
It's one of those neuropathy experiences that's hard to explain to someone who hasn't felt it: you step into a lukewarm shower and it feels scalding. You go outside on a mild spring day and your feet start burning. Or the opposite — a winter chill makes the pain so much worse that you dread leaving the house, even when it isn't that cold.
Temperature sensitivity is one of the more disabling and under-discussed aspects of living with peripheral neuropathy. It's not just that you're more sensitive to hot and cold — it's that your perception of temperature can become fundamentally inaccurate in ways that are confusing, unpredictable, and sometimes dangerous.
Here's what's actually happening in your nervous system when temperature stops making sense.
Which Nerve Fibers Are Responsible for Temperature Sensation?
To understand why neuropathy disrupts temperature sensitivity, it helps to know which nerve fibers normally handle temperature.
Key Takeaway
Temperature sensation is carried by small nerve fibers (A-delta and C-fibers) — the same thin, delicate fibers that are most vulnerable in peripheral neuropathy. When they're damaged, the entire temperature-reporting system can become unreliable, distorted, or absent.
Temperature sensation isn't carried by large, fast-conducting nerve fibers — it's the job of the smaller, thinner fibers:
- A-delta fibers are lightly myelinated (thinly insulated) and carry signals for cool and sharp cold sensations. They respond quickly and give you the immediate “that's cold” signal.
- C-fibers are unmyelinated (no insulation) and carry signals for warmth, prolonged cold, and heat pain. They're slower but responsible for the sustained sense of temperature — the lingering warmth of a hot bath, the spreading cold of a winter night.
Both A-delta and C-fibers are categorized as “small nerve fibers” — and they're among the first and most commonly damaged in many types of peripheral neuropathy, particularly small fiber neuropathy, diabetic neuropathy, and chemotherapy-induced neuropathy.
When these fibers are damaged, your temperature sensing system loses precision. The signals it sends become unreliable, distorted, or absent — leading to the full spectrum of temperature complaints that people with neuropathy describe.
Why Cold Makes Neuropathy Symptoms Worse

For the majority of people with peripheral neuropathy, cold is the enemy. There are multiple reasons for this, and they compound each other.
2 m/s
Nerve conduction velocity slows by approximately 2 meters per second for every 1°C temperature drop. For already-compromised neuropathic nerves, cold-weather slowdown can push marginal function into symptomatic territory.
Nerve conduction slows in the cold. The speed at which nerve signals travel is temperature-dependent. Research shows nerve conduction velocity decreases by approximately 2 meters per second for every degree Celsius drop in temperature. For healthy nerves, this slowdown is a minor inconvenience. For nerves already compromised by disease, even a modest temperature drop can push impaired function over the edge into symptomatic territory.
Cold triggers vasoconstriction. When ambient temperature drops, blood vessels in the extremities constrict — the body's way of conserving core heat. This is entirely normal physiology, but it's a problem for nerves that are already receiving inadequate blood supply. Peripheral nerve fibers depend on a network of small blood vessels (vasa nervorum) for oxygen and nutrients. Vasoconstriction reduces this already-compromised supply, worsening symptoms. This is one reason neuropathy and cold weather are so consistently difficult.
Cold activates altered pain pathways. In damaged small fibers, cold can paradoxically trigger burning pain — a symptom called cold-induced dysesthesia or “cold allodynia.” What should feel like cold instead registers as burning or stabbing pain. This is the confusing experience of having feet that feel like they're on fire while they are actually cold to the touch — not imagination, but a specific consequence of how damaged C-fibers process thermal signals.
Cold stiffens muscles and connective tissue. Reduced flexibility in cold temperatures affects movement patterns and increases the load on already-sensitive nerves, contributing to symptom flares beyond just the direct nerve-cold interaction.
Why Heat Can Also Make Neuropathy Worse

Heat sensitivity in neuropathy is less universal but affects a significant portion of people — and it operates through different mechanisms.
Heat increases inflammatory signaling. Elevated tissue temperature accelerates metabolic processes, including the inflammatory pathways that contribute to nerve pain. For people with inflammatory neuropathies or whose nerve damage involves significant inflammation, heat can trigger and amplify pain responses.
Blood shifts away from extremities. In hot conditions, blood flow is redirected to the skin for cooling — and paradoxically away from the deep tissues. This can reduce circulation to peripheral nerves, similar to but opposite in mechanism from cold vasoconstriction. The end result — reduced nerve perfusion — can be similar.
Heat lowers the threshold for thermal pain. In damaged small fibers, heat pain thresholds are often reduced — a process called thermal hyperalgesia. What would feel like warm (but not painful) heat to a healthy person activates pain pathways in damaged fibers at much lower temperatures. A shower that would be comfortable for your family members produces a burning sensation in your feet.
People with multiple sclerosis have a well-known and dramatic heat sensitivity (Uhthoff's phenomenon) that briefly worsens their neurological symptoms with any rise in body temperature. A similar but usually less dramatic effect occurs in some peripheral neuropathy patients — particularly relevant if your neuropathy has any involvement of the autonomic nervous system. If summer heat or hot baths consistently worsen your symptoms significantly, discussing this with your neurologist is worthwhile. See also: neuropathy and heat sensitivity.
Autonomic Neuropathy and Temperature Regulation
There's a second dimension of temperature problems in neuropathy that goes beyond sensation — the body's ability to regulate its own temperature.
Autonomic Involvement
If you notice you rarely sweat in numb areas, overheat more easily than you used to, or have areas that sweat excessively while others are completely dry — these are signs of autonomic fiber involvement beyond simple sensory neuropathy. Mention them specifically to your neurologist, as they affect how your condition is classified and managed.
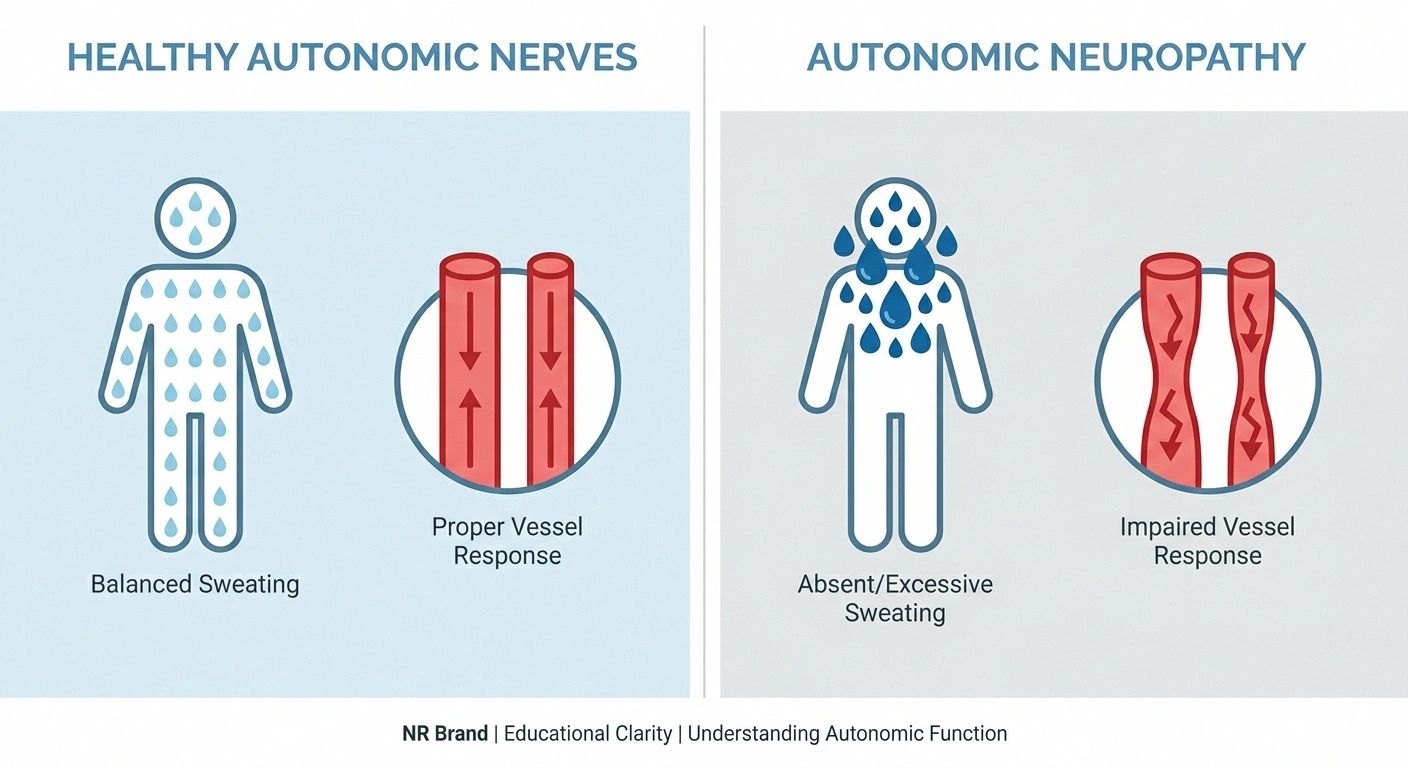
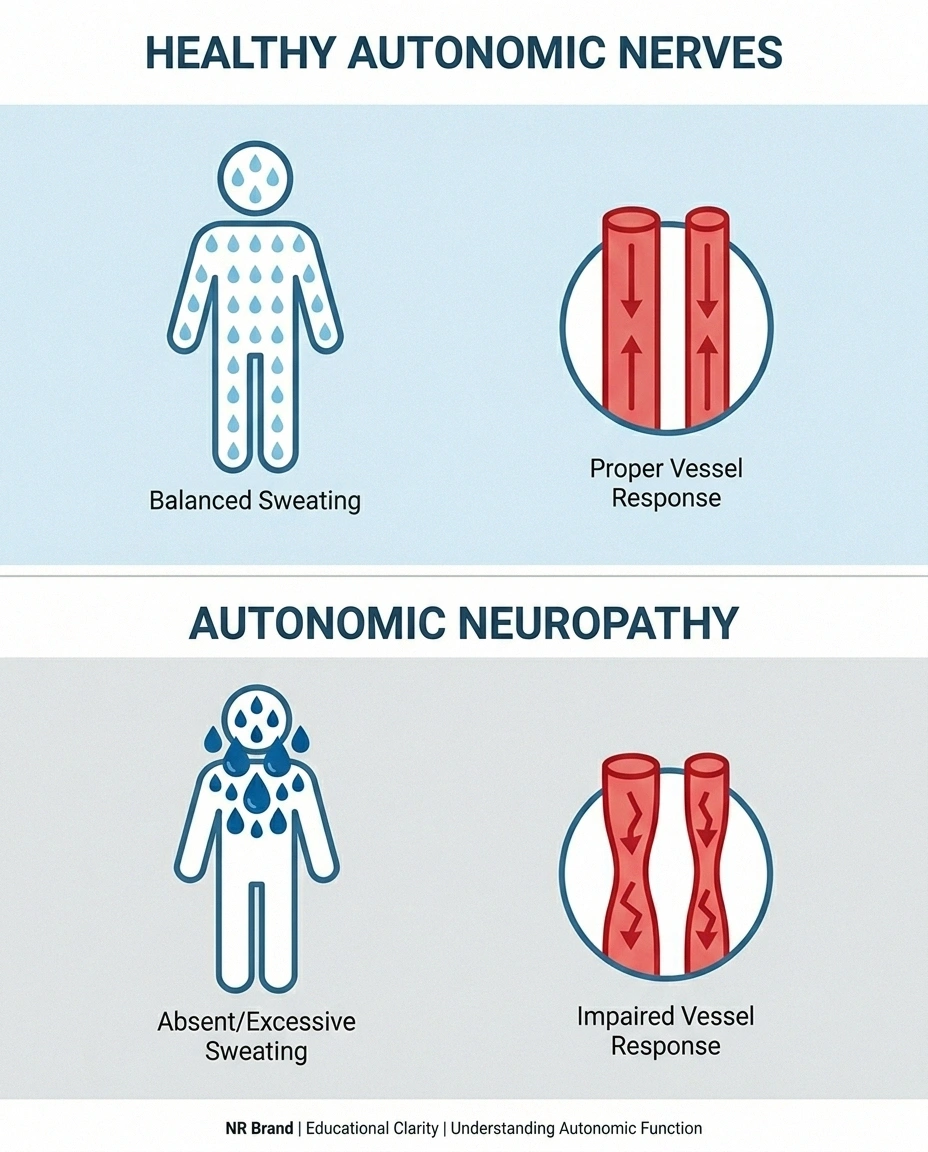
Autonomic nerves control sweat glands, blood vessel diameter, and other processes that manage body temperature. When autonomic neuropathy affects these systems, thermoregulation itself can go wrong:
Anhidrosis (reduced or absent sweating): Autonomic damage to sweat glands in affected areas causes reduced or absent sweating. Without sweating, the body can't cool itself properly in those regions. In hot weather, this creates a genuine overheating risk — particularly dangerous if large areas of the body are affected.
Compensatory hyperhidrosis: When some areas can't sweat, other areas sometimes compensate by sweating excessively. This creates a mismatch — one part of the body is dry and overheating while another is drenched — a disconcerting experience that's not well understood even by many healthcare providers.
Impaired vascular response: Healthy autonomic nerves dynamically adjust blood vessel diameter to manage heat distribution. Autonomic neuropathy impairs this, meaning blood redistribution in response to temperature changes becomes sluggish or absent. Both overheating and overcooling become more likely.
If you notice you rarely sweat in areas that are numb, or if you seem to overheat more easily than you used to, discussing this with your doctor is important — these are signs of autonomic involvement that may need evaluation.
The Dangerous Side: When You Can't Feel Temperature Accurately

Temperature sensitivity in neuropathy isn't only about pain and discomfort — there's a safety dimension that deserves direct attention.
Safety Warning: Temperature Burn Risk
When temperature sensation is impaired, burns can occur without any warning pain. Take these precautions:
- Test bath water with a thermometer — not your neuropathic foot or hand
- Never use a heating pad directly on neuropathic skin or fall asleep with one
- Use oven mitts even when things feel manageable
- Inspect skin visually after temperature exposure rather than relying on sensation
When sensory neuropathy is severe enough, temperature perception doesn't just become distorted — it disappears. People lose the ability to accurately detect how hot or cold something is with the affected body part. This creates real hazards:
Burns from hot water: People with significant foot or hand neuropathy regularly burn themselves testing bath or dishwater temperature with their feet or hands. The recommended practice is to test water temperature with a thermometer or use a temperature-sensitive tap — not with the numb limb itself.
Burns from heating pads and electric blankets: Applying heat for comfort can cause burns if sensation is impaired. Heat pads should be used with timers, set to low temperature, and placed on unaffected or less-affected skin areas. Never fall asleep with a heating pad directly on neuropathic skin.
Frostbite from cold exposure: Cold-exposed neuropathic skin can develop frostbite without the usual warning pain. Checking for skin changes visually after cold exposure — rather than relying on sensation — is important in severe neuropathy.
For people with diabetic neuropathy, this is part of the reason neuropathy foot care is so extensively emphasized — visual inspection and protective footwear substitute for the sensory protection that damaged nerves can no longer provide.
Temperature as a Diagnostic Tool
Interestingly, the specific pattern of temperature sensitivity changes in neuropathy carries diagnostic value.
Research Says
Warm detection threshold (WDT) and cold detection threshold (CDT) — measured through Quantitative Sensory Testing — are among the most sensitive early markers of small fiber neuropathy. They can show abnormality before standard nerve conduction studies detect any change.
Clinical implication: Tell your neurologist about temperature sensitivity early — it may guide which tests to order.
Neurologists use a procedure called Quantitative Sensory Testing (QST) to precisely measure thermal detection thresholds — how warm or cold a stimulus needs to be before the patient detects it, and how much heat is needed before pain is triggered. These measurements assess small fiber function more directly than standard nerve conduction studies, which primarily measure large-fiber function.
Warm detection threshold (WDT) and cold detection threshold (CDT) are among the most sensitive early markers of small fiber neuropathy — they can be abnormal before large-fiber nerve conduction testing shows any changes. If you're in the process of diagnosis and experiencing temperature sensitivity issues, mentioning this to your neurologist may prompt appropriate small fiber testing.
Practical Strategies for Managing Temperature Sensitivity

There's no medication specifically for temperature sensitivity in neuropathy, but a range of practical strategies can significantly reduce its impact:
Quick Reference: Temperature Management by Symptom
Cold Sensitivity
Layer up, wool socks, heated insoles, gradual transitions, avoid prolonged cold exposure
Heat Sensitivity
Moisture-wicking socks, pre-cooling, cool water soaks, air conditioning, schedule activity for cooler hours
Temperature Safety
Bath thermometer, no heating pads directly on skin, visual inspection after exposure, oven mitts
For Cold Sensitivity
- Layering: Multiple thin layers trap warmth more effectively than single thick layers and allow adjustment as temperature changes throughout the day.
- Wool and thermal socks: Merino wool maintains warmth even when damp and provides cushioning. Avoid constrictive sock tops that restrict circulation.
- Heated insoles: Battery-operated heated insoles can maintain foot temperature in cold weather. Particularly useful for people who can't rely on sensing when feet are getting too cold.
- Gradual transitions: Rather than going from warm indoors to cold outdoors abruptly, spend time in an intermediate temperature space. Gradual temperature changes give the nervous system less abrupt input to process.
- Avoid extended cold exposure: In extreme cold, plan activities to minimize foot and hand exposure, and check skin color regularly.
For Heat Sensitivity
- Cooling socks and moisture-wicking fabrics: Materials that wick sweat away prevent the buildup of moisture that can trap heat against neuropathic skin.
- Pre-cooling strategies: Before outdoor activity in heat, cool the feet and hands briefly. Some athletes with heat-sensitive neurological conditions use ice vests — the same principle applies.
- Cool water baths: Lukewarm (not cold) water for foot soaks can reduce burning sensations without the shock of cold water on damaged nerves.
- Air conditioning and fans: Maintaining a cooler indoor environment reduces baseline heat load on the nervous system during hot months.
- Time activities appropriately: Exercise and outdoor activity in early morning or evening when temperatures are lower, rather than midday.
For Temperature Safety
- Use a bath thermometer or thermostatic mixing valve to set water temperature before exposure
- Never use heating pads or hot water bottles directly on neuropathic skin without another layer of protection
- Inspect feet and hands visually after any significant temperature exposure
- Use oven mitts and pot holders even for objects that “feel” manageable
- Mention temperature perception problems to all treating physicians, as it affects care planning
Temperature Triggers and Neuropathy Flare-Ups
Temperature is one of the most reliable neuropathy flare triggers for many people — and tracking when your symptoms worsen in relation to temperature changes can be revealing. Some people discover their symptoms are dramatically better in moderate weather and dramatically worse at temperature extremes, which is useful information both for daily planning and for communicating with your medical team about the pattern of your condition.
If you're tracking symptoms, note the ambient temperature and recent temperature changes alongside your pain and symptom scores. Many people find patterns they hadn't previously recognized.
Frequently Asked Questions
Why do my feet burn when it's cold outside?
Cold-induced burning is called cold allodynia or cold dysesthesia. It occurs when damage to small nerve fibers causes the temperature-sensing pathway to misinterpret cold signals as burning heat. The damaged C-fibers and A-delta fibers that normally distinguish hot from cold produce distorted signals that the brain registers as burning. This is not imagined — it is a specific and well-documented consequence of small fiber neuropathy.
Why does hot water feel scalding when it isn't?
Damaged heat-sensing nerve fibers develop lower thresholds for triggering the pain response — a phenomenon called thermal hyperalgesia. Water temperature that would be comfortable for an unaffected person activates pain pathways in damaged neuropathic fibers at much lower temperatures. This is why many people with neuropathy experience what they describe as scalding sensations from lukewarm water.
Is temperature sensitivity a sign of severe neuropathy?
Not necessarily. Temperature sensitivity is often an early sign of small fiber neuropathy specifically, because the fibers responsible for temperature sensation are small fibers that are frequently the first affected. Someone can have significant temperature sensitivity early in the course of neuropathy before large-fiber tests show any abnormality. Severity of temperature sensitivity does not directly correspond to overall severity of neuropathy.
Can I use heating pads safely with neuropathy?
With precautions, yes. Use the lowest effective setting, always place a layer of fabric between the heating pad and skin, set a timer so you cannot fall asleep with it on, and check your skin visually rather than relying on sensation to detect overheating. Electric blankets should be used with similar precautions and turned off before sleep.
Does weather affect neuropathy symptoms?
For most people with peripheral neuropathy, yes. Cold weather increases symptoms for the majority, partly due to slower nerve conduction, vasoconstriction reducing blood flow to nerves, and altered pain signaling in cold. Hot humid weather worsens symptoms for a subset of patients, particularly those with autonomic involvement or heat-sensitive neuropathy types.
Why does my body seem unable to regulate temperature properly with neuropathy?
When autonomic nerve fibers are affected by neuropathy, the systems that control sweating and blood vessel response to temperature can malfunction. This can cause reduced or absent sweating in affected areas, compensatory excessive sweating elsewhere, and impaired blood vessel response to temperature changes. The result is that the body loses some of its ability to maintain stable temperature across different conditions.
How does temperature affect nerve conduction in neuropathy?
Nerve conduction velocity is temperature-dependent — it decreases approximately 2 meters per second for every 1 degree Celsius drop in temperature. In healthy nerves this is a minor effect. In already-compromised neuropathic nerves, this temperature-related slowdown can push marginal function into symptomatic failure, explaining why cold reliably worsens symptoms for most people with neuropathy.


