
Burning Feet: Neuropathy vs. B12 Deficiency vs. Thyroid vs. Erythromelalgia
Your feet are burning. It's worse at night. You've Googled it, and now you have four possible explanations and more anxiety than answers. Is it neuropathy? A vitamin deficiency? Your thyroid? Something you've never even heard of?
Burning feet is one of the most common complaints I hear from our neuropathy community — and one of the most frustrating, because the burning sensation can come from several completely different conditions. The treatment that fixes one cause does nothing for another. Getting the right diagnosis isn't just academic — it's the difference between relief and months of wasted effort.
This guide walks you through the four most common causes of burning feet: peripheral neuropathy, vitamin B12 deficiency, thyroid disorders, and erythromelalgia. For each one, I'll explain what the burning actually feels like, what sets it apart, and which tests your doctor should order. By the end, you'll know what questions to ask at your next appointment.
How Each Condition Causes Burning Feet
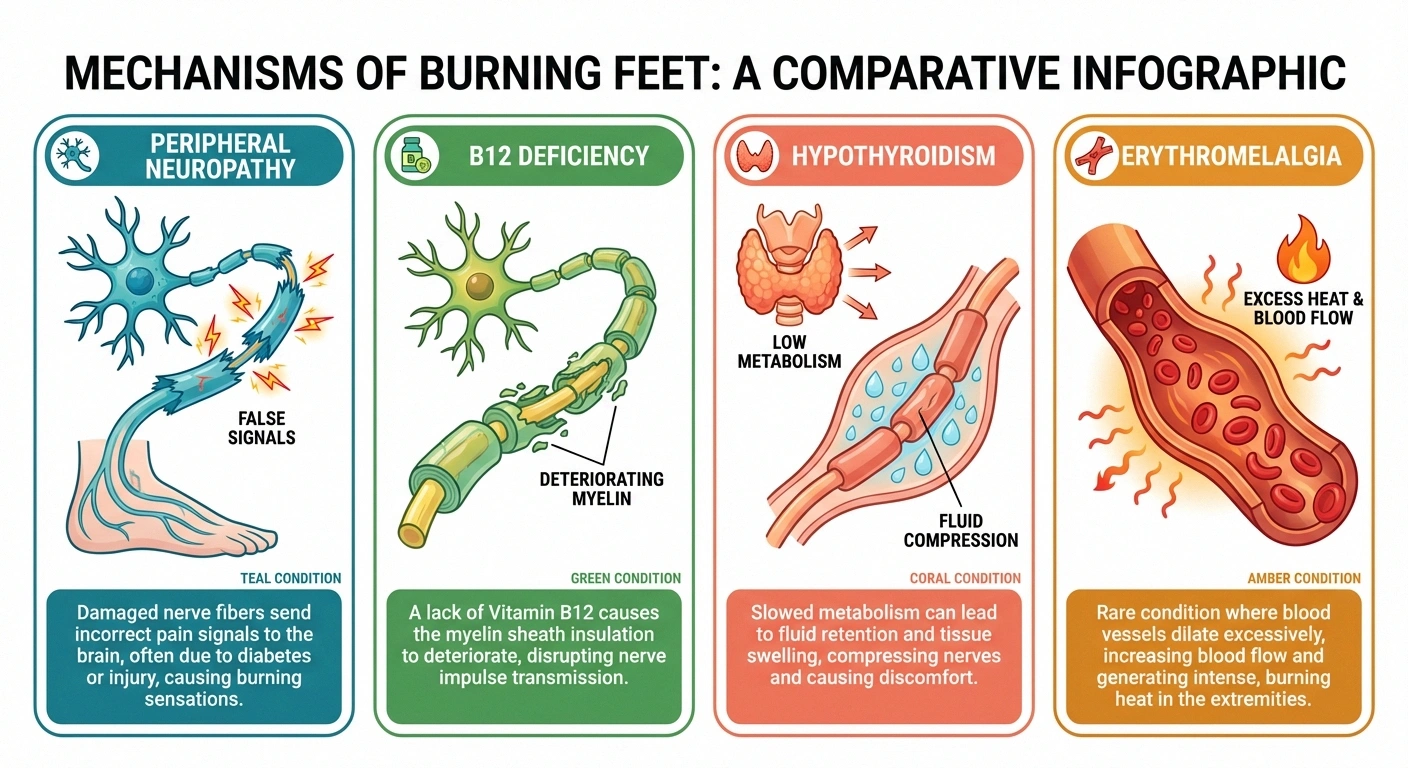
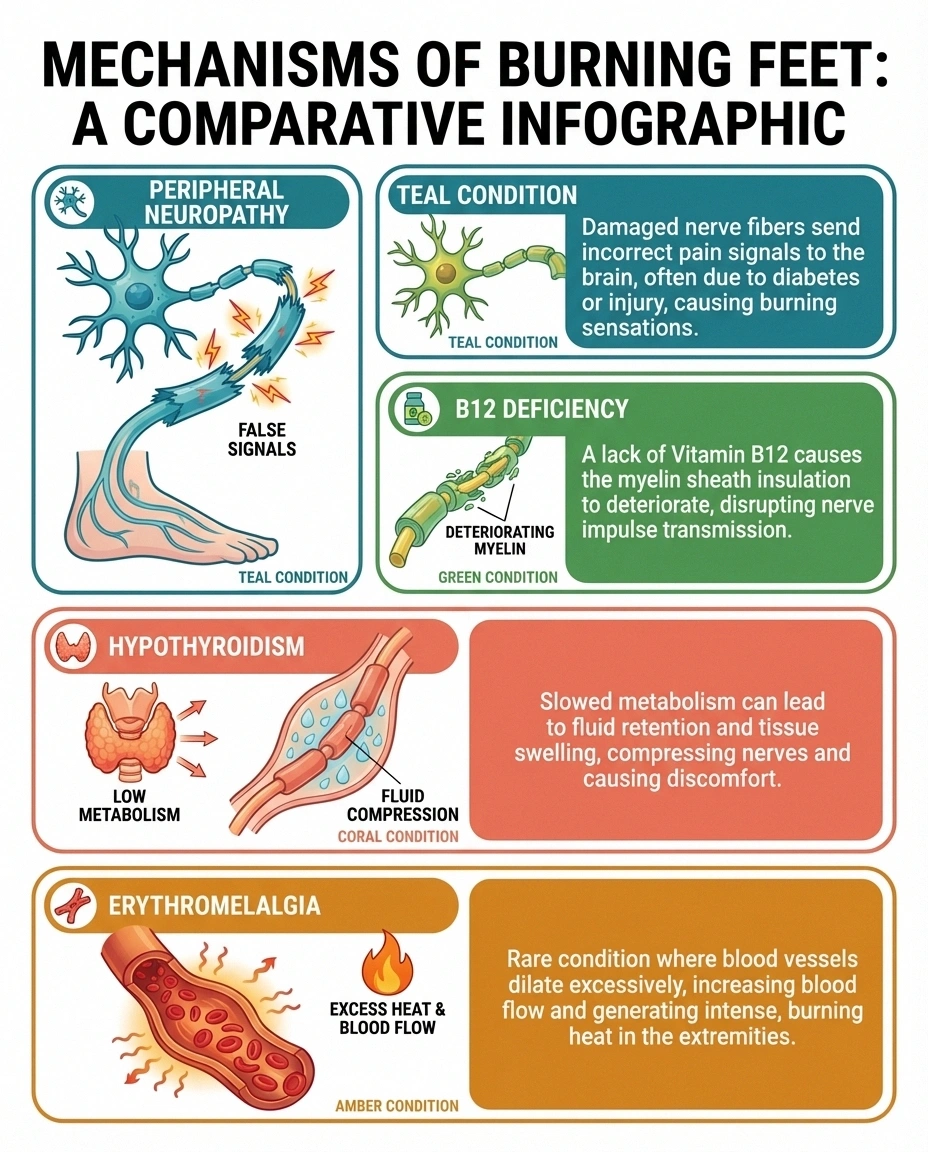
Before we compare symptoms side by side, it helps to understand the mechanism — why each condition makes your feet burn. The burning sensation has a different origin in each case, and that's why the treatments are so different.
Americans affected by peripheral neuropathy — the #1 cause of burning feet
Peripheral neuropathy causes burning because damaged nerve fibers send incorrect pain signals to the brain. The small nerve fibers (C-fibers and A-delta fibers) that detect temperature and pain malfunction, firing when they shouldn't. It's like a smoke alarm going off when there's no fire. This is the most common cause of burning feet, affecting roughly 20 million Americans according to the National Institute of Neurological Disorders and Stroke.
Vitamin B12 deficiency causes burning through a different pathway. B12 is essential for maintaining the myelin sheath — the protective insulation around your nerve fibers. When B12 levels drop, the myelin deteriorates, exposing the raw nerve to stimulation. This is technically a form of neuropathy (nutritional neuropathy), but it's worth distinguishing because it's often completely reversible with supplementation.
Hypothyroidism (underactive thyroid) can cause burning feet through fluid retention that compresses nerves, direct metabolic effects on nerve function, and by promoting B12 deficiency. A 2019 study in the Journal of Family Medicine and Primary Care found that subclinical hypothyroidism was associated with increased neuropathy severity, even in patients who didn't know they had a thyroid problem.
Erythromelalgia causes burning through a vascular mechanism — the small blood vessels in your feet dilate excessively, causing intense heat, redness, and burning pain. The feet literally become hotter than normal. Research published in Mayo Clinic Proceedings describes the classic presentation as episodic flares of redness, warmth, and burning pain, primarily affecting the feet in about 90 percent of patients.
Side-by-Side Symptom Comparison
Here's how these four conditions differ when you look at the specific patterns of burning feet. No single symptom is a definitive diagnosis on its own, but the pattern of symptoms together can point strongly toward one cause.
Quick Comparison: Where Do Your Feet Burn?
Neuropathy
Both feet equally, “stocking” pattern from toes upward. Gradual, symmetrical.
B12 Deficiency
Hands AND feet at the same time. This simultaneous pattern is a crucial clue.
Hypothyroidism
Diffuse, may include hands and legs. Often with heaviness or puffiness.
Erythromelalgia
Episodic. Feet turn visibly RED and HOT during flares. Normal between episodes.
Location and Distribution
Peripheral neuropathy: Burning typically starts in both feet symmetrically and progresses upward in a “stocking” pattern — toes first, then soles, then ankles. The key word is gradual and symmetrical. If one foot burns much more than the other, pure peripheral neuropathy is less likely.
B12 deficiency: Burning affects both hands and feet simultaneously. This is a crucial distinguishing feature. Unlike typical peripheral neuropathy, which starts in the feet and takes months or years to reach the hands, B12 deficiency can affect hands and feet at the same time because it damages the spinal cord (subacute combined degeneration) as well as the peripheral nerves.
Hypothyroidism: Burning tends to be diffuse and may affect areas beyond the feet — hands, arms, and legs. It's often accompanied by a general feeling of heaviness or puffiness in the affected limbs from fluid retention.
Erythromelalgia: Burning occurs in episodes and may affect one foot more than the other, or alternate between feet. During a flare, the affected foot will be visibly red and hot to the touch — you can actually feel the temperature difference with your hand. Between episodes, the foot looks and feels normal.
Timing and Triggers
Peripheral neuropathy: Burning is typically constant or worse at night. It doesn't come and go in dramatic episodes. Warmth, standing, and walking may worsen it, but it's generally always present to some degree.
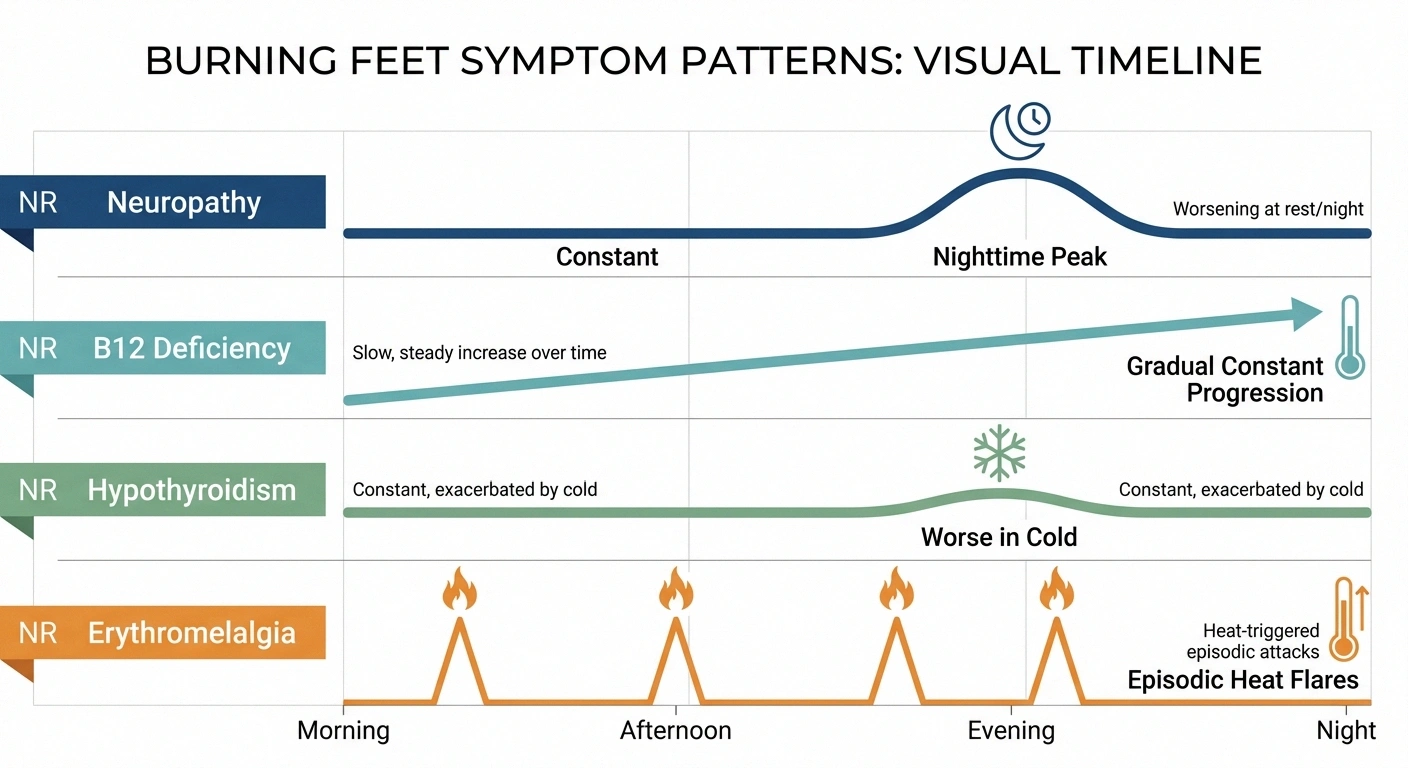
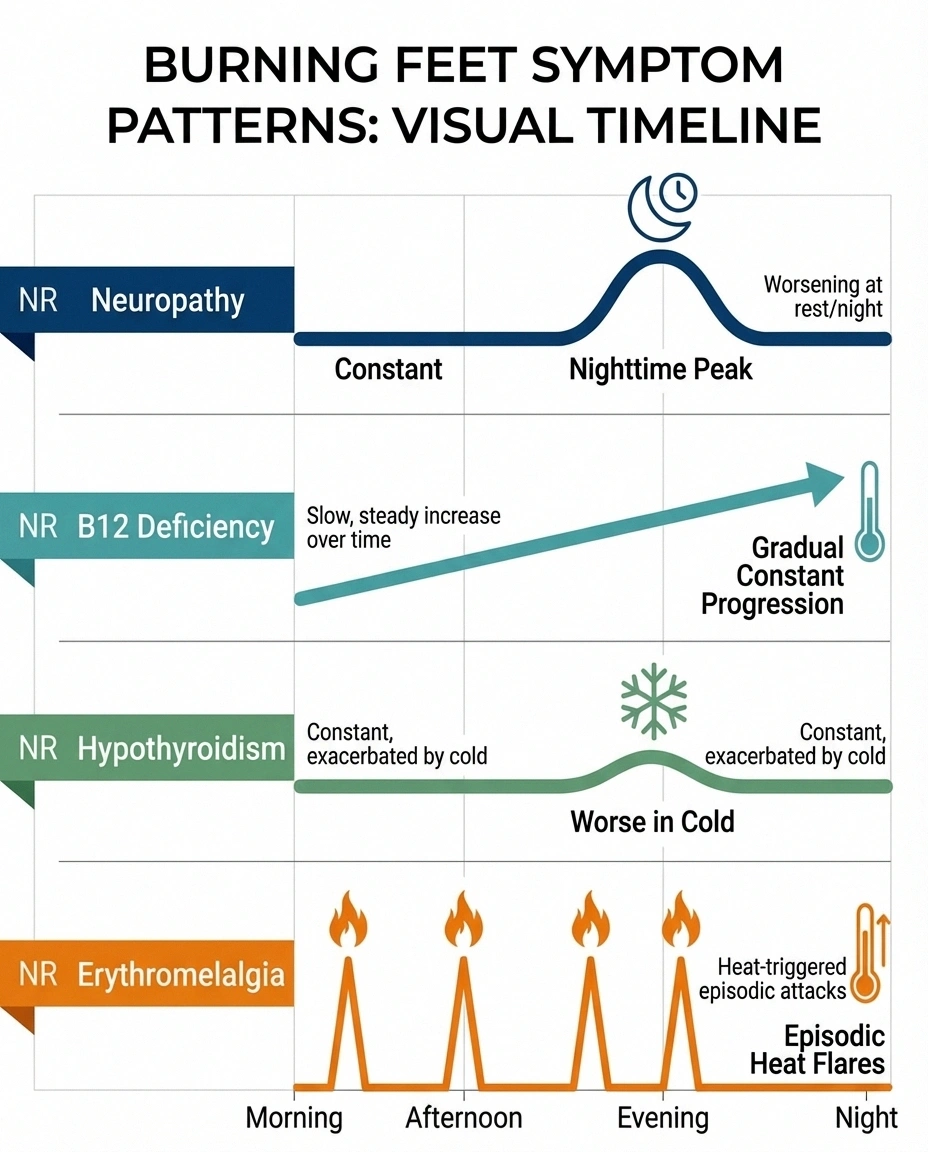
B12 deficiency: Symptoms develop gradually over weeks to months and are generally constant once they appear. They don't dramatically fluctuate with triggers.
Hypothyroidism: Burning may worsen with cold weather and improve slightly in warmth — the opposite of what you'd expect with neuropathy. Symptoms tend to worsen gradually alongside other thyroid symptoms.
Erythromelalgia: Burning occurs in episodes triggered by heat, exercise, warm water, standing, or wearing shoes. This is the most distinctive timing pattern. Cooling the feet provides dramatic, rapid relief — people with erythromelalgia often keep their feet in cold water or in front of a fan. Between flares, which can last minutes to hours, the feet feel relatively normal.
Accompanying Symptoms
Peripheral neuropathy: Numbness, tingling, pins and needles, reduced ability to feel touch or temperature, balance problems, muscle weakness in advanced cases. The burning is one symptom among many.
Pro Tip: Photo Your Symptoms
If your feet turn red during burning episodes, photograph them during a flare AND when normal. Erythromelalgia is often diagnosed by the visible redness, but your feet may look completely normal at your appointment. A photo is worth a thousand words to your doctor.
B12 deficiency: Fatigue, memory problems, difficulty concentrating (“brain fog”), a smooth or sore tongue, pale or slightly yellow skin, mood changes, and unsteadiness when walking (from posterior column damage). If your burning feet come with pronounced fatigue and cognitive symptoms, B12 deficiency should be high on the list.
Hypothyroidism: Weight gain, cold intolerance, dry skin, constipation, thinning hair, puffy face, slow heart rate, and depression. If you have several of these alongside burning feet, get your thyroid checked.
Erythromelalgia: The defining accompanying symptom is visible redness and measurable increased skin temperature during episodes. Some people also experience swelling. Unlike neuropathy, there's typically no numbness — the problem is too much sensation, not too little.
The Diagnostic Tests You Need
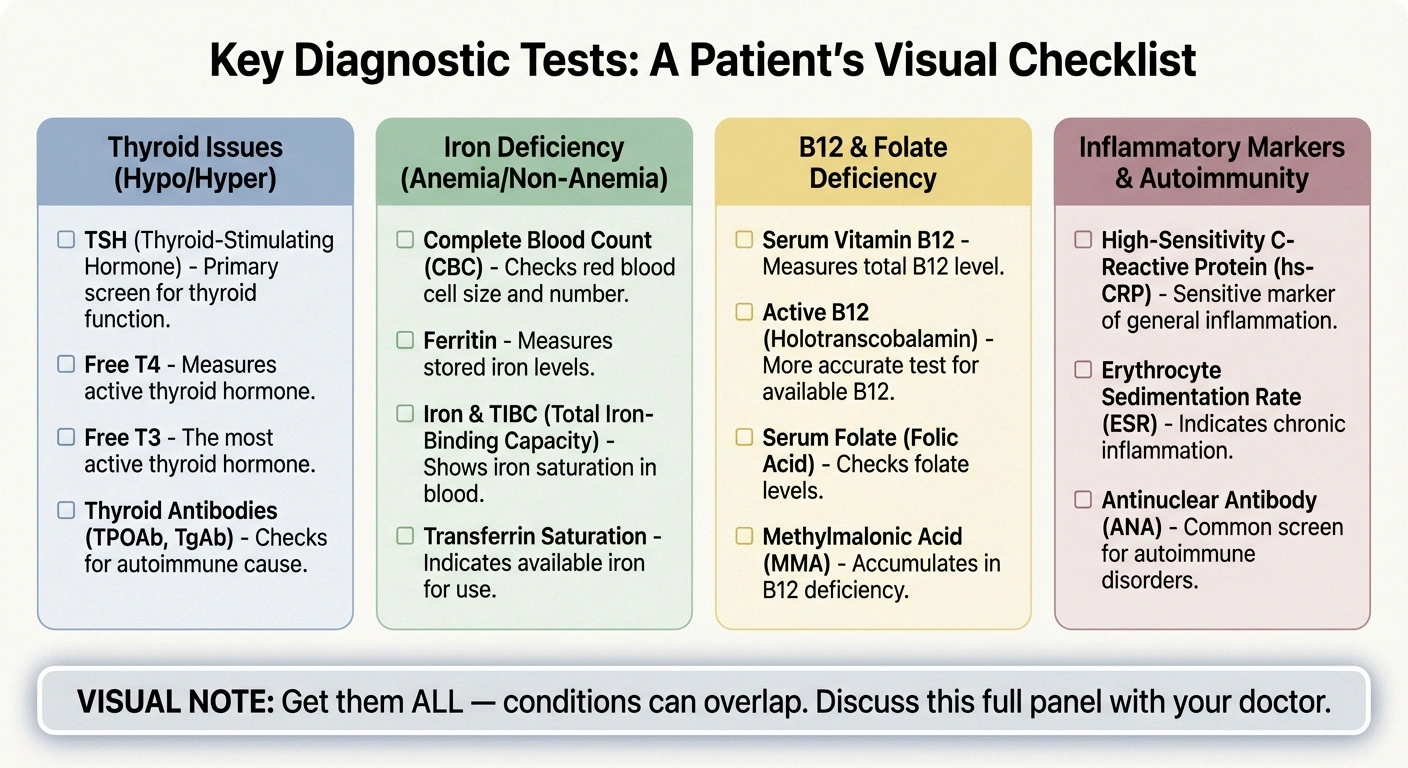
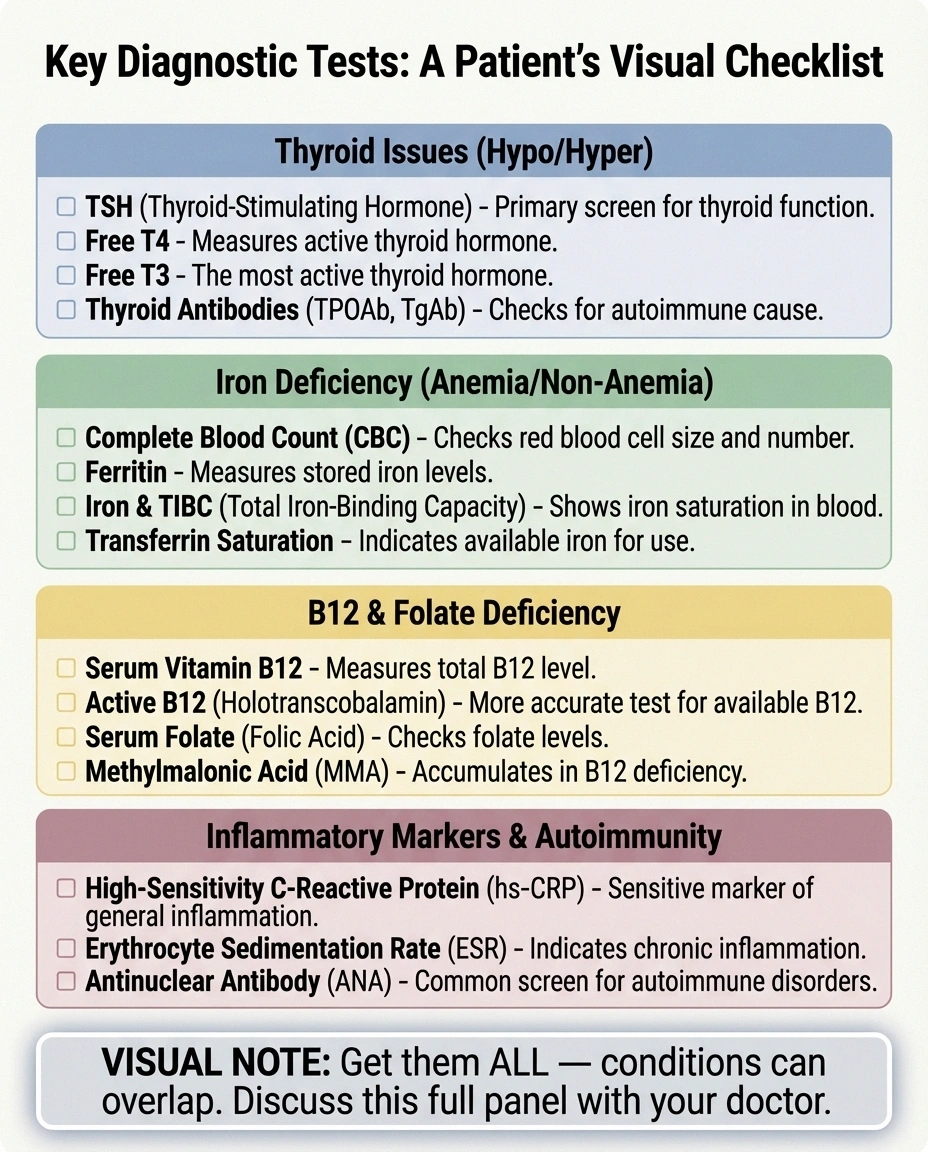
Here's what to ask your doctor to test for each condition. A thorough workup for burning feet should include most of these, because the conditions can overlap — you can have both B12 deficiency and neuropathy, for instance. For more detail on neuropathy testing, see our complete guide to neuropathy diagnosis.
For Peripheral Neuropathy
- Nerve conduction study (NCS) and electromyography (EMG) — measures how well your nerves transmit electrical signals. The gold standard for diagnosing large-fiber neuropathy.
- Skin biopsy (punch biopsy) — measures small nerve fiber density. This is the test for small fiber neuropathy, which NCS/EMG can miss.
- Hemoglobin A1c and fasting glucose — to check for diabetes or prediabetes, the most common cause of peripheral neuropathy.
For B12 Deficiency
- Serum B12 level — but be aware that “normal” ranges (typically 200-900 pg/mL) may be too broad. Neurological symptoms can begin at levels below 400 pg/mL, well within the “normal” range.
- Methylmalonic acid (MMA) — a more sensitive marker that rises when B12 is functionally low, even if serum B12 looks “normal.” This is the test that catches early deficiency.
- Homocysteine — also rises with B12 deficiency. Elevated homocysteine plus elevated MMA strongly confirms functional B12 deficiency.
- Complete blood count (CBC) — may show macrocytic anemia (large red blood cells), though neuropathy can develop before blood changes appear.
For Thyroid Disorders
- TSH (thyroid-stimulating hormone) — the primary screening test. Elevated TSH suggests hypothyroidism. Optimal range is typically 0.5-2.5 mIU/L, though “normal” lab ranges extend to 4.5 or higher.
- Free T4 and Free T3 — thyroid hormone levels. Low Free T4 with elevated TSH confirms hypothyroidism.
- Thyroid antibodies (TPO, thyroglobulin) — detect autoimmune thyroid disease (Hashimoto's), which is the most common cause of hypothyroidism and can co-occur with other autoimmune conditions that cause neuropathy.
For Erythromelalgia
- Clinical observation during a flare — the visible redness and measurable temperature increase are often diagnostic. Ask your doctor if you can photograph your feet during an episode to show at your appointment.
- Complete blood count with platelet count — to rule out myeloproliferative disorders (like essential thrombocythemia or polycythemia vera) that can cause secondary erythromelalgia.
- Genetic testing — in rare cases of early-onset erythromelalgia, mutations in the SCN9A gene (which encodes a sodium channel) may be responsible.
- Thermoregulatory sweat test — can help differentiate erythromelalgia from small fiber neuropathy.
Can You Have More Than One Condition?
Yes — and this is more common than many doctors realize. Several of these conditions overlap or feed into each other:

Conditions Can Chain Together
Hypothyroidism can cause B12 deficiency, which causes neuropathy. Diabetes increases risk of thyroid disorders AND B12 deficiency (via metformin). A thorough workup — not just one test — is essential. If your doctor finds one cause, ask: “Could there be an underlying cause of that?”
- B12 deficiency causes neuropathy. If your burning feet are from B12 deficiency, you technically have neuropathy — it's just a nutritionally-caused, potentially reversible type.
- Hypothyroidism can cause B12 deficiency. Autoimmune thyroid disease (Hashimoto's) is associated with pernicious anemia, which prevents B12 absorption. So you could have thyroid problems causing B12 deficiency causing neuropathy — a chain of causes.
- Erythromelalgia and small fiber neuropathy overlap. Research published in PAIN journal found that many patients with erythromelalgia also have evidence of small fiber neuropathy on skin biopsy. The two conditions may share underlying mechanisms.
- Diabetes complicates everything. Diabetic neuropathy is the most common cause of burning feet, but diabetes also increases the risk of thyroid disorders and B12 deficiency (especially if you take metformin, which impairs B12 absorption).
This is why a thorough workup — not just one test — is essential. If your doctor tests only for neuropathy and finds it, they may miss an underlying B12 or thyroid problem that's actually the treatable root cause.
Treatment Approaches by Condition
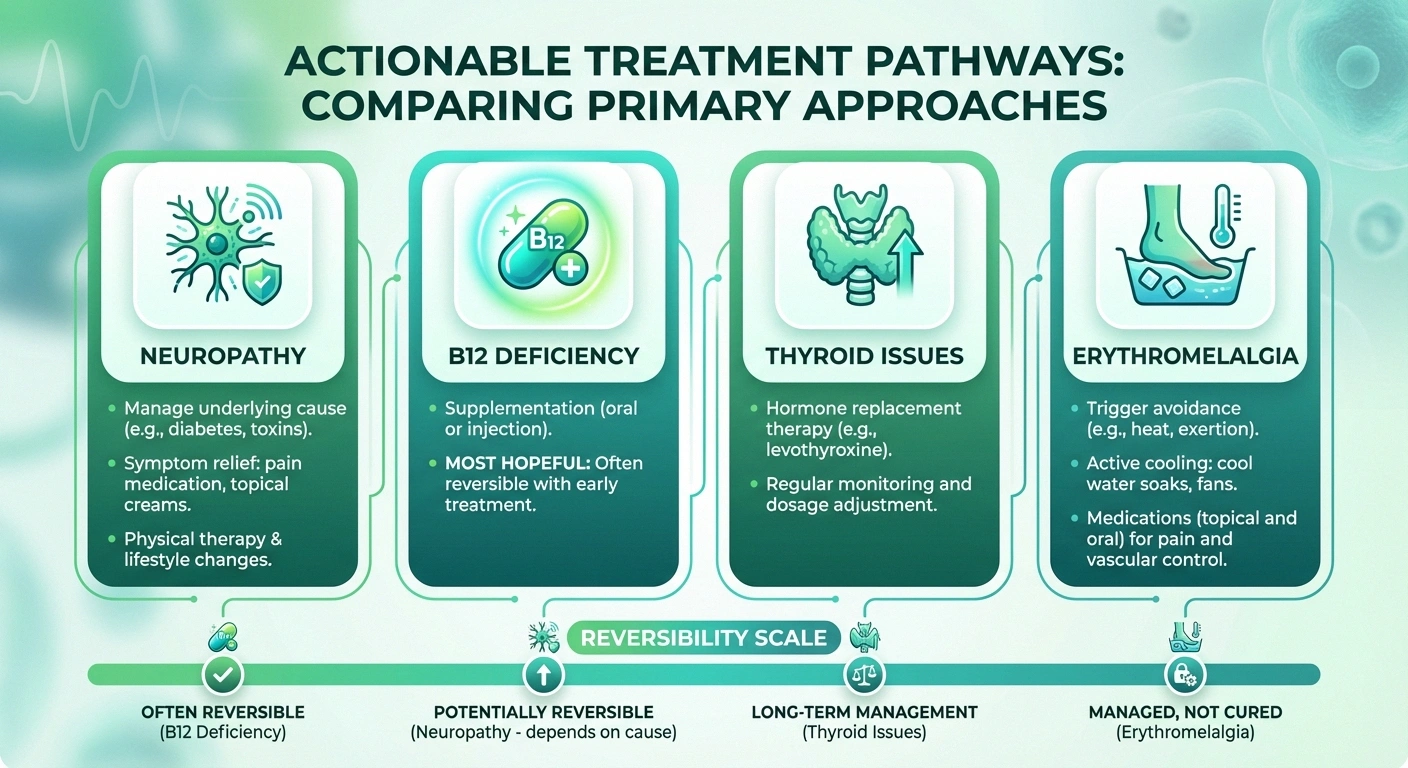
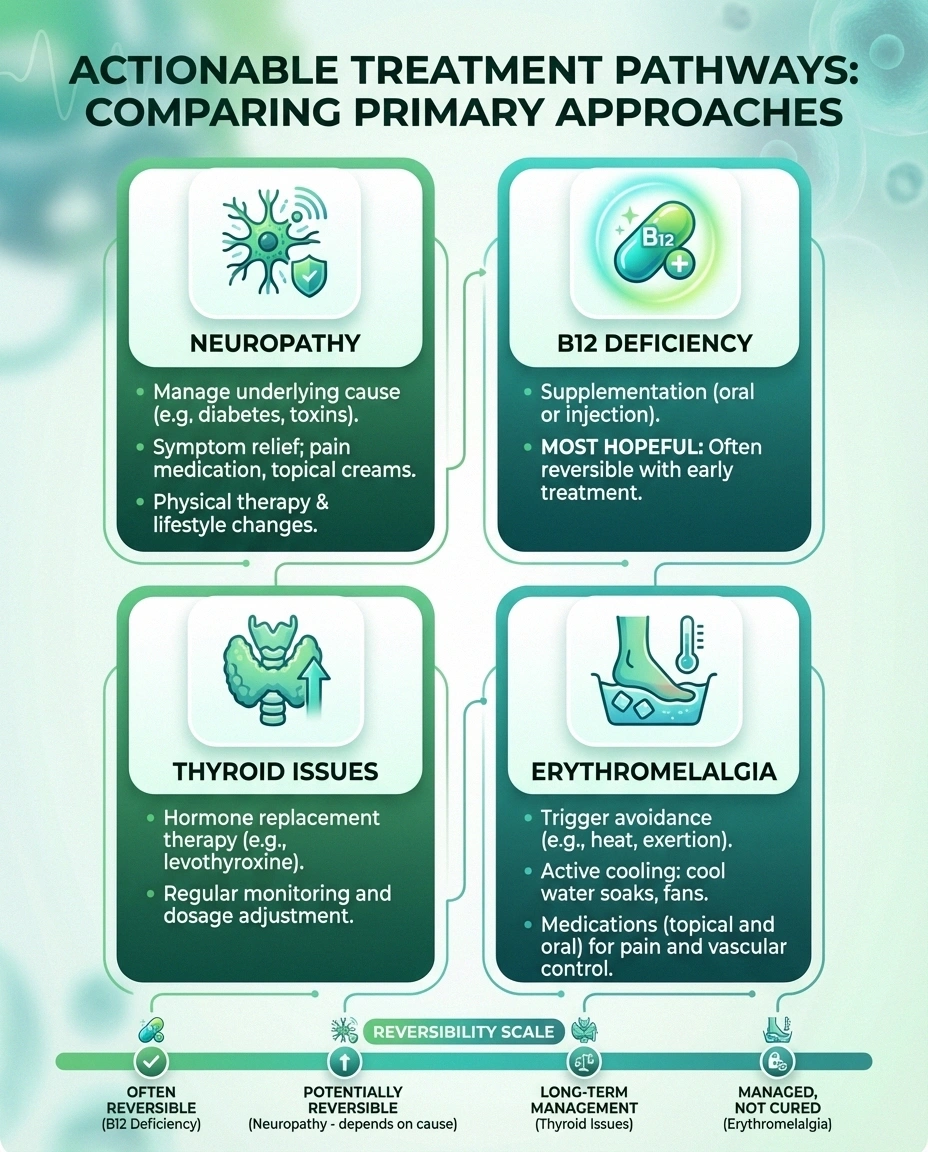
Treatment varies dramatically depending on which condition is causing your burning feet. Here's a high-level overview — each of these warrants a deeper conversation with your healthcare provider.
Peripheral Neuropathy Treatment
The focus is on treating the underlying cause (managing blood sugar for diabetic neuropathy, for instance) and managing symptoms. Options include medications like gabapentin, pregabalin, or duloxetine; topical treatments like capsaicin cream or lidocaine patches; and lifestyle approaches like exercise, diet modifications, and targeted supplements.
B12 Deficiency Treatment
This is the most hopeful scenario — B12 deficiency neuropathy is often reversible if caught early. Treatment involves B12 supplementation, either through intramuscular injections (faster repletion) or high-dose oral supplements (1,000-2,000 mcg daily). Improvement typically begins within weeks to months, though complete recovery can take 6-12 months depending on how long the deficiency persisted.
Hypothyroidism Treatment
Thyroid hormone replacement (levothyroxine) is the standard treatment. If hypothyroidism is causing your burning feet, nerve symptoms typically improve as thyroid levels normalize — though this can take several months. Your doctor should also check B12 levels, as thyroid disease and B12 deficiency frequently co-occur.
Erythromelalgia Treatment
Erythromelalgia treatment focuses on avoiding triggers (heat, prolonged standing, tight shoes) and cooling the feet during flares. Medications may include low-dose aspirin (especially for secondary erythromelalgia associated with blood disorders), topical lidocaine, gabapentin, or calcium channel blockers. Some patients respond to sodium channel blockers like mexiletine. This is a condition that often requires a specialist — a neurologist or dermatologist with experience in erythromelalgia.
When to See a Doctor
Burning feet should always be evaluated by a healthcare provider. But certain symptoms warrant more urgent attention:

Seek Urgent Care If
Sudden onset of burning in both feet with weakness (possible Guillain-Barré syndrome), burning with visible purple discoloration (vascular emergency), or rapidly progressive numbness moving upward. These require same-day medical evaluation.
- Sudden onset of burning in both feet, especially if accompanied by weakness — this could indicate Guillain-Barré syndrome, which requires emergency treatment
- Burning with visible color changes (redness, purple discoloration) — suggests a vascular component that needs assessment
- Progressive numbness moving upward from the feet — indicates worsening neuropathy that needs attention before motor nerves are affected
- Burning accompanied by difficulty walking or frequent falls — suggests motor nerve involvement
- Symptoms starting after a new medication — several medications can cause neuropathy as a side effect
For a deeper look at warning signs, see our guide on what neuropathy feels like and how to describe your symptoms to your doctor.
Frequently Asked Questions
What is the most common cause of burning feet?
Peripheral neuropathy is the most common cause of burning feet, with diabetic neuropathy being the single most frequent type. According to the Cleveland Clinic, about 50 percent of people with diabetes will develop some form of neuropathy. However, vitamin B12 deficiency is the most common reversible cause and should be tested in anyone with burning feet, regardless of other diagnoses.
Can burning feet be cured?
It depends entirely on the cause. Burning feet from B12 deficiency can often be completely reversed with supplementation if caught early enough. Burning from hypothyroidism typically improves with thyroid hormone replacement. Burning from diabetic neuropathy may be slowed or stabilized with good blood sugar control but is rarely fully reversed once nerve damage has occurred. Erythromelalgia is usually managed rather than cured, though some secondary cases resolve when the underlying condition is treated.
Should I take B12 supplements if my feet are burning?
Do not start supplementing without testing first. While B12 supplementation is generally safe, it is important to first confirm a deficiency with blood work. Taking B12 when your levels are already normal will not help burning feet and may mask the true underlying cause. Ask your doctor for a serum B12 level and a methylmalonic acid test for a complete picture.
How do I know if my burning feet are from erythromelalgia?
The most distinctive sign of erythromelalgia is visible redness and measurable warmth of the feet during burning episodes, with complete or near-complete resolution between episodes. If your feet turn red and feel hot to the touch when they burn, and if cooling them provides rapid and dramatic relief, erythromelalgia should be investigated. Take photos during a flare to show your doctor, as the feet may look completely normal at the time of your appointment.
Can thyroid problems really cause burning feet?
Yes. Hypothyroidism can cause peripheral neuropathy through several mechanisms: direct metabolic effects on nerve function, fluid retention that compresses nerves (similar to carpal tunnel syndrome), and by promoting B12 deficiency. A simple TSH blood test can screen for thyroid problems and should be included in the workup for anyone with unexplained burning feet.
What specialist should I see for burning feet?
Start with your primary care doctor for initial blood work including B12, thyroid function, and blood sugar. If the cause is not clear, a neurologist is the appropriate specialist for neuropathy evaluation including nerve conduction studies and skin biopsy. If erythromelalgia is suspected, a neurologist or dermatologist with experience in vascular pain conditions is ideal. For thyroid-related issues, an endocrinologist can optimize treatment.
The Bottom Line
Burning feet is a symptom, not a diagnosis. The same sensation can come from damaged nerves, missing vitamins, a sluggish thyroid, or overactive blood vessels — and each cause requires a completely different treatment. The worst approach is to assume it's “just neuropathy” without investigating the specific cause.
Ask your doctor for a complete panel: B12 with methylmalonic acid, thyroid function, blood sugar, and a neurological exam. If your current doctor dismisses your burning feet or doesn't run these basic tests, consider seeking a second opinion from a neurologist. The right diagnosis is the first step toward relief — and some of these causes are entirely treatable.
For more on understanding your symptoms and getting the right diagnosis, explore our guides on the stages of neuropathy, vitamin deficiency and neuropathy, and the thyroid-neuropathy connection.


