: the existing studies show real benefit, but many were small, methodology varied, and the field needs better trials before HBOT becomes standard of care.
For other types of neuropathy — chemo-induced, idiopathic, radiation-induced — the evidence is even thinner. There's animal research and small case series, but few rigorous trials.
How Might HBOT Help Damaged Nerves?
The proposed mechanisms are biologically plausible and worth understanding because they help explain who might benefit most.
Proposed Mechanisms of HBOT in Nerve Damage
Reverse Tissue Hypoxia
Forces dissolved oxygen into plasma, reaching nerves with poor microvascular supply.
Stimulate Angiogenesis
Repeated sessions encourage new small blood vessel growth around damaged nerves.
Reduce Oxidative Stress
Counterintuitively upregulates antioxidant defenses and dampens inflammatory cytokines.
Support Schwann Cells & Myelin
Better-oxygenated Schwann cells maintain myelin and may promote remyelination.
Reversing tissue hypoxia. In diabetic neuropathy, microvascular damage leaves the nerves chronically oxygen-starved. The peripheral nerves are unusually sensitive to low oxygen because they have high metabolic demands. HBOT delivers a temporary surge of oxygen that may reach areas otherwise underperfused.
Stimulating angiogenesis. Repeated HBOT sessions appear to encourage the growth of new small blood vessels (angiogenesis). Better blood supply means better long-term oxygen and nutrient delivery to nerves and surrounding tissues.
Reducing oxidative stress and inflammation. Counterintuitively — given that oxygen is involved in oxidative damage — HBOT at therapeutic pressures appears to upregulate the body's antioxidant defenses and dampen inflammatory cytokines that drive nerve injury.
Supporting Schwann cell function and myelin. Better-oxygenated Schwann cells are better at maintaining myelin and supporting axon function. Some animal studies show HBOT promotes remyelination after experimental nerve damage.
Modulating pain pathways. A 2017 study in mice (PMC5446542) showed HBOT increased autophagy in the spinal cord via inhibition of the mTOR pathway, attenuating neuropathic pain. The translation to humans is unclear, but it's another piece of the mechanistic puzzle.
None of these mechanisms is unique to HBOT, and none guarantee a clinical effect. But they explain why the therapy has plausible biology even if the trial evidence is still emerging.
Hard-Shell vs. Soft-Shell Chambers (This Distinction Matters)
Walk into a wellness center or browse online and you'll see two very different categories of HBOT, and they're not equivalent.
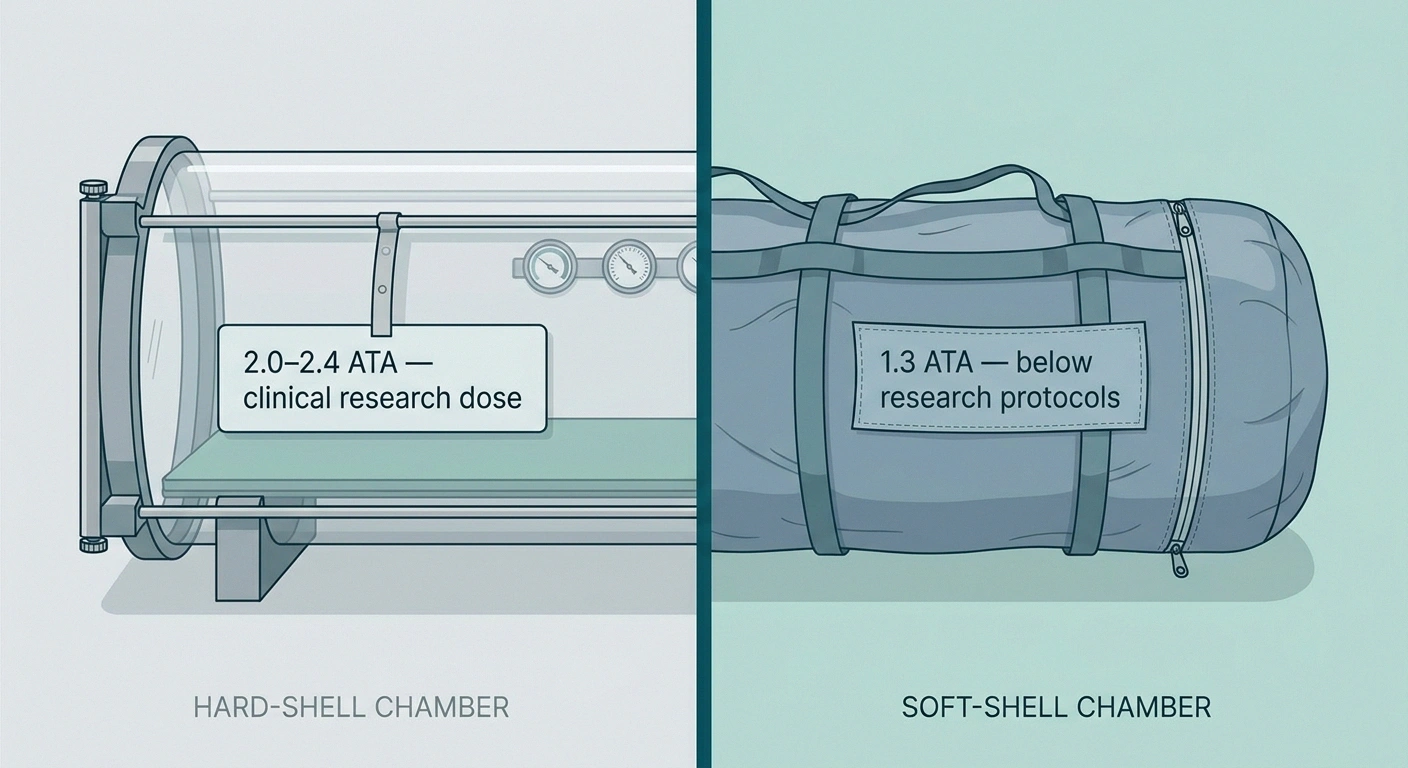
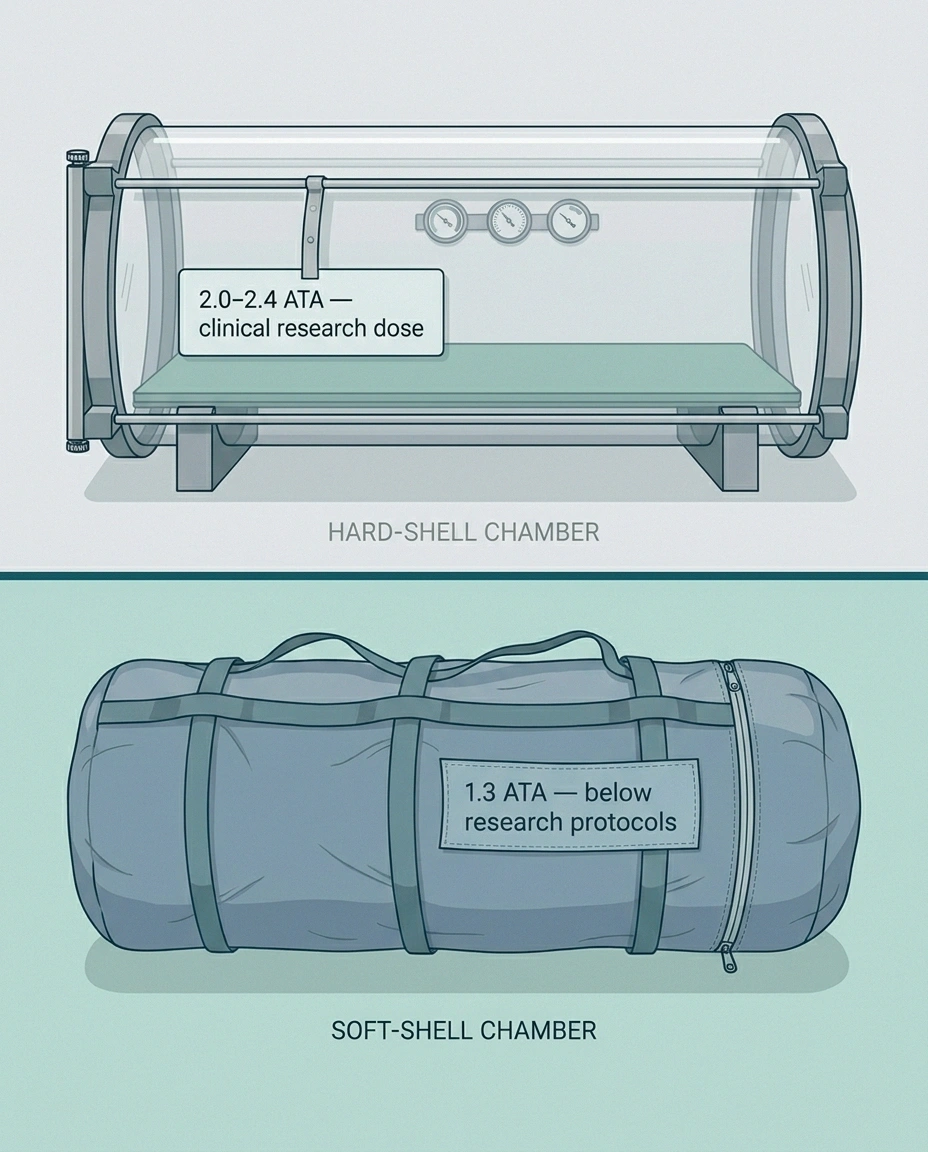
Hard-Shell vs. Soft-Shell HBOT: The Pressure Difference Matters
| Factor | Hard-Shell Medical | Soft-Shell Mild |
|---|---|---|
| Typical pressure | 2.0 – 2.4 ATA | 1.3 ATA |
| Used in trial research? | Yes — most studies | Rarely |
| Setting | Hospital / clinic | Home / wellness center |
| Typical cost | $200-450/session | $5K-25K to buy |
| Likely to deliver therapeutic dose for neuropathy | Yes | Uncertain |
Hard-shell (medical) chambers can pressurize to 2.0-3.0 ATA — the pressure range used in essentially all the published clinical research. These are the chambers used in hospitals and FDA-monitored clinics. They're built to medical safety standards. A typical session is 60-90 minutes at 2.0-2.4 ATA.
Soft-shell (mild) chambers typically pressurize only to 1.3 ATA — about a third of the way to the therapeutic dose. These are sold for home use, often marketed under the term “mild HBOT” or “mHBOT.” They're cheaper to buy and to operate, and there are real safety advantages to the lower pressure. But the research showing benefit for diabetic neuropathy used 2.0-2.4 ATA hard-shell pressures. Whether 1.3 ATA produces meaningful nerve benefit is much less certain.
If someone is selling you on the benefits of “HBOT for neuropathy” and the device is a soft-shell home chamber, ask whether the trial evidence they're citing was conducted at the same pressure their device delivers. Often the answer is no.
What Will It Cost (Time, Money, and Effort)?
Let's be honest about the practical commitment, because this matters more than most clinic websites are willing to discuss.
$6K–$15K+
Out-of-Pocket for a Full Course
30-40 sessions × 90 minutes each at $200-450/session. Insurance generally does not cover HBOT for neuropathy alone.
Money. Off-label HBOT for neuropathy in the US typically costs $200-450 per session at private clinics. A 30-40 session course runs $6,000-15,000 or more out of pocket. Soft-shell home chambers cost $5,000-25,000 to buy outright, plus operating costs and maintenance. Insurance — including Medicare — generally does not cover HBOT for plain neuropathy. The exception is if you have a Wagner Grade 3+ diabetic foot ulcer, where HBOT IS covered.
Time. A typical course is 30-40 sessions at 90 minutes each, plus travel time. If you're driving to a clinic three times a week for 10-12 weeks, you're looking at well over 100 hours of total time invested.
Logistics. Most chambers require you to wear cotton clothing only (synthetic fabrics are static fire risks in pure oxygen). No deodorant, no lotions, no makeup. Phones, watches, and metal items are removed. Some people find the confinement claustrophobic and need to acclimate. If you experience ear barotrauma — pressure pain in your ears — sessions can be uncomfortable until you learn to equalize.
Risks and Contraindications

HBOT is generally safe in trained hands, but it's not without risks.
Pre-Treatment Screening Required
HBOT is contraindicated with untreated pneumothorax, certain chemotherapy drugs (bleomycin, doxorubicin), severe CO2-retaining COPD, and recent ear/sinus surgery. Always disclose your full medication list and medical history before starting.
Common side effects:
- Middle ear barotrauma — pressure pain in the ears, the most common issue. Learning to equalize (yawn, swallow, gentle Valsalva) usually solves it. Severe cases may cause eardrum perforation.
- Sinus pressure — similar mechanism, especially with congestion or allergies.
- Temporary myopia — vision can become more nearsighted during a course of HBOT and typically returns to baseline within weeks of finishing. Don't update your glasses prescription mid-course.
- Claustrophobia — chambers are sealed; some people need to acclimate gradually.
Serious risks (rare):
- Oxygen toxicity (seizures) — more likely at higher pressures and longer durations
- Pulmonary oxygen toxicity — typically only with very prolonged exposure
- Fire risk — pure oxygen environments are highly flammable; this is why no synthetics or flammable products are allowed
Contraindications:
- Untreated pneumothorax (collapsed lung) — absolute contraindication
- Certain chemotherapy drugs (e.g., bleomycin, doxorubicin) — discuss with oncology
- Severe COPD with CO2 retention
- Recent ear or sinus surgery
- Inability to equalize ear pressure
If you're considering HBOT, your doctor should review your medication list and medical history before clearing you. Pre-treatment chest X-ray is sometimes done to rule out occult pneumothorax.
Will Insurance or Medicare Cover HBOT for Neuropathy?
For peripheral neuropathy as a standalone condition: almost never. Medicare and most private insurers cover HBOT only for the 13 FDA-approved indications. The diabetic foot ulcer indication is the loophole — if you have a non-healing diabetic foot ulcer of Wagner Grade 3 or higher, HBOT IS covered, and the nerve benefit may come along incidentally.
For details on what Medicare covers and doesn't, the neuropathy and Medicare coverage guide breaks down the gaps.
Some clinics will offer “cash pay” rates that are slightly more affordable, particularly if you commit to a full course upfront. Negotiation is sometimes possible. Always ask.
Who Might Reasonably Consider HBOT for Neuropathy?
HBOT isn't for everyone, and given the cost and time commitment, it deserves careful thought. Here are situations where considering it is reasonable:
You have diabetic peripheral neuropathy with a non-healing foot ulcer. This is the strongest case. The ulcer indication is FDA-approved AND Medicare-covered, and the nerve benefit may come as a bonus.
You've exhausted other reasonable options. If you've genuinely tried gabapentin, duloxetine, pregabalin, topical agents, physical therapy, and addressed underlying causes (blood sugar control, B12 deficiency, alcohol exposure), HBOT becomes a more reasonable next step.
You can afford it without significant financial harm. Spending $10,000+ on a treatment with promising-but-not-definitive evidence is reasonable for someone with means; for someone for whom that's a serious financial sacrifice, the math is harder.
You can commit to a full course at therapeutic pressure. Half-courses at sub-therapeutic pressures are unlikely to provide meaningful benefit. Going all in on 30-40 sessions at 2.0-2.4 ATA is the protocol most likely to produce results.
And situations where HBOT is probably NOT a good fit:
You're hoping it will reverse permanent axonal loss. No therapy reliably regrows nerves with established axonal damage. Whether neuropathy can be reversed depends heavily on type, cause, and stage.
You're considering it instead of, not in addition to, standard care. HBOT is an adjunct, not a replacement for blood sugar control, medication, lifestyle changes, and addressing root causes.
The clinic offering it is using a soft-shell chamber at 1.3 ATA but citing trials done at 2.0-2.4 ATA. The pressures aren't equivalent.
Honest Expectations
If you decide to try HBOT for neuropathy, here's what realistic expectations look like:
Track Outcomes Objectively
If you commit to a course, track pain scores, walking distance, and sensory symptoms in a diary. After 30-40 sessions and $10K+, you'll want real data — not hope or skepticism — to judge whether it worked for you.
You may notice gradual improvement over the course of 20-40 sessions — typically not dramatic week-to-week, but sometimes recognizable in retrospect after a full course. Some people notice less burning, less numbness, better sleep, or improved sensation. Others notice nothing.
The benefit may not be permanent. Some studies show maintenance of improvement at 6-12 months; others show return of symptoms over time. Whether maintenance sessions help is unclear.
The therapy is not a cure. Even responders typically retain some neuropathy and still benefit from continuing other treatments.
If you respond well, the people around you may notice changes you don't — improved walking confidence, less complaint about foot pain, better sleep. Track outcomes objectively (a pain diary, a symptom score) so you can make a real assessment at the end of a course rather than relying on hope or skepticism alone.
Frequently Asked Questions
Does hyperbaric oxygen therapy work for neuropathy?
A 2024 meta-analysis of 14 randomized trials with 1,323 patients with diabetic peripheral neuropathy found that HBOT plus standard care produced significantly higher overall treatment efficacy and improved nerve conduction velocity compared to standard care alone. The effect is real but the studies have varied methodology, and the field calls for higher-quality trials. For non-diabetic neuropathy, the evidence is much thinner. HBOT is not FDA-approved specifically for peripheral neuropathy.
How many HBOT sessions are needed for neuropathy?
Most clinical protocols use 20 to 40 sessions of 60 to 90 minutes each, scheduled 3 to 5 times per week. The total course typically takes 6 to 12 weeks. Half-courses at fewer sessions are unlikely to produce meaningful benefit based on the trial protocols. Some clinics recommend a re-evaluation after 20 sessions to decide whether to continue or stop.
Does insurance cover HBOT for neuropathy?
Generally no. Medicare and most private insurers cover HBOT only for the 13 FDA-approved indications, which do not include plain peripheral neuropathy. The exception is diabetic foot ulcers of Wagner Grade 3 or higher — these are covered, and the nerve benefit may come along with the ulcer treatment. Off-label HBOT for neuropathy alone typically costs $200 to $450 per session paid out of pocket.
How much does HBOT cost for neuropathy?
Per-session costs at US clinics typically range from $200 to $450 for off-label use. A standard 30 to 40 session course runs $6,000 to $15,000 or more. Soft-shell home chambers can be purchased for $5,000 to $25,000 but typically deliver only 1.3 ATA pressure, which is below the 2.0 to 2.4 ATA used in clinical trials. Insurance rarely covers any of these costs for neuropathy.
What's the difference between hard-shell and soft-shell hyperbaric chambers?
Hard-shell medical chambers can pressurize to 2.0 to 3.0 ATA — the range used in clinical research. They are built to medical-grade safety standards and used in hospitals and FDA-monitored clinics. Soft-shell mild HBOT chambers typically pressurize only to 1.3 ATA, which is well below the trial protocols. Whether soft-shell pressures produce meaningful nerve benefit is much less certain. If a clinic cites neuropathy research, ask whether their device delivers the same pressure as the studies.
Can HBOT reverse nerve damage?
HBOT does not reliably reverse permanent axonal loss. It may improve nerve conduction velocity and symptoms in nerves that are damaged but not destroyed, particularly in diabetic neuropathy where microvascular hypoxia is part of the cause. Realistic expectations are gradual improvement over a course of treatment, not full reversal. Whether benefits persist long-term is still an open research question.
What are the risks of HBOT?
The most common side effect is middle ear barotrauma — pressure pain in the ears — which typically resolves with techniques to equalize ear pressure. Other common issues include sinus pressure, temporary myopia (returns to baseline after the course), and claustrophobia. Serious but rare risks include oxygen toxicity seizures and fire risk in the oxygen-rich environment. HBOT is contraindicated in untreated pneumothorax, certain chemotherapy regimens, and severe COPD with CO2 retention.
Is HBOT safe for diabetic neuropathy?
For most patients with diabetic peripheral neuropathy, HBOT at standard pressures is well tolerated. The 2024 meta-analysis of over 1,300 patients reported six adverse events in the HBOT group versus zero in standard care, with no statistically significant difference. The most common issues were ear and sinus pressure problems. Patients on certain chemotherapy drugs, with untreated pneumothorax, or with severe lung disease should not undergo HBOT. A pre-treatment evaluation is standard.


