
For decades, neuropathy treatment has been a frustrating story of borrowed drugs. Antidepressants borrowed from depression. Anticonvulsants borrowed from epilepsy. Pain relievers borrowed from arthritis and back pain. Every one of them came to neuropathy through the side door — repurposed because nothing was designed specifically for damaged nerves.
That is changing right now. In 2026, the late-stage clinical-trial pipeline is the deepest it has ever been for peripheral neuropathy. There are first-in-class drugs targeting receptors and pathways that nobody had heard of ten years ago. There is gene therapy being injected into the spinal canal. There are pain drugs being engineered to engage opioid receptors WITHOUT the addiction profile. And several of these are weeks or months away from FDA decisions that will reshape what your doctor can offer.
This is the comprehensive 2026 snapshot — every drug in Phase 2b or later trials for neuropathy or neuropathic pain, what stage they're in, what they do, who they're for, and the realistic timeline for if and when they could reach patients. I'm going to be honest about what we know and don't know, because investigational drugs deserve that honesty. Hope without honesty leads to bad decisions, and at this stage of life, our decisions need to be sharp.
Why a 2026 Pipeline Article Right Now?
The reason this snapshot matters in 2026 specifically is that the next eighteen months contain more potential approval decisions for neuropathy drugs than the last ten years combined. Pivotal Phase 3 results are being reported. End-of-Phase-2 meetings with the FDA have already happened for some of these compounds. Gene-therapy first-patient dosing has been announced. Several mechanisms that were only theoretical when I started writing about neuropathy have moved into late-stage testing on humans.
The catch — and this is important to say up front — is that “in clinical trials” is NOT the same as “available to patients.” Late-stage trials succeed at a rate of roughly 50–60% even after the drug has cleared earlier hurdles. Some of the candidates below will work. Some won't. Some will work for one indication but not the one you have. And even the ones that succeed in trials face a years-long path through FDA review and insurance coverage before they reach a corner pharmacy.
So read this like a weather forecast, not a calendar. The shapes are clearer than they've ever been. The exact dates aren't.
How to Read This Pipeline: Phase Definitions in Plain Language
If you've read drug news before, you've seen the phase numbers. Here's the practical translation.
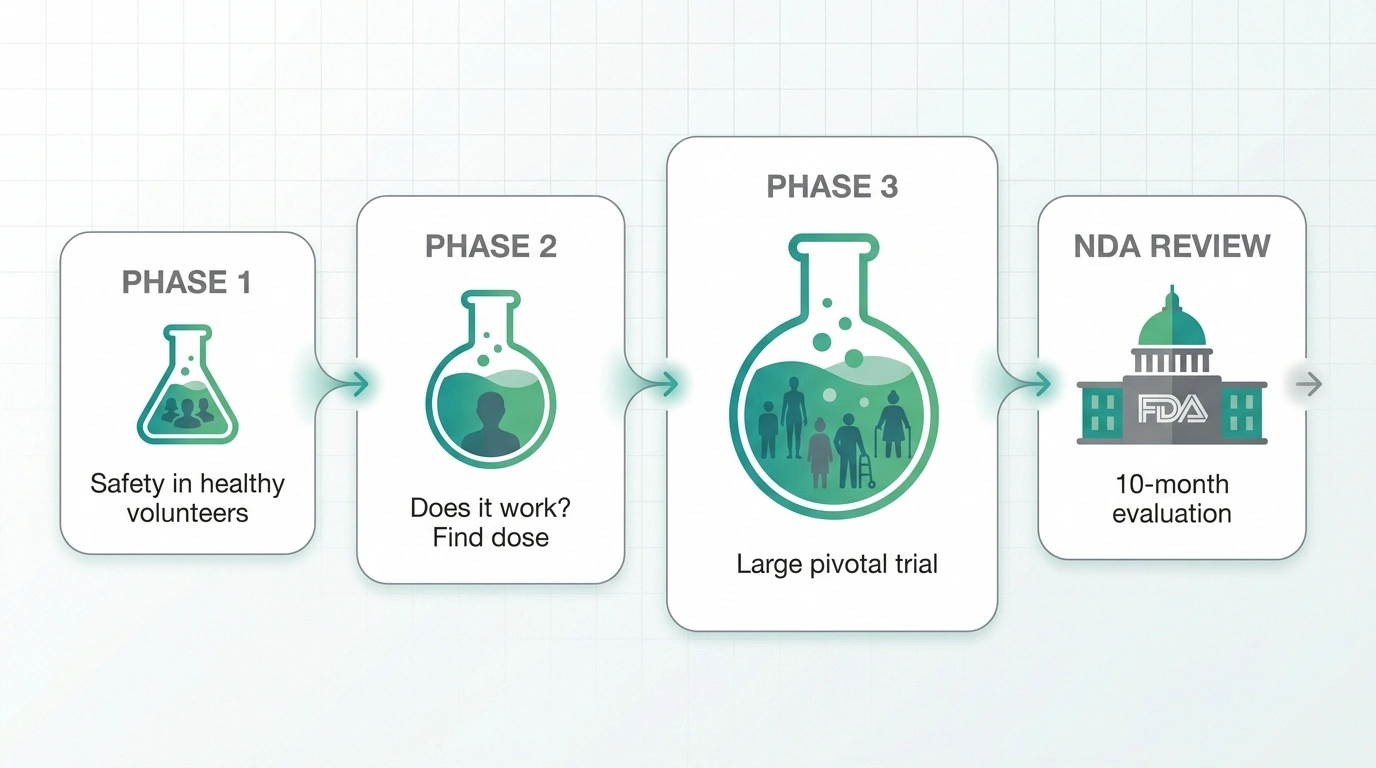
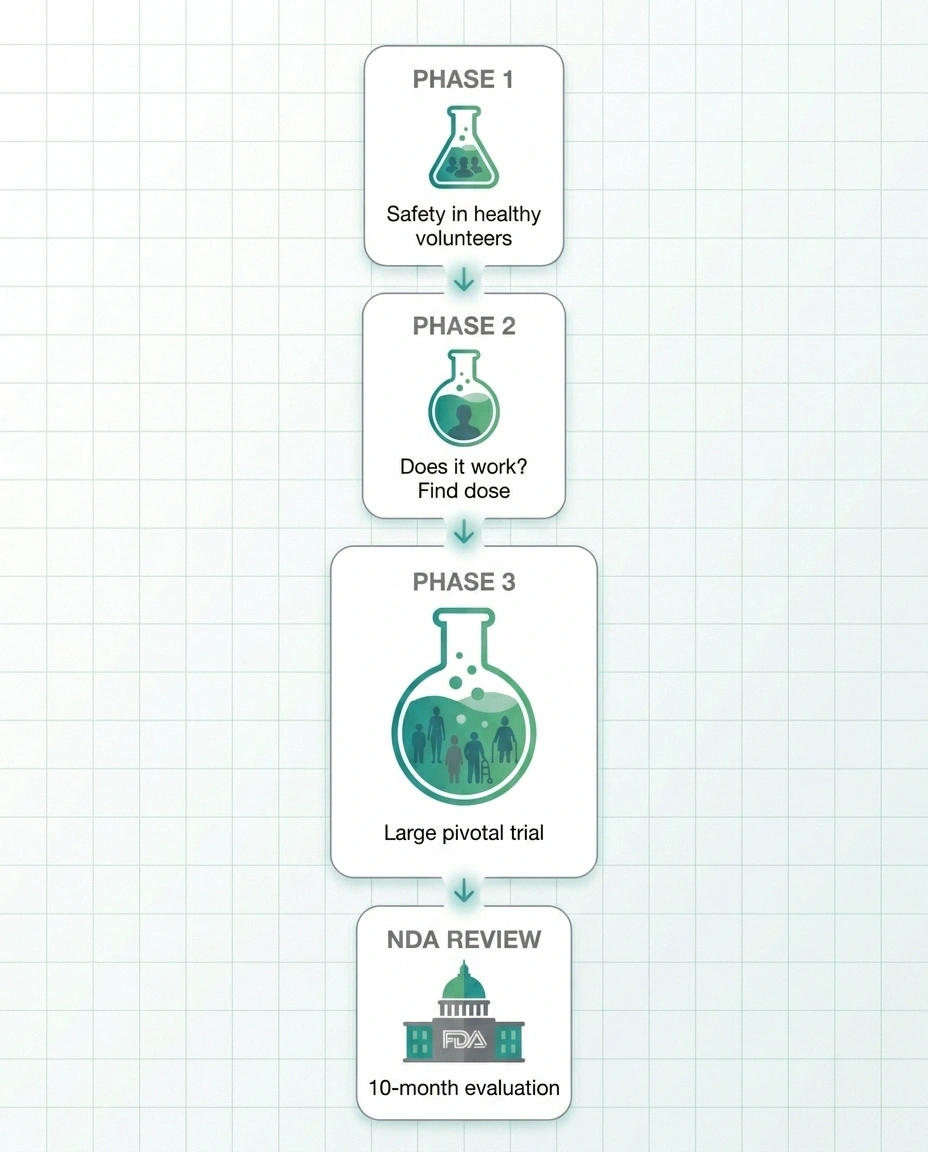
Phase 1 — Small studies in healthy volunteers, mostly checking that the drug is safe at increasing doses. Years away from any patient access. Not in this article.
Phase 2 — Mid-sized studies in actual patients. Does the drug do anything? What's the right dose? Phase 2b is the “find the right dose for the pivotal trial” stage. A successful Phase 2b is the green light for Phase 3.
Phase 3 — Large, multi-center pivotal trials. Hundreds or thousands of patients. These are the studies the FDA uses to decide whether to approve. If both Phase 3 trials succeed, the sponsor submits a New Drug Application (NDA).
NDA review — The FDA evaluation period after a sponsor submits its complete data package. Standard review is 10 months; priority review (granted for serious unmet need) is 6 months. Approval is not guaranteed even with positive Phase 3 results.
For neuropathy drugs in 2026, “late-stage” means Phase 2b through NDA submission. That's the focus below.
The Late-Stage Drug Pipeline at a Glance
The table below summarizes where each candidate sits as of early 2026. I'll go into the details of each one in the sections that follow.
| Drug / Sponsor | Target Indication | Mechanism | Stage |
|---|---|---|---|
| Pilavapadin (LX9211) Lexicon Pharmaceuticals |
Diabetic peripheral neuropathic pain | AAK1 inhibitor (first-in-class) | Phase 3 approved by FDA; trials launching |
| Cebranopadol Tris Pharma |
Acute pain (approved-path); diabetic neuropathy (Phase 2 positive) | Dual NOP / µ-opioid agonist | Phase 3 complete (acute pain); FDA submission in progress |
| VX-993 Vertex Pharmaceuticals |
Painful diabetic neuropathy | Selective Nav1.8 sodium-channel blocker (oral) | Phase 2 ongoing |
| ST-503 Sangamo Therapeutics |
Idiopathic small-fiber neuropathy | AAV gene therapy reducing Nav1.7 in DRG neurons | Phase 1/2 ongoing; first patient dosed |
| SP16 Dogwood Therapeutics |
CIPN prevention | LRP1 agonist peptide | IND accepted; Phase 1b enrolling |
| Mirogabalin Daiichi Sankyo |
Peripheral neuropathic pain; CIPN | Selective α2δ ligand | Approved in Japan/Asia; US trials ongoing |
Pilavapadin (LX9211): The Phase 3 Frontrunner for Diabetic Neuropathy Pain

If I had to pick the single drug most likely to be the next FDA-approved option specifically for diabetic peripheral neuropathic pain, it would be pilavapadin. The Phase 3 program got the green light from the FDA in January 2026 after a successful end-of-Phase-2 meeting.
Pilavapadin works by inhibiting an enzyme called adaptor-associated kinase 1 (AAK1) — a protein involved in nerve-cell signaling. The mechanism is novel; nothing approved today targets AAK1 for any indication. That novelty is both the promise and the question mark. A new target could mean a meaningfully different patient response than the drugs we already use. It also means we have less long-term safety data than for established compounds.
The Phase 2b PROGRESS study enrolled 496 adults with type 1 or type 2 diabetes and moderate-to-severe diabetic peripheral neuropathic pain. The 10-mg dose produced an average daily pain score reduction of 1.74 points from baseline at week 8, versus 1.31 points for placebo. That gap is statistically significant but modest — roughly half a point on a 10-point pain scale. For people in severe pain, even half a point can matter. For others, it might feel like the difference between “this barely helps” and “this changes my life,” depending on the person.
Phase 3 is two 12-week placebo-controlled trials at the 10-mg dose. Both trials must show statistically significant improvement in average daily pain score at week 12 for the FDA to approve. Realistic earliest approval: late 2027 or 2028, assuming both trials succeed and the NDA review moves smoothly.
Cebranopadol: The Dual-Receptor Drug That's Trying to Untangle Pain Relief From Addiction
Cebranopadol is the one that has the pain-medicine world watching most closely, because it's attempting something genuinely hard: keeping the powerful pain relief that comes from engaging opioid receptors while side-stepping the abuse liability and respiratory-depression risk that has made opioids a public-health disaster.
It works by simultaneously activating two receptors: the µ-opioid receptor (MOP) — the same one engaged by morphine and oxycodone — AND the nociceptin/orphanin FQ peptide receptor (NOP). The NOP activation, in the theory and the preclinical data, dampens the parts of the µ-opioid response that drive reward and dependence while preserving the analgesia.
The Phase 3 program is for acute, post-surgical pain — not neuropathy. ALLEVIATE-1 (post-abdominoplasty surgery) and ALLEVIATE-2 (post-bunionectomy surgery) both met their primary pain-reduction endpoints, with ALLEVIATE-2 showing greater pain relief than oxycodone IR 10 mg in a post-hoc analysis. Tris Pharma is preparing an FDA submission for acute pain.
For our purposes, the more important data point is that cebranopadol completed earlier Phase 2 trials in diabetic neuropathic pain with positive efficacy signals. Over the entire development program, more than 32 trials and 2,200 participants, the drug has shown activity in acute pain, chronic pain, and diabetic neuropathic pain.
The realistic neuropathy path:
- If acute-pain approval lands in 2026 or 2027, doctors may have legal access to it for off-label use in chronic neuropathy. Off-label use is widespread for nerve pain — gabapentin, duloxetine, and amitriptyline are all used off-label or on-label for various neuropathic conditions.
- A dedicated neuropathy indication would require a separate Phase 3 program, almost certainly not finishing before 2028-2029.
- Whether insurance will cover off-label use of a brand-new drug is unpredictable.
Read the full background in our deeper guide on cebranopadol for nerve pain.
VX-993: The Next-Generation Sodium-Channel Blocker
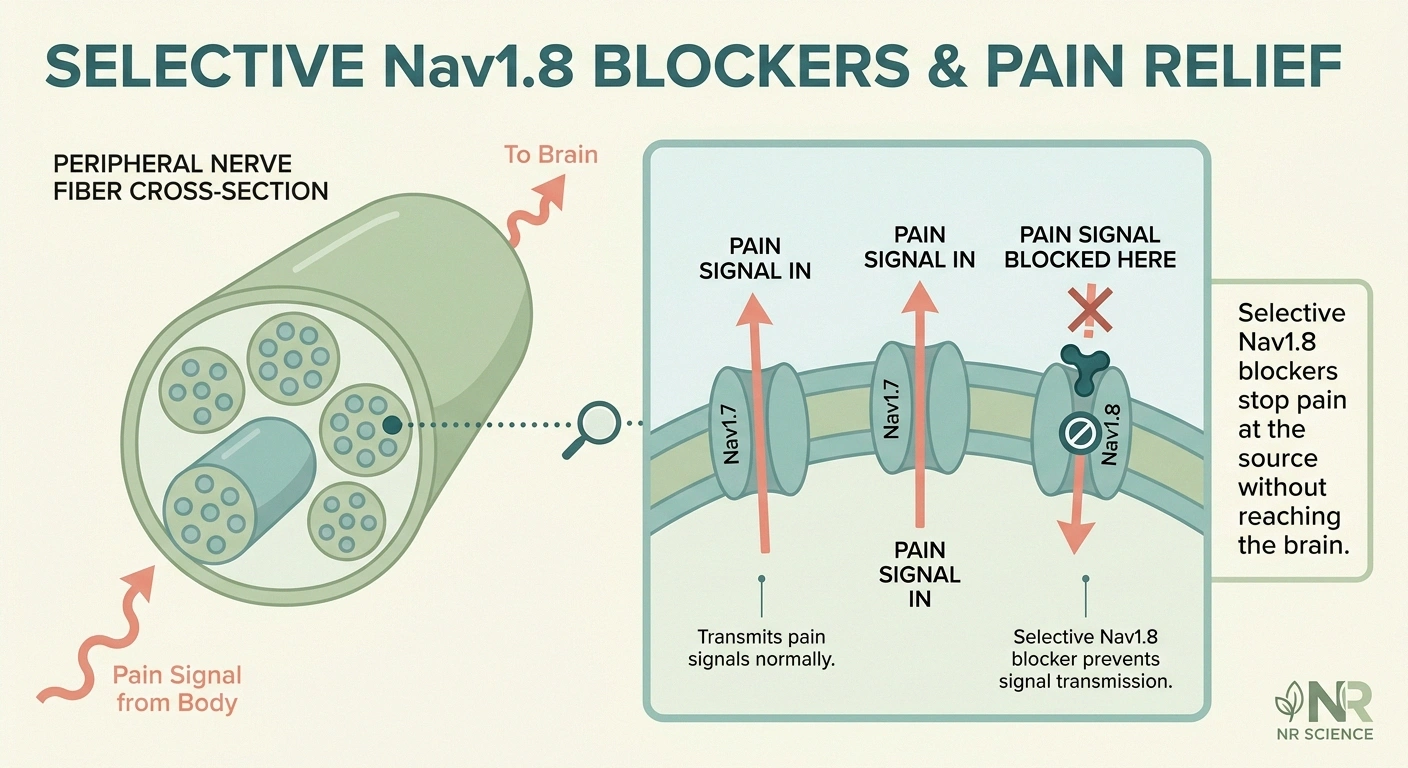
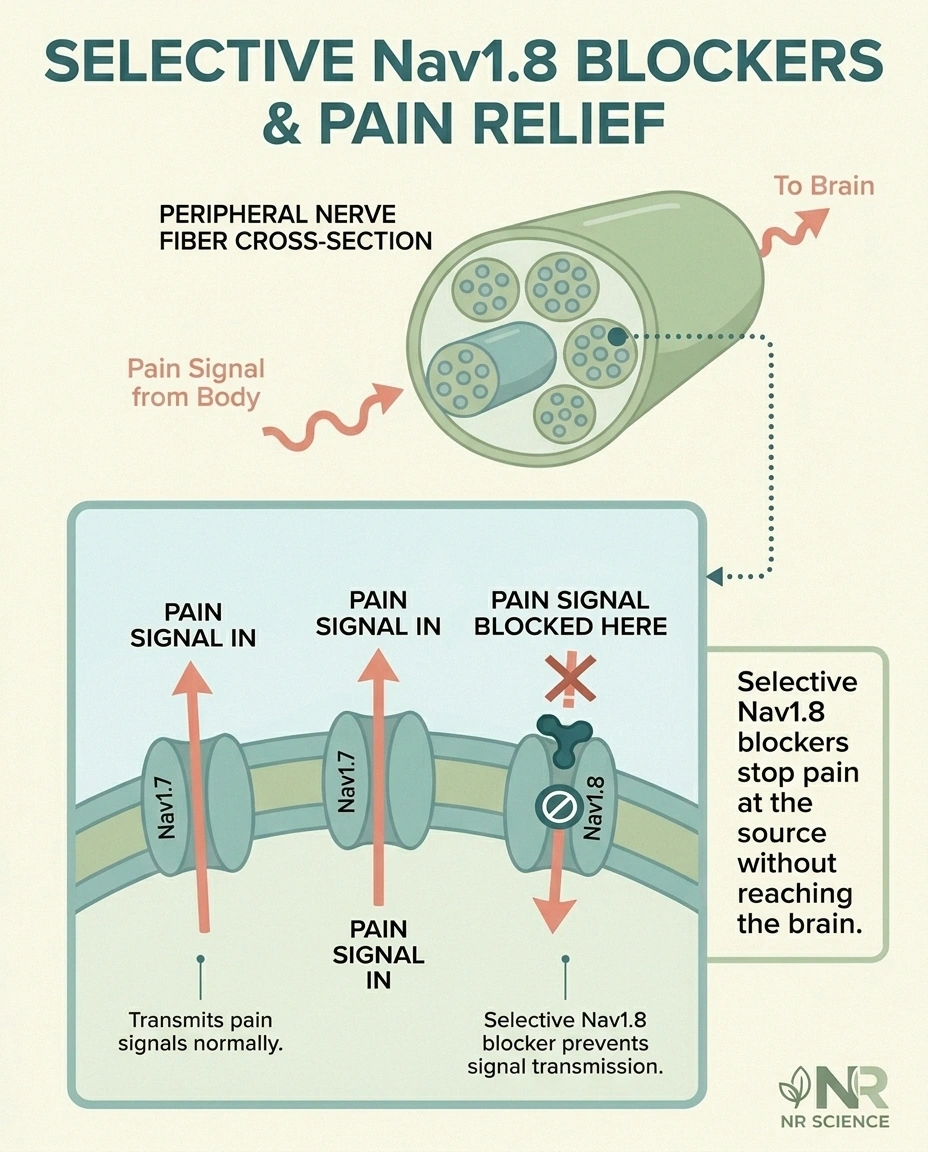
VX-993 is Vertex Pharmaceuticals' follow-up to suzetrigine (Journavx) — the Nav1.8 sodium-channel blocker the FDA approved in early 2025 for acute pain. Both drugs target a specific sodium channel found primarily in pain-signaling sensory neurons, which means they should provide pain relief WITHOUT the central nervous system effects of opioids or gabapentinoids (no sedation, no euphoria, no dependence).
VX-993 is being studied specifically in painful diabetic peripheral neuropathy (PDN), which would be the first time a Nav1.8 blocker is tested as a chronic neuropathy treatment rather than for acute pain. Phase 2 is ongoing. If results are positive, Phase 3 could begin in 2026 or 2027, with potential approval not before 2028.
The mechanism is one of the most important to understand because it changes what a “pain medication” can look like. Selective sodium-channel blockers don't reach the brain in a way that produces opioid-like effects, which means they can't be abused in the same way and don't cause cognitive side effects. If a chronic-pain Nav1.8 blocker proves out in diabetic neuropathy, it could change first-line treatment.
For more detail on this candidate specifically, see our VX-993 article.
ST-503: The Gene Therapy for Small-Fiber Neuropathy

ST-503 is the most futuristic-sounding entry in the pipeline, because it actually is a gene therapy. Sangamo Therapeutics developed an AAV (adeno-associated virus) vector that delivers a zinc-finger transcription factor designed to REDUCE expression of the Nav1.7 sodium channel in the dorsal root ganglia — the cluster of sensory nerve cell bodies just outside the spinal cord.
The science behind this is elegant. People born with naturally low Nav1.7 function have congenital insensitivity to pain — they don't feel pain normally. By turning down Nav1.7 in the DRG (not throughout the body), the therapy aims to dial down the pain-signal volume in patients with idiopathic small-fiber neuropathy without producing a complete sensation blackout.
Delivery is a single intrathecal injection — meaning into the spinal canal — at a specialized center. One treatment. The first patient was dosed in 2025; the Phase 1/2 trial is ongoing.
Realistic timeline: gene therapy programs typically run 8-10 years from first dose to commercial availability. ST-503 is at the very beginning of that arc. But if it works, it would represent a treatment paradigm — a single procedure providing durable relief — that no neuropathy drug today offers.
Full background on this candidate in our ST-503 gene therapy article.
SP16: The First Drug Aiming to PREVENT Chemo-Induced Neuropathy
SP16 from Dogwood Therapeutics is conceptually different from the other entries on this list. Every other drug here is trying to TREAT neuropathy that already exists. SP16 is trying to PREVENT chemotherapy-induced peripheral neuropathy (CIPN) before it starts.
CIPN affects 30-40% of patients receiving common chemotherapy regimens like taxanes (paclitaxel) and platinum drugs (oxaliplatin, cisplatin). For some patients it resolves after treatment ends. For many it doesn't — and there is currently no FDA-approved drug that prevents it from happening.
SP16 is a peptide that activates the LRP1 receptor, which is involved in nerve-cell protection and inflammation regulation. The hypothesis is that delivering SP16 alongside chemotherapy will protect peripheral sensory nerves from the toxic effects of the cancer drugs.
The FDA accepted the IND (Investigational New Drug application) in April 2026, and Phase 1b patient enrollment is underway. Realistic timeline is long — likely 6-9 years to approval — but if it succeeds, it changes the calculus for every cancer patient facing taxane or platinum chemotherapy.
Full details in our SP16 CIPN prevention article.
Mirogabalin: Already Approved Outside the US
Mirogabalin (sold as Tarlige in Japan) is a special case because it's already approved and used by patients — just not in the United States. Daiichi Sankyo developed it as a more selective version of pregabalin (Lyrica). It binds the α2δ-1 subunit of voltage-gated calcium channels with higher affinity than pregabalin and theoretically with fewer α2δ-2-related side effects (which is where some of the dizziness and sedation come from).
In Japan and several Asian markets, mirogabalin has been approved for peripheral neuropathic pain since 2019. Real-world data have generally supported the trial findings — comparable analgesic effect to pregabalin with potentially lower rates of certain side effects.
The U.S. path is more uncertain. Daiichi Sankyo has run Phase 3 trials in CIPN in the U.S., but a full U.S. neuropathy approval has not yet happened. Whether the company files a U.S. NDA for chronic neuropathic pain in the next two years remains to be seen.
For patients who have tried pregabalin and found the side-effect profile difficult, mirogabalin would be a meaningful addition to the U.S. toolbox if it arrives.
How to Find and Join a Neuropathy Clinical Trial
Several of the drugs above are actively enrolling. If you're considering it — and your doctor agrees it could be a fit — here's how to actually find one.
Start at ClinicalTrials.gov. This is the U.S. government registry of clinical trials. The search box accepts the condition name (“diabetic peripheral neuropathy” or “chemotherapy-induced peripheral neuropathy”) and the drug name (pilavapadin, cebranopadol, VX-993, etc.). Filter by “Recruiting” status and your geographic area.
Read the eligibility criteria carefully. Most trials have strict inclusion/exclusion criteria — specific pain scores, specific neuropathy duration, specific blood-test parameters, specific medications you can or can't be taking. Most patients who think they qualify don't actually meet every criterion.
Talk to your neurologist or primary care provider before contacting a site. Some criteria require physician documentation (e.g., nerve conduction study results, dates of diagnosis). Having those records in hand speeds everything up.
Understand what “investigational” means for your care. If you enroll in a Phase 3 placebo-controlled trial, there's a meaningful chance you'll be on placebo for the trial duration. You'll need to think through what that means for your symptom management.
Our guide to finding and joining neuropathy clinical trials covers the practical mechanics in more detail.
What Approval Would Actually Mean for Patients

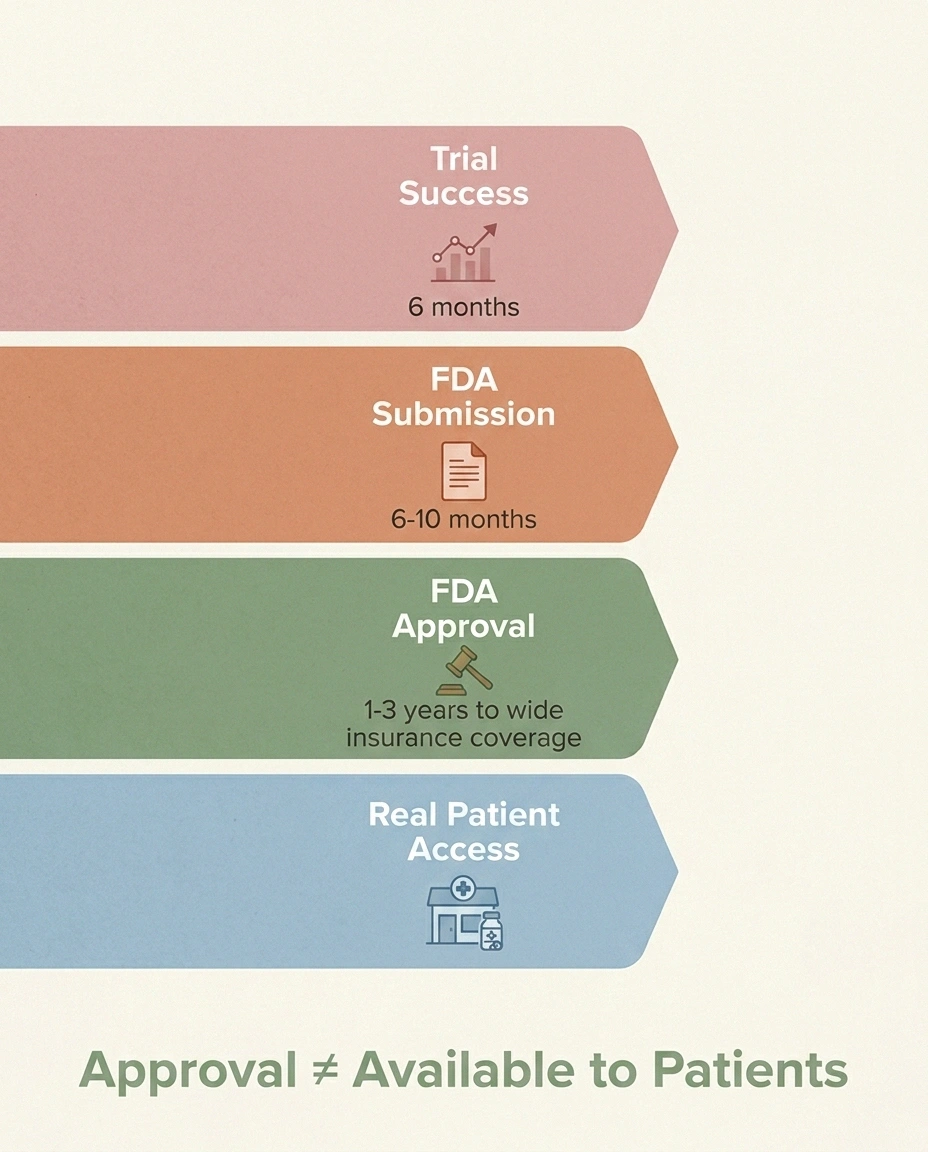
An FDA approval is not the moment a drug reaches your medicine cabinet. There are three layers between approval and access.
Layer 1 — pharmacy availability. Most new drugs reach major pharmacy chains within weeks of approval, though specialty drugs (especially gene therapies and biologics) may only be available at specific specialty pharmacies or treatment centers.
Layer 2 — insurance coverage. A new branded drug may be added to a formulary as preferred, non-preferred, or excluded — or it may require prior authorization (your doctor has to submit paperwork justifying it). Initial coverage for new neuropathy drugs is often restrictive. Generic alternatives stay first-line until prior authorization clears.
Layer 3 — clinical adoption. Even after approval, physician comfort with prescribing a brand-new drug takes time to build. Your community neurologist may not write the first script. Academic centers and pain specialists tend to lead.
The practical implication: if pilavapadin or cebranopadol or VX-993 gets approved in 2027, “real” patient availability for most people is more likely 2028-2030. Not the day after the press release. Plan around the realistic timeline, not the optimistic one.
Tracking the Pipeline Yourself
If you want to follow updates between now and approval (or between trial readouts), these are the most reliable sources:
- ClinicalTrials.gov — every U.S.-registered trial, including status updates and result postings.
- FDA Drug Approvals page (accessdata.fda.gov) — official approval announcements.
- Each sponsor's investor relations page — Lexicon, Tris Pharma, Vertex, Sangamo, Dogwood. They post trial-result press releases here first.
- NeurologyLive and Patient Care Online — regular industry coverage of neurology drug approvals.
- This site — we publish drug-specific deep dives as data emerges. The articles linked above are kept current.
The Bigger Picture
What's encouraging about the 2026 pipeline isn't any single drug — it's the diversity. AAK1 inhibitors and dual-receptor opioid alternatives and selective sodium-channel blockers and gene therapy and prevention strategies. These are very different mechanisms aimed at very different problems. The chance that one of them produces a clinically meaningful new option in the next few years is much higher than the chance any single drug succeeds.
- ✓ Read every eligibility criterion — most patients miss at least one
- ✓ Get your medical records (EMG, nerve-conduction, diagnosis dates) ready
- ✓ Discuss with your neurologist BEFORE contacting a trial site
- ✓ Understand the placebo arm — you may not get the drug
For patients living with neuropathy today, the practical move is to keep doing the things that already work for you — the diet adjustments, the supplements your doctor approved, the exercise routine, the current medication regimen — while keeping a watchful eye on the readouts that are coming. The treatment landscape will probably look different in three years than it does today. That's not a guarantee of relief, but it's a real reason for measured optimism.
Frequently Asked Questions
Are any of these drugs available now?
None of the drugs in this article are FDA-approved for neuropathy as of 2026. Mirogabalin is approved in Japan and several Asian markets but not the United States. Suzetrigine (Journavx, a related Nav1.8 blocker) is approved for acute pain but not for chronic neuropathy.
Can my doctor prescribe one of these off-label?
For drugs that are not FDA-approved at all, no — those are only available through clinical trial enrollment. For a drug like cebranopadol if it gets approved for acute pain, off-label use for chronic neuropathy would be at the doctor's discretion, subject to insurance and clinical judgment. Off-label use is common in neuropathy treatment but isn't guaranteed.
Which one is most likely to actually reach patients first?
Cebranopadol for acute pain is closest, with an FDA submission planned following the positive ALLEVIATE Phase 3 results. For diabetic neuropathy specifically, pilavapadin is the next major milestone — but its Phase 3 program is just starting, so a realistic earliest approval is 2027-2028.
What's the difference between these drugs and gabapentin or pregabalin?
Gabapentin and pregabalin work by binding the α2δ-1 subunit of voltage-gated calcium channels, dampening nerve signaling broadly. The drugs in this pipeline use different mechanisms entirely — sodium-channel blockade (VX-993), dual opioid-receptor engagement (cebranopadol), AAK1 inhibition (pilavapadin), Nav1.7 gene silencing (ST-503), or LRP1 activation for prevention (SP16). Different mechanisms mean potentially different efficacy and side-effect profiles.
How do I join a clinical trial?
Search ClinicalTrials.gov by drug name or condition, find a trial that's actively recruiting in your area, review the eligibility criteria carefully, then contact the trial site directly or talk with your neurologist about a referral. See the trials-guide article linked above for the practical mechanics.
Is gene therapy for neuropathy really happening?
Yes — ST-503 (Sangamo) has dosed its first patient in a Phase 1/2 trial for idiopathic small-fiber neuropathy as of 2025. The trial is ongoing. Gene therapy is at the earliest stage of any drug in this article — even if it works as hoped, the commercial-availability timeline is likely the longest, in the 8-10 year range from first dose.
Will insurance cover any of these when they're approved?
That depends on the drug, the insurer, the formulary placement, and the specific indication approved. New branded drugs for neuropathy typically require prior authorization initially and may be designated as second-line behind older generics. Plan to budget for prior-authorization paperwork and possible appeals.
Why is the pipeline so much deeper now than five years ago?
Three factors have converged: better understanding of the molecular biology of pain (Nav1.7, Nav1.8, LRP1, AAK1 are all relatively recent targets), the opioid crisis driving urgent investment in non-opioid alternatives, and large pharmaceutical companies seeing diabetic and chemo-induced neuropathy as commercially significant unmet need with growing patient populations.
Should I wait for one of these drugs before trying current options?
No. The realistic timeline for most candidates here is 2028 at earliest, and waiting on the chance that a specific drug works for you is not a good treatment plan. Work with your current care team on what's available now — and stay informed about what's coming.


