A few years ago, if you told me that strapping a video-game headset to my face would make my nerve pain quieter, I would have politely raised an eyebrow. I've been around long enough to be skeptical of shiny new things, especially anything promising relief from chronic pain. But the research on virtual reality for neuropathic pain has grown to the point where I can no longer dismiss it — and one VR program is even FDA-cleared and starting to be covered by Medicare. So let's talk honestly about what's real, what's hype, and where it might fit in your life.
This isn't a sales pitch. VR for nerve pain has genuine evidence behind it for some conditions and very thin evidence for others. The most useful thing I can do is walk you through what each of those looks like.
What VR Therapy for Pain Actually Looks Like

When most of us hear “virtual reality,” we think of gamer headsets and video games. The medical version overlaps with that hardware, but the use is very different. A VR therapy program for chronic pain typically looks like this: you put on a head-mounted display, which immerses you visually and audibly in a 3D environment. The environment might be a peaceful nature scene, a guided breathing exercise, a body-awareness training session, or in some programs, a kind of “embodiment” experience where you see and feel a virtual body that responds when you move.
Some programs are short, single-session experiences (10–30 minutes of distraction-based relief during a flare). Others are structured multi-week programs (the FDA-cleared option below is an 8-week home program with a daily session). The goal isn't to entertain you — it's to retrain your nervous system's relationship with pain, or to interrupt pain signals long enough to function.
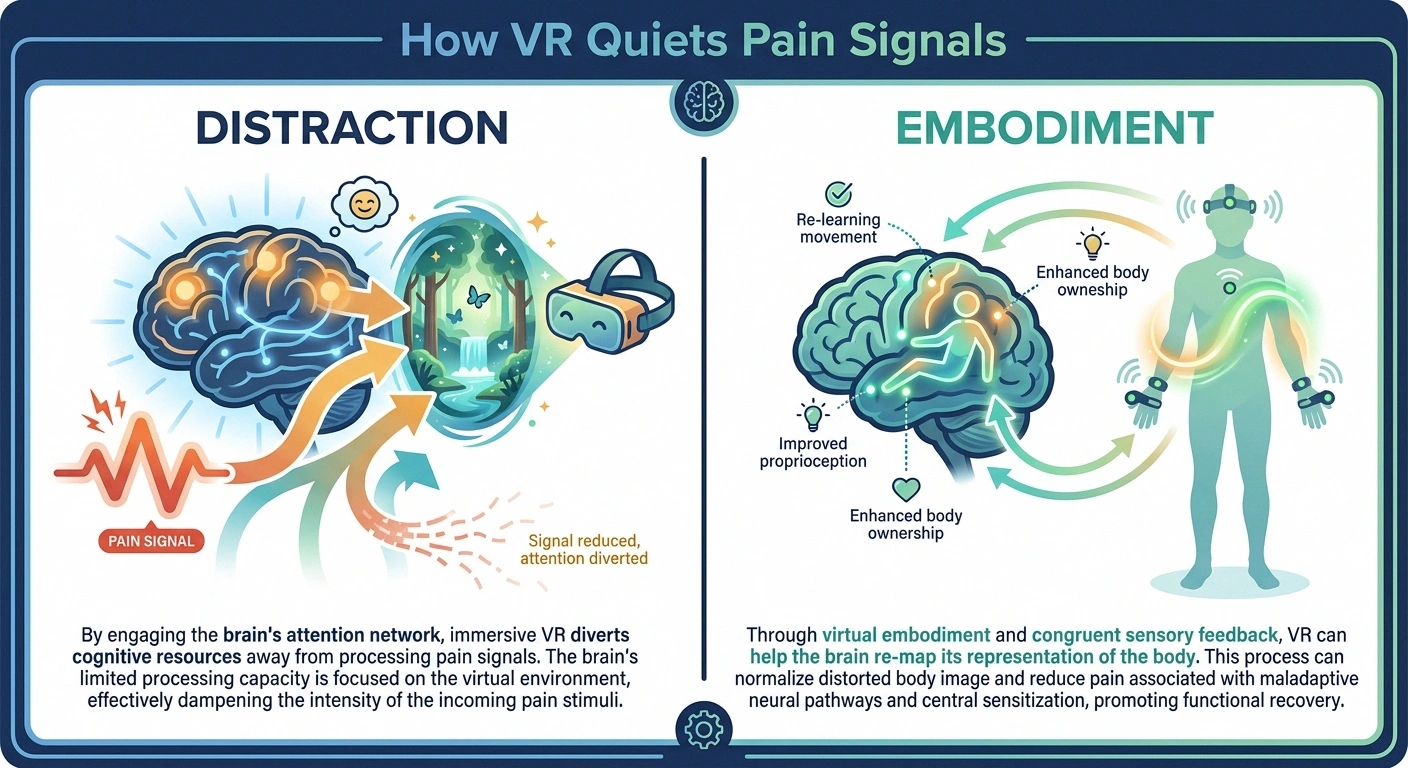
There are two main mechanisms researchers point to:
- Distraction and attention competition. Pain demands attention. VR demands attention more loudly. When the immersive experience occupies the brain's processing capacity, the pain signal — which has been competing for that same bandwidth — gets relatively quieter. This is the same mechanism behind why a captivating movie or absorbing conversation can briefly turn down nerve pain, except VR is more reliable and more controllable.
- Embodiment and body remapping. Some VR programs let you see a virtual version of your body and explore it from new angles. For conditions where the brain's “map” of the affected body part has gotten distorted — phantom limb pain after amputation, CRPS, certain neuropathies — gently remapping that representation can quiet the pain. This is the same principle as old-school mirror therapy for phantom limb pain, only made more flexible by VR.
What the Research Actually Shows
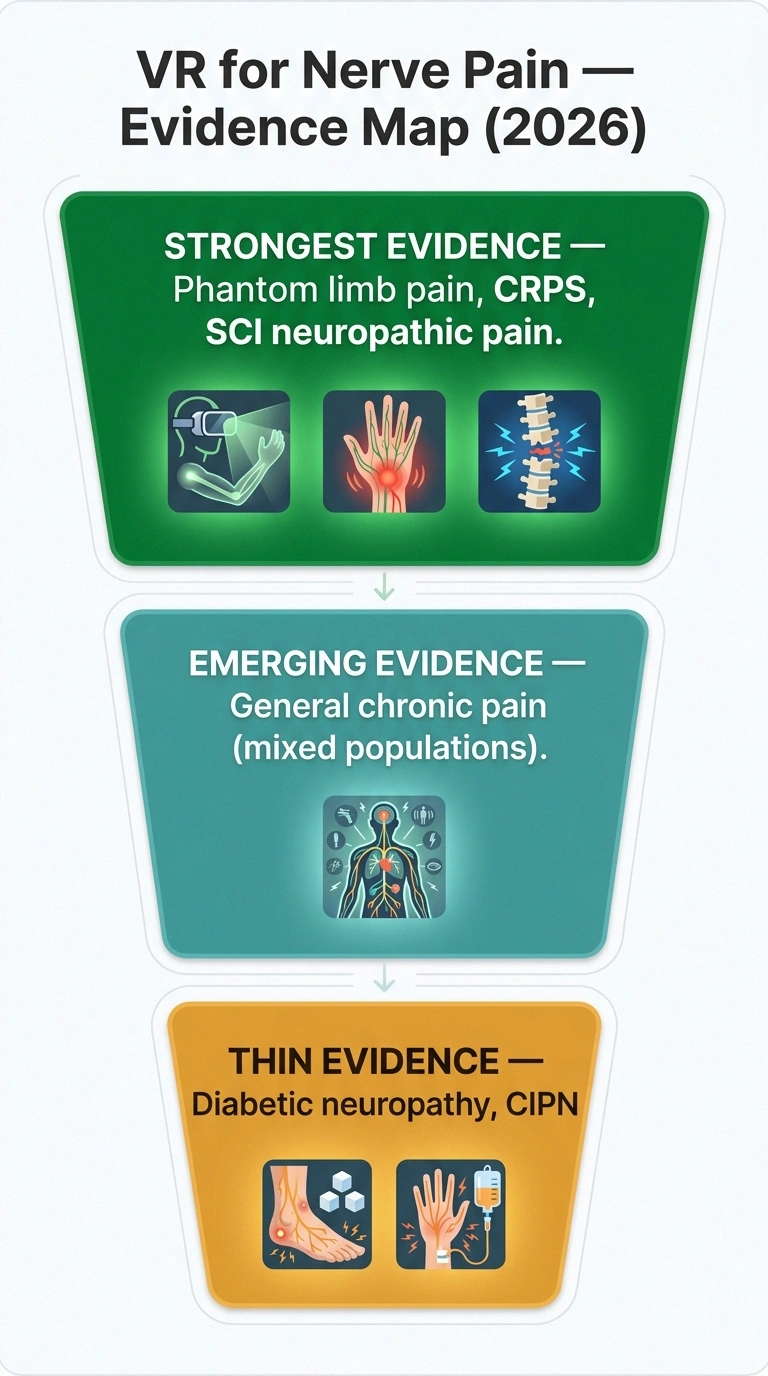
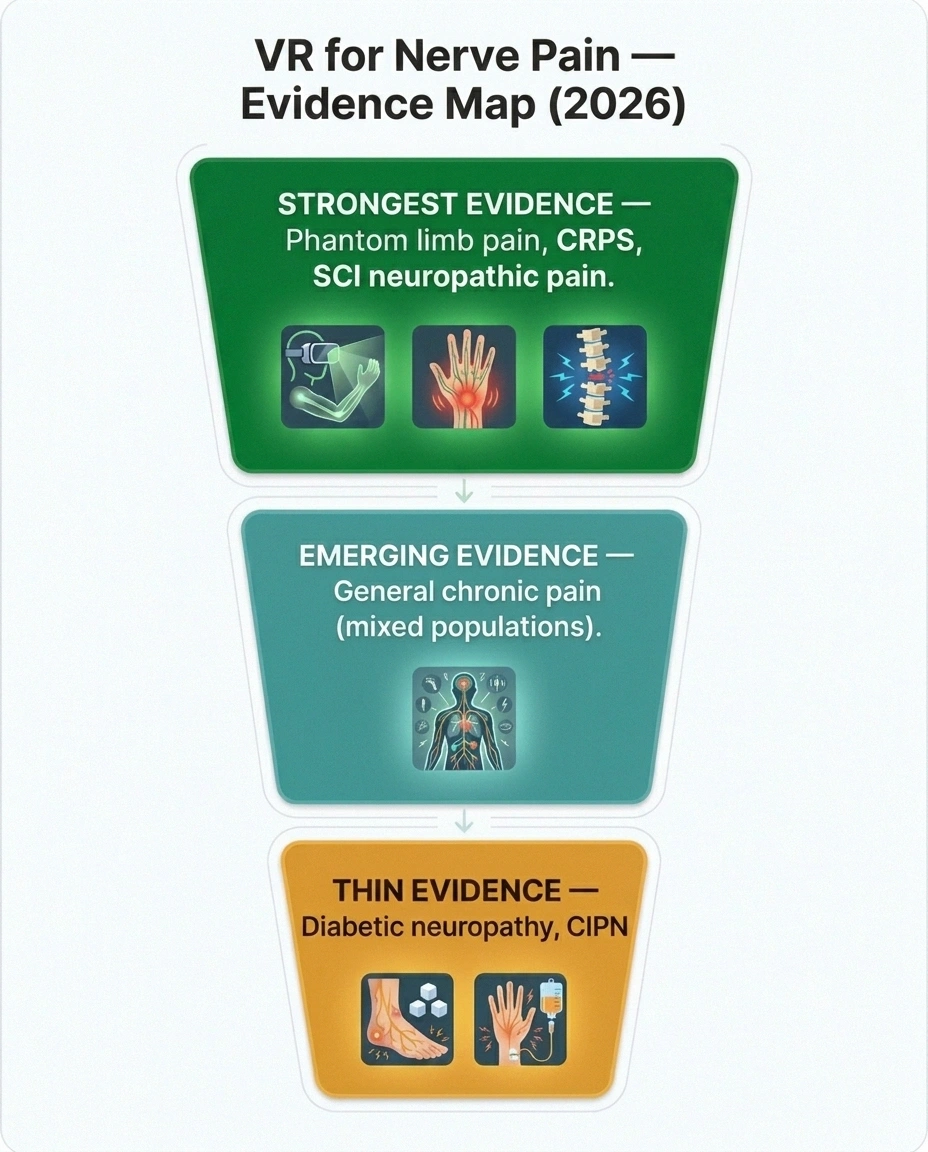
Let me be careful here, because this is where overstatement is common. The evidence for VR in chronic pain is strongest for some specific situations and much weaker for others. Here's an honest map of the landscape.
Strongest Evidence: Phantom Limb Pain and Spinal Cord Injury Neuropathic Pain
This is where VR has been studied the longest and most rigorously. A 2024 pilot randomized controlled trial published in PAIN Reports looked at immersive VR for chronic neuropathic pain after spinal cord injury and found it was feasible, well-tolerated, and produced meaningful short-term pain reductions. Earlier studies of short VR exposure in spinal cord injury patients showed numeric pain ratings dropping from about 5 to about 3 on a 10-point scale during sessions — a significant change.
For phantom limb pain, VR has essentially become the modern, more flexible version of mirror box therapy, which has been used for decades. A 2025 systematic review on body-representation remapping in chronic neuropathic pain found consistent (though modest) benefits across phantom limb, CRPS, and SCI populations.
Emerging Evidence: General Chronic Pain (Including Some Neuropathy)
The most notable 2026 finding comes from a study published in the Journal of Medical Internet Research. It was a 2-year follow-up of a skill-based VR program for what's called “high-impact chronic pain” — pain that significantly limits daily function. At the end of the treatment program, 70% of participants had moved from the high-impact pain category to the low-impact category. One year later, 67% were still there. That's a substantial sustained effect for a non-pharmacological intervention.
Caveat: that study population was mixed — it included neuropathic pain alongside other chronic pain conditions, so we can't say with certainty that pure neuropathic pain patients responded the same as the overall group. Still, the size and durability of the effect is hard to dismiss.
Thinner Evidence: Diabetic Peripheral Neuropathy and CIPN
For the most common forms of peripheral neuropathy that bring readers to this site — diabetic peripheral neuropathy and chemotherapy-induced peripheral neuropathy — the VR evidence is genuinely thin. Small pilot studies show some effect on pain during sessions. Few high-quality trials have been done yet. This is an area to watch, not an area where I'd tell you “the research is in.”
The FDA-Cleared Option: RelieVRx (Formerly EaseVRx)

One specific VR program has crossed a regulatory threshold that matters: RelieVRx (originally called EaseVRx), made by AppliedVR. It received FDA clearance in November 2021 for the treatment of chronic low back pain in adults. It's not cleared for neuropathy specifically, and that's an important distinction. But it represents the first commercial VR therapy for chronic pain to pass FDA review, and many of its underlying skill-building principles (pain neuroscience education, relaxation training, attention shifting, breathing exercises) are exactly the things that may help neuropathic pain too.
The structure: An 8-week home program. A VR headset is shipped to you. Daily sessions of 5–15 minutes. The program teaches a series of cognitive and behavioral skills for managing chronic pain, delivered through VR experiences. You don't need to be tech-savvy — the device is designed for older adults and arrives ready to use.
It requires a prescription from a healthcare provider. As of 2026, it is covered by some Medicare Advantage plans (varies by plan and region), some commercial insurance plans, and is available out-of-pocket for those without coverage. Out-of-pocket cost varies but is typically in the low hundreds of dollars for the 8-week program.
Whether your specific neuropathic pain will respond to a program designed for chronic low back pain is an open question. Some pain specialists are using it off-label for other chronic pain types with mixed reported results. If you're going to try it, the right conversation is with your pain management doctor or neurologist about whether your specific situation is a reasonable fit.
Other VR Programs Worth Knowing About
RelieVRx isn't the only player. The field is moving quickly. A few others to be aware of:
- Karuna Labs. Focuses on movement-based VR for chronic pain, often used in physical therapy clinics rather than at home. Includes graded motor imagery, body-mapping exercises, and movement re-training. Used by some PT and pain practices.
- DeepStream VR. Makes both clinical and home VR pain programs, often used for acute medical pain (burns, wound care) but expanding into chronic pain applications.
- Reducept. A Netherlands-based program with structured pain neuroscience education delivered through VR, now available in several countries.
- Consumer hardware + third-party apps. If you own a Meta Quest, an Apple Vision Pro, or a similar consumer headset, dozens of pain-management and relaxation apps exist on those platforms. These are not regulated medical devices, the quality varies enormously, and your insurance won't be involved. They can still be useful — many patients report meaningful relief from guided meditation and immersive nature apps — but use the same critical eye you'd use for any unregulated wellness product.
Who Should Consider Trying VR Therapy?

VR isn't right for everyone, and I want to be honest about who's most likely to get something out of it.
Good Candidates
- People with chronic neuropathic pain that hasn't been controlled by current medication and therapy
- People looking to reduce reliance on pain medications, especially opioids
- People who want a non-pharmacological tool to add to their existing toolkit (not replace it)
- People who do reasonably well with screen-based learning
- People with sleep disruption from chronic pain — many programs include relaxation modules that have helped some users sleep better
- People with phantom limb pain, CRPS, or post-spinal-cord-injury neuropathic pain (where evidence is strongest)
Probably Not the Right Fit
- People with significant motion sickness or vertigo — VR can make these worse
- People with active severe psychiatric symptoms — immersive experiences can be intense and overwhelming for some patients in acute distress
- People with active seizure disorders that are not well controlled (talk to your neurologist first)
- People with significant vision or hearing impairments that would make the experience inaccessible
- People who simply hate technology and won't use it consistently — VR only works if you actually do the sessions
About 10–15% of users experience some “cybersickness” — nausea, dizziness, or disorientation from VR exposure. For most people this fades with short, gradual sessions. For some, it doesn't, and VR is just not their tool. You'll know within the first few sessions.
What VR Therapy Does NOT Do
I want to be very direct about this, because there's some breathless marketing in this space that needs to be checked.
- Regenerate nerves or reverse the underlying nerve damage
- Replace your medications or your medical management
- Work in a single session for durable benefit — sustained use over weeks matters
- Work the same way for everyone — responses vary substantially person-to-person
VR does not regenerate damaged nerves. It does not reverse neuropathy. It does not heal the underlying nerve damage that's producing your pain. It is a symptom-management tool — sometimes a very effective one — but it doesn't fix what's broken at the nerve level.
VR is not a replacement for medical care. If you have diabetic neuropathy, you still need good blood sugar control. If you have CIPN, you still need your oncology follow-up. If your neuropathy has a treatable underlying cause, you still need to treat that cause. VR is something you add, not something you swap in.
VR is not a one-and-done. The studies that show durable benefit involve consistent use over weeks or months. A single session might feel good in the moment, but the carryover effects come from sustained practice — usually daily sessions over an 8 to 12-week program.
VR effects vary widely between individuals. Some people get profound relief. Some people get modest relief. Some people get none. There's no reliable way to predict which group you'll fall into until you try, which is part of why I think VR is worth considering for people who haven't gotten enough relief from current options — the downside risk is low.
How to Talk to Your Doctor About VR Therapy

If you're interested in exploring VR for your nerve pain, here's how to bring it up productively at your next appointment:
- Frame it as adding a tool, not replacing one. Most doctors are more comfortable with “I'd like to add VR therapy to my current treatment plan” than “I want to stop my medications and try VR instead.”
- Ask whether your insurance covers RelieVRx or any other VR pain program. Coverage varies and is changing rapidly. Your insurance company's customer service line can sometimes tell you faster than your doctor's office can.
- Ask if your pain clinic or PT has a VR-based program. Some pain management practices now have in-clinic VR options that don't require buying a home headset.
- Ask whether your specific type of nerve pain has been studied for VR response. Phantom limb pain, CRPS, and SCI neuropathic pain have stronger evidence. Diabetic neuropathy and CIPN have less.
- If you're going to buy a consumer headset and try an unregulated app, tell your doctor you're doing it. Particularly important if you have a seizure history or significant motion sensitivity.
You may also want to pair VR with other non-pharmacological pain strategies. Several of these have surprisingly good evidence on their own, and VR may amplify their effect: mindfulness meditation for nerve pain, cognitive behavioral therapy for neuropathy, and gentle yoga for neuropathy.
The Bigger Picture: Where VR Fits in Modern Pain Care

I think VR is most useful when you understand what it is: not a cure, not a miracle, but a genuinely new tool that didn't exist for chronic pain patients ten years ago. It joins a growing toolkit of “behavioral pain neuroscience” interventions — things that change how your brain processes pain signals rather than blocking pain receptors with chemistry.
For some people, that toolkit changes everything. For others, it's a useful add-on but not a game-changer. The most honest framing I can give you is this: VR therapy is one more thing on the menu, with a stronger evidence base than it had even three years ago, and a reasonable cost-benefit profile for many people with refractory chronic neuropathic pain. It's worth knowing about. It's worth talking to your doctor about. It may or may not be the thing that helps you.
If you're thinking about how this fits with other newer options, I keep an honest overview of what's in the research pipeline at New Neuropathy Treatments in 2026, and I cover the broader range of non-drug strategies in Neuropathy Treatments Compared and Ranked by Evidence. For the broader emerging-tech space, scrambler therapy and red light therapy are worth understanding too, with their own honest evidence reviews.
The most important thing — and this is true whether we're talking about VR, a new medication, or a new supplement — is that you stay curious, stay critical, and don't give up. The pace of progress in chronic pain care has finally started catching up to what patients have needed for decades. VR is one piece of that. It won't be everyone's answer. But for the right person, at the right time, with the right expectations, it can take some real weight off.
Frequently Asked Questions
Does VR therapy actually work for nerve pain?
The honest answer is: sometimes, for some people, for some conditions. The evidence is strongest for phantom limb pain, complex regional pain syndrome, and spinal cord injury-related neuropathic pain. It is emerging but promising for general chronic pain. It is thinner for diabetic peripheral neuropathy and chemotherapy-induced peripheral neuropathy. A skill-based VR program studied in 2026 showed 67 percent of participants maintained meaningful pain reduction at 1 year, but that study population was mixed. For an individual patient, VR is worth a thoughtful trial if other options have not provided enough relief.
Is VR therapy FDA approved for neuropathy?
No. As of 2026, the only FDA-cleared VR therapy for chronic pain is RelieVRx by AppliedVR, and that clearance is specifically for chronic low back pain, not neuropathy. Some clinicians use it off-label for other chronic pain types, but it is not specifically approved for nerve pain. Other VR programs you may encounter are either unregulated consumer apps or research-stage protocols not available outside a study.
How much does VR therapy for chronic pain cost?
It varies. The FDA-cleared RelieVRx program is covered by some Medicare Advantage plans and some commercial insurance plans. Where covered, your out-of-pocket cost may be a copay only. Without insurance coverage, the 8-week program is typically in the low to mid hundreds of dollars. Consumer headsets like Meta Quest range from a few hundred dollars; unregulated VR apps for pain or relaxation are usually free to $20-50.
Will VR cure my neuropathy?
No. VR is a symptom-management tool. It does not regenerate damaged nerves, reverse neuropathy, or fix the underlying cause of your nerve pain. It can sometimes meaningfully reduce pain intensity and pain interference with daily life, which is a real and valuable outcome, but it is not a cure.
Can I just buy a Meta Quest and download a pain-relief app?
You can, and many people do. The caveat is that consumer VR apps for pain relief are not regulated, so the quality varies enormously. Some are well-designed guided relaxation experiences that closely resemble what's used in clinical research. Others are essentially gimmicks. If you go this route, look for apps with a clear evidence base or a known clinical psychology or pain neuroscience team behind them, talk to your doctor about it, and treat the experience as a stress-management tool rather than medical treatment.
How long do I need to use VR therapy to see results?
It depends on the program. Single-session distraction-based use produces short-term relief during and shortly after the session. Structured programs that teach pain-management skills, like the FDA-cleared RelieVRx, run for 8 weeks of daily sessions, and the durable benefits accrue over that period. Many users report initial benefits within the first 2 weeks but the best sustained outcomes after completing the full program.
What are the side effects of VR therapy?
The most common side effect is cybersickness, a form of motion sickness that affects roughly 10 to 15 percent of users. It produces nausea, dizziness, eye strain, or disorientation, especially during the first few sessions. For most people it fades with short, gradual exposure. People with significant motion sensitivity, certain vestibular disorders, or active seizure disorders should talk to their doctor before starting. Some people also report fatigue from the cognitive engagement of immersive experiences, especially early on.
Is VR therapy a replacement for my neuropathy medications?
No. VR therapy is an addition to your current treatment, not a replacement for it. Decisions about reducing or stopping medications should always be made with the doctor managing your neuropathy. Many patients have been able to reduce their medication doses over time as VR and other non-pharmacological strategies take hold, but that should be a guided clinical decision, not a self-directed substitution.