If you have neuropathy and you are scheduled for any kind of procedure — a knee replacement, a colonoscopy, a hernia repair, a dental implant under sedation — there is a conversation you need to have before the day of surgery. Most people do not have it, because nobody tells them they should. This piece is so you can.
I'm Janet Ellis. I am a community advocate who has lived with neuropathy for years; I am not a doctor or an anesthesiologist. What I can do is translate what the medical literature actually says about operating on people who already have nerve damage, and turn it into a practical script you can use with your own surgical team. The stakes are real but the prep is manageable.
Why This Conversation Matters
People with pre-existing peripheral neuropathy have a higher rate of perioperative nerve injury than the general population. This is not a fringe observation — it is documented across major reviews of anesthesia-related nerve injuries. The reason is something clinicians call the “double crush” idea: a nerve that already has one source of damage is more vulnerable to a second insult. The second insult can be small — a tourniquet held a little long, an arm positioned a little awkwardly under drapes, a regional block that nicks a nerve that was already irritated. In a healthy person these things often pass without trace. In a person with neuropathy, they sometimes do not.
Pre-existing neuropathy raises perioperative nerve injury risk through the “double crush” effect — but the same care that protects you is well documented. A pre-op baseline, a clear anesthesia conversation, deliberate positioning, and a one-page summary handed to every clinician do most of the protective work.
That is the bad news, and you should know it. The good news is that the same literature documents what actually helps: a clear pre-op neurological baseline, a thoughtful conversation about anesthesia choice, deliberate positioning and padding decisions, and an explicit plan for how new symptoms get reported and acted on afterward. None of this is exotic. All of it requires that your surgical team knows what they are working with — which means it requires you to tell them, clearly and early.
“Disclose Every Time” — Why This Sounds Excessive and Isn't
Every surgical encounter involves at least three or four separate teams that may not perfectly communicate: the surgeon's office, the pre-op nurse, the anesthesiologist, the OR team, and sometimes a pre-admission testing department. Your neuropathy may be in the surgeon's chart and somehow not in the anesthesiologist's notes. The way you protect against this is by mentioning it to every single person who touches your care, every time you see them. On every form, in every conversation, including the day-of intake nurse who is just confirming your name.
This feels excessive. It is not. It is what closes the chart-to-chart gaps that exist in every hospital. Bring a one-page neuropathy summary — type, severity, current medications, most recent EMG/NCS date and findings if you have one — and hand a copy to each clinician. You are not being difficult; you are giving them the information that lets them protect you.
The Pre-Op Neurological Baseline
One of the most useful things you can ask for is a documented pre-operative neurological examination. The reason is simple: if a new symptom appears after surgery, the only way anyone can tell whether it is new or pre-existing is by comparison to a baseline that was recorded before you went into the OR.
Major reviews of perioperative nerve injury, including the Mayo Clinic Proceedings descriptive review and the 2018 Anaesthesia review by Hewson et al., document a higher rate of nerve injury in patients with pre-existing neuropathy and identify the “double crush” mechanism. The same literature consistently recommends pre-op neurological examination, deliberate positioning and padding, and clear post-op vigilance protocols.
If you have had a recent EMG (electromyography) or nerve conduction study, bring the report. Our guide to reading EMG and nerve conduction results can help you make sense of what the report says. If you do not have a recent one, you can still ask the surgical team or your neurologist to document where you have numbness, weakness, or reduced sensation. Even a simple written note of “decreased sensation to monofilament testing in both feet, baseline pre-op,” dated and signed, is far better than nothing. It changes the conversation entirely if a new symptom shows up post-op.
General Anesthesia vs Regional Anesthesia — The Real Trade-Off
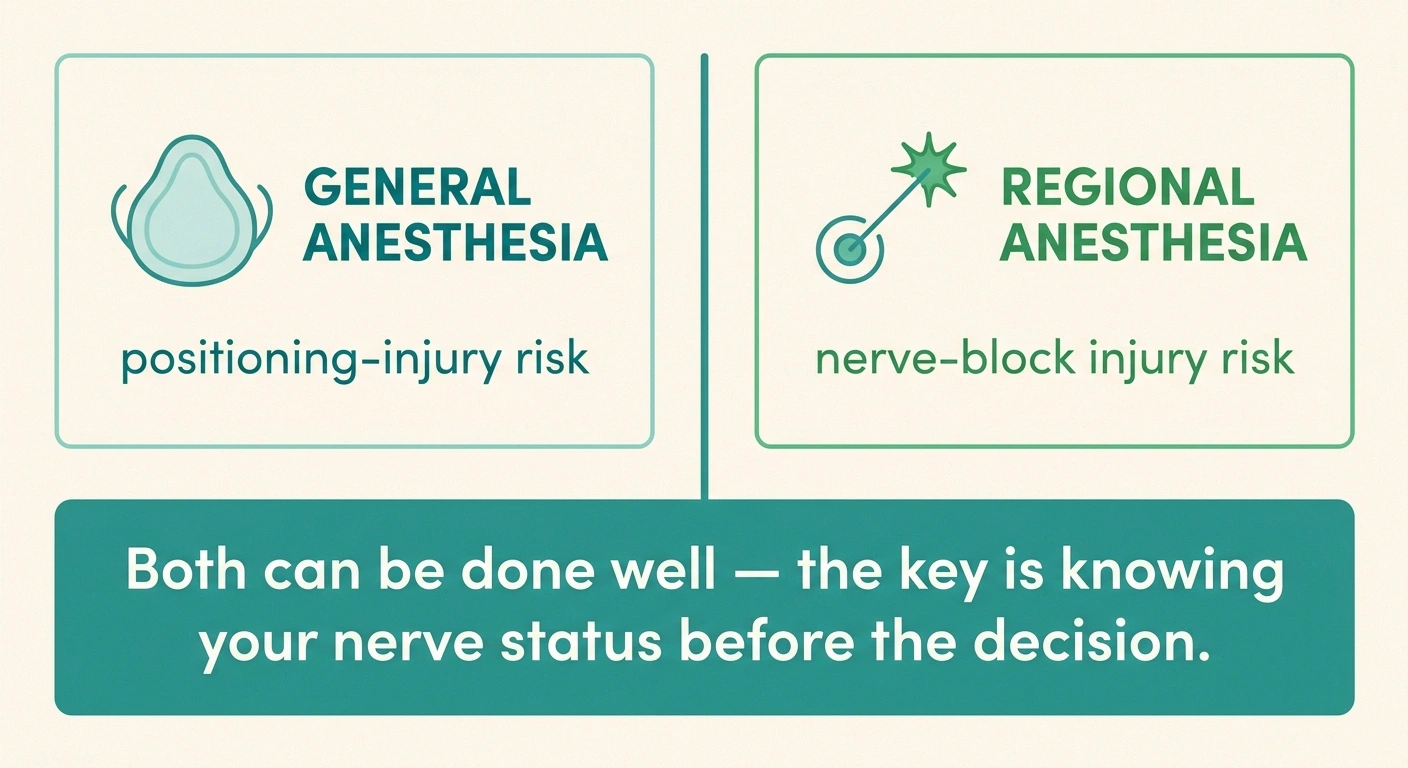
One of the questions you should expect to discuss is the type of anesthesia. The simplified version is that general anesthesia (you are fully unconscious) carries the risk of positioning-related nerve injury — pressure on the ulnar nerve at the elbow, the brachial plexus at the shoulder, the peroneal nerve at the knee. Regional anesthesia (a nerve block or spinal/epidural that numbs a specific area) avoids positioning concerns for that region but introduces its own small risk of direct nerve injury from the needle or from the local anesthetic.
General vs Regional Anesthesia — The Real Trade-Off
Mitigation: Deliberate padding, position changes, surgical team alerted to your existing weak areas.
Mitigation: Ultrasound + nerve stimulator + injection pressure monitoring (“triple guidance”). Ask whether your existing neuropathy in the region changes the choice.
Both can be done well. The point is making sure the anesthesiologist knows your nerve status before choosing.
Your One-Page Neuropathy Summary
Hand a printed copy to every clinician — surgeon, pre-op nurse, anesthesiologist, intake nurse.
For someone with existing neuropathy, both options can be done well and both have considerations. The point of the conversation is not for you to dictate which to use — that decision belongs to your anesthesiologist, who knows the specific procedure and your specific case. The point is to make sure the anesthesiologist knows about your neuropathy before making the choice, so the trade-off they are weighing includes your existing nerve status. If a nerve block is being proposed in the same region where your neuropathy is worst, that is the moment to ask, clearly: “Given my existing neuropathy in this area, what is your plan to reduce the risk of further injury, and is regional still the best option?”
Positioning, Padding, and Tourniquets
Most surgery-related nerve injuries are positioning injuries, not anesthetic injuries. They happen because an unconscious body holds an awkward position for hours without the protective reflex of “ow, this hurts” that an awake body uses to shift. Modern OR teams are well aware of this and use careful padding for known pressure points — but the team needs to know which areas are already compromised.
Tourniquets, used for procedures on the arms or legs to reduce bleeding, are another specific risk. Tourniquet-related nerve injury is more likely in people with pre-existing neuropathy, longer cuff times, and certain underlying conditions. It is reasonable to ask: “Will a tourniquet be used? For how long? Is the time being kept as short as the procedure allows, given my neuropathy?”
Your Neuropathy Medications Around Surgery

This is one of the things that catches people, because the instructions can vary by hospital, by surgeon, and by drug. A few useful general principles, all of which you should confirm with your own anesthesia team:
Duloxetine (Cymbalta) + intraoperative drugs: raises serotonin-syndrome risk if combined with meperidine, tramadol, or methylene blue. The anesthesia team needs to know you're on it.
Most supplements: stopped 1–2 weeks before surgery (alpha-lipoic acid, acetyl-L-carnitine, fish oil, turmeric). Confirm the specific list with your team.
- Gabapentin and pregabalin (Neurontin, Lyrica) are usually continued through surgery. They actually help reduce post-operative pain and lower opioid needs in many cases. Your team needs to know the dose and timing.
- Duloxetine (Cymbalta) is usually continued, but it is on a short list of medications with a specific intraoperative concern: it raises the risk of serotonin syndrome if combined with certain other drugs the anesthesia team may use, including meperidine, tramadol, methylene blue, and some intra-operative serotonergic agents. The team needs to know.
- Opioids for chronic neuropathy pain create tolerance that affects how much post-operative pain medication you will need. Tell the team your typical daily dose. Stopping abruptly around surgery causes withdrawal and is not the answer; planning is.
- Topical capsaicin or lidocaine patches are usually fine but should not be applied to the surgical site.
- Alpha-lipoic acid, acetyl-L-carnitine, and other supplements for neuropathy: the standard guidance is to stop most supplements one to two weeks before surgery because some affect bleeding or interact with anesthesia. Ask specifically about each one you take.
None of this is something to figure out in the pre-op holding area the morning of surgery. It is the conversation you have at your pre-op appointment a week or two ahead.
Blood Sugar If Your Neuropathy Is Diabetic
If your neuropathy is related to diabetes, ask about the perioperative glycemic plan. Tight glucose control before and during surgery reduces nerve-stress, infection risk, and healing complications. The plan may involve adjusting your insulin or oral medications the morning of surgery — these adjustments are specific to your drugs and your procedure and should be made by the team, not by you. Bring your current diabetes medication list and your most recent A1c. Our diabetic neuropathy guide covers the bigger picture of how blood sugar control protects nerves.
What to Watch for After Surgery

The first 24 to 48 hours after waking up are when new nerve symptoms are most likely to appear if positioning or anesthesia was a factor. Pay attention to:
New numbness, tingling, or weakness in an area unrelated to surgery; a sudden symptom flare beyond expected post-op stress; a “patch” of altered sensation; a foot or hand that suddenly doesn't work; or electric/burning pain in a specific nerve distribution. Call the same day — early reporting opens the window for action.
- New numbness, tingling, or weakness in areas not directly related to the surgical site (especially the opposite arm or leg).
- A sudden worsening of existing neuropathy symptoms beyond what would be expected from surgery-related stress.
- A new “patch” of altered sensation — a numb spot on a finger, a strip of skin that feels different, a foot that suddenly drops when you try to walk.
- Disproportionate pain in a specific nerve distribution (an electric, burning quality rather than the typical surgical ache).
Report these immediately. Not at your one-week follow-up. Immediately, while you are still in the recovery area or before discharge if possible. Early reporting gives the team a chance to act — and gives you the documentation that something new started in the perioperative window, which matters for everything that follows.
The Short Script for Day-Of

When the anesthesiologist comes to talk to you in the holding area, they have about three minutes. Make those three minutes count with something like this:
Your Four Lines for the Pre-Op Holding Area
- “I have peripheral neuropathy in [location], with [type/severity]. I have a one-page summary here for your records.”
- “My last EMG showed [findings] on [date]. I have brought the report.”
- “I take [list], including the dose and time of my last dose this morning.”
- “I would like a clear plan for what we will do if I report new nerve symptoms after surgery.”
That is it. You have just given the anesthesiologist exactly the information that helps them protect you, in the time available. The good ones will respond with their plan; the great ones will adjust something based on what you just told them. Either way, you have done the part that is yours to do.
If Something Goes Wrong
The honest reality is that even with perfect care, some perioperative nerve injuries occur. Most resolve, often over weeks to months, as the nerve recovers from the temporary insult. Some leave residual symptoms. Knowing this in advance does not change the math, but it does change how you interpret the recovery period — a new symptom that is gradually improving is the expected trajectory; one that is worsening or persistent at three months deserves further workup, including a repeat EMG/NCS to compare against your pre-op baseline.
This is also the reason the pre-op documentation matters so much. If you ever need to make a case to a specialist or, in rare cases, to a hospital, the baseline-versus-now comparison is the most important piece of evidence.
The Bottom Line
Surgery with pre-existing neuropathy is not something to avoid — most procedures go fine, and many surgeries (joint replacements, decompressions, vascular procedures) actually improve nerve symptoms by addressing the underlying cause. What it is, is something to walk into informed. The team that knows what you bring is the team that can protect you. The team that does not, cannot. Bringing a one-page summary, a recent EMG, a clear medication list, and the four-line script above is most of the work. Our wider guide to talking to your doctor about neuropathy reinforces the same posture: prepared, specific, and clear.
Frequently Asked Questions
Is it safe to have surgery if I have neuropathy?
For the vast majority of people, yes — but pre-existing neuropathy raises the risk of perioperative nerve injury slightly, which is why the pre-op conversation matters. The same literature that documents the higher risk also documents what protects against it: a clear neurological baseline, deliberate anesthesia and positioning choices, and an explicit plan for reporting new symptoms. Surgery is not something to avoid; it is something to prepare for.
Can anesthesia cause neuropathy?
It can contribute to perioperative nerve injury in two ways. Direct injury from a regional nerve block (the needle or the local anesthetic itself) and positioning-related injury under general anesthesia (an unconscious body cannot shift away from pressure). Both are uncommon and both are more likely in patients with pre-existing neuropathy. Disclosing your neuropathy to the anesthesia team is the single most useful protective step.
Should I take my gabapentin or Lyrica before surgery?
Usually yes — both medications are typically continued through surgery and can help reduce post-operative pain. But the specific instructions belong to your anesthesia team. Bring your medication list, dose, and timing of your last dose to the pre-op appointment, and confirm the plan there. Do not stop these medications on your own without guidance.
What should I tell the anesthesiologist about my neuropathy?
The location and type of your neuropathy, its severity, your most recent EMG or nerve conduction findings if you have them, every medication you take (including supplements), and a specific question about the anesthesia plan if regional anesthesia is being considered in an area where your neuropathy is worst. A one-page written summary handed to the anesthesiologist makes this conversation much more efficient.
Will surgery make my neuropathy worse?
Most of the time, no. Sometimes there is a temporary flare of symptoms in the days after surgery from positioning, swelling, and the systemic stress of the procedure, which typically settles. A small percentage of people experience a more persistent new symptom; this is why the pre-op baseline and the post-op vigilance both matter. Some surgeries — particularly nerve decompression procedures and vascular surgery for ischemic neuropathy — can actually improve nerve symptoms.
Do I need to stop my neuropathy supplements before surgery?
Many anesthesia teams ask patients to stop most supplements one to two weeks before surgery because some affect bleeding or interact with anesthesia medications. This includes common neuropathy supplements like alpha-lipoic acid, acetyl-L-carnitine, fish oil, and turmeric. The specific list depends on the procedure and the team's preferences — ask explicitly about each supplement you take.
What is the double crush phenomenon and why does it matter for surgery?
The double crush idea is that a nerve already damaged by one cause is more vulnerable to a second insult. A small positioning compression that would pass unnoticed in a healthy person may produce a noticeable injury in someone whose nerve was already struggling. This is why pre-existing neuropathy raises perioperative risk, and why padding, positioning, and tourniquet time matter more for these patients.
What should I do if I notice new nerve symptoms after surgery?
Report them immediately — to the recovery-room nurse if you are still there, to the surgeon's office if you are home, and ideally before your scheduled follow-up. Early reporting allows the team to evaluate, document, and intervene if anything is reversible. New numbness, tingling, weakness, or a foot or hand that suddenly does not work as expected all warrant a same-day call.