
Neuropathy vs. Fibromyalgia: How to Tell the Difference
One of the most common questions I hear in my support groups is: “How do I know if this is neuropathy or fibromyalgia?” It is a great question — and one that even doctors sometimes struggle with. Both conditions involve chronic pain, both can cause tingling and burning sensations, and both are frustratingly invisible to the people around you. But they are fundamentally different conditions with different causes, different diagnostic paths, and different treatment approaches.
If you have been dealing with unexplained pain, numbness, or tingling and are not sure which condition — or both — you might be facing, this guide will help you understand the key differences, know what questions to ask your doctor, and navigate the path to an accurate diagnosis.
What Is Peripheral Neuropathy?
Peripheral neuropathy is damage to the peripheral nerves — the vast network of nerves that carry signals between your brain and spinal cord and the rest of your body. When these nerves are physically damaged, they malfunction: sending pain signals when there is no injury, failing to transmit sensations like touch or temperature, or losing the ability to control muscles properly.
An estimated 20 million Americans live with peripheral neuropathy, though the actual number is likely higher since many cases go undiagnosed. The condition has identifiable, measurable nerve damage that can be detected through diagnostic tests like nerve conduction studies and skin biopsies.
Common causes include diabetes (the most common cause), vitamin deficiencies, chemotherapy, excessive alcohol use, autoimmune disorders, infections, and toxic exposures. In some cases, the cause is never identified — what doctors call idiopathic neuropathy.
What Is Fibromyalgia?
Fibromyalgia is a chronic pain condition characterized by widespread musculoskeletal pain, fatigue, sleep disturbances, and cognitive difficulties often called “fibro fog.” Unlike neuropathy, fibromyalgia is not caused by physical damage to the nerves themselves. Instead, it is believed to result from abnormal pain processing in the central nervous system — the brain and spinal cord essentially “turn up the volume” on pain signals.
🔬 Neuropathy
Physical damage to peripheral nerve fibers. The nerves themselves are injured. Can be detected through nerve conduction studies and skin biopsies.
🧠 Fibromyalgia
Abnormal pain processing in the central nervous system. The “volume knob” is turned up. Peripheral nerves are typically intact on testing.
Approximately 4 million American adults have fibromyalgia, with women affected roughly twice as often as men. The condition tends to develop between ages 30 and 50 and is often triggered by physical trauma, surgery, infection, or significant psychological stress — though sometimes it develops gradually with no single identifiable trigger.
Key Differences: Side-by-Side Comparison
Understanding the differences between these conditions is the first step toward getting the right diagnosis and treatment. Here is how they compare across the most important dimensions:
Quick Self-Assessment: Which Pattern Matches?
This is not a diagnostic tool — but it can help you have a more productive conversation with your doctor.
Pain is concentrated in hands and/or feet → more typical of neuropathy
Pain is widespread and moves around day to day → more typical of fibromyalgia
Symptoms are constant (same location, varying intensity) → more typical of neuropathy
Symptoms come and go with flare-ups → more typical of fibromyalgia
Significant fatigue, brain fog, and sleep problems → more typical of fibromyalgia
Numbness + muscle weakness in extremities → more typical of neuropathy
Where the Pain Comes From
Neuropathy: The pain originates from actual physical damage to peripheral nerve fibers. The nerves themselves are injured, and the pain signals they send are a direct result of that damage.
Fibromyalgia: The pain originates from how your brain and spinal cord process pain signals. Think of it as the volume knob being turned up — normal sensory input gets amplified into pain. The peripheral nerves themselves are typically intact and functioning normally.
Pain Location and Pattern
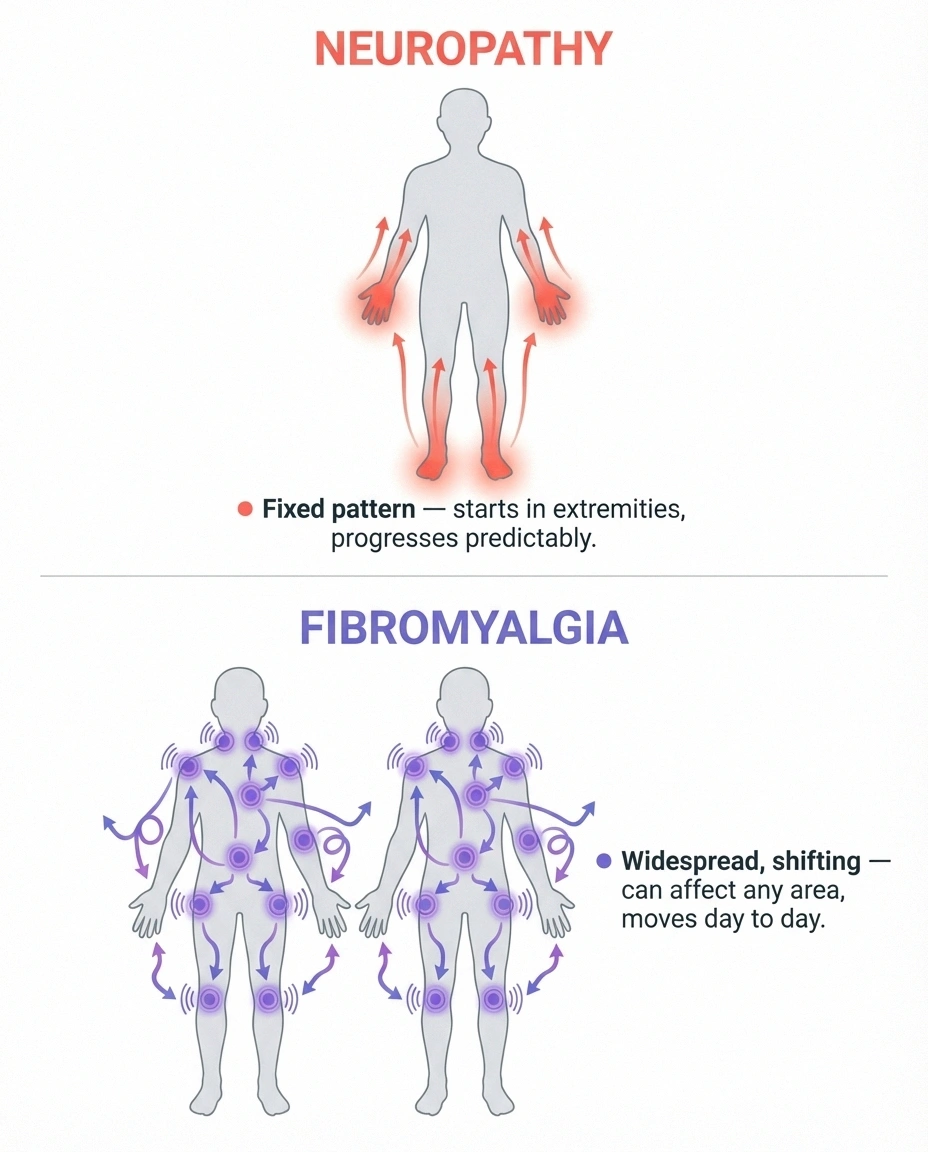
Neuropathy: Pain typically starts in the extremities — feet and hands — and follows a predictable “stocking and glove” distribution. It usually begins in the longest nerves first (the toes and feet) and gradually progresses upward. The pattern is consistent and does not move around day to day.
Fibromyalgia: Pain is widespread and can occur virtually anywhere in the body — muscles, joints, soft tissues. It often migrates: your shoulders might hurt one day, your hips the next. There is no predictable pattern to which body parts are affected on any given day.
Symptom Consistency
Neuropathy: Symptoms are typically constant. You may have good days and bad days in terms of intensity, but the numbness, tingling, or burning in your feet does not disappear and reappear in a different location. Flare-ups increase severity but in the same areas.
Fibromyalgia: Symptoms tend to wax and wane. You might have a terrible week followed by several better days. The pain can migrate between body regions, and flare-ups can be triggered by stress, weather changes, poor sleep, or overexertion.
Associated Symptoms
Neuropathy: The primary symptoms are sensory (tingling, numbness, burning, electric shock sensations) and potentially motor (muscle weakness, difficulty with fine movements). People with neuropathy typically do not experience the fatigue, cognitive problems, or mood disturbances that characterize fibromyalgia — unless those symptoms have a separate cause.
Fibromyalgia: Beyond pain, fibromyalgia includes a constellation of other symptoms: profound fatigue, unrefreshing sleep, “fibro fog” (difficulty concentrating, memory problems), anxiety, depression, irritable bowel syndrome, headaches, and sensitivity to light, sound, or temperature. This broad symptom profile is a distinguishing feature.
How Each Condition Is Diagnosed
This is one of the biggest practical differences between the two conditions — and one that directly affects how quickly you get answers.
Diagnosing Neuropathy
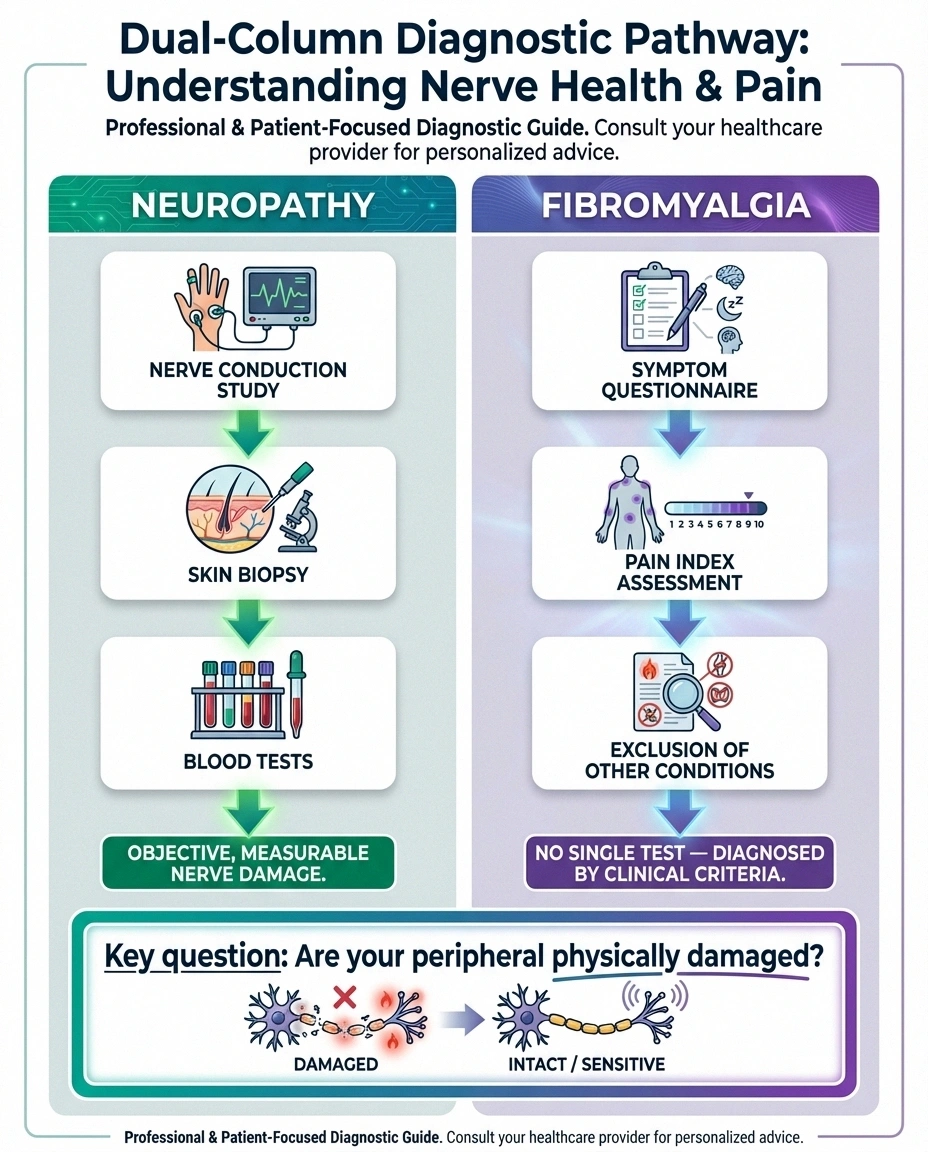
Neuropathy can be objectively measured. Doctors have several tools to detect and quantify nerve damage:
Nerve conduction studies (NCS) and electromyography (EMG) measure how quickly and efficiently your nerves transmit electrical signals and how your muscles respond. Abnormal results confirm peripheral nerve damage.
Skin biopsy examines the density of small nerve fibers in a tiny skin sample. This is particularly useful for diagnosing small fiber neuropathy, which NCS/EMG can sometimes miss.
Blood tests can identify common causes: blood sugar levels, B12 levels, thyroid function, autoimmune markers, and more. The goal is not just to confirm neuropathy but to find its cause.
Diagnosing Fibromyalgia
Fibromyalgia is a diagnosis of exclusion — there is no single lab test or imaging study that confirms it. Doctors use the American College of Rheumatology criteria, which include the widespread pain index and symptom severity scale. Key requirements include: widespread pain in at least 4 of 5 body regions lasting at least 3 months, and no other condition that better explains the symptoms.
Importantly, when nerve biopsies and nerve conduction tests are performed on people with fibromyalgia — even those with tingling and numbness — the results are typically normal. The nerves are physically intact; it is the pain processing system that is malfunctioning.
The Overlap: Small Fiber Neuropathy and Fibromyalgia
Here is where it gets complicated — and where ongoing research is reshaping our understanding of both conditions.
Research Finding
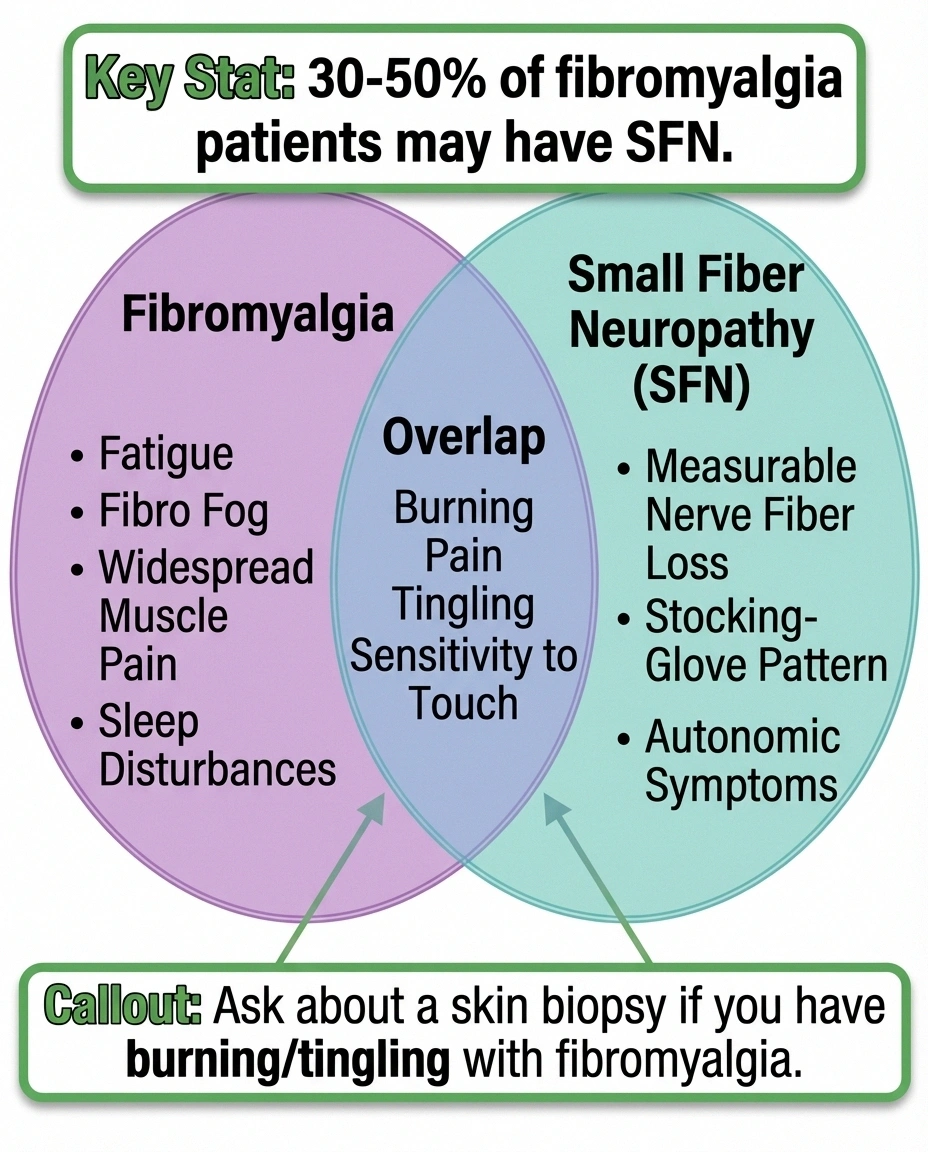
30-50% of people diagnosed with fibromyalgia show evidence of small fiber neuropathy on skin biopsy — a test most fibromyalgia patients never receive. If you have burning, tingling, or numbness with a fibromyalgia diagnosis, ask about skin biopsy testing.
Studies have found that a significant percentage of people diagnosed with fibromyalgia — estimates range from 30% to over 50% — actually have evidence of small fiber neuropathy on skin biopsy. Small fiber neuropathy affects the tiniest nerve endings that transmit pain and temperature sensations. Because these fibers are too small to detect with standard nerve conduction studies, SFN can only be diagnosed through a skin biopsy — a test that many people with fibromyalgia never receive.
This has led researchers to ask a provocative question: how many people diagnosed with fibromyalgia actually have an undiagnosed neuropathic component driving some or all of their symptoms? The answer matters because the treatment approach may be different.
If you have been diagnosed with fibromyalgia and your symptoms include significant burning, tingling, or numbness in your extremities, asking your doctor about a skin biopsy to evaluate for small fiber neuropathy is worth considering. It will not change everything — but it may open additional treatment options.
Can You Have Both Conditions at the Same Time?
Yes, absolutely. Having both neuropathy and fibromyalgia simultaneously — what doctors call comorbidity — is not uncommon. The two conditions are not mutually exclusive, and chronic pain from neuropathy may actually contribute to central sensitization (the mechanism behind fibromyalgia) over time.
Key Takeaway
You can have both neuropathy and fibromyalgia simultaneously. Chronic pain from neuropathy may even contribute to central sensitization over time. If you suspect both, a neurologist (for neuropathy) and rheumatologist (for fibromyalgia) working together provides the most comprehensive care.
Living with both conditions can be especially challenging because the pain comes from two different sources and may require different management strategies. If you suspect you have both, work with a neurologist (for the neuropathy component) and a rheumatologist (for the fibromyalgia component), or ideally a pain specialist familiar with both conditions.
Treatment Approaches: Where They Overlap and Diverge
Some treatments work for both conditions, while others are specific to one or the other.

Medications That Help Both
Three medications are FDA-approved for fibromyalgia that also commonly treat neuropathic pain: pregabalin (Lyrica), duloxetine (Cymbalta), and milnacipran (Savella). These work because they affect pain processing in the central nervous system — which is relevant whether the original pain signal comes from damaged nerves or from central sensitization.
Gabapentin is widely prescribed for both conditions as well, though it is FDA-approved only for neuropathic pain.
Neuropathy-Specific Treatments
Addressing the underlying cause — managing blood sugar, correcting vitamin deficiencies, adjusting medications that cause nerve damage — is unique to neuropathy management. Topical treatments like lidocaine patches and capsaicin cream target damaged nerve endings specifically. Supplements like alpha-lipoic acid and B vitamins address nerve damage pathways.
Fibromyalgia-Specific Treatments
For fibromyalgia, treatments focus more on resetting the central pain processing system: cognitive behavioral therapy, graded exercise programs, sleep hygiene optimization, and stress management. Low-dose naltrexone (LDN) has shown promise specifically for fibromyalgia. Trigger point therapy and myofascial release address the muscle and soft tissue pain that neuropathy treatments do not target.
Lifestyle Approaches That Help Both
Regular gentle exercise — walking, swimming, yoga — benefits both conditions by reducing pain, improving mood, and promoting better sleep. An anti-inflammatory diet supports nerve health and reduces systemic inflammation. Good sleep hygiene is critical for both, since poor sleep amplifies both neuropathic and fibromyalgia pain. Mindfulness and meditation can help with pain management regardless of the underlying condition.
Getting the Right Diagnosis: What to Do Next
If you are unsure whether you are dealing with neuropathy, fibromyalgia, or both, here is a practical path forward:
Your Path to an Accurate Diagnosis
Document Your Symptoms
Track pain location, pattern, consistency, and associated symptoms like fatigue or brain fog in a journal.
Get Blood Work
Request tests for B12, blood sugar, thyroid function, and inflammatory markers to rule out common neuropathy causes.
See a Neurologist
Nerve conduction studies and skin biopsy can objectively detect nerve damage — confirming or ruling out neuropathy.
Ask About SFN Testing
If diagnosed with fibromyalgia but have burning/tingling in extremities, request a skin biopsy for small fiber neuropathy.
Step 1: Document your symptoms carefully. Note where the pain occurs, whether it stays in the same location or moves, what makes it better or worse, and whether you have associated symptoms like fatigue, cognitive difficulties, or sleep problems. A symptoms journal is invaluable.
Step 2: See your primary care doctor and request initial workup including blood tests for common neuropathy causes (B12, blood sugar, thyroid, inflammatory markers).
Step 3: If neuropathy is suspected, ask for a referral to a neurologist for nerve conduction studies and potentially a skin biopsy. If the neurological workup is normal but your symptoms are consistent with fibromyalgia, a rheumatologist can evaluate further.
Step 4: If you have been diagnosed with fibromyalgia but have prominent burning, tingling, or numbness, ask specifically about small fiber neuropathy testing (skin biopsy). This overlap is underdiagnosed.
Getting the right diagnosis matters because it directs you toward the most effective treatments. You deserve answers, not just a prescription to manage symptoms. Browse our understanding neuropathy guides for more resources on diagnosis and management.
Frequently Asked Questions
Can fibromyalgia turn into neuropathy?
Fibromyalgia does not transform into neuropathy because they are different conditions with different mechanisms. However, some research suggests that chronic pain conditions like fibromyalgia may, over time, contribute to changes in nerve sensitivity. Additionally, many people with fibromyalgia may have undiagnosed small fiber neuropathy that existed alongside the fibromyalgia from the beginning.

Why do neuropathy and fibromyalgia symptoms overlap so much?
Both conditions involve abnormal pain signaling, which is why symptoms like burning, tingling, and sensitivity to touch appear in both. In neuropathy, the abnormal signals come from damaged peripheral nerves. In fibromyalgia, the abnormal signals result from the central nervous system amplifying normal input. The end experience for the patient can feel remarkably similar even though the underlying mechanism is different.
Is there a blood test that can distinguish between neuropathy and fibromyalgia?
There is no single blood test that definitively diagnoses either condition. Blood tests can identify causes of neuropathy such as vitamin deficiencies, diabetes, or autoimmune conditions. For fibromyalgia, blood tests primarily serve to rule out other conditions. The key diagnostic tools for neuropathy are nerve conduction studies and skin biopsies. Fibromyalgia is diagnosed based on clinical criteria including symptom patterns and duration.
What percentage of fibromyalgia patients also have small fiber neuropathy?
Research estimates vary, but studies suggest that 30% to over 50% of people diagnosed with fibromyalgia show evidence of small fiber neuropathy on skin biopsy. A 2024 study in PAIN Reports specifically examined the overlap and found that distinguishing the two conditions remains a clinical challenge. This is why some researchers believe that small fiber neuropathy is significantly underdiagnosed in the fibromyalgia population.
Can the same medications treat both conditions?
Yes. Pregabalin, duloxetine, and gabapentin are commonly prescribed for both neuropathic pain and fibromyalgia. These medications work by modifying pain processing in the central nervous system, which is relevant regardless of whether the original pain signal comes from damaged peripheral nerves or from central sensitization. However, neuropathy may also require addressing its underlying cause, which fibromyalgia treatment does not involve.


