If you have spent any time researching neuropathy, you already know the problem: there are dozens of treatments, everyone online swears by a different one, and almost nobody tells you which ones actually have evidence behind them versus which ones are mostly hope and marketing. I have been down that rabbit hole myself, late at night, with numb feet and a browser full of tabs. So I built the page I wish I'd had back then.
This is a plain-English comparison of essentially every mainstream neuropathy treatment, sorted not by how loudly it's advertised but by how strong the evidence is, balanced against how risky, expensive, and demanding it is for a real person. Think of it as a map. It won't tell you exactly which treatment is right for you — only you and your doctor can decide that — but it will tell you where the solid ground is and where the quicksand is.
Start Here: What “Treatment” Actually Means With Neuropathy
The first thing I had to unlearn is that “treating neuropathy” is really three different jobs, and most products blur them together on purpose. Job one is treating the underlying cause so the nerve stops being damaged. Job two is relieving the symptoms — the burning, tingling, and pain — while the rest plays out. Job three is protecting function and quality of life so the condition takes as little from your daily life as possible.
Almost every disappointment I see in my support group comes from expecting a job-two treatment (a pill or a cream that quiets the pain) to do a job-one task (actually repairing the nerve). They're not the same thing, and a treatment that's excellent at one can be useless at another. As you go through this guide, keep asking: which job is this option for? That single question cuts through most of the noise.
The Single Most Important Treatment Is Treating the Cause
Here is the most important sentence in this entire article: the treatment with the strongest evidence is almost never a product. It is finding and fixing whatever is damaging your nerves in the first place. For the most common form, diabetic neuropathy, tight blood-sugar control is the single best-supported intervention for slowing or stopping progression — no supplement comes close. If the cause is a vitamin B12 deficiency, replacing B12 is the actual treatment. If it's alcohol, thyroid disease, a medication, or another driver, addressing that is the lever that matters most.
The strongest-evidence treatment is almost never a product
It is finding and fixing whatever is damaging your nerves — blood sugar, B12, alcohol, an offending drug. Everything else in this guide works better, or only works at all, when the underlying fire is being put out at the same time.
This is why the very first step is a real diagnostic workup, not a shopping spree. If you don't yet know your cause, that is the highest-value thing you can pursue — our guide to neuropathy diagnosis and the tests your doctor may order walks through it. Everything else in this comparison works better, or only works at all, when the underlying fire is being put out at the same time. A treatment that addresses the cause can sometimes allow real improvement; you can read more about what's realistic in can neuropathy be reversed.
How We Ranked These Options

I want to be transparent about the yardstick, because “ranked by evidence” can be misleading if evidence is the only axis. A treatment can have strong clinical-trial evidence and still be a poor first choice for a specific person if it's risky, expensive, or grueling. So I weighed four things together:
A treatment can have strong trial data and still be a poor first choice if it is risky, expensive, or grueling. For a real person, risk and access are not footnotes — they are the whole point. That is why a cheap, safe option with moderate evidence often outranks an invasive one with slightly stronger numbers.
Evidence quality — what well-designed studies and treatment guidelines actually show, not testimonials. Risk and side effects — how much it can harm you, and how reversible that harm is. Cost and access — whether an ordinary person can realistically obtain and afford it. Effort and burden — how much of your life it demands. A cheap, safe option with moderate evidence often beats an expensive, invasive one with slightly stronger trial data, because for a real human, risk and access are not footnotes — they're the whole point. The tiers below reflect that combined judgment.
The Master Comparison Table
Here is the whole landscape in one place. “Evidence” reflects clinical-trial and guideline support; “Best for” notes the job it actually does. This table is a starting point for a conversation with your clinician, not a substitute for one.
| Treatment | Evidence | Risk | Best for |
|---|---|---|---|
| Treating the cause (blood sugar, B12, alcohol, offending drug) | Strongest | Low | Stopping the damage |
| Exercise / movement | Low–moderate | Very low | Function, circulation, mood |
| Physical / occupational therapy | Moderate (function) | Very low | Balance, falls, daily life |
| Gabapentin / pregabalin | Strong (pain) | Moderate | First-line pain relief |
| Duloxetine / venlafaxine (SNRI) | Strong (pain) | Moderate | First-line pain relief |
| Amitriptyline / nortriptyline (TCA) | Strong (pain) | Moderate | First-line pain relief |
| High-concentration capsaicin patch | Moderate (focal) | Low | Localized pain |
| CBT / mindfulness | Moderate (coping) | Very low | Pain coping, mood |
| TENS unit | Modest | Very low | Cheap symptom add-on |
| Acupuncture | Mixed / promising | Low | Adjunct pain relief |
| Alpha-lipoic acid | Mixed | Low | Optional supplement |
| Tramadol / combination therapy | Moderate | Moderate–high | Second-line pain relief |
| Spinal cord stimulation | Strong (selected) | High (surgical) | Severe, refractory cases |
| Strong opioids | Limited | High | Last resort only |
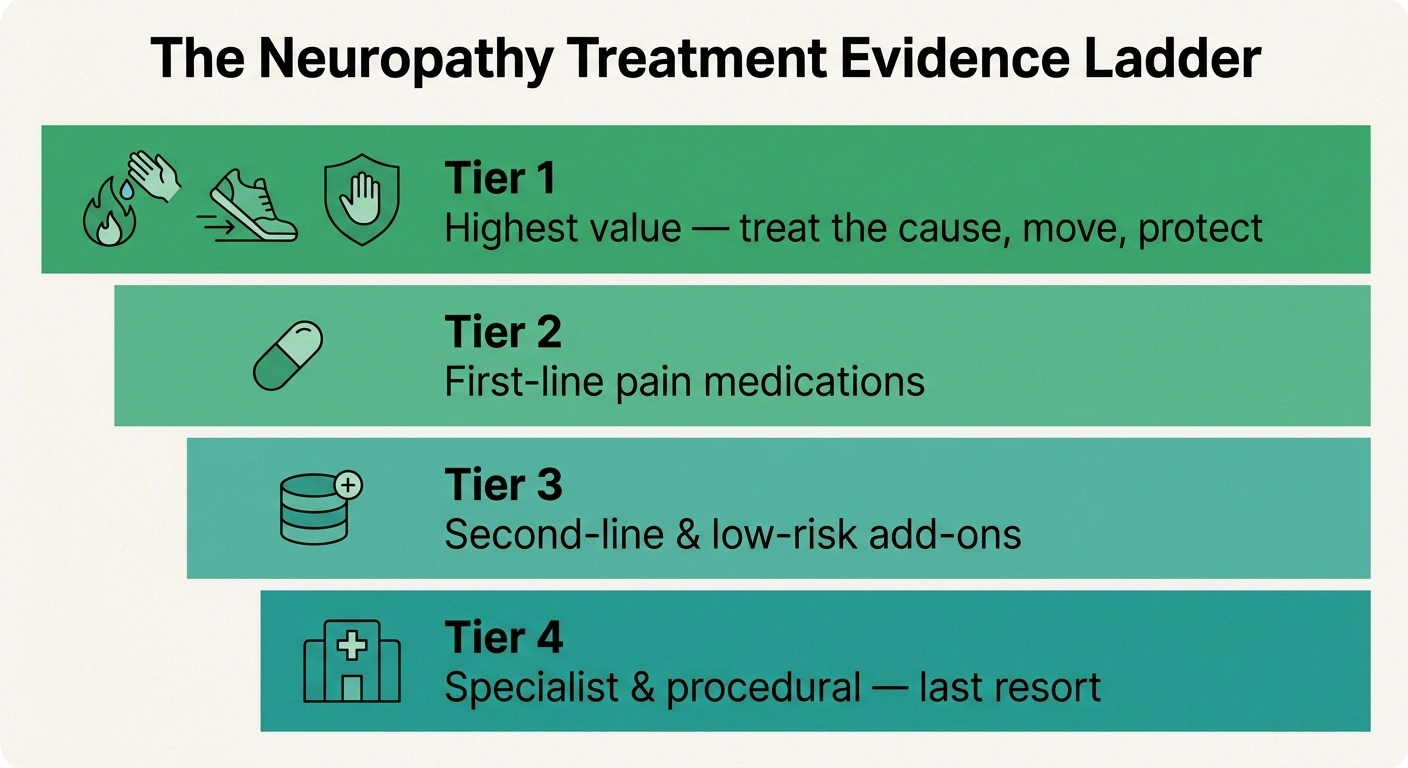
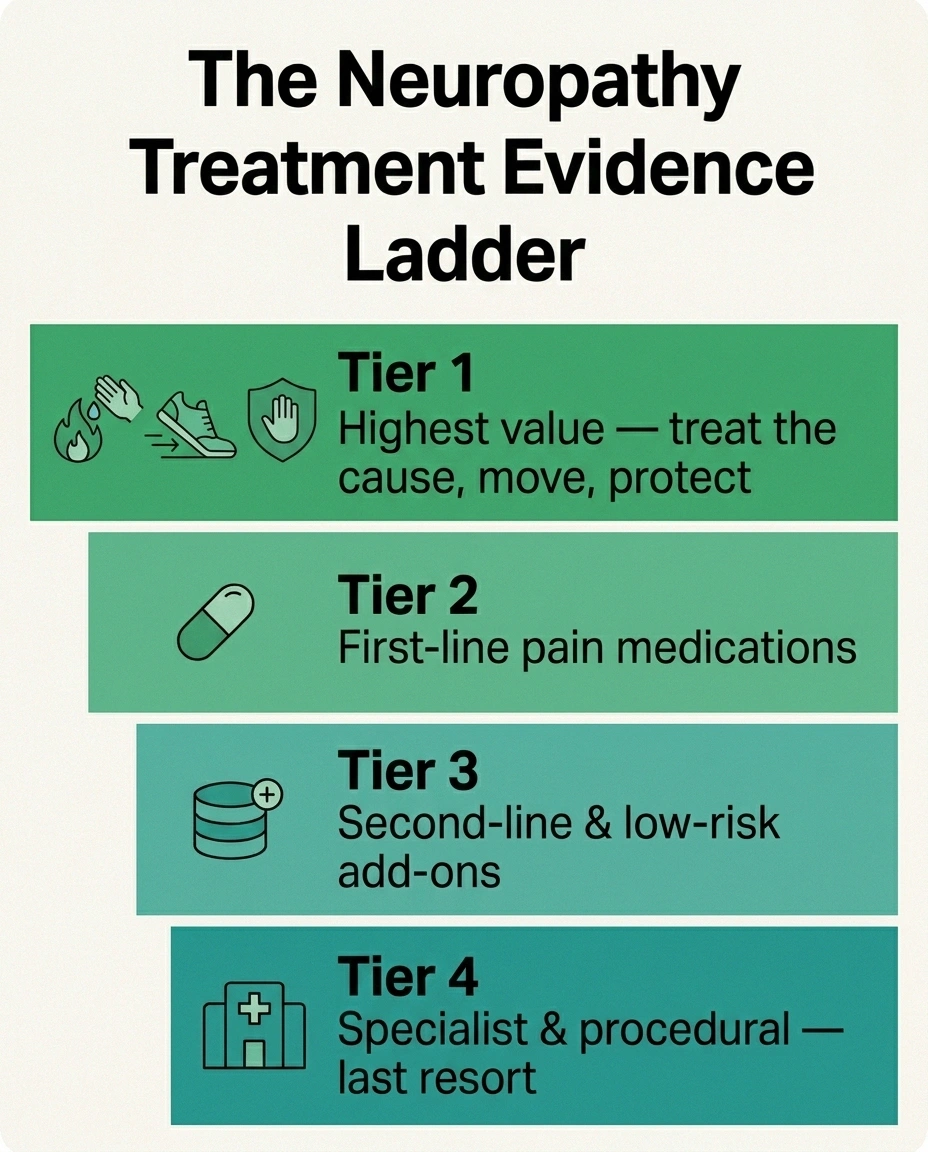
Tier 1 — Highest Value: Treat the Cause, Move, and Protect

If I could give one piece of advice to my younger, newly diagnosed self, it would be: spend your first energy here, not on a supplement aisle. Tier 1 is the cluster of options where evidence, safety, cost, and real-life payoff all line up. Treating the underlying cause leads it, as we covered. Right behind it is movement. Regular, gentle exercise has low-to-moderate evidence but an outstanding safety and cost profile, and it improves circulation, balance, mood, and sleep all at once — our guide on whether walking helps neuropathy is a good starting point, and the full structured recovery plan ties the lifestyle pieces together.
The third leg is structured rehabilitation. Physical and occupational therapy won't “cure” the nerve, but they have solid evidence for what arguably matters most day to day — balance, fall prevention, and keeping your independence. You can see how that works in our overview of physical therapy for neuropathy. None of Tier 1 is glamorous. All of it is where the real return is.
Tier 2 — First-Line Medications
When pain itself is the problem, this is where the strongest symptom evidence lives. Major treatment guidelines converge on four core drugs as first-line for neuropathic pain: the gabapentinoids gabapentin and pregabalin (Lyrica); the SNRI antidepressant duloxetine (Cymbalta); and the tricyclic antidepressant amitriptyline. A large head-to-head trial found these have roughly equivalent average efficacy, and that combining two of them helps many people who don't respond to one alone.
The Four First-Line Pain Drugs
Gabapentin — a gabapentinoid, very widely used first choice.
Pregabalin (Lyrica) — the other gabapentinoid.
Duloxetine (Cymbalta) — an SNRI antidepressant.
Amitriptyline or nortriptyline — a tricyclic. Roughly equal average efficacy; combining two helps partial responders.
Two honest caveats. First, “first-line and strong evidence” does not mean “works for everyone” — in trials, a minority to roughly half of people get meaningful relief from any single one, which is exactly why doctors rotate and combine them. Second, these are not nerve-repair drugs; they quiet the pain signal. They carry real side effects (drowsiness, dizziness, weight changes, and for some, dependence concerns), so they're a genuine risk-benefit decision, not a default. The takeaway: if pain is dominating your life, the best-evidenced relief is a conversation with your doctor about these four, not the next supplement ad.
Tier 3 — Second-Line and Add-On Options

When first-line drugs alone aren't enough, several options have moderate evidence and a place as add-ons or alternatives. The high-concentration capsaicin patch is well supported for localized neuropathic pain — a focused tool, not a whole-body answer. Tramadol and formal combination therapy (an antidepressant plus a gabapentinoid) are recognized second-line choices, though tramadol carries more dependence and interaction risk than its mild reputation suggests.
One add-on I wish more people took seriously is the mind-body track. Cognitive behavioral therapy and mindfulness have moderate evidence as second-line, in conjunction with other treatment — not because the pain is “in your head,” but because chronic pain genuinely rewires how the nervous system amplifies signals, and these approaches measurably turn that volume down. They are among the lowest-risk things on this entire page. There is no contradiction in using a first-line drug and a coping skill; the strongest plans usually stack a Tier 1 foundation, a Tier 2 medication, and a Tier 3 add-on.
Tier 4 — Specialist and Procedural Options

These are the high-intensity tools, reserved for severe, refractory pain that hasn't responded to the tiers above. Spinal cord stimulation has genuinely strong evidence in carefully selected patients — it's now cleared for painful diabetic neuropathy — but it is a surgical implant with surgical risks, real cost, and a screening trial first. Repetitive transcranial magnetic stimulation of the motor cortex is a recognized third-line option in specialized centers. Botulinum toxin injections can help focal neuropathic pain in expert hands.
And then there are strong opioids. I'll be blunt because the people I've watched struggle deserve bluntness: the evidence for long-term opioids in neuropathic pain is limited, the risks are high, and every serious guideline now lists them as a last resort when nothing else is available. They are not a Tier 1 shortcut you've been unfairly denied; they're a high-risk option of last resort, and that ranking reflects the evidence, not gatekeeping.
Supplements: What the Evidence Actually Supports
This is the category with the widest gap between marketing and data, so let's be careful and fair. Alpha-lipoic acid is the most-studied supplement; the evidence is genuinely mixed — some trials show benefit, others show none, with intravenous forms more consistent than oral. It's reasonably safe, so it's a defensible optional add-on, not a cornerstone. B vitamins are a true treatment only when you actually have a deficiency — vital then, unremarkable otherwise. Acetyl-L-carnitine, CBD, and others remain “needs more study.”
My honest framing: a supplement with mixed evidence and low risk can be a reasonable experiment after the higher tiers are in place — never instead of them, and never the thing you spend your hope and budget on first. Our supplements-for-nerve-health hub goes option by option, and the broader natural remedies guide applies the same evidence lens to non-pill approaches.
Devices and Hands-On Therapies

Several lower-tech options earn a real, if modest, place. A TENS unit has modest evidence but is inexpensive, very low risk, and something you control at home — a sensible symptom add-on rather than a primary treatment. Acupuncture has mixed but promising evidence, strongest for diabetic and chemotherapy-related neuropathy, and a low risk profile in trained hands. Foot massage, warm soaks, and similar comfort measures won't change the nerve but can genuinely improve a hard day, and dignity and comfort count.
TENS, acupuncture, and comfort measures offer modest, real, low-risk relief — but they work best stacked on a strong Tier 1 foundation, not asked to carry the whole load alone. The strongest plans combine a Tier 1 base, a Tier 2 medication, and a low-risk Tier 3 add-on.
The pattern across this whole tier is the same: modest, real, low-risk relief that works best layered on top of a strong Tier 1 foundation — not asked to carry the whole load alone. If a device promises to “reverse” or “cure” neuropathy, that single word tells you it has left the evidence behind.
What to Be Skeptical Of
I won't name brands, but I will name patterns, because the patterns are how you protect yourself and your wallet. Be skeptical of anything that promises to “reverse” or “cure” neuropathy in a fixed number of days, anything that bundles a cheap mixed-evidence supplement at a premium price with urgent countdown timers, any “clinic protocol” that requires large upfront cash and discourages a second opinion, and any therapy whose only evidence is testimonials and before/after stories.
The Word That Should Make You Pause
If a product, clinic, or device promises to “reverse” or “cure” neuropathy on a fixed timeline — or pairs a cheap mixed-evidence supplement with countdown timers and large upfront cash — that single word tells you it has left the evidence behind. Skepticism here protects your money and your hope for the options that have actually earned them.
Regenerative treatments like stem-cell and platelet-rich-plasma injections deserve special mention: they are biologically interesting and heavily promoted, but for neuropathy they remain experimental, with hype well ahead of high-quality evidence. That doesn't make them frauds — it makes them unproven and expensive, which is a very different thing from “Tier 1.” Healthy skepticism isn't pessimism. It's what keeps your money and hope available for the options that actually earn them.
How to Build Your Own Plan

Here's how I'd put this together if I were starting over. One: pin down the cause and treat it — that's non-negotiable and highest-value. Two: build the Tier 1 foundation (movement, rehab, protecting your feet and balance) regardless of what else you do. Three: if pain is significantly limiting your life, talk with your doctor about a first-line medication, expecting to trial and possibly combine. Four: layer a low-risk add-on you control — a coping skill, a TENS unit, an optional supplement — on top, not instead. Five: reserve Tier 4 procedures for genuinely refractory pain, with a specialist.
Spend your energy in evidence order, not advertising order
Treat the cause, build the Tier 1 foundation, add a doctor-guided first-line drug if pain limits your life, layer a low-risk add-on on top, and reserve procedures for truly refractory cases. A plan you understand and can stick with beats a “perfect” plan you abandon in three weeks.
Bring this framework to your appointment and ask, for any option offered: which job does this do, what's the evidence, what's the risk, and what's plan B if it doesn't work? Our guide to talking to your doctor about neuropathy pain can help you have exactly that conversation. A plan you understand and can stick with beats a “perfect” plan you abandon in three weeks.
Frequently Asked Questions
What is the most effective treatment for neuropathy?
For most people, the most effective treatment is identifying and treating the underlying cause, because that addresses the actual nerve damage rather than just masking symptoms. For diabetic neuropathy, tight blood-sugar control has the strongest evidence for slowing progression. When pain itself is the target, the best-evidenced symptom relief comes from first-line medications such as gabapentin, pregabalin, duloxetine, or amitriptyline, often combined with exercise and rehabilitation. There is no single treatment that works for everyone, which is why most effective plans layer several approaches.
Which neuropathy treatment has the strongest scientific evidence?
Treating the underlying cause has the strongest evidence overall. Among symptom treatments, the four first-line medications for neuropathic pain — gabapentin, pregabalin, duloxetine, and amitriptyline or nortriptyline — have the strongest clinical-trial support, with roughly equivalent average efficacy and added benefit from combining them. Spinal cord stimulation has strong evidence in carefully selected severe cases but is invasive. Exercise and physical therapy have lower-grade evidence but an excellent safety and quality-of-life profile.
Do supplements like alpha-lipoic acid actually work for neuropathy?
The evidence for alpha-lipoic acid is genuinely mixed. Some trials show benefit and others show none, with intravenous forms more consistent than oral capsules. It is reasonably safe, so it can be a defensible optional add-on, but it should not replace treating the cause or first-line care. B vitamins are a true treatment only when you have a measured deficiency. Most other supplements marketed for neuropathy lack strong evidence, so it is wise to treat them as experiments after the higher-evidence steps are in place.
Can any treatment reverse neuropathy?
It depends entirely on the cause and how early it is caught. Some neuropathies can improve substantially when the underlying driver is removed early, such as correcting a B12 deficiency, stopping alcohol, or stopping an offending medication. Long-standing nerve damage, especially from poorly controlled diabetes, is often only partly reversible, and the realistic goal becomes stopping progression and managing symptoms. Be very skeptical of any product that guarantees to reverse or cure neuropathy in a set number of days.
Why didn't the medication that helped someone else work for me?
Neuropathic pain responds very individually. In clinical trials, any single first-line drug gives meaningful relief to only a portion of people, and which drug works is not predictable in advance. This is normal and expected, not a sign that nothing will help you. The standard approach is to trial first-line options one at a time at adequate doses, and to combine two of them if a single drug is only partly effective, which research shows helps many people who did not respond to monotherapy.
How do I avoid wasting money on neuropathy treatments?
Spend in evidence order, not advertising order. Put your first energy and money into diagnosing and treating the cause, then into low-cost high-value steps like exercise and rehabilitation, then into doctor-guided first-line treatment. Be skeptical of anything promising to cure or reverse neuropathy on a timeline, anything sold with urgency and large upfront cash, and any therapy backed only by testimonials. Keeping your budget and hope available for the options that have actually earned them is itself a strategy.